Since the subvariant was first detected at the end of April, experts say, it's been a slow rise to the top for BA.5. Here's what else to know.

news.yahoo.com
(fair use applies)
BA.5 makes up nearly 80% of new COVID-19 cases. Here's what to know about the subvariant
Adrianna Rodriguez, USA TODAY
Thu, July 21, 2022, 12:39 PM
The BA.5 subvariant of omicron dominates the summer wave of COVID-19 in the USA, making up nearly 80% of new cases,
according to the Centers for Disease Control and Prevention Nowcast model.
In the most recent week, ending Wednesday, 29 states reported more cases than the week before, a USA TODAY analysis of Johns Hopkins University data shows. Twenty states had more deaths than a week earlier.
Hospitals in 35 states reported more COVID-19 patients, and hospitals in 25 states had more patients in intensive care beds, according to Health and Human Services data.
Here’s what you should know about BA.5.
When did BA.5 start?
BA.5 was detected in the USA at the end of April, experts said.
The subvariant was first seen in South Africa “but that doesn’t mean that it arrived (to the U.S.) from South Africa,” said David Dowdy, an epidemiologist at Johns Hopkins Bloomberg School of Public Health. Researchers don’t know where it came from because of limited surveillance.
The first cases appeared in the Northeast, then spread during the past month to Southern, Midwestern and Western states, Dowdy said.
“It’s been sort of a slow rise since that time,” he said. “It’s taken about two months to get to the current state where we think BA.5 probably accounts for about two-thirds of all COVID cases.”
What does BA.5 stand for?
The World Health Organization uses the Greek alphabet as a classification system to simplify understanding and avoid stigmatizing countries where strains of the SARS-CoV-2 virus that causes COVID-19 are identified.
The WHO named the original B.1.1.529 variant after the 15th letter, omicron. Within variants, the agency assigns numbers to sublineages.
“These represent the numbers and types of mutations within that particular variant,” said Dr. David Weber, professor of medicine pediatrics and epidemiology at University of North Carolina, Chapel Hill. “It’s a way of knowing which variant they’re dealing with.”
BA.5 is classified as an omicron variant but has mutations that distinguish it from other omicron subvariants, such as BA.1 and BA.2.
BA.5 variant symptoms in adults, kids
Clinicians said many BA.5 symptoms are similar to those seen in previous variants, including congestion, headaches, cough and fever.
Children tend to have more gastrointestinal symptoms, such as nausea, abdominal pain, vomiting and diarrhea, compared with adults, said Dr. Claire Bocchini, an infectious disease specialist at Texas Children’s Hospital.
She’s seen more cases of croup in kids.
The Mayo Clinic defines croup as an infection of the upper airways that obstructs breathing and causes a “barking” cough.
“Certainly this is an infection to pay attention to for parents of children because while most children don’t require hospitalization, a few do,” Bocchini said.
How long does BA.5 last?
Though some people don't experience any symptoms with BA.5, experts said those who do can expect to feel sick for a few days up to a few weeks.
“It varies on a wide spectrum,” said Dr. Mobeen Rathore, professor at the University of Florida College of Medicine and a member of the American Academy of Pediatrics committee on infectious diseases.
Bocchini said the normal course of illness is “one to two weeks of acute symptoms,” but those who are hospitalized may have the disease for much longer.
“We are very familiar with the prolonged hospitalizations from complications from COVID,” she said.
Can you get BA.5 twice?
There's limited data to support whether a person can get BA.5 twice, but health experts said it's unlikely to happen within the first month after infection.
“For the first couple of weeks, if you have a healthy immune system, you’re probably going to be fully resistant to get reinfected,” Dowdy said.
That protection wanes, he said. If a person is exposed to COVID-19, it’s possible to get reinfected with the same variant two to four months after infection.
It’s unlikely BA.5 will keep circulating over the next few months as the population builds up immunity against the subvariant. It’s more likely that another variant or subvariant of omicron will emerge as the virus attempts to bypass that immunity and infect as many people as it can.
It’s a “bit of a cat and mouse game between the virus and our immune systems,” Dowdy said. “If we don’t see another subvariant emerge for the next couple of months, then yes, absolutely people will be reinfected with BA.5.”
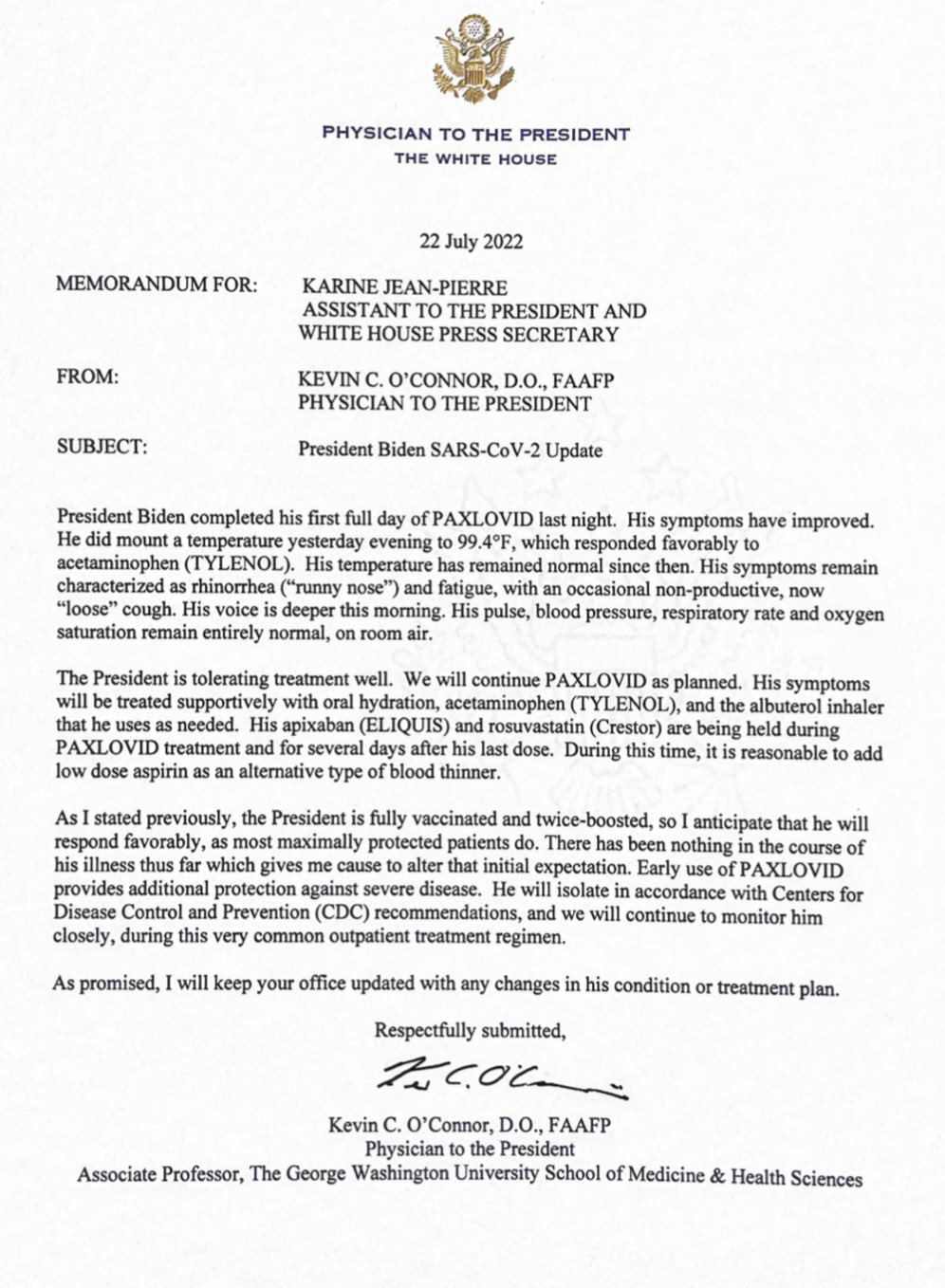
What to do if you get infected by BA.5
If you test positive for the coronavirus or feel sick with related symptoms, the
CDC recommendations say stay home for at least five days and isolate from other household members.
The agency advises wearing a well-fitted mask around others in the home.
If you're fever-free for 24 hours and symptoms improve after the five days, the CDC says you can end isolation, but take precautions for five additional days. This includes wearing masks and avoiding travel.
How are BA.4 and BA.5 different? What other COVID-19 variants are there?
BA.4 and BA.5 share mutations with other omicron subvariants, such as BA.1 and BA.2, but contain additional mutations within the spike protein,
according to the National Institute for Communicable Diseases, a public health institute in South Africa.
The two subvariants are identical to each other in terms of spike protein mutations, the institute said, but differ in mutations that are outside the spike gene.
BA.5 evades immunity better than BA.4, Weber said; however, it’s not believed to be more transmissible or cause more severe disease.
Except for a few random cases, Dowdy said, there’s probably no other coronavirus variants in circulation outside omicron and its sublineages. Delta and the variants that preceded it are likely out of the picture.
“When we’re talking about COVID, we’re talking about omicron now,” he said.





















") !
!

 I hope we hear back and what would be great is if Del hosted another debate between the two (they did a debate and a round table for Epoch Times a few months back, they are friends, they appear together at events, etc.).
I hope we hear back and what would be great is if Del hosted another debate between the two (they did a debate and a round table for Epoch Times a few months back, they are friends, they appear together at events, etc.).