https://www.msn.com/en-us/health/medical/with-a-sniff-or-a-swallow-new-vaccines-aim-to-put-the-brakes-on-covid-19-spread/ar-AAZI9mb
(fair use applies)
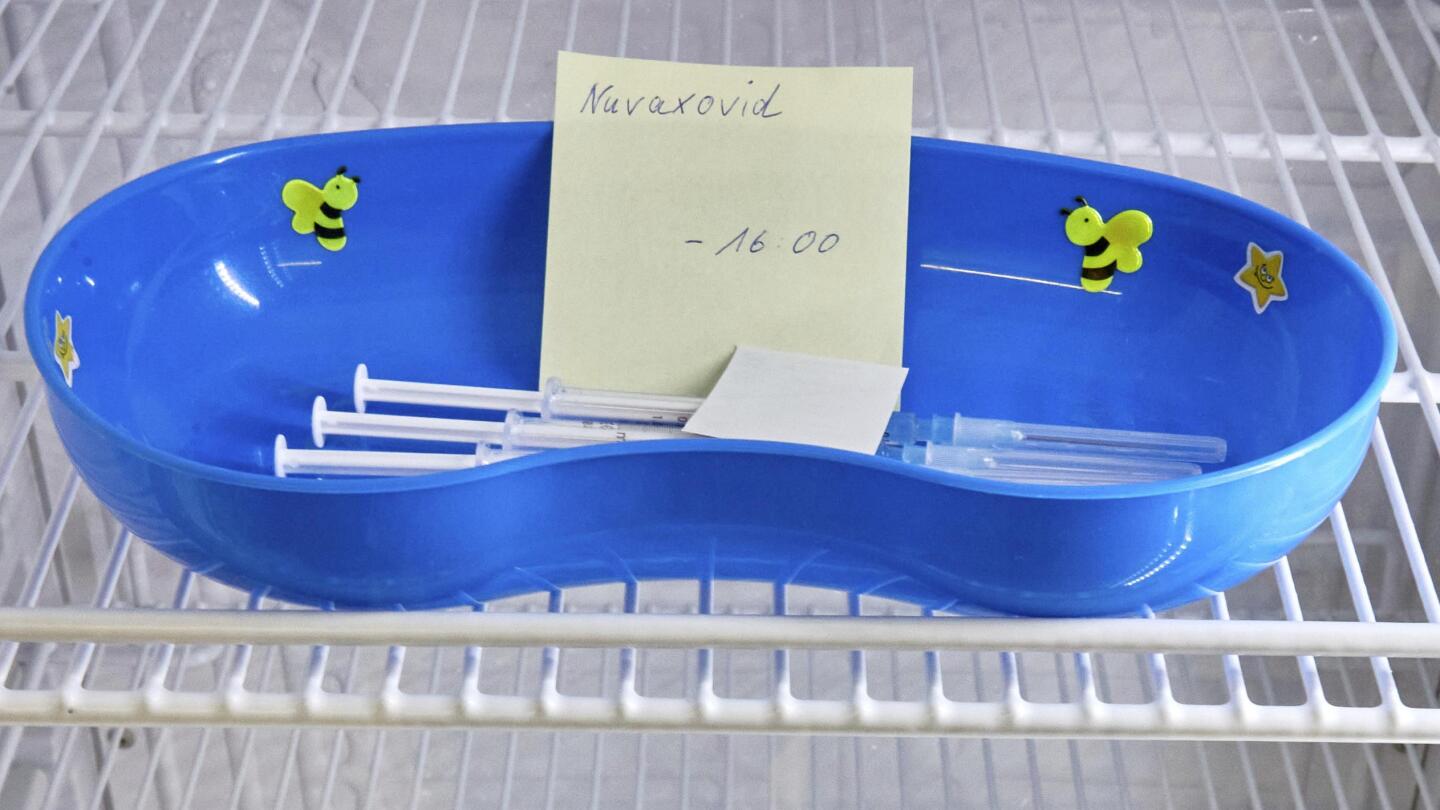
With a sniff or a swallow, new vaccines aim to put the brakes on Covid-19 spread
Brenda Goodman
5 hrs ago
Injected vaccines against the coronavirus that causes Covid-19 have been hugely successful, saving nearly 20 million lives globally in their first year of use and slashing the pandemic’s death toll by an estimated 63%, according to a
recent study.
Yet good as these shots are, they have not stopped the virus from spreading from person to person.
As the SARS-CoV-2 virus spreads, it changes. That’s helped it get past our firewalls, the immunity created by vaccines or left behind after we recover from an infection. Which is why, well into the third year of the pandemic, we’re in the midst of another wave of Covid-19 caused by the most immune-evasive variant yet, BA.5. And more variants are coming.
Even as vaccine manufacturers race to update the first-generation shots in the hopes of patching up our protection for the fall, other scientists are taking a different approach, making vaccines delivered via nasal sprays or tablets that would deploy more immune defenders to the body’s front lines: the lining of the mouth, nose and throat.
“The hope is to shore up the defenses right there in the nose so that the virus can’t even replicate in the nose,” said Dr. Ellen Foxman, an immunobiologist at the Yale School of Medicine. “And then someone who has a really effective mucosal vaccination can’t even really support viral replication or make viruses that can infect other people.
“That would be like the holy grail,” said Foxman, who helped plan the International Congress of Mucosal Immunology
meeting this week in Seattle, which is sponsored by pharmaceutical companies Pfizer, Janssen and Merck.
If it works, there’s hope that mucosal immunity could slow the development of new coronavirus variants and finally bring the Covid-19 pandemic under control.
There’s a long way to go before that happens, however, and many scientists say the approach needs an injection of funding to accelerate the pace of development, much in the same way the billions of dollars doled out by Operation Warp Speed delivered the first generation of Covid-19 vaccines in record time.
An old approach meets new technology
The idea behind vaccinating the mucosa – the lining of “the tube” (as mucosal immunologists refer to it) that runs from our nose and mouths to our lungs and guts – isn’t new. There are
nine existing vaccines that work this way, including oral drops that protect against polio, cholera, salmonella and rotavirus, and a nasal spray, FluMist, that inoculates against the flu.
Most are based on the oldest types of vaccine technologies, using killed or weakened versions of a virus or bacteria to teach the body how to recognize it and fight it off when a real infection gets underway.
Because of those actual pathogens, some people can’t use these kind of vaccines. It’s risky to expose certain groups – including pregnant women and those with weakened immune systems – to even weakened viruses.
None has achieved the goal of blocking the transmission of an infection, but that may be because they haven’t gotten the same kind of investment as injectable vaccines, says Ed Lavelle, an immunologist at Trinity College in Dublin.
“What hasn’t really happened with mucosal vaccines is kind of huge advances in technology that have happened with injectable vaccines, even before Covid,” Lavelle said.
That may be about to change, however.
Can nasal spray vaccines put the brakes on new variants?
More than a dozen nasal spray vaccines against Covid-19 are being tested around the world. Many use new kinds of technologies, like delivering instructions for making the spike protein of the coronavirus through harmless Trojan horse viruses. Others aim to deploy the mRNA technology that was so successful in the injectable vaccines in the form of a nasal spray.
One company, Vaxart, has even made a tablet that delivers instructions for making parts of the new coronavirus to the gut, which then builds immunity in “the tube.”
In
animal tests, hamsters vaccinated in the nose or mouth have been less likely to spread a SARS-CoV-2 infection to uninfected animals that are in separate cages but share the same air.
“What we found is that if you did an oral immunization, you inhibited the ability for that breakthrough to infect other animals,” said Sean Tucker, chief scientific officer for Vaxart.
The Vaxart tablet, which is about the size and shape of an aspirin, uses an adenovirus – the same delivery system utilized by the Johnson & Johnson and AstraZeneca Covid vaccines – to ferry instructions for making parts of the SARS-CoV-2 spike protein into cells in the gut, which stimulates the release of antibodies in the nose and mouth.
In an early trial that included 35 participants, 46% had an increase of antibodies in their nose after taking the tablet vaccine. Those who did seemed to create a broad spectrum of immunity to a number of types of coronaviruses, and they appeared to hold on to that protection for about a year. That may be a bit longer than injectable vaccines, though more research is needed to confirm those results.
Tucker is presenting these early results Monday at the Seattle conference. He says they’ll also be published as a preprint study in the coming days.
A phase 2 trial of a tablet with a slightly different formulation, involving almost 900 participants, is also underway, Tucker says. It is scheduled to be completed next summer.
Most of the mucosal vaccines under development are designed to be delivered as a squirt of liquid or mist up the nose, and many are intended to be used as boosters in people who’ve had a complete primary series of Covid-19 vaccines.
“I don’t think of them as nasal vaccines. I think of them as nasal boosts,” said Jennifer Gommerman, an immunologist at the University of Toronto who specializes in tissue-specific immunity.
That’s important, Gommerman says, because nasal vaccines – like FluMist – haven’t really worked all that well.
The next generation of inoculations will be something different, she says. They will build on the body-wide immunity that was created by shots; they’ll just redeploy it to the nose and throat where it is needed most, she says.
“But here, we’re actually talking about something else, where we’re talking about building on the systemic immunity that was induced by a vaccine to a three shots of mRNA and then training that systemic immunity to go to the upper respiratory tract by boosting through the nose,” Gommerman says.
One such approach was recently tested by Akiko Iwasaki, an immunobiologist at Yale University. According to their
preprint study, Iwasaki and her team inoculated mice with a low dose of Pfizer’s Comirnaty mRNA vaccine and followed up two weeks later with a boost of mRNA vaccine delivered via a nasal spray. The low dose of the injected vaccine was meant to simulate waning immunity. Other groups of mice got only an injection or only a dose of vaccine in the nose.
Only the group that got the injection followed by the nasal spray developed robust immunity against the Covid-19 virus.
“That approach we have shown in the mouse model to be 100% protective against lethal dose of SARS-CoV-2 infection, and it dramatically reduces the viral load in the nose and in the lung,” Iwasaki said.
Going for IgA antibodies
Mucosal vaccines also target a slightly different part of the immune system than shots.
Injections trigger the body to make antibodies against the virus that causes Covid-19. Most of these are Y-shaped proteins called IgG antibodies that are programmed to recognized and block specific parts of the SARS-CoV-2 virus along its spikes, the parts of the virus that latch onto and infect our cells.
A much smaller portion of these are IgA antibodies, and they look like two Ys joined together at their tails and turned sideways so it looks more like a dog bone, Gommerman says.
Like bouncers at a bar, IgA antibodies are the primary immune molecules on guard in the mucosa.
These molecules are beefier than IgG antibodies. They have four arms instead of two, and they’re special because they’re less picky about what they grab onto than IgG antibodies.
“They might be a little more promiscuous in the way they recognize different variants. And that’s obviously a plus,” Gommerman said.
Shots increase IgA antibodies in the nose for a short time, but the hope is that mucosal vaccines will really ramp up the population of these sentries and help them stay active for longer.
“Whether they’ll be able to confer complete sterilizing immunity, that’s a very tall order,” Gommerman said. “But we should be now working on ways to slow down person-to-person transmission, because this virus continues to mutate and then fools our immune system and gets past that mucosal layer.
“This is now a very contagious virus,” she said.
Iwasaki says she would love to move her vaccine out of animal studies and into clinical trials in people.
“We’re still at the stage where we’re kind of struggling to raise money, even make the vaccine for human use, because it takes millions of dollars, and we are not sitting on that kind of money for research lab,” she said, “so not yet.”


 www.theepochtimes.com
www.theepochtimes.com














 Igor’s Newsletter
Igor’s Newsletter



")