Heliobas Disciple
TB Fanatic
Pfizer's COVID-19 mRNA Product is 13-Times Less Effective at Preventing Infection With SARS-CoV-2 than Naturally Acquired Immunity!
More People Must Start Listening to Scientists Who Are Actually Following the Science
Pfizer's COVID-19 mRNA Product is 13-Times Less Effective at Preventing Infection With SARS-CoV-2 than Naturally Acquired Immunity!
More People Must Start Listening to Scientists Who Are Actually Following the Science
Dr. Byram W. Bridle
12 hr ago
A high-impact peer-reviewed scientific paper was just brought to my attention. It has been accepted for publication but has not made it into the print version of the journal yet. It was posted ‘online ahead of print’ back on April 5th, but I had not seen it until today. The paper is entitled “SARS-CoV-2 Naturally Acquired Immunity vs. Vaccine-induced Immunity, Reinfections versus Breakthrough Infections: a Retrospective Cohort Study”. It is being published in the journal Clinical Infectious Diseases, which has an impressive impact factor of 20.999. For a layperson, this means it is one of the top medical journals in the world.
Here is the take-home message as concluded by the authors in the discussion section of the paper:
“Our analysis demonstrates that SARS-CoV-2-naïve vaccinees had a 13.06-fold increased risk for breakthrough infection with the Delta variant compared to those previously infected, when the first event (infection or vaccination) occurred during January and February of 2021. The increased risk was significant for a symptomatic disease as well.”
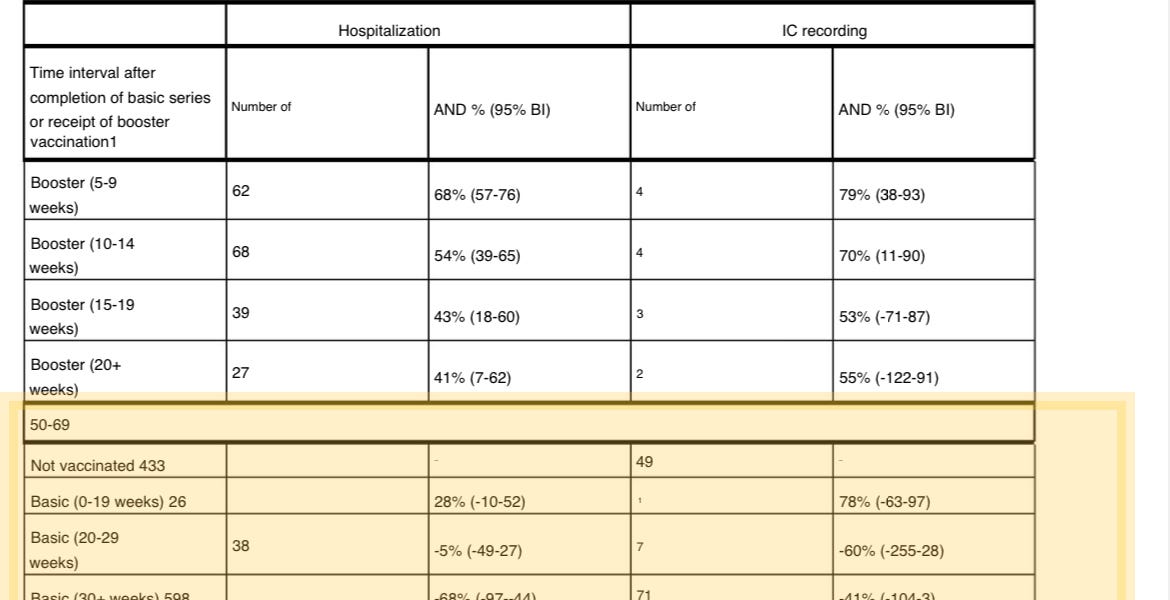
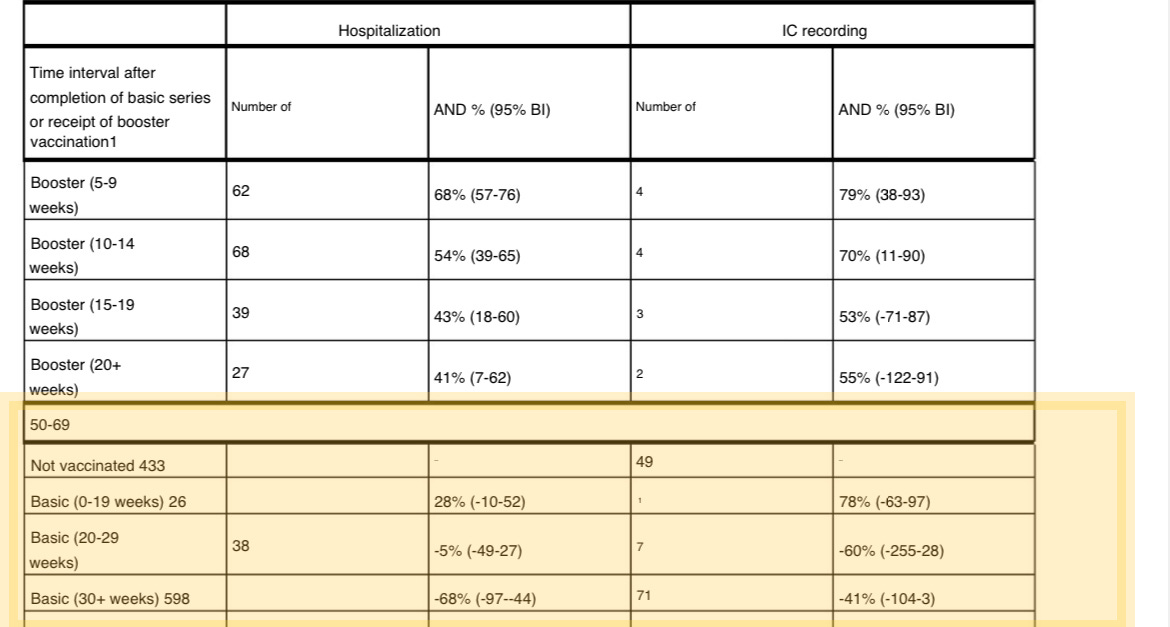
This study represents a critical head-to-head comparison of naturally acquired immunity to SARS-CoV-2 versus the SARS-CoV-2-specific immune response conferred by the two doses of the Pfizer-BioNTech mRNA product that was required to obtain the so-called ‘fully vaccinated’ status. This largely occurred in the context of the wave of cases that was dominated by the Delta variant. People whose first exposure was to natural infection with SARS-CoV-2 were compared to those whose first exposure was via receipt of Pfizer’s mRNA product. In other words, which source of ‘immunity’ could confer the best long-term protection against infection with SARS-CoV-2, which is the virus that causes COVID-19 in some people.
As demonstrated in this paper, people whose immune response was induced by Pfizer’s mRNA product were at 13-times greater risk of being infected with SARS-CoV-2 as compared to people with naturally acquired immunity!
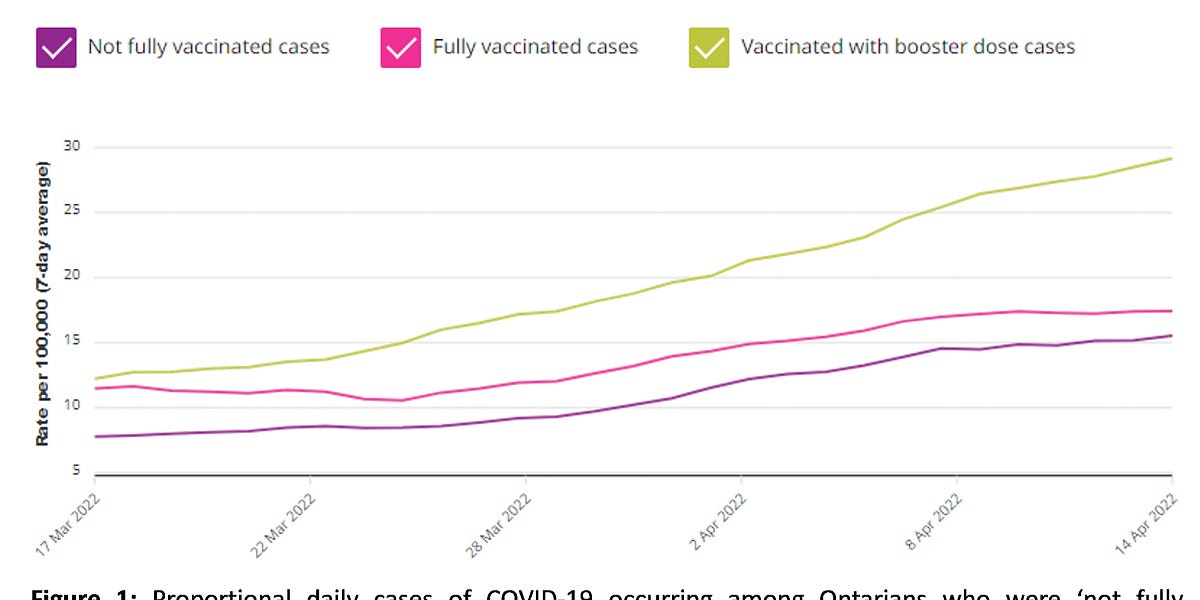
For those who had received Pfizer’s mRNA product, this increase in risk of infection also translated into a greater risk of the infection progressing to the disease that we call COVID-19. This news will be shocking for many. However, for many of us who have actually been following the science, this is not at all surprising. We have seen this unfolding for quite some time in public health data around the world. For example, see figure 1 below, which showed the trend in cases of COVID-19 by vaccination status in Ontario, Canada (where I live).
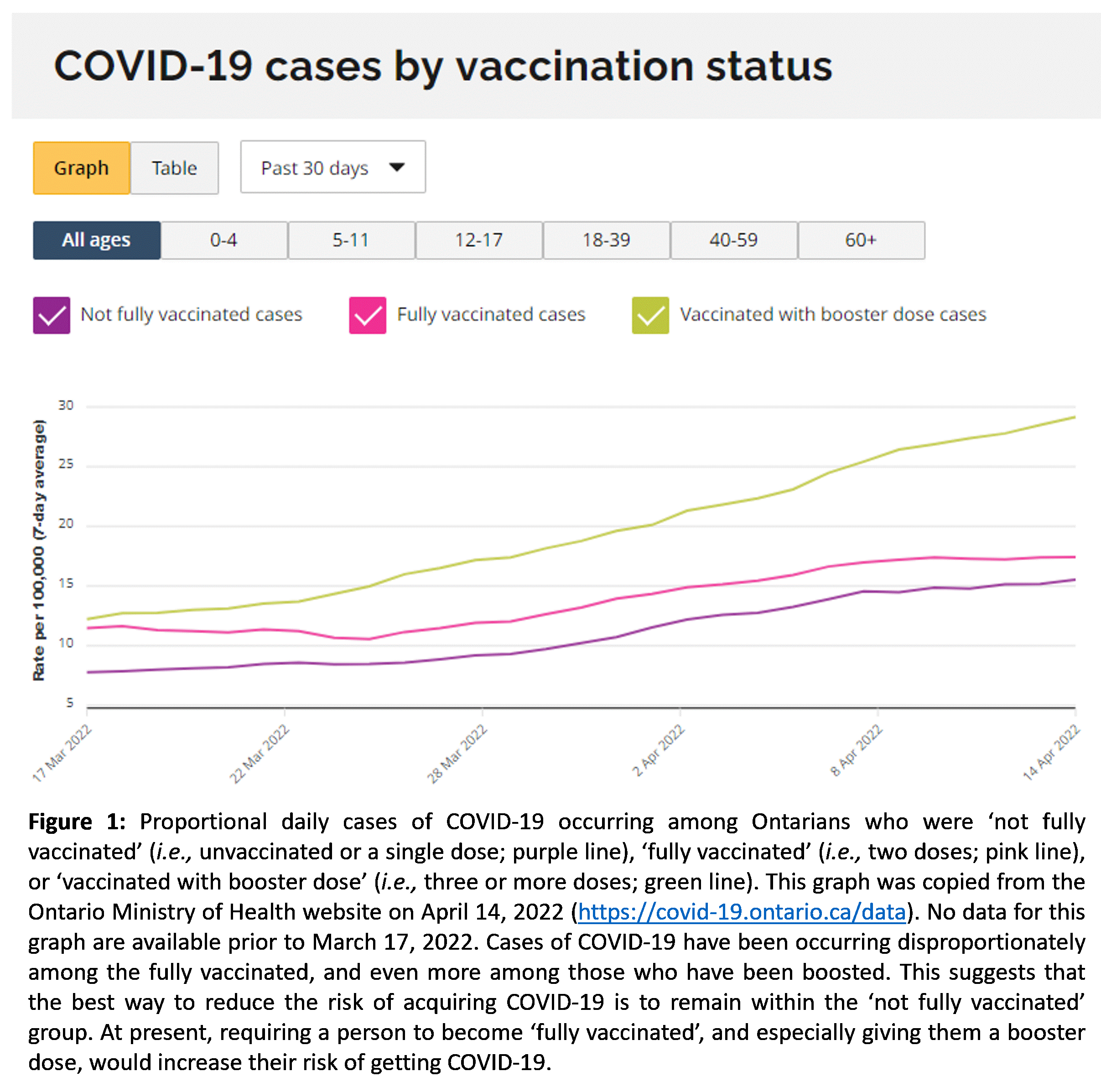
…I had been forewarning people since early 2022 about the the increased risk of acquiring COVID-19 if they were formally ‘vaccinated’ against COVID-19 as compared to those with broadly reactive naturally acquired immunity. This was based on a plethora of public health data. I used this particular figure to highlight the additional risk posed by third or more doses.
Some of this risk is likely accounted for by an increase in ‘risky behaviours’ by inoculated individuals who have become over-confident about the misleading information that overestimates the effectiveness of the shots. But a bigger concern is the potential for vaccine-enhanced infection or similar harmful mechanisms.
Here is an interesting side-note. As has been happening at high frequency throughout the declared pandemic, readily accessible and easy to digest data like those shown in Figure 1 above are no longer provided to the public. Check for yourself. Go to the same link from which I acquired the graph on April 14th. The link is here. The best that you can do is get tabulated raw data that you would need to graph yourself. Public health agencies should be held accountable for failing to consistently provide fully transparent and highly informative data in easy-to-interpret formats. They should also be questioned as to why they have constantly changed the way data are provided and shown; apparently correlating with when the data start to consistently contradict the so-called ‘acceptable narrative’.
Human Immune Systems Can Still Function Naturally in the Year 2022
What the scientific article by Gazit, et al. tells us is that naturally acquired immunity against SARS-CoV-2 is superior to the limited protection conferred by Pfizer’s mRNA product. This is just one of >150 peer-reviewed scientific publications that now confirm that natural immunity against this particular virus is better in every way to what can be conferred by the Pfizer shots. For me, as a vaccinologist, this is not at all surprising. Those of us developing vaccines always hold natural immunity as the gold standard. We endeavour to better understand natural immunity so we can try to come close to recapitulating it with a new vaccine against an infectious agent. It isn’t unusual for vaccines to induce sub-par responses compared natural immunity because we still have an imperfect understanding of the inner workings of the immune system. However, when it comes to responses induced by Pfizer’s mRNA product, they have obviously fallen far below the gold standard of natural immunity.
Another Call for Critical Thinking and Promoting Scientific Debate
I understand that many people are completely sold-out on the single public health narrative that has been deemed acceptable by power brokers. However, for the sake of their safety, that of their loved ones, and to avoid unnecessary mandate-induced segregation of the well-informed again, they really need to start critically assessing the science and asking tough questions of their physicians, public health officials and others who are promoting these inoculations.
Following are a few examples of questions for which answers should be demanded. Importantly, demand that a person’s answers be backed up by original science. Have them show you their reference(es). Hearsay evidence based on things like ‘because so-and-so said it is true and they seem to have a good reputation’ carries no weight. I am an expert in vaccinology and this has been officially confirmed in many court cases. This does not preclude me from having to provide references to justify all of my major assertions, nor should it. A fact is not defined by a person’s reputation. Scientific principles are defined by the weight of the scientific evidence.
Key Questions
- Why would I want to get a ‘vaccine’ targeting an outdated version of the SARS-CoV-2 spike protein that leaves me at a 13-fold greater long-term risk, compared to natural immunity, of getting infected with the virus and acquiring the disease that it is supposed to protect me against?
- I keep hearing that the ‘vaccine’ will dampen the severity of disease. Isn’t the best way to dampen severity by not acquiring the infection and the disease in the first place? As such, why is the importance of natural immunity being downplayed?
- If naturally acquired immunity is superior to immune responses conferred by Pfizer’s inoculations, why hasn’t testing for acquisition of natural immunity been made a priority? In Canada, we shut-down our task force assigned to monitor acquisition of naturally acquired immunity early in the declared pandemic.
- Why would anybody want to push a ‘vaccine’ on me without first knowing my natural immunity status, especially since the latter has proven to be superior to the former?
- Why would anyone push Pfizer’s mRNA product on children who are at almost no risk of experiencing severe COVID-19 when their immune systems are naïve to SARS-CoV-2; and worse, when the vast majority already have superior naturally acquired immunity?
- When most people have likely been exposed to SARS-CoV-2, especially following the highly infectious Omicron wave, why are outdated booster doses being promo