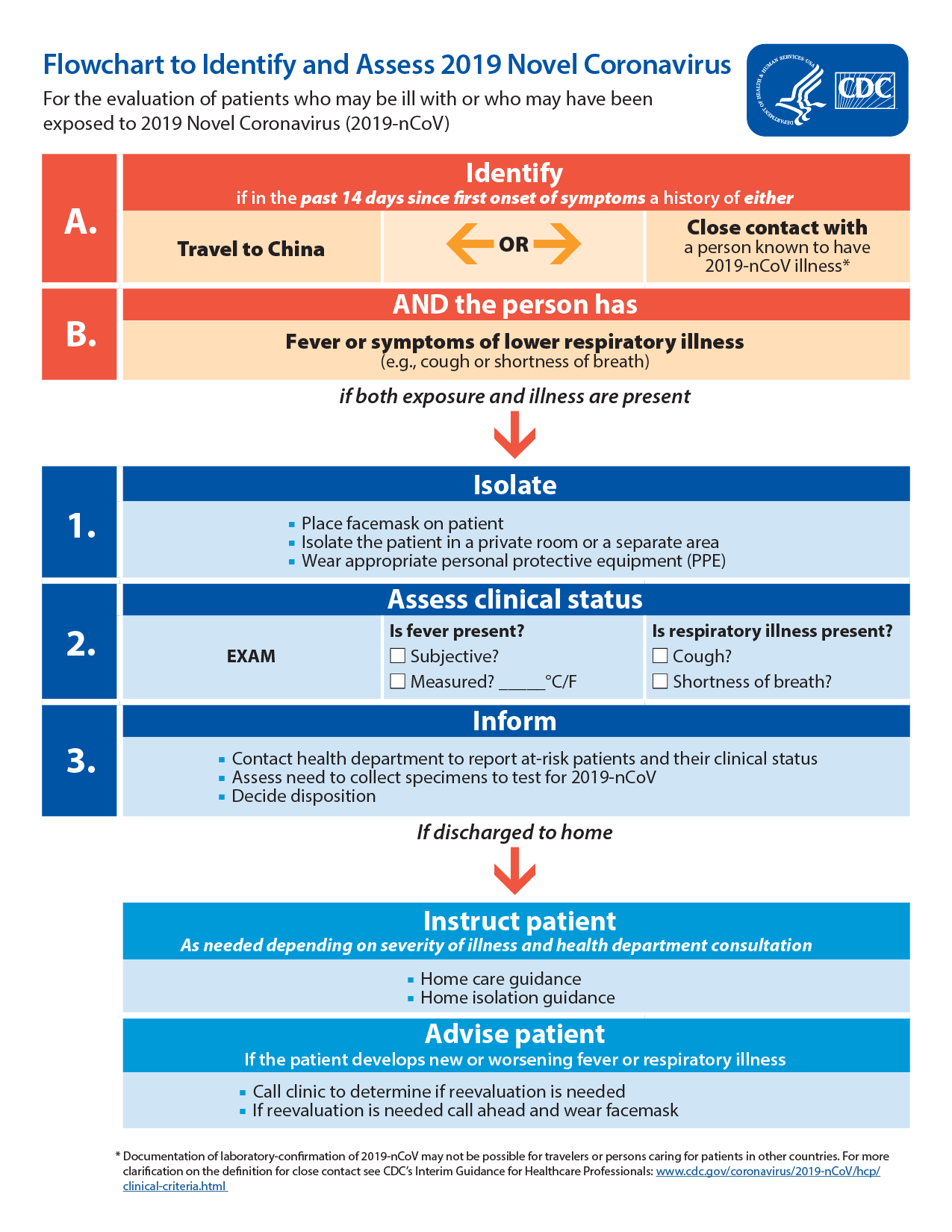
ICU Doctor in Wuhan describe his experience
Thank you Michael Lipman for this link from Chinese news site Caixin
Feb 06, 2020 07:40 AM
Reporter’s Notebook: Life and Death in a Wuhan Coronavirus ICU
By
Xiao Hui
A front-line coronavirus doctor tells of life in death in the ICU. Photo: Xiao Hui/Caixin
(Wuhan)–In the coronavirus epidemic, doctors on the front lines take on the greatest risk and best understand the situation. Peng Zhiyong, director of acute medicine at the Wuhan University South Central Hospital, is one of those doctors.
In an interview Tuesday with Caixin, Peng described his personal experiences in first encountering the disease in early January and quickly grasping its virulent potential and the need for stringent quarantine measures.
As the contagion spread and flooded his ICU, the doctor observed that
three weeks seemed to determine the difference between life and death. Patients with stronger immune systems would start to recover in a couple of weeks, but in the second week some cases would take a turn for the worse.
In the third week, keeping some of these acute patients alive might require extraordinary intervention [such as ventilator support and ECMO]. For this group, the death rate seems to be 4% -5%.
The doctors and nurses at his hospital are
overwhelmed with patients. Once they don
protective hazmat suits, they go without food, drink and bathroom breaks for their entire shifts. That’s because there’s aren’t enough of the suits for a mid-shift change, he said.
Over the past month on the front lines of the coronavirus battle, Peng has been brought to tears many times when
forced to turn away patients for lack of staffing and beds.
Screening criteria were too tough in the beginning
Caixin: When did you encounter your first novel coronavirus patient?
Peng Zhiyong: Jan. 6, 2020. There was a patient from Huanggang who had been refused by multiple hospitals, who was sent to the South Central Hospital emergency room. I attended the consultation. At the time, the patient’s illness was already severe, and he had difficulty breathing. I knew right then that he contracted this disease. We debated at length whether to accept the patient. If we didn’t, he had nowhere to go; if we did, there was a high likelihood the disease would infect others. We had to do a very stringent quarantine. We decided to take the patient in the end.
I called the hospital director and told him the story, including the fact that we had to clear the hospital room of other patients and to remodel it after SARS standards by setting up a “contamination area,” “buffer area,” “cleaning area,” and separate the living areas of the hospital staff from the patients’.
On Jan. 6, with the patient in the emergency room,
we did quarantine remodeling in the emergency room and did major renovations to the ICU (intensive care unit). South Central Hospital’s ICU has 66 beds in total. We kept a space dedicated to coronavirus patients. I knew the infectiousness of the disease. There were bound to be more people coming in, so
we set aside 16 beds. We did quarantine renovations on the infectious diseases area because respiratory illnesses are transmitted through the air, so even air has to be quarantined so that inside the rooms the air can’t escape.
At the time, some said that the ICU had a limited number of beds and 16 was excessive. I said it wasn’t excessive at all.
Caixin: You predicted back in January that there would be person-to-person transmission and even took quarantine measures. Did you report the situation to higher-ups?
Peng: This disease really did spread very fast.
By Jan. 10, the 16 beds in our ICU were full. We saw how dire the situation was and told the hospital’s leadership that they had to report even higher. Our head felt it was urgent too and reported this to the Wuhan city health committee. On Jan. 12, the department sent a team of three specialists to South Central to investigate. The specialists said that clinical symptoms really resembled SARS, but they were still talking about diagnosis criteria, that kind of stuff. We replied that those standards were too stringent. Very few people would get diagnosed based on those criteria. The head of our hospital told them this multiple times during this period. I know other hospitals were doing the same.
Before this, the specialists already went to Jinyintan Hospital to investigate and made a set of diagnosis criteria. You had to have had exposure to the South China Seafood Market, you needed to have had a fever and test positive for the virus. You had to meet all three criteria in order to be diagnosed. The third one was especially stringent. In reality,
very few people were able to test for a virus.
On Jan. 18, the high-level specialists from the National Health Commission came to Wuhan, to South Central Hospital to inspect. I told them again that the criteria were too high. This way it was easy to miss infections. I told them this was infectious; if you made the criteria too high and let patients go, you’re putting society in danger. After the second national team of specialists came, the criteria were changed. The number of diagnosed patients rose quickly.
Caixin: What made you believe that the new coronavirus could be transmitted between people?Peng: Based on my clinical experience and knowledge, I believed that the disease would be an acutely infectious disease and that we had to do high-level protection. The virus isn’t going to change based on man’s will. I felt we needed to respect it and act according to science. Under my requirements, South Central Hospital’s ICU took strict quarantine measures, and as a result, our department only had two infections. As of Jan. 28, of the entire hospital’s medical personnel, only 40 have been infected. This is way less compared with other hospitals in terms of percentage of total medical staff.
It pains us to see the coronavirus develop to such a desperate state. But the priority now is to treat people; do everything we can to save people.
Fatality rate for acute patients is 4%-5%; 3 weeks determine life and death
Caixin: Based on your clinical experience, what’s the disease progression of the new coronavirus?
Peng: A lot of viruses will die off on their own after a certain amount of time. We call these self-limited diseases. I’ve observed that the
breakout period of the novel coronavirus tends to be three weeks, from the onset of symptoms to developing
difficulties breathing.
Basically going from mild to severe symptoms takes about a week. There are all sorts of mild symptoms: feebleness, shortness of breath, some people have fevers, some don’t. Based on studies of our 138 cases, the most common symptoms in the first stage are fever (98.6% of cases), feebleness (69.6%), cough (59.4%), muscle pains (34.8%), difficulties breathing (31.2%), while less common symptoms include headaches, dizziness, stomach pain, diarrhea, nausea, vomiting.
But some patients who enter the second week will suddenly get worse. At this stage, people should go to the hospital. Elderly with underlying conditions may develop complications; some may need machine-assisted respiration. When the body’s other organs start to fail, that’s when it becomes severe, while those with strong immune systems see their symptoms decrease in severity at this stage and gradually recover.
So the second week is what determines whether the illness becomes critical.
The third week determines whether critical illness leads to death. Some in critical condition who receive treatment can
raise their lymphocyte [count], a type of white blood cell, and see an improvement in their immune systems, and have been brought back, so to speak. But
those whose lymphocyte numbers continue to decline, those whose immune systems are destroyed in the end, experience multiple organ failure and die. [Summary: Prolonged low lymphocyte counts in the 3rd week of illness predict death.]
For most, the illness is over in two weeks, whereas for those for whom the illness becomes severe, if they can survive three weeks they’re good. Those that can’t will die in three weeks.
Caixin: Will you please give more details on clinical research? What percentage of cases would develop from mild conditions to severe conditions? What percentage of serious cases would develop into life-threatening cases? What is the mortality rate?Peng: Based on my clinical observations, this
disease is highly contagious, but the
mortality rate is low. Those that progressed into the life-threatening stage often occurred in the
elderly already with
chronic diseases.
As of Jan. 28, of 138 cases, 36 were in the ICU, 28 recovered, five died. That is to say, the mortality rate of patients with severe conditions was 3.6%. Yesterday (Feb. 3), another patient died, bringing the mortality rate to 4.3%. Given patients in the ICU, it is likely to have more deaths. The mortality rate is also likely to edge up but not significantly.
Those hospitalized tend to have severe or life-threatening conditions.
Patients with slight symptoms are placed in quarantine at home. We have not gathered data on the percentage of cases that progress from slight symptoms to serious symptoms. If a patient goes from serious conditions to life-threatening conditions, the patient will be sent to the ICU. Among 138 patients, 36 were transferred to the ICU, representing 26% of all patients. The percentage of deaths among life-threatening cases is about 15%. The mean period to go from slight conditions to life-threatening conditions is about 10 days. Twenty-eight patients recovered and were discharged. Right now, the recovery rate is 20.3% while other patients remain hospitalized.
It is notable that 12 cases were linked to South China Seafood Market; 57 were infected while being hospitalized, including 17 patients already hospitalized in other departments; and 40 medical staff, among 138 cases (as of Jan. 28). That demonstrates that a hospital is a high-risk zone and appropriate protection must be taken.
Caixin: What is the highest risk a serious patient faces?
Peng: The biggest assault the virus launches is on a patient’s immune system. It causes a fall in the count of lymphocytes, the damage in the lungs and shortness of breath. Many serious patients died of choking. Others died of the failure of multiple organs following complications in their organs resulting from a collapse of the immune system.
Caixin: [Some patients did not appear too sick] but they died suddenly. Some experts argue that the virus triggers a cytokine storm, which ravages the stronger immune system of young adults. Eventually excessive inflammations caused by cytokine result in the higher mortality rate. …
Peng: Based on my observations,
a third of patients exhibited inflammation in their whole body. It was not necessarily limited to young adults. The mechanism of
a cytokine storm is about whole-body inflammation, which leads to a failure of multiple organs and quickly evolves into the terminal stage. In some fast-progressing cases, it took two to three days to progress from whole-body inflammation to the life-threatening stage.
Caixin: How do you treat serious and life-threatening cases?
Peng: For serious and life-threatening cases, our main approach is to
provide oxygen, high-volume oxygen. At first noninvasive machine-pumped oxygen, followed by
intubated [with a ventilator] oxygen if conditions worsen. For life-threatening cases, we use
ECMO (extracorporeal membrane oxygenation, or pumping the patient’s blood through an artificial lung machine). In four cases, we applied ECMO to rescue patients from the verge of death.
Currently there are no special drugs for the coronavirus. The primary purpose of the ICU is to help patients sustain the functions of their body. Different patients have different symptoms. In case of shortness of breath, we provided oxygen; in case of a kidney failure, we gave dialysis; in case of a coma, we deployed ECMO. We provide support wherever a patient needs it to sustain their life.
Once the count of lymphocytes goes up and the immune system improves, the virus will be cleared. However,
if the count of lymphocytes continues to fall, it is dangerous because the virus continues to replicate. Once a patient’s immune system is demolished, it is hard to save a patient.
[Very important negative prognostic sign: failure of the low lymphocyte count to recover.]
Caixin: There is news of some drugs that work. People are hopeful of the effect of U.S.-made remdesivir, which cured the first case in the United States. What do you think of the drugs?
Peng: There are not 2019 novel coronavirus-targeted drugs so far. Some patients may recover after taking some drugs along with supportive treatment. But such individual cases do not indicate the universal effect of the drugs. The effect is also related to how serious each case is and their individual health conditions. People want a cure urgently, and that is understandable. But we need to be cautious.
Caixin: Do you have any advice for coronavirus-infected patients?
Peng: The most effective approach to the virus epidemic is to control the source of the virus, stem the spread of the virus and prevent human-to-human transmission. My advice for a patient is going to a special ward for infectious diseases, early detection, early diagnosis, early quarantine and early treatment. Once it has developed into a severe case, hospitalization is a must. It is better to contain the disease at an early stage. Once it reaches the life-threatening stage, it is way more difficult to treat it and requires more medical resources. With regard to life-threatening cases, try to save them with ICU measures to reduce the mortality rate…..
Caixin: What are your work load and pace like?
Peng: The work in the ICU is overloaded. There are three patient wards with 66 beds in South Central Hospital, housing 150 patients. Since Jan. 7 when we received the first patient, no one took any leave. We took turns to work in the ICU. Even pregnant medical staff did not take leave.
After the epidemic got worse, none of the medical staff ever went home. We rest in a hotel near the hospital or in the hospital. [The medical staff working in the ward would be considered “under quarantine” after their shifts and could not go home.
In the segregated ward, we wear
level-3 protective gear. One shift is
12 hours for a doctor and
eight hours for a nurse. Since protective gear is in a shortage, there is
only one set for a medical staff member a day. We refrain from eating or drinking during our shift because the gear is no longer protective once we go to the washroom. The gear is thick, airtight and tough on our body. It felt uncomfortable at the beginning, but we are used to it now.
Caixin: Did you experience a very dangerous moment? For example, in case of intubation, what do you do to prevent yourselves from being infected?
Peng: It is a new coronavirus. We are not sure of its nature and its path of spread. It is not true if we say we are not afraid. Medical staff members do fear to some extent. But patients need us. When a patient is out of breath and noninvasive oxygen provision fails, we must apply intubation.
The procedure is dangerous as the patient may vomit or spit. Medical staff are likely to be exposed to the danger of infection. We strictly require doctors and nurses to apply the highest-level protection. The biggest problem we face now is the shortage of protective gear. The protective stock for ICU staff is running low, although the hospital prioritizes the supply to us.
Caixin: Is there anything that moved you in particular? Did you cry?Peng: I often cried because so many patients could not be admitted to the hospital. They wailed in front of the hospital. Some patients even knelt down to beg me to accept him into the hospital. But there was nothing I could do since all beds were occupied. I shed tears while I turned them down. I ran out of tears now. …..
The deputy director of our department told me one thing, and he cried too. Wuhan 7th Hospital is in a partnership with our hospital, South Central Hospital. The deputy director went there to help in their ICU.
He found that two-thirds of the medical staff in the ICU were already infected. Doctors there were running “naked” as they knew they were set to be infected given the shortage of protective gear. They still worked there nonetheless. That was why ICU medical staff were almost all sickened. It is too tough for our doctors and nurses.



 pdf icon
pdf icon






















") , nitrile gloves in stock. I placed an order this morning and received the tracking# and notice that it ships today. See the link below.
, nitrile gloves in stock. I placed an order this morning and received the tracking# and notice that it ships today. See the link below.

