On June 28, the FDA decided that henceforth THEY will choose the variants for reformulated Covid-19 shots and NO clinical trials will be conducted to evaluate safety. Because $cience.

tobyrogers.substack.com
(fair use applies)
The end of Covid-19 vaccine safety science in America
On June 28, the FDA decided that henceforth THEY will choose the variants for reformulated Covid-19 shots and NO clinical trials will be conducted to evaluate safety. Because $cience.
Toby Rogers
7 hr ago
I. The end of the beginning
Yesterday, the FDA’s Vaccines and Related Biological Products Advisory Committee approved a bivalent Covid-19 shot with the Wuhan strain and the Omicron variant.
The vote was:
19 yes.
2 no.
A few thoughts:
The Wuhan strain is no longer in circulation. So they are vaccinating against a strain that no longer exists.
The Omicron variant that they are going to put into this shot is Omicron BA.4/BA.5:
1. By the time it gets to market in the fall, Omicron BA.4/BA.5 will likely no longer be in circulation.
2. There is no efficacy data whatsoever on vaccines against Omicron BA.4/5.
3. There is no safety data whatsoever on vaccines against Omicron BA.4/5.
4. They do not intend to gather any efficacy or safety data between now and when these shots will be released in the fall:
At the meeting, the manufacturers (Moderna, Pfizer, and Novavax) were asked what their production timelines are… and they said
out loud, “So long as we don’t have to provide any clinical data, we’ll have them ready by fall.”
No one had a problem with that.
Ofer Levy said that he was concerned about the lack of safety data (there is none) and asked if the FDA intended to gather any. FDA vaccine head Peter Marks said that he was “comfortable” that the Sentinel BEST Initiative would catch any safety signals
after these shots are introduced into the market. No one has ever heard of Sentinel BEST. Meanwhile Dr. Marks disparaged the Vaccine Adverse Events Reporting System (VAERS) that has shown
29,031 reports of death following Covid-19 shots.
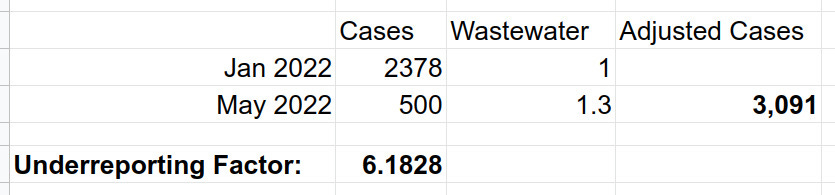
So the FDA is going to introduce reformulated shots into the population this autumn with no safety data and then try to spot adverse events in the population after the fact using a safety system no one has ever heard of — while ignoring the system that has existed for 32 years that is showing a
massive safety signal right now.
We are the experiment. But it’s not even really an experiment because they do not care about the data. We are the people they want to democide.
The FDA’s Actions yesterday were a violation of the
Nuremberg Code, the
Declaration of Helsinki, and the
Hippocratic Oath.
The FDA has plunged the United States into a pre-scientific dark ages.
II. Wait, hold up, I thought the FDA was voting on the Future Framework yesterday?
The policy question was whether reformulated Covid-19 shots would be treated as new molecular entities (which they are) in which case they should be subject to formal review or whether reformulated shots would be treated as “biologically similar” to existing Covid-19 shots and be allowed to skip clinical trials altogether.
Apparently the FDA did not have the votes to just pass this as a policy question. If you ask anyone whether reformulated mRNA represents a new molecular entity, well of course it is, so that would require formal regulatory review.
What the FDA did instead was to smuggle the policy question in disguised as a vote about reformulated “boosters” for the fall. In essence, the FDA just started
doing the Future Framework (picking variants willy nilly, skipping clinical trials) and essentially dared the committee members to turn down a booster dose — knowing that all of the VRBPAC members are hand-picked because they’ve never met a vaccine they did not like. So of course only two people on the committee had the courage to turn down a booster dose — even though it was based on this preposterous process (that was never formally adopted) where there was literally no data at all.
Paul Offit even said prior to the vote, “This is a new product… we need a higher standard of protection.” Offit was one of two VBBPAC members who voted no (the other was Hank Bernstein).
By stealth, the FDA replaced a system based on evidence with a system based entirely on belief.
III. The meeting itself
The meeting was chaos. You can watch the whole thing (
here) — in general, the discussion starting at
6:33:23 is where you will find the most damning quotes.
The guy they brought into to model the future of the pandemic,
Justin Lessler, who
by my count has TWENTY conflicts of interest, presented slide after slide with confidence intervals so wide, the prediction was literally ‘anything can happen.’
Hats off to this grifter for stealing millions of dollars from Bill Gates and Tony Fauci and producing nothing in return.
At one point, Wayne Marasco at Harvard suggested abandoning mRNA shots altogether (yes, good idea) and switching to the Novavax platform because he liked the CEO’s presentation. Then Peter Marks came in and slapped that idea down (Novavax does not have an approved EUA in part because they are now on their third contract manufacturer and their last manufacturer, Emergent BioSolutions, contaminated 400 million Covid-19 vaccine doses).
At the end of the meeting, the chair, 89-year-old Arnold Monto, did not even know what strains were in the proposed fantasy bivalent shot — he thought it included beta but literally no one was proposing that yesterday. Of course Dr. Monto voted yes anyway. Like many members of the committee his attitude is ‘shoot ‘em all up and let God sort ‘em out.’
Dr. Monto did not look well, so I imagine there is a better than zero chance that he just voted for the product that will end his life.
Late stage capitalism is wild.
The representative from the World Heath Organization proposed a monovalent Omicron (BA.1) booster but the committee blew right on by that idea to the latest and greatest variant (BA.4/5) — even though no one knows how to target that.
In the weeks leading up to the meeting, Moderna and Pfizer already started making bivalent Covid-19 shots with Wuhan and Omicron BA.1 variants. But the committee blew right on by that idea as well. Not to worry, at the end of the meeting Peter Marks assured them that the federal government would “make them whole” — i.e. pay Moderna and Pfizer, with our tax dollars, for shots that no one even asked for.
The committee spent a fair amount of time discussing a slide from Pfizer showing antibody response — and apparently no one other than me bothered to look at the note in the bottom left hand corner that read “N = 8 Balb/c mice.” Quite literally, this “immunogenicity data” was based on 8 mice specifically bred to be “
exceptional responders to immunization.” That’s how miserable the data were.
Most of the presentations at this meeting were so flawed they would have failed a high school biology class.
FDA, VRBPAC, and the WHO admitted that they have no correlates of protection.
VRBPAC member Bruce Gellin (the new guy) admitted that the flu vaccine is not a good comparator for Covid-19 vaccines.
They all admitted that they have no safety data.
And then they approved this reformulated fantasy shot by a vote of 19 to 2 because they are incapable of critical thinking.
IV. What does this all mean?
Peter Marks and the members of VRBPAC think that they achieved a great victory. Indeed the vote Tuesday was the last piece of their Final Solution for Amerika — shots approved for all ages — with no clinical trials ever again.
The reality is that FDA/VRBPAC and CDC/ACIP with their reckless votes across 8 meetings during the month of June, guaranteed the collapse in our lifetime of these regulatory agencies, allopathic medicine, and the vaccine program.
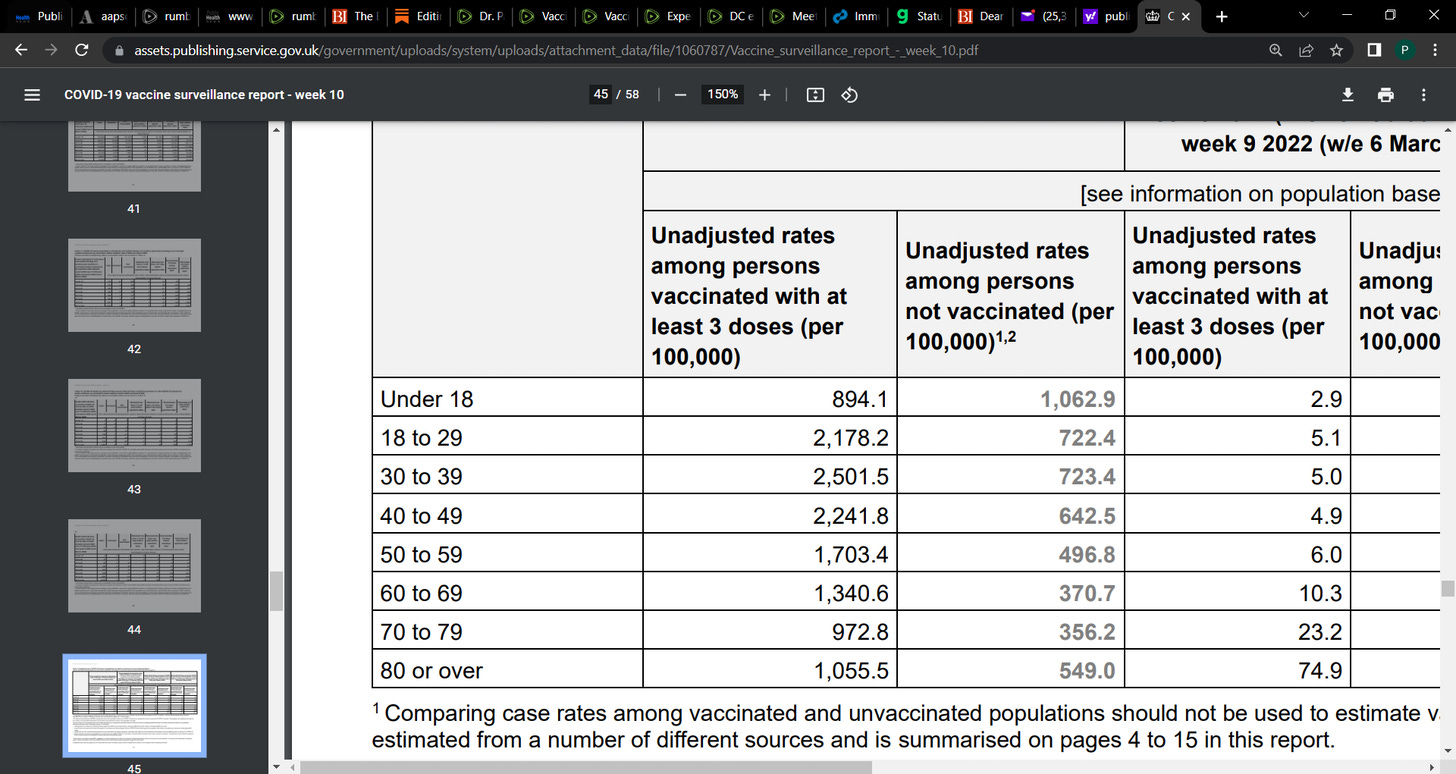
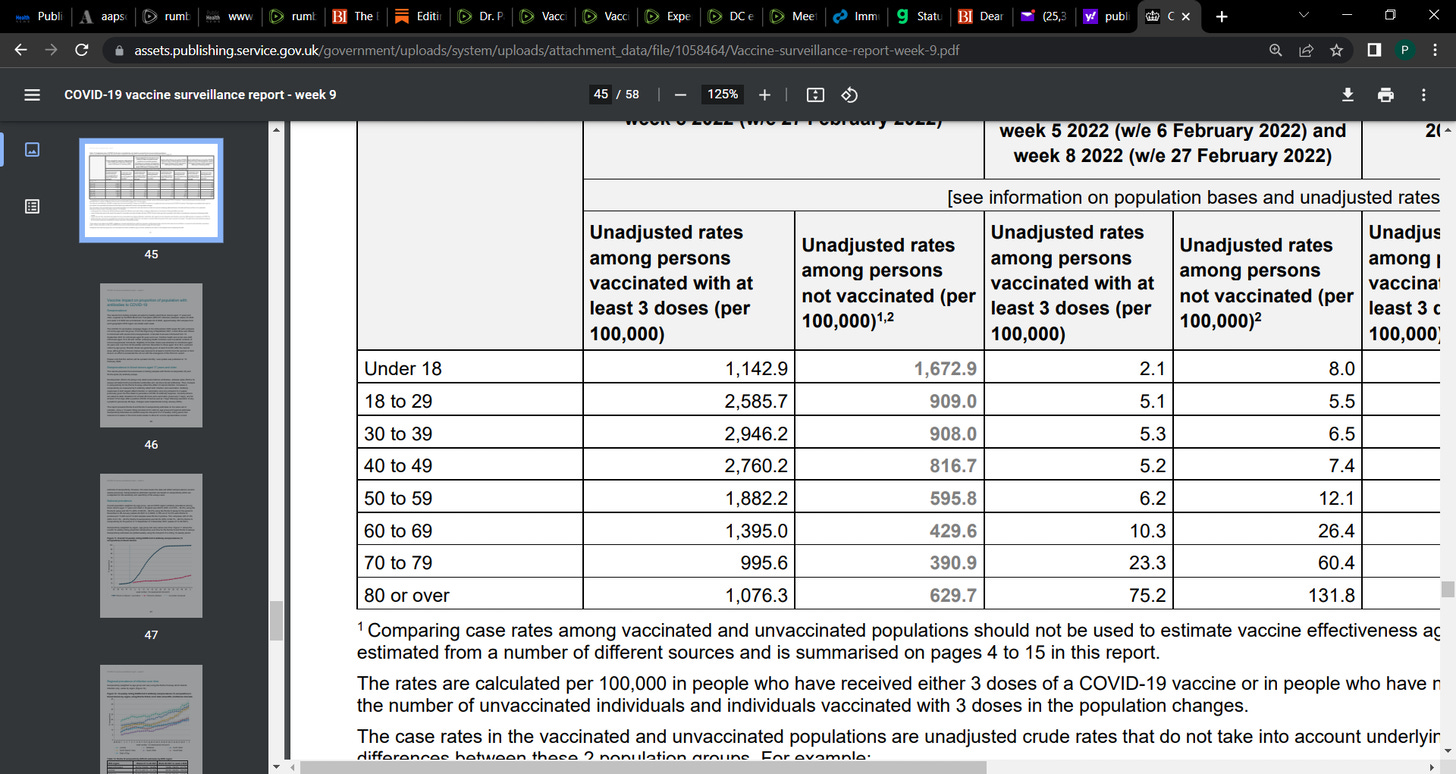
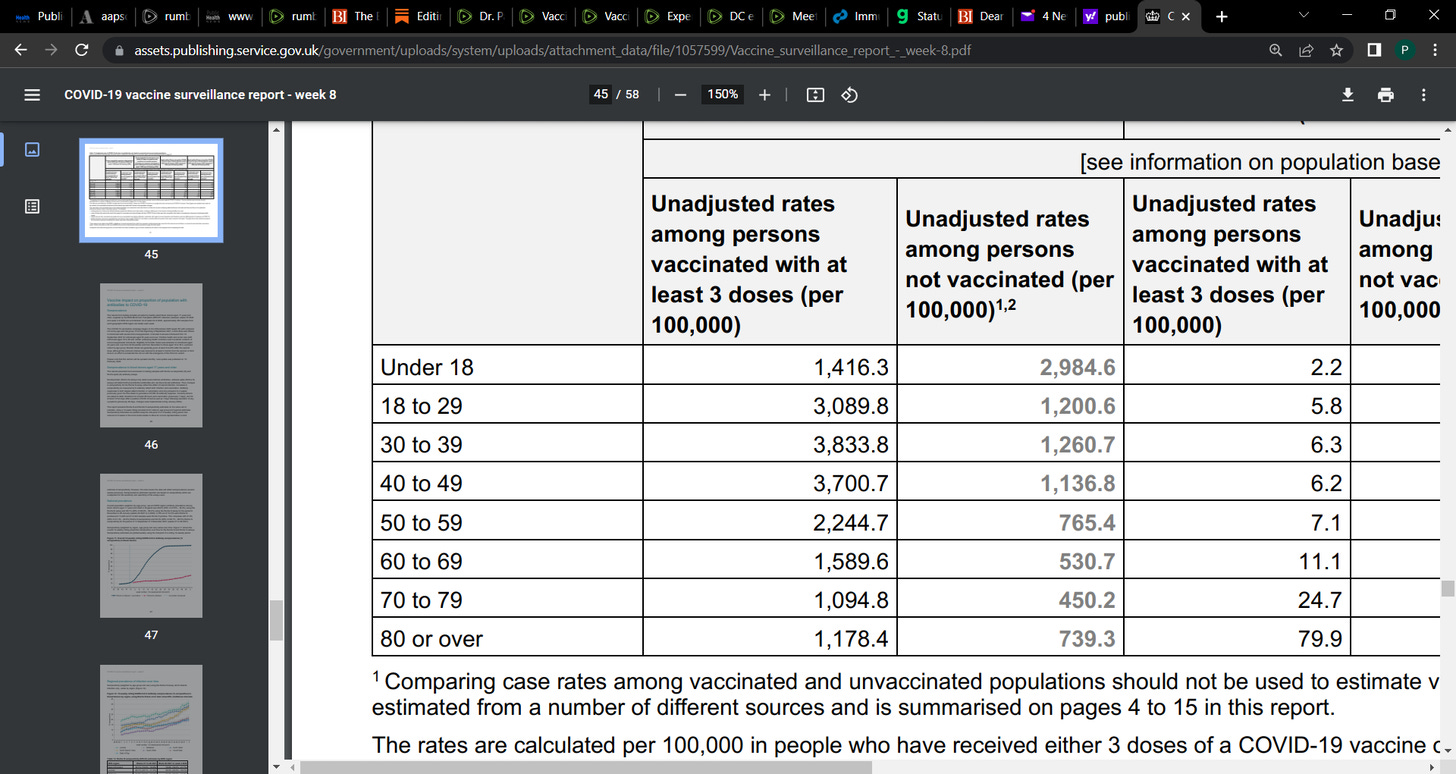
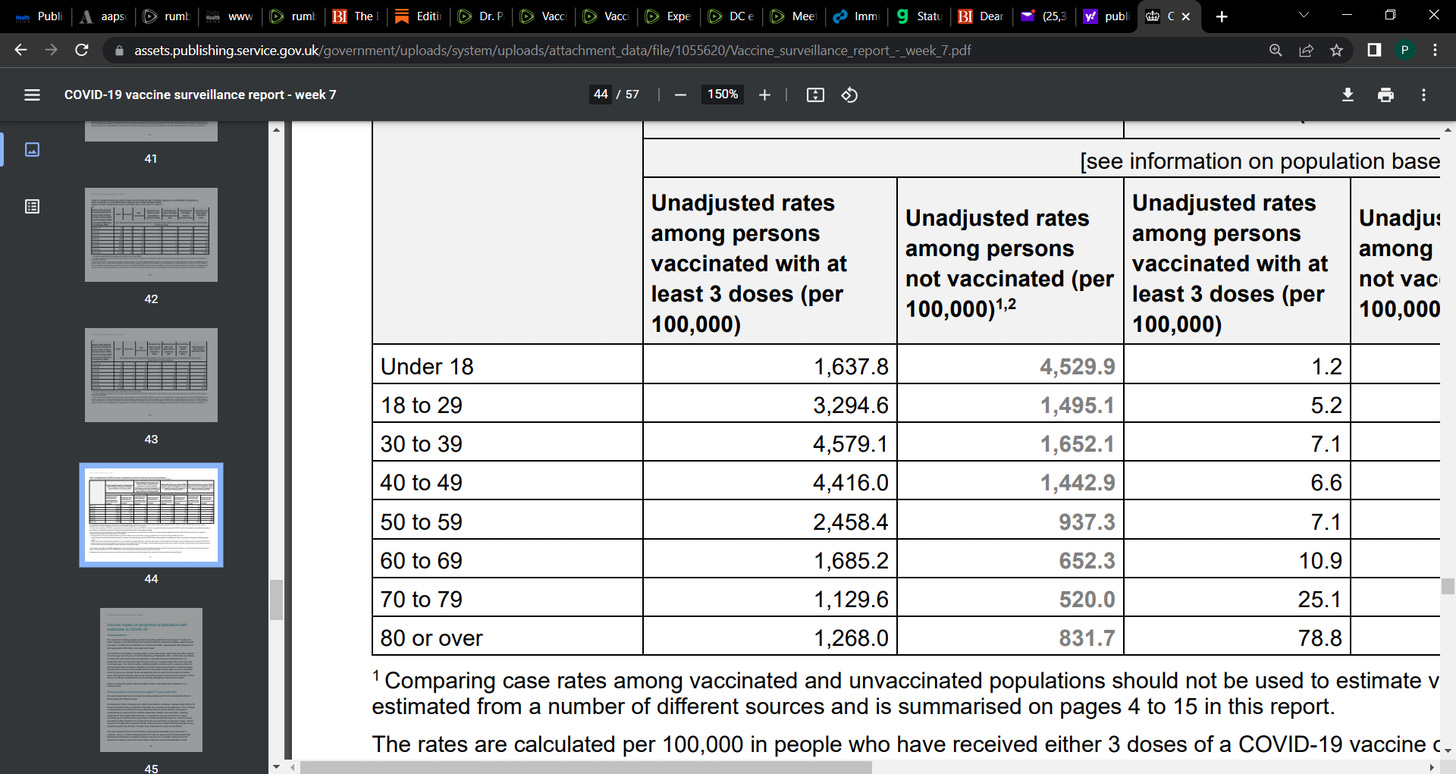
Think about it: going forward, only about 25% of the population — the hypochondriacs — are going to want these dangerous shots with no clinical safety data. It’s an unnatural experiment. The people who receive the most shots will develop Covid-19 at higher rates and experience side effects including heart attacks, strokes, infertility, and death at higher rates than the population that is not vaccinated. There will also be a dose-response relationship — the more shots, the worse the health outcomes (thereby confirming one of the
Bradford Hill criteria). This is already happening, and lots of people are starting to notice.
The FDA’s decision to authorize this junk is the most effective plan ever devised to completely discredit and destroy the FDA/CDC, mainstream allopathic medicine, and vaccines in general. The harms are heartbreaking and they will get worse.
But we just have to keep the faith, stand back, and the other side will destroy itself.
Before Covid-19 shots were introduced, I imagine it would have taken us another 50 years to bring down the Pharma cartel. Now we can do it in less than 10 years. If we work hard, perhaps we can get there in 5?
V. Where do we go from here?
I spent 5 months of my life trying to stop the FDA from committing these crimes against humanity. Between all of the medical freedom groups working on this issue we generated tens of thousands of comments and over a million emails to politicians and FDA officials. In the end, we only picked off 2 votes — Hank Bernstein and Paul Offit of all people.
Was it worth it? Absolutely.
When we started this fight back in January, 30% of parents said they were going to rush out to get their kids vaccinated right away. In April that number was down to 18%. By today I imagine it’s even smaller.
Only half of Americans have gotten “boosters”. With these new crazy shots that will have no safety data, that number will come down even further.
When we get loud to educate the FDA/CDC, we also end up educating the public. And that saves lives.
The other thing is that we forced the FDA to reveal who they truly are. This is extremely valuable because it helps us to update our strategy. Before this fight, the FDA pretended to be a regulatory agency. Well, we removed that mask and showed that the FDA absolutely does not care about science nor health. Furthermore we discovered that the FDA has been
laundering Moderna and Pfizer’s data for them throughout the Emergency Use Authorization process. And now the FDA is abandoning clinical trials altogether in connection with Covid-19 shots. What an extraordinary admission of failure on their part. We now know that the FDA is NOT a regulatory agency. The FDA is the data laundering branch of the Pharma cartel. Our challenge is no longer to educate these fascist clowns but rather to replace them with people who actually care about science and health.
Going forward, there are a few things I want to do:
I intend to launch a campaign through my Substack called “This Is On You.” Lots of Americans are going to be maimed and killed by these shots in the coming months. It’s going to be heartbreaking. And what I want to encourage people to do is, every time you see a heartbreaking story of vaccine injury online I want you to print it and
mail it to the members of VRBPAC who approved these toxic shots — along with a note that says, “This is on you!” All of their mailing addresses are (
here). There is no reason we should carry the emotional burden for their crimes.
But over the long term, we absolutely have to take power. Every non-profit that works on medical freedom needs to set up a 501(C)(4) to do political work. When you go to see your heroes speak at these medical freedom conferences, ask them when they are going to set up a 501(C)(4) and see what they say.
Attorney Jeff Childers at
Covid & Coffee does these wonderful targeted fundraising operations called Operation Multiplier. Anytime a politician stands up and fights for us, he encourages all of his readers to send small donations as a token of appreciation. “He says, donate ANY AMOUNT that you can easily afford ending in the number ‘2’.” That way the campaign can track the contributions that come from his appeal. We should all amplify this effort because it is one of the best things going in the movement.
In the comments, I’m interested to read your thoughts on the steps we should take going forward to right these egregious wrongs.
Warriors, I am more grateful than you will ever know for the community we have built and the extraordinary actions you have taken over the last many months.
Today is a sad day for America. But keep your chin up because we are absolutely going to win this war.
Blessings to the warriors!
Hugs and prayers for everyone in the movement.
In the comments please let me know what’s on your mind.
As always, I welcome any corrections.
p.s. for those who are interested, I went on
Bannon and
CHD.TV after the vote to share my thoughts. The Bannon clip is raw and angry and the CHD clip from this morning is more forward-focused.
Update: June 29, 2022
Well, well, well, Paul Offit just published an Op Ed in StatNews titled, “
FDA: Don’t rush a move to change the Covid-19 vaccine composition.” Reading between the lines, it appears the Offit is backing a rival product and is somehow trying to clear a path for its approval:
Would the country be better off using the available resources to accelerate the creation of next-generation vaccines that can produce neutralizing antibodies in amounts high enough to deal with most variants? Or vaccines that can be delivered into the nose, a route that may provide stronger protection against infection?
Offit is the biggest name on the VRBPAC and if he’s publicly pouring cold water on the FDA’s decision there’s a chance it ain’t over yet. Stay tuned.