Advisors to the Centers for Disease Control and Prevention on Tuesday unanimously recommended Novavax’s COVID-19 vaccine, claiming the unvaxxed are the product’s “primary target population."

childrenshealthdefense.org
(fair use applies)
What You Don’t Know Could Hurt You: Novavax’s ‘Loud-and-Clear’ Nanoparticle Adjuvant
Advisors to the Centers for Disease Control and Prevention on Tuesday unanimously recommended Novavax’s COVID-19 vaccine, claiming the unvaxxed are the product’s “primary target population."
By
Children's Health Defense Team
07/20/2022
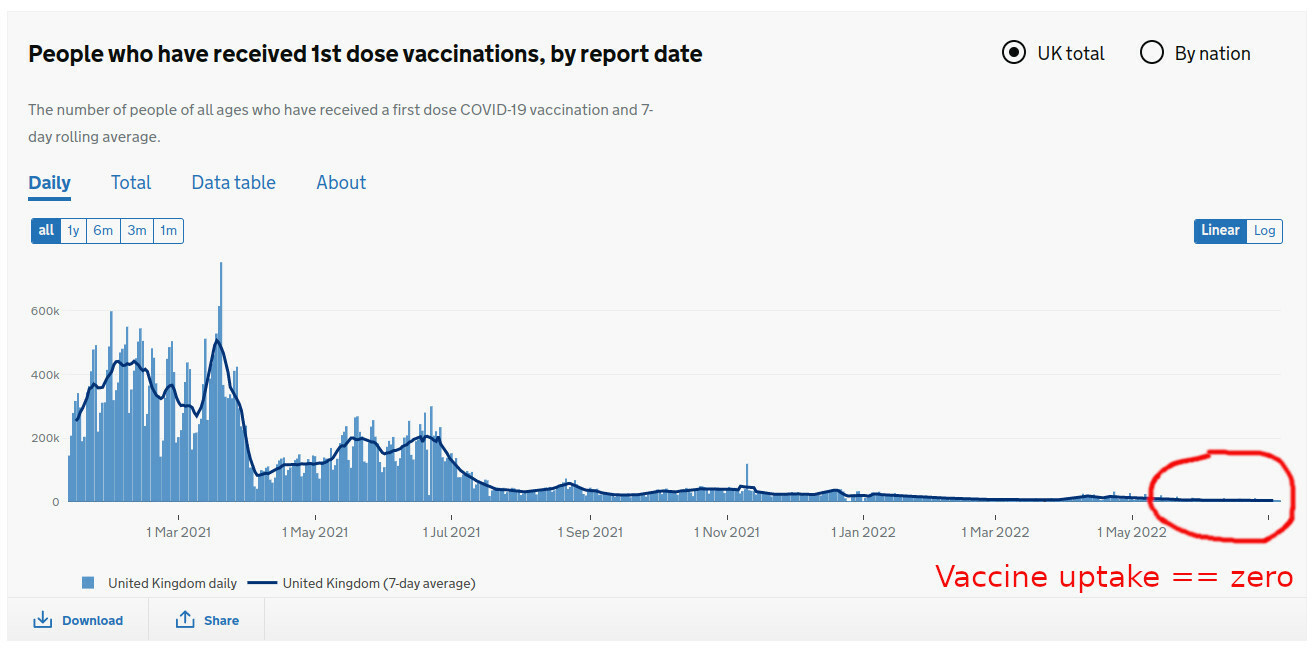
In recent months, COVID-19 vaccination in the U.S. has “
slowed to a crawl” as an increasingly distrustful public says “no thanks” to primary shots and boosters.
Still, U.S. public health agencies continue to authorize,
approve and recommend
COVID-19 vaccines —
even for infants.
On Tuesday, advisors to the Centers for Disease Control and Prevention (CDC) — perhaps believing they can reverse the slowdown in “vaccine uptake” and without admitting to the
ravages caused by the Pfizer/BioNTech, Moderna and Johnson & Johnson (J&J) shots —
unanimously recommended the “
Novavax COVID-19 Vaccine, Adjuvanted.”
The U.S. Food and Drug Administration (FDA) last week
granted Novavax Emergency Use Authorization (EUA) for its COVID-19 vaccine, for adults age 18 and up.
Back in 2020,
Operation Warp Speed awarded Novavax — another company that like Moderna,
never brought a product to market before COVID-19 — a
secret contract worth
$1.6 billion (now being reported as
$1.8 billion).
It was one of the largest taxpayer handouts channeled through Operation Warp Speed.
The media’s obliging sales pitch is that the Novavax injection is a “game changer” in comparison to the mRNA and adenovirus-vectored
gene therapy shots, and should be “reassuring to those who are hesitant.”
In fact, according to the CDC’s advisors, the
unvaccinated represent the “primary target population for Novavax.”
To further entice the unvaccinated, headlines feature the
misleading claim that Novavax’s EUA jab — featuring recombinant
moth-cell-based nanoparticle technology, the problematic surfactant
polysorbate 80 and a never-before-approved nanoparticulate
adjuvant called Matrix-M — is “free of side effects.”
However, the day after the FDA issued its Novavax authorization, the European Medicines Agency (EMA) made its own announcement, stating it was
updating its product information for the Novavax COVID-19 shot to disclose “new” side effects.
The EMA’s list of side effects included “severe allergic reaction [anaphylaxis] and unusual or decreased feeling in the skin” (called paresthesia and hypoesthesia, respectively).
In addition, the EMA said it is
assessing myocarditis and pericarditis as Novavax side effects — safety signals that also were on display in the FDA’s briefing
document.
And in clinical trials, older adults who received the Novavax vaccine experienced an increased incidence of
hypertension compared to those in the placebo group.
In short, as reported
last week and
last month by The Defender, the evidence contradicts Novavax’s downplaying of its vaccine’s association with heart problems and other side effects.
Apparently unaware of any potential cardiac risks, die-hards who have swallowed the slanted Novavax messaging blithely
suggested in online comments that they would take bizarre skin problems over the
heart problems they associate with other COVID-19 vaccines any day.
Adjuvants — ‘leave them out if you can’
Adjuvants, sometimes referred to as “the immunologist’s
dirty little secret,” are components of at least
80% of all vaccines. They are supposed to “stimulate and enhance the magnitude and durability of the
immune response.”
Additional adjuvant
actions include
modifying or broadening the immune response in certain age groups (such as infants and older adults) who tend not to respond to vaccines as strongly as vaccine makers would like, and increasing the body’s uptake of the vaccine antigen and protecting the antigen “from degradation and elimination.”
Less often admitted is the sordid association between adjuvants’ tenacious and “immunostimulatory” properties and
systemic adverse events — such as
neurotoxicity, “enigmatic”
autoimmune issues (dubbed “autoimmune/inflammatory syndrome induced by adjuvants” or “ASIA” by Israeli autoimmunity expert
Yehuda Shoenfeld),
narcolepsy,
infertility and other wild-card effects.
For these reasons,
Dr. Martin Friede — lead scientist at the World Health Organization’s (WHO) Initiative for Vaccine Research — candidly
remarked to other global vaccine insiders in late 2019, “We do not add adjuvants to vaccines because we want to do so” but out of perceived necessity.
Friede added:
“The first lesson is, while you’re making your vaccine, if you can avoid using an adjuvant, please do so. Lesson two is, if you’re going to use an adjuvant, use one that has a history of safety. And lesson three is, if you’re not going to do that, think very carefully.”
Undermining these seeming appeals to safety, Friede has since gone on to shill for
Pfizer’s COVID-19 shot and for
mRNA vaccine technology more broadly.
Nanoparticles times two
For many decades, aluminum-based adjuvants were the
only game in town.
However, with the burgeoning of
nanotechnology and encouragement from
sponsors like the National Institutes of Health, manufacturers shifted gears toward a new generation of “novel” nanotech adjuvants designed to not only amplify vaccine responses but also to serve as
carrier systems that distribute the vaccine’s payload to “key cells of the immune system.”
Generally left unmentioned in the hype surrounding these next-generation, nanoparticle-based adjuvants is the abundant evidence of
nanoparticle toxicity.
Well before COVID-19 vaccines came along, researchers warned about nanomaterials’ ability to “cross biological membranes and access cells, tissues and organs” — such as the brain, heart, liver, kidneys, spleen, bone marrow and nervous system — “that larger-sized particles normally cannot.”
They also cautioned that in the cells, “nanomaterials may be taken up by cell mitochondria and the cell nucleus,” with the potential for DNA mutation, structural damage to mitochondria and cell death.
Moreover, researchers identified extensive biotoxic impacts of nanoparticles on the
cardiovascular system, including “cardiac damage and dysfunction, vascular dysfunction, EC [epithelial cell] abnormities [sic], atherosclerosis, abnormal angiogenesis, platelet activation, blood coagulation and thrombosis.”
Nevertheless, in pre-COVID-19 studies of experimental vaccines containing Novavax’s Matrix-M, researchers waxed enthusiastic about the nanoparticle-based adjuvant’s “
significant” and “
potent” action — including its strong “
immunostimulatory properties” even without any accompanying antigen.
And, where nanoparticles are concerned, the Novavax COVID-19 shot actually delivers a
double whammy, combining Matrix-M with genetically engineered spike protein nanoparticles.
As Novavax
explains it (for some reason putting the word “adjuvant” in quotes), “The spike protein is the ‘signal,’ but … we want your immune system to hear that signal loud and clear [and] that signal boost comes from our Matrix-M ‘adjuvant.’”
Phospholipids and autoimmunity
Not unlike the
lipid nanoparticle “carrier systems” in the Pfizer and Moderna COVID-19 injections, the “immunostimulant” Matrix-M adjuvant includes two types of fat molecules — cholesterol and
phospholipids — bundled with detergent-like
saponins.
In human biology, phospholipids are essential for properly functioning cell membranes. But in the vaccine laboratory, synthetic versions are
viewed as “essential components of advanced vaccines.”
Unheeded by the pharmaceutical industry is the fact that
up to 5% of healthy individuals are estimated to harbor antiphospholipid antibodies, produced in a “mistaken” autoimmune response.
Researchers have linked the autoantibodies to the risk of
antiphospholipid syndrome (APS), an autoimmune disorder characterized by recurring blood clots as well as fetal loss, fetal growth retardation and other obstetric complications.
Although researchers claim to be baffled as to why some people develop APS, studies have noted the emergence of APS and
other autoimmune conditions following receipt of numerous vaccines, including those against
tetanus,
influenza,
human papillomavirus (HPV) — and now
COVID-19.
In a
study published in August 2021, the authors suggested that in people with preexisting antiphospholipid antibodies, both the mRNA and adenovirus-vectored COVID jabs — and presumably other types such as the Novavax injection — could plausibly function as “the straw that breaks the camel’s back,” triggering “aberrant activation of the coagulation pathway.”
Rheumatologists are also
reporting surges in blood clotting disorders, including APS.
Will the unvaccinated public take the bait?
In 2005, the EMA
mused that while new adjuvants often had trouble gaining approval due to safety concerns such as “acute toxicity and the possibility of delayed side effects … an increased level of toxicity may be acceptable if the benefit of the vaccine is substantial.”
In a 2017 study, investigators studying Matrix-M approvingly noted that “
rapid activation” of the immune system “is highly desirable in adjuvants used for emergency vaccination.”
With its authorization of Novavax’s souped-up COVID-19 jab, the FDA appears to have endorsed both of these views.
Outside the U.S., Novavax’s potent adjuvant also is being test-driven in children in the African nation of Burkina Faso, where
almost 1 in 10 of the unfortunate toddlers who received an experimental Matrix-M-containing malaria vaccine withdrew or were “lost to follow-up” before or just after the third dose.
Acknowledging only seven serious adverse events, the researchers concluded, “None … were attributed to the vaccine.”
Does Novavax even take its product seriously?
In a comment posted at Yahoo!Finance, a person who signed up for the Novavax clinical trials and then, after researching the untried company, decided to withdraw, noted the doctor running the trial
responded, “Oh sure, that’s fine. You want to wait and get one of the real vaccines.”
In another sign of Novavax’s lackadaisical corporate attitude, the labels on the COVID-19 vaccine vials will contain
no information about expiration dates, forcing healthcare providers into using an “online expiry date checker tool,” which CDC advisors acknowledge could be both burdensome and a source of “confusion.”
The Merriam-Webster dictionary
defines a “nova” as “a star that suddenly increases its light output tremendously and then fades away to its former obscurity in a few months or years.”
Will we say the same for “Nova”-vax’s shot in a few months’ or years’ time?








")