Here is an article that summarizes the video from Dr. Mercola's site:
Dr. Robert Malone returns for another interview regarding the mRNA technology behind the COVID-19 shots. Listen to our entire conversation for free here.

articles.mercola.com
(fair use applies)
mRNA Platform Inventor Sifts Through the Lies
Analysis by
Dr. Joseph Mercola
July 24, 2022
Story at-a-glance
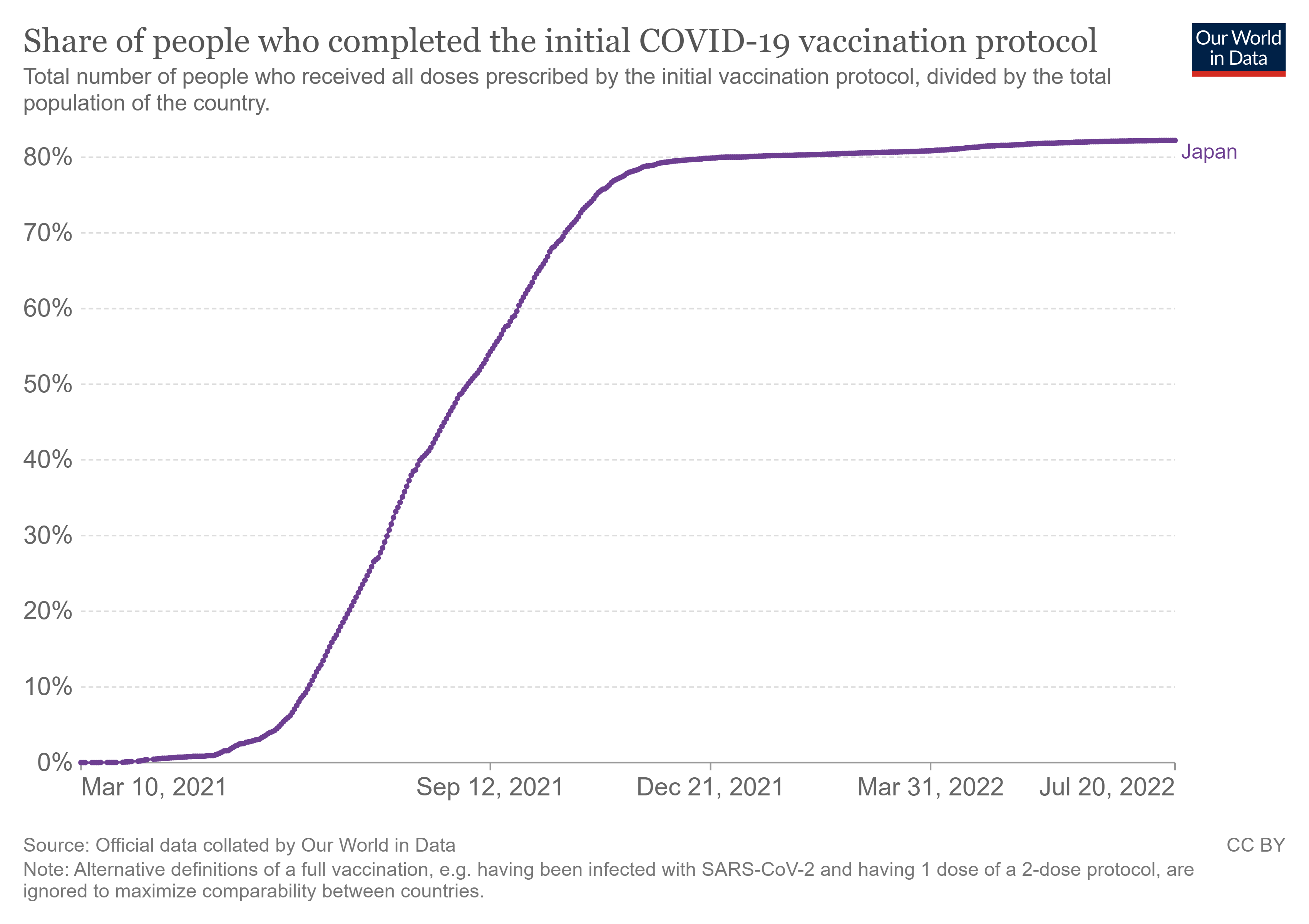
- Media and health authorities also ignore what Dr. Robert Malone and others have warned about from the start, which is that vaccinating during a pandemic will drive the evolution of resistant strains. This is precisely what we’re now seeing with Omicron variants BA.4 and BA.5, which circumvent both natural immunity and COVID jab-induced antibodies
- The CDC and the FDA are also ignoring the reality of immune imprinting, which is causing COVID-jabbed individuals to contract COVID more frequently, and repeatedly
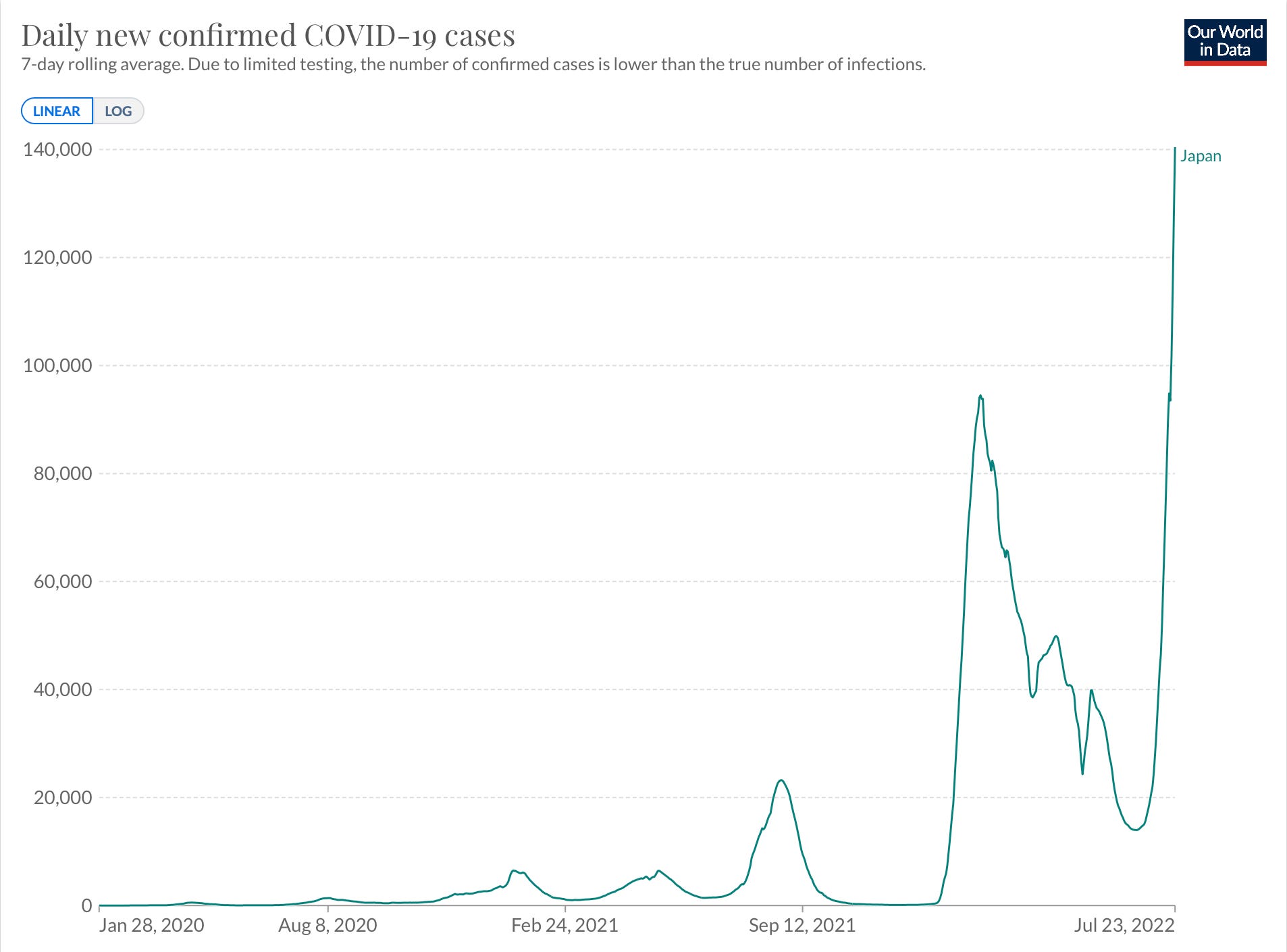
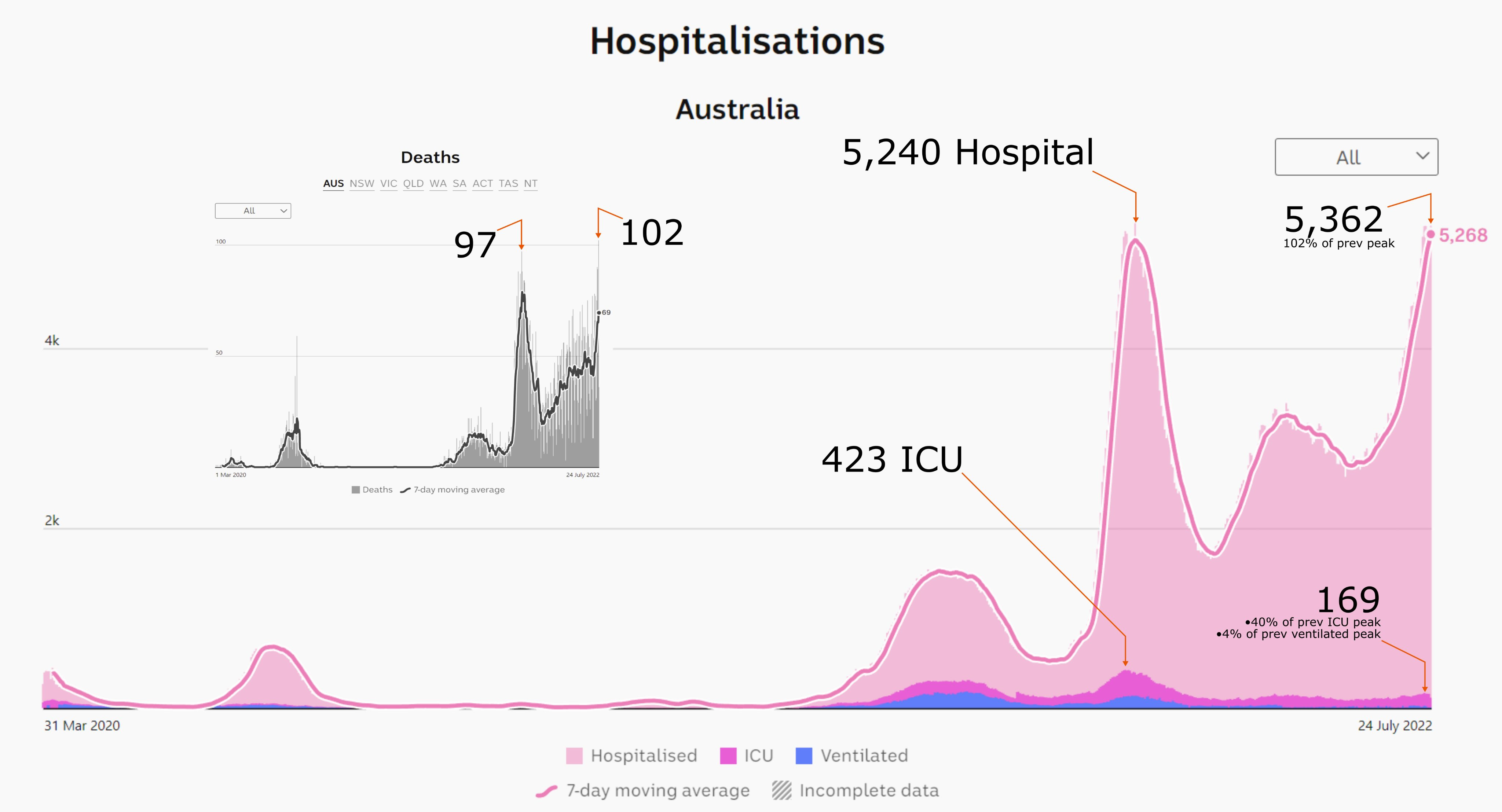
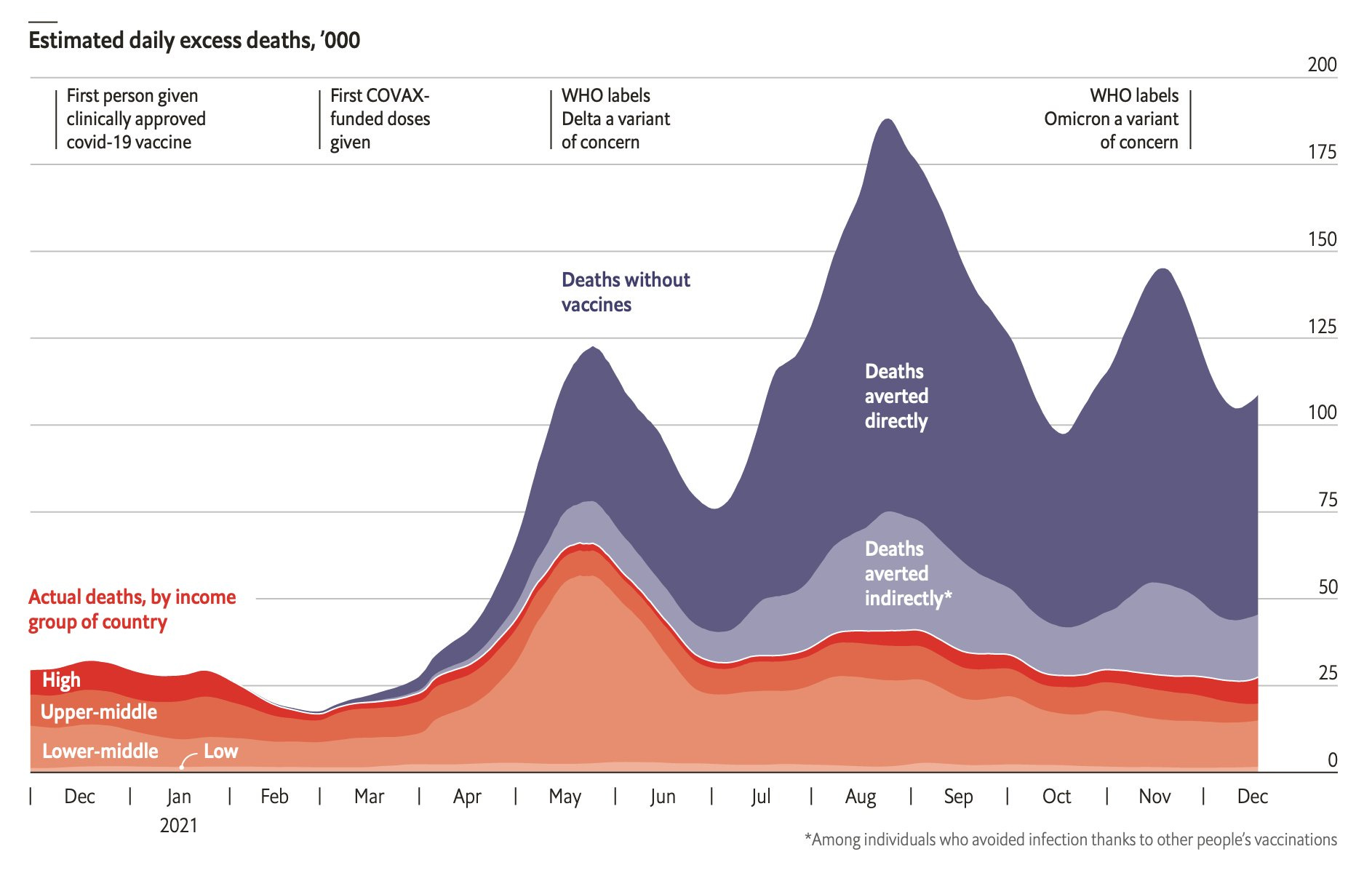
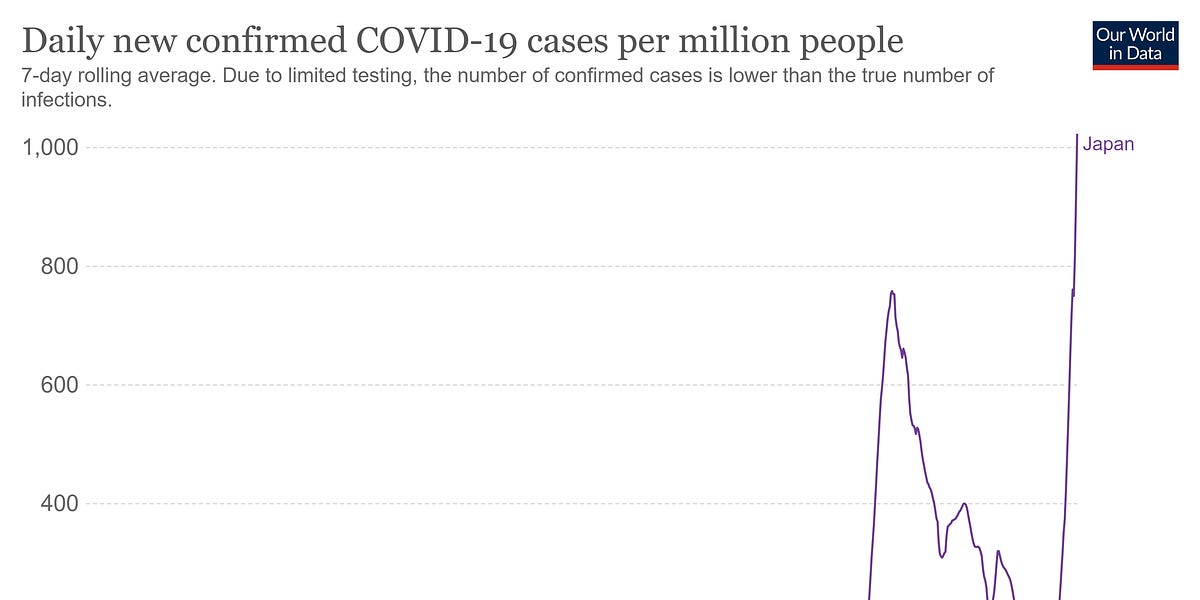
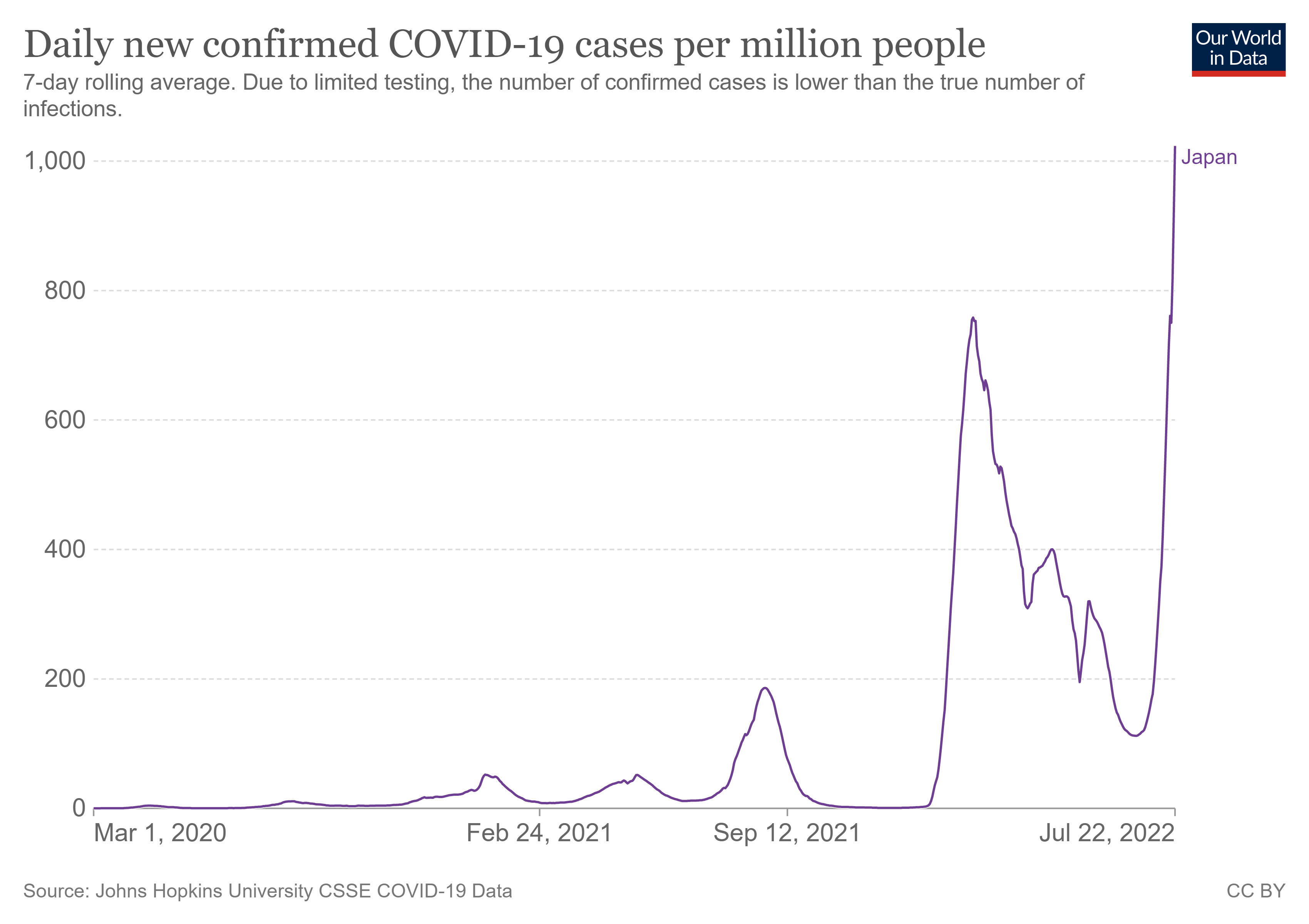
- Media are again trying to drum up fear over new COVID strains, despite data clearly showing hospitalization rates remain steady even though the infection rate is rising
- When RNAs include pseudouridine — as all mRNA COVID shots do — they will last longer and be less inflammatory. However, we’ve now discovered pseudouridine-containing RNA also causes immunosuppression, which we’re seeing in many who have received the jabs
- Malone’s book, “The Lies My Government Told Me” is now available
By now, many of you will be familiar with Dr. Robert Malone, inventor of the core mRNA and DNA vaccine platform technology1 that the various COVID shots are based upon. (To be clear, he’s not the inventor of the COVID shots themselves but rather the foundational platform that underlies them, for which Malone holds several patents.)
Malone rose to prominence after his appearance on the DarkHorse podcast2 in June 2021, where he, Steve Kirsch and DarkHorse host Bret Weinstein, Ph.D., spent three hours dissecting the COVID fraud. Interestingly, Malone and Kirsch were both double-jabbed before realizing there were problems with the shots, but once they did, they boldly stepped into the limelight to warn and inform others.
Malone also appeared on the Joe Rogan podcast3 December 30, 2021, which ended up being the most-viewed podcast of all time with some 50 million views. The transcript of that interview was even entered into the Congressional Record4 January 3, 2022, by Congressman Troy Nehls, R-Texas, after Twitter and YouTube removed it from their platforms.
Malone also helped promote the work of Dr. Matthias Desmet, a clinical psychologist at the University of Gantt in Belgium and author of
“The Psychology of Totalitarianism.” Desmet was the first to introduce the concept of “mass formation” to explain how and why people were going along with a narrative that was clearly false and evidently destructive.
Like so many others who have tried to share truth and opinions that differ from the official COVID narrative, myself included, Malone has been viciously attacked by media and relentlessly “fact checked.” Alas, with the passage of time, his wisdom and knowledge are now being validated on a near-daily basis.
“I would say we've been gaslighted, ridiculed, defamed — but I don't think we've been discredited,” he says. “I think we could both hold our heads up high. We've called it amazingly well.
I'm just in the middle of reviewing and building the chapters for the book that has to do with what's gone wrong with the HHS [Health and Human Services] and what we need to fix, which includes a litany of things that have been miscalled by the CDC [Centers for Disease Control and Prevention].
The list is enormous. And we continue to see on a daily basis the weaponization of fear porn, the two most recent examples being the monkeypox and the Omicron BA.4 [and] BA.5.”
Immune Imprinting Is Making the Vaxxed Sicker
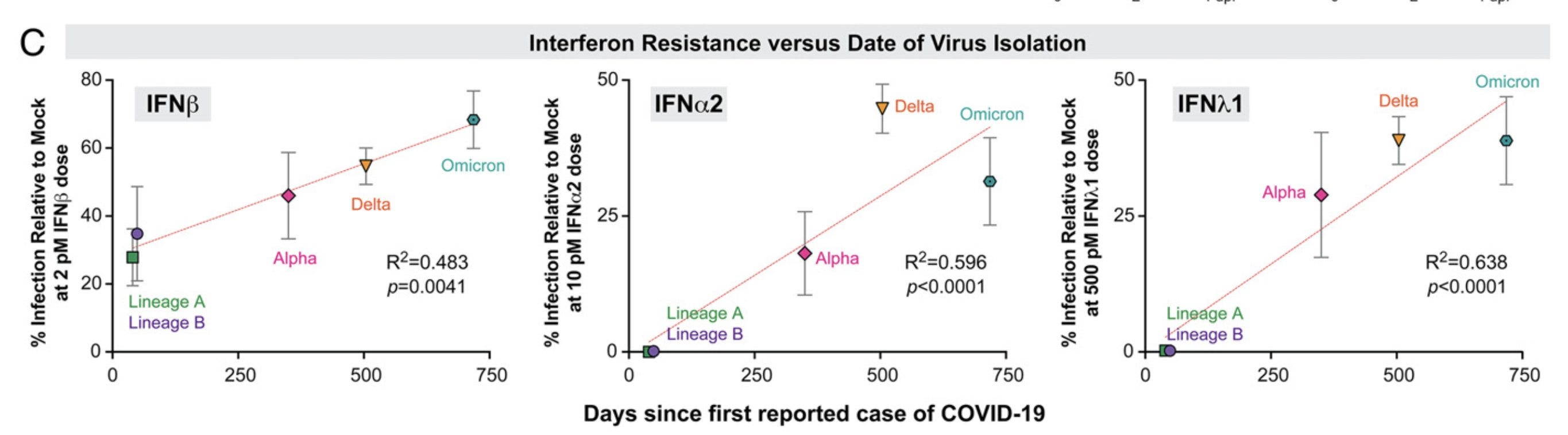
As noted by Malone, media are again trying to drum up fear porn, despite data clearly showing hospitalization rates remain steady even though the infection rate is rising. They’re also ignoring what Malone and others warned about from the start, which is that vaccinating during a pandemic is a beyond foolish strategy as it is virtually guaranteed to drive the evolution of resistant strains.
This is precisely what we’re now seeing with BA.4 and BA.5, which circumvent both natural immunity and COVID jab-induced antibodies. The CDC and the Food and Drug Administration are also ignoring the reality of immune imprinting, which Malone says is backed by more than 10 high-end, highly visible peer reviewed journals.
“We're literally driving the highly vaccinated to an immune compromised state in which they're more susceptible to infection by Omicron — as a consequence of their prior vaccination — and they are becoming chronically or multiply infected,” Malone says.
“This is precisely the situation that's been shown in peer reviewed literature to be driving the development of the further development of the escape mutants. So, our public policies are completely contrary to the need here. I'm speechless concerning the mismatch between what our government promotes and what the true public health need is.”
Is Malone Controlled Opposition?
In scanning through the comments on my newsletter, I’ve noticed that some people are convinced Malone is controlled opposition. Considering that he’s the developer of the mRNA technology that underlies the jabs, and the fact that he’s been double-jabbed himself, and has worked extensively with the Deep State intelligence community, Malone believes his current actions speak for themselves:
“I have historically worked with people who have been truly Deep State intelligence community. I have decades of experience in biodefense. I have been deep in the belly of the beast. I have won literally billions of dollars for my clients in grants and contracts. I have managed hundreds of millions of dollars in grants and contracts in the vaccine space.
[I’ve been] ... study section chair or key study section member on many hundred-plus million-dollar contract reviews, typically for the NIH [National Institutes of Health] ... but also DOD [Department of Defense]. I historically been deeply embedded in this whole enterprise. I know it upside down.
I understand this system. So, I think the concerns that I could be controlled opposition are valid. I think that it's appropriate to acknowledge the basis for those concerns. Now, [those] concerns, I think, are refuted by my behaviors and actions.
Let's start with the inventions. I have many patents. I've contributed to the development of many technologies. My wife and I helped found Inovia, the post electrical field gene delivery company that is promoting its own vaccine technology, which is a DNA-based platform and could well be adapted to RNA-based vaccines.
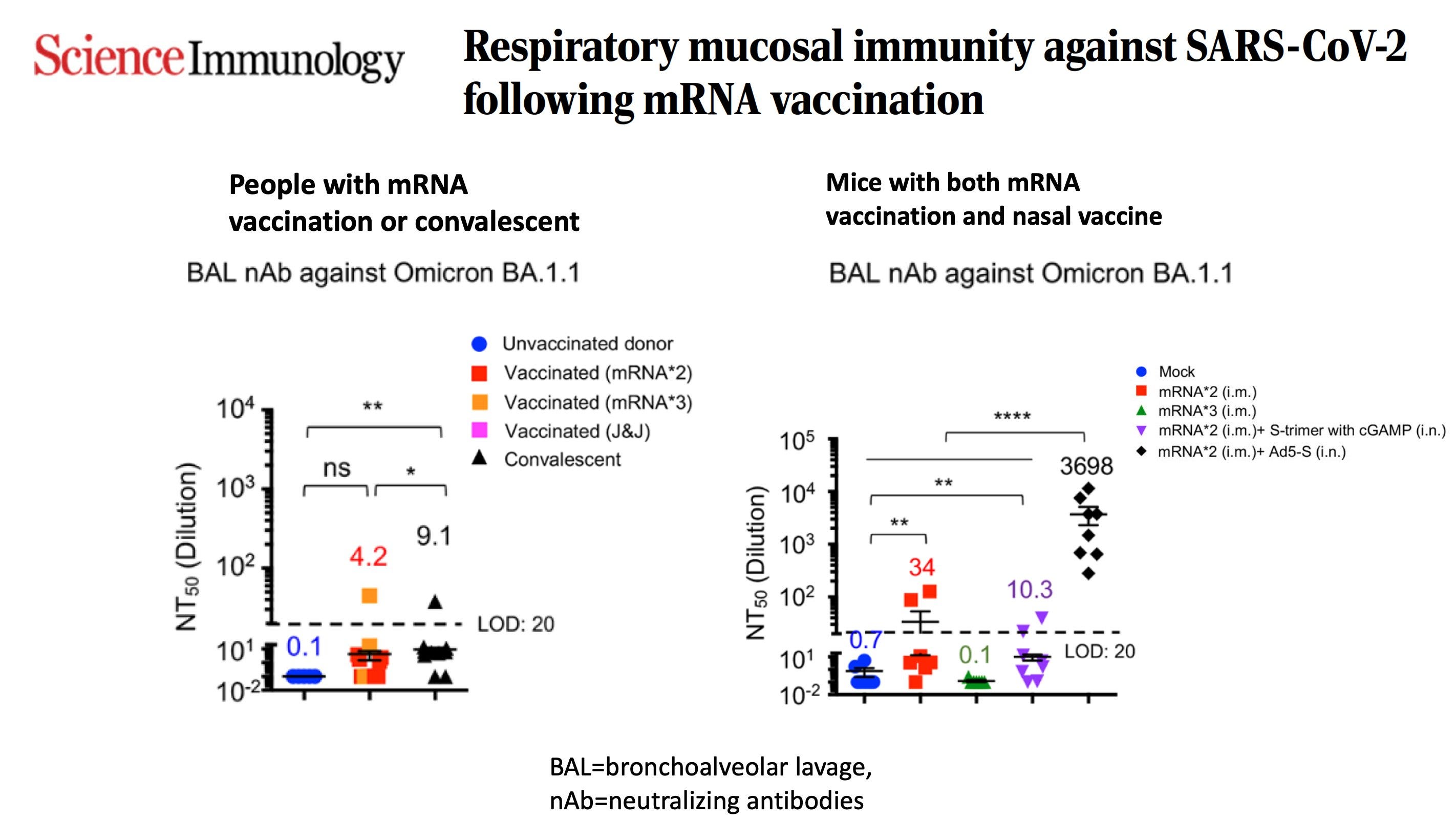
I certainly have those nine initial issued patents and others that relate to virtually any delivery system used to administer polynucleotides to the nasal pharynx, to mucosal tissues, to elicit a mucosal immune response ... I have many patents on various [nano] lipids, these positively charged fats that are used to deliver the polynucleotides, but I'm also an objective scientist.
As a consequence of the decades of experience in basic discovery research in this area, we've turned away from this technology because we could never overcome the inflammatory problems, this acute immune response and the recruitment of inflammatory cells into the injected tissues. We ran into this again and again and again, both in mice and then in monkeys, and could never overcome it. We abandoned the technology.”
Malone Explains the Patent Controversy
Malone goes on to explain the origin of the patent controversy — why some claim he didn’t actually invent the mRNA platform the COVID jabs are using, and why the technology was used at all if it had already been abandoned due to excessive hazards:
“Kati Karikó called me up in the mid-‘90s and wanted some advice. I told her about the problems with the RNA and the problems with the inflammatory response and, together with Drew Weissman, she applied the pseudouridine discoveries that were just emerging and put pseudouridine all the way through the RNA, which is both immunosuppressive and increases the half life of the RNA.
So, these RNAs that are now being used are really nothing like the natural RNA. They're synthetic product. The basis for their assertion that they're the true inventors and I am not — despite all the prior art and multiple patents — is that they made this improvement on the art that was enabling.
[However], the CureVac technology demonstrates that's not enabling, that, in fact, you can get good immune responses with mRNA that does not include pseudouridine. But I had turned away from the tech. There were better ways to provide an immune response, I believed. Those are still investigational.
Talking about eyes wide open, I have intimate understanding of the good, the bad and the ugly of this approach and this technology. That's always been my position — that of an objective scientist. Then, on the last point on this, I never received substantial revenue of any kind from my inventions.
The patents were filed from a company that's now called Vical that had partnered with Merck years ago. Over a billion dollars were spent to advance the technology. Merck and Vical only focused on the DNA and they failed.
But as a consequence of the terms of my employment, I received — in addition to my technician salary, which was about $20,000 a year — $1 for all those patents. I've had no patent royalty. So, I have no financial conflict of interest here. It doesn't matter to me one way or the other.
What matters is integrity and honesty and truthfulness ... Let me put it this way ... I was in a dark room, I backed into the light switch, and what I saw was such that I could never unsee it.”
On Malone’s CIA Connections
Malone was also, once upon a time, in business with a former CIA agent named Michael Callahan, who held a senior position in the Defense Threat Reduction Agency (DTRA). Callahan was in Wuhan, China, in the fourth quarter of 2019 and called Malone in early January 2020, asking him to get a team together to address a novel virus that had broken out in China.
“I had a series of interactions with him subsequently, until I became completely disillusioned and aware that he was lying to me almost constantly, including about things like whether or not the pathogen was engineered. So, I think I can certainly empathize, and understand why some might have these concerns ...
[But] I don't ask people to accept what I say, I ask people to think for themselves. I've tried to be truthful, honest, act with integrity, provide access to information, try to help people to think through things by themselves, and I've made a number of predictions and comments and analyses and, like you, I stand by what I've said.
So even if I was controlled opposition, that's kind of irrelevant. The question is not who I am; the question is what is the information? Is it useful to you? Is it helping you to manage your own affairs, make conformed choices about vaccinating your children? If so, I think that even if I was controlled opposition, I suspect that I'm fairly useful controlled opposition for those of us that are in this boat together of seeking truth ...
Frankly, all of my contacts with the government now are destroyed. The colleagues that I used to communicate with regularly at the FDA will no longer take my call ... I've dropped my contract with Defense Threat Reduction Agency.
Largely I just became disillusioned with them, particularly after I found out that another branch of DTRA is continuing to support the Wuhan Institute of Virology and disclose that.
I shared a number of fragments of information about what I know that's been going on within DTRA, as well as within NIAID [National Institutes of Allergy and Infectious Diseases] and the NIH. In doing so, I compromised that part of my career. I've thrown away, for the second time by the way, a big career path that I've developed over decades.”
Malone’s COVID Jab Experience
Malone also discusses his reasoning for taking the COVID shots. He needed to travel, and thought the shot might be helpful for his “long-COVID,” which he developed after contracting the infection early on in the pandemic.
Unfortunately, like so many others, he suffered a series of complications, particularly after the second dose, including cardiac damage resulting in hypertension with a frequent systolic pressure of up to 230, narcolepsy, central nervous brain fog, restless leg and several other symptoms now known to be associated with the shot.
When he later looked up his batch number on HowBadIsMyBatch.com,5 he discovered his second dose was from a batch associated with a high rate of complications. “So that's that. We all make mistakes. I acknowledge now [that taking the vaccine] was absolutely not the proper way to approach this,” he says.
Dr. Meryl Nass, who has since lost her medical license for the crime of talking about COVID treatments, was instrumental in actually curing Malone’s long-COVID. She prescribed ivermectin, which gave him near-immediate relief. “So, tip of the hat to Meryl Nass, a true truth warrior and another inspirational figure in all of this,” Malone says.
Pseudouridine-Enhanced RNA Can Cause Immunosuppression
In the interview, Malone delves into some of the mRNA jab quality control problems that have arisen, and whether or not the addition of pseudouridine actually reduces the inflammatory reaction associated with mRNA gene therapy as claimed.
As explained earlier, Karikó — a former Hungarian spy — had sought Malone’s help, and he told her about the problems with the RNA he was finding. Karikó and Weissman — a post-doc of Dr. Anthony Fauci — then went on to experiment with the addition of pseudouridine, which we now know influences things like RNA stability, folding, processing and splicing. It's highly regulated, but that wasn't known at the time.
What was known was that if RNAs include pseudouridine, they will last much longer and be far less inflammatory. Basically, immune responses against cells that have pseudouridine-modified mRNA in them are suppressed. On the basis of that, Karikó and Weissman incorporated pseudouridine throughout the entire mRNA molecule, which were synthesized using the methods Malone developed, and then purified.
When this product was injected, they got a better adaptive immune response and less inflammatory response. This is the science that the COVID shots are based on. However, recent investigations, using needle biopsies, have shown RNA persists in axillar lymph nodes for at least 60 days. They didn’t test any longer than that, so it could be far longer. The levels of spike protein produced was also found to be far higher than expected and lasted for at least 60 days.
“So, what we now know is that pseudouridinee can cause RNA to behave in ways that are absolutely not like natural RNA, as I had originally proposed,” Malone says. “The RNA is typically degraded within a couple of hours, so if people were to have adverse events, the inciting molecule would be gone and physicians could elect not to readminister it.
But in the current formulation with the pseudouridine incorporated throughout the entire backbone of the RNA, which is something that never happens in a natural situation, they do suppress the acute inflammatory response, but they also seem to suppress overall adaptive immune responses or immune function.
This may be something that's contributing to the immunosuppression that's observed after dosing with these products. That's unresolved, but there's no question that adverse event exists, that nonspecific immunosuppression.
So, we have now ... lots of evidence that the discovery of Karikó and Weissman had negative aspects to it, which were not well characterized by Pfizer, Moderna, BioNTech, et cetera.”
Malone also reviews other ingredients and quality control issues that can contribute to a “hot,” or more lethal batch, so to learn more, be sure to listen to the interview in its entirety. For example, he reviews the problem of aggregation, the toxicity of PEG, and how fatigue may be related to the fact that spike protein is not merely attached to cell surfaces but actually poison the mitochondria.
He also admits there may be some truth to claims that graphene oxide is being used, although he still hasn’t seen any conclusive proof. “Initially, I thought that was crazy talk, but the unwillingness of the pharmaceutical companies to disclose their ingredients, which is just mind boggling — that's completely contrary to anything I've ever encountered in any teaching I've ever had about regulated products — so, there's something amiss here. There's no question,” he says.
Upcoming Fall Trivalent Jab Will Likely Be More Dangerous
The FDA recently approved a new trivalent COVID jab for fall 2022, which won’t be going through any additional testing, even though it will be a brand-new composition to cover some of the newer strains. I fear this will radically increase side effects, as does Malone.
“The trivalent story goes back to the logic of influenza vaccines ... Reasoning by analogy, apparently, the FDA and the CDC have now concurred that a similar strategy shall be taken for these unlicensed experimental use authorized products that have produced an adverse event signal like no vaccine in history — which they deny — and are clearly not stopping infection replication and spread of the viruses.
What they've decided is they're going to now use the flu model, which will enable them to continue the manufacturing process, which, as we've just discussed, is poorly characterized, not really adequately provided with oversight, and [has poor] lot consistency.
We know from the ‘How Bad Is My Batch’ analysis, the lot consistency is horrid. But that's all apparently OK. And, one antigen is good so let's go to three. The problem is multifaceted.
Typically, when you do this, you maintain approximately the same dose of each antigen, so that would be, in the case of Pfizer, we're going to go from 50 to 150 micrograms of RNA in a jab. Let's hope they don't do that. But even if they only double the dose, then we know that the adverse events are going to go up considerably.”
[continued next post]

 apnews.com
apnews.com











")