[continued from post above]
Another recent article is titled: “Why are some people naturally immune to COVID?”
Here are some key excerpts.
“Recent scientific evidence has shown that some people are naturally immune to COVID and all its mutations. …Recent scientific evidence indicates that some people are naturally immune to COVID and all its mutations. The story of entire families except one person being infected with an illness is not new, and there are also people who continue to become infected even after they have been fully vaccinated and have recovered from the virus. According to the UK
Office for National Statistics, one out of every 25 people in the United Kingdom is infected with coronavirus; however, a large number of people are not infected. Scientists have clearly stated that some people have natural defences against coronavirus, and it is not exactly clear why, especially since they continue to be immune even in the face of new mutations.”
“Researchers in countries such as the United States and Brazil are analysing the genetic variations found in such [virus resistant] people. At
University College London, the scientific community is investigating the group of health workers who, despite being on the front line of the pandemic, have turned out to be immune. One such worker is 34-year-old emergency nurse Lisa Stockwell, who has always had negative tests since 2020.”
“The UCL researchers examined the health workers’ blood before the vaccines were launched, confirming that they did not have antibodies and had therefore never been infected. However, they did have T cells, which are found in people who have recovered from coronavirus. This type of cell is created by the immune system to defend the body and has the function of attacking and destroying viral cells.”
Another October 2021 article is titled “Some people might be genetically resistant to COVID-1.”
“Can you be genetically resistant to the novel coronavirus? A
new paper suggests it is possible people might have the power to fight off COVID-19 because of their genetics. Researchers said in the paper — published in the medical journal
Nature Immunology — there might be people who are resistant to the SARS-CoV-2 virus, which causes COVID-19.”
“Scientists said the virus has been known to invade households but leave one or two people without an infection, per
Science Alert.”
“The introduction of SARS-CoV-2 to a naive population, on a global scale, has provided yet another demonstration of the remarkable clinical variability between individuals in the course of infection, ranging from asymptomatic infections to life-threatening disease,” researchers wrote in the paper.”
“Our understanding of the pathophysiology of life-threatening COVID-19 has progressed considerably since the disease was first described in December 2019, but we still know very little about the human genetic and immunological basis of inborn resistance to SARS-CoV-2,” they wrote.”
“Virologists Theodora Hatziioannou and Paul Bieniasz, who both work at the Rockefeller University in New York City, are trying to figure out how people can be super immune to the coronavirus. Those who are super immune can block mutant coronavirus strains in many cases.”
Another article is titled “A lucky few seem ‘resistant’ to Covid-19. Scientists want to know why.”
The article begins with a story of a husband in Brazil who got deathly ill with COVID. But the wife sharing the same close quarters with her husband while he was infected and able to transmit the virus and who never wore a mask in the home with him, and who shared the same bed and was physically intimate never got infected. She was tested for an active or past infection — twice — and her bloodwork came up negative.
Moreover, the woman went to a meeting at the University of São Paulo where an infected attendee set off a chain reaction of positivity – but the woman did not get infected as shown by negative tests.
This case defines the medical mystery baffling scientists.
This article noted: “Some people become infected but their immune systems spontaneously clear the virus, keeping them from developing the actual disease. These individuals may be asymptomatic, but this is not the same as resistance; an antibody test would generally detect evidence of a prior infection. Instead, resistance is broadly understood as having cleared a virus before it enters cells and gets a foothold – preventing infection, in other words, not just disease.”
“A team of scientists at New York University and the Icahn School of Medicine at Mount Sinai were the first to report finding genes possibly tied to resistance to Covid-19. In early 2020, … [a set of researchers] set out to sort through the potential genetic factors underlying Covid resistance. To do this, they used CRISPR genome editing technology to disable each of the 20,000 human genes in lung cells and then exposed them to SARS-CoV-2. Most of the cells died within a few days. ‘Anything that lives is clearly missing something essential for a virus, and so potentially has a significant gene mutation, [said one of the researchers].’”
“In January 2021, the group published a paper in
Cell, reporting that RAB7A, a gene important for the movement of cargo from inside the cell to the cell surface, topped their quantitative ranking of genes the coronavirus can’t do without. Inhibiting RAB7A reduces SARS-CoV-2 infection by ensuring ACE2 receptors are retained inside the cell, making them unavailable as the required point of attachment for the spike protein of SARS-CoV-2 (which attaches and then enters the cell).”
“In a paper accepted for publication in Nature Immunology, [several scientists] with the
COVID Human Genetic Effort propose several potential sites in the genome that could govern resistance to SARS-CoV-2, and suggested undertaking large genome-wide association studies that screen large populations for gene variants associated with resistance to SARS-CoV-2.”
Another recent 2022 article is titled: “Are some people naturally Covid-proof? Scientists around the world are studying the phenomenon of health workers and others who are regularly exposed to the disease but have yet to become infected.”
“Mounting evidence that people are naturally resistant to Covid and its mutations. One theory is that they have previously recovered from different coronaviruses.”
“It’s a common yet curious tale: a household hit by Covid, but one family member never tests positive or gets so much as a sniffle. Now scientists may have an answer: there is mounting evidence that some people are naturally Covid-resistant. For reasons not fully understood, it’s thought that these people were already immune to the Covid virus, and they remain so even as it mutates. The phenomenon is now the subject of intense research across the world.”
“In America and Brazil, researchers are looking at potential genetic variations that might make certain people impervious to the infection. And at University College London (UCL), scientists are studying blood samples from hundreds of healthcare staff who – seemingly against all odds – avoided catching the virus.”
“One such frontline worker is Lisa Stockwell, a 34-year-old nurse from Somerset who worked in A&E and, for most of 2020, in a ‘hot’ admissions unit where Covid-infected patients were first assessed. Towards the end of last year she signed on with a nursing agency, which assigned her daily shifts almost exclusively on Covid wards. Colleagues working by her side have, at various points throughout the pandemic, ‘dropped like flies’. But she says: ‘I didn’t get poorly at all, and my antibody test, which I took at the end of 2020, before I was vaccinated, was negative.’”
“’I expected to have a positive test at some stage, but it never came. I don’t know whether I have a very robust immune system, but I’m just grateful not to have fallen sick.”
“Early on in the pandemic, Lisa’s loved ones were also succumbing to the virus. She adds: ‘My husband was sick for two weeks with a raging temperature that left him delirious.’”
‘Despite sharing a bed with him, I never caught it.
“I even shared a car to work every day for two weeks with a nurse friend who, days later, was laid low with Covid.”
“She says: ‘I was working every day on Covid wards, wearing PPE that was far from the best quality, and was initially terrified of catching the virus.’”
“But I never did and now I’m beginning to think maybe I never will.”
Nasim Forooghi, 46, a cardiac research nurse at St Bartholomew’s Hospital in Central London, has a similar tale.
“The mother-of-two, whose husband is an NHS doctor, has been heavily involved in research tracking Covid among frontline staff – a role that has potentially exposed her to hundreds of infected people since the pandemic began in early 2020.”
“Like Lisa, she too has had a succession of antibody tests which found no trace of the virus ever being in her system. ‘Obviously I was using protective clothing but, even so, I was exposed to a lot of infected people,’ says Nasim.”
“I was having blood tests every week but they found nothing, even though I was exposed to it regularly.” She adds: ‘Every day for weeks on end I was dealing with doctors and nurses who were on the front line and face-to-face with patients on Covid wards.’”
“When the UCL researchers examined the blood of seemingly Covid-proof healthcare workers that had been taken before the vaccine rollout, it confirmed they had no Covid antibodies – meaning it was unlikely they had ever been infected.”
“However, they discovered other immune system cells, called T cells, similar to those found in the immune systems of people who have recovered from Covid. Like antibodies, T cells are created by the immune system to fend off invaders.
But while antibodies stop viral cells from entering the body, T cells attack and destroy them.”
“T cells remain in the system for longer and will have snuffed out the virus before it had a chance to infect healthy cells or do any damage, experts suggested. But why were they there in the first place? One theory is that the protection came from regular exposure in the past. This could have been through their jobs dealing with sick patients or facing other, less destructive types of coronavirus.”
“The UCL team carried out further tests on hundreds more blood samples collected as far back as 2011, long before the pandemic struck, and discovered that about one in 20 also had antibodies that could destroy Covid. Samples taken from children had the highest levels. Scientists said this was possibly because they were regularly exposed to cold-causing coronaviruses through mixing with large numbers of other youngsters at nursery and school, which could explain why, now, Covid rarely causes severe illness in this age group.”
“It appears the most likely explanation for a Covid-proof immune system is that, after it has been repeatedly exposed to another coronavirus, it is then able to detect and defeat any mutated relatives because it is recognising proteins found inside the virus rather than on its surface. These vary little between coronaviruses. ‘Internal proteins don’t mutate at anything like the same rate as external ones,’ says Professor Andrew Easton, a virologist at Warwick University.”
Another 2022 article is titled: “Irish study seeks people who have avoided Covid-19 to determine natural immunity.”
“Irish researchers are seeking people who have avoided Covid-19 to take part in an international study. Researchers at Trinity College Dublin are trying to establish if some people are “naturally resistant” to the virus, with those who have shared a bed with someone with Covid-19 without becoming infected themselves of particular interest to the study.”
“Professor Cliona O’Farrelly, the principal investigator of the study, says that researchers are seeking people who resisted Covid-19 before receiving a vaccine and after the outbreak of the Omicron variant. She says that some people have an immune system that is able to “keep the virus away without becoming infected at all.”
“The study will examine healthcare workers at St. James’s Hospital in addition to members of the general public who have not contracted the virus despite sharing the same household as someone with Covid. Researchers are seeking adults who shared a bed with a confirmed case of Covid-19 over the first three symptomatic days of the person becoming infected or those who were exposed to a confirmed case for at least an hour a day over the first five symptomatic days.”
“O’Farrelly said that researchers expect to find some mutations in people’s innate immune genes that provide natural resistance. This consortium is looking for genetic markers of resistance to infection. So it means having to sequence the whole genome of the people who are resistant – it is like looking for a needle in a haystack because the human genome is so hugely variable, O’Farrelly said.”
“We’re anticipating that we will see some mutations in some of the innate immune genes that give people resistance.”
“A study in Nature Communications published earlier this year found that people who had previous exposure to other coronavirus strains may have built up a resistance through a pre-existing memory T-cell phenotype.”
Conclusion
The widespread and intense push for COVID vaccination and booster shots has ignored the reality that a certain fraction of people has effective resistance or immunity to COVID infection. Ongoing research is documenting this, and precise explanations are evolving and worth more attention. Eventually, better vaccines and therapeutics may be developed based on the answers discovered for effective COVID infection resistance.




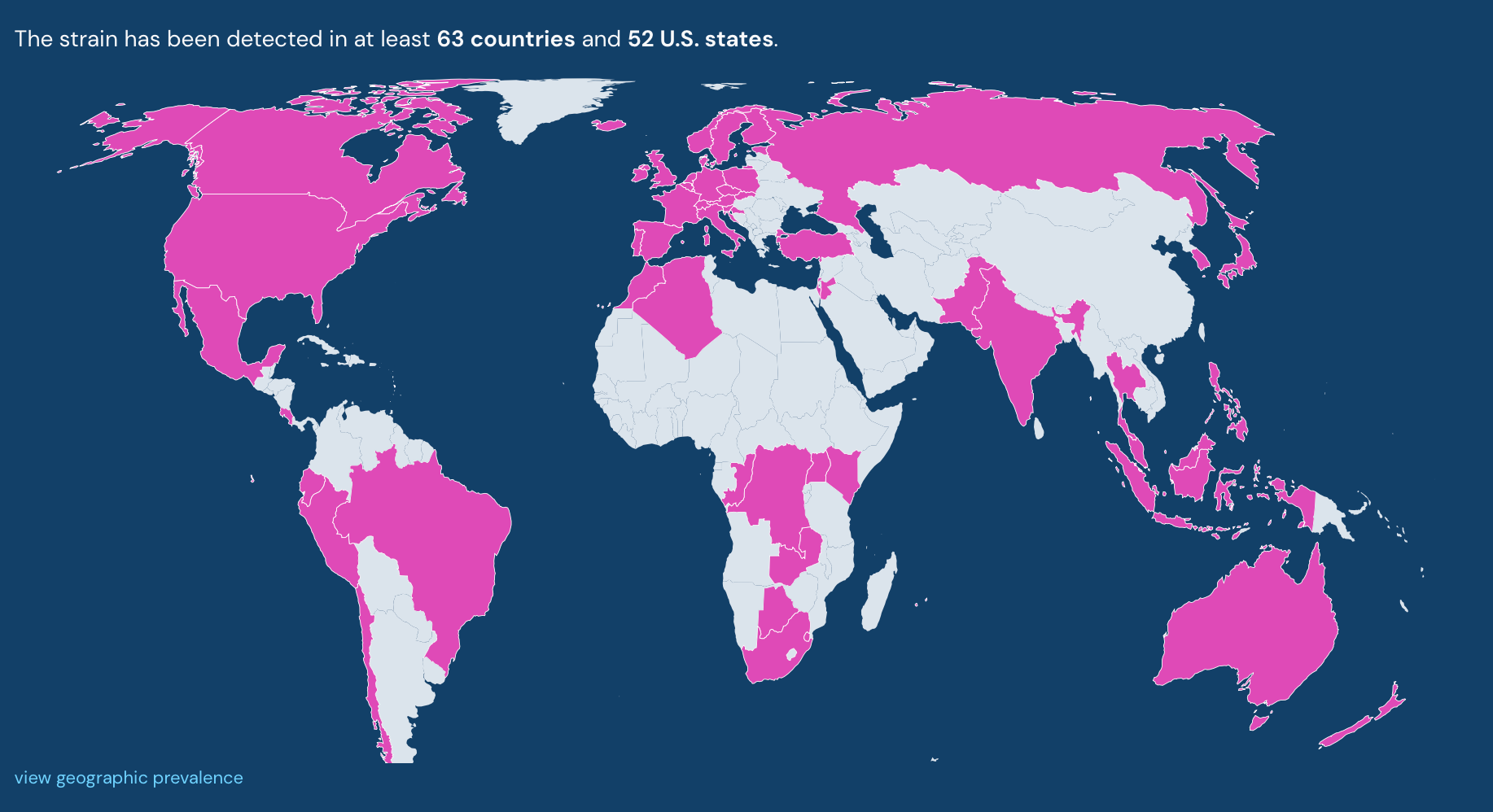





































") . The CDC also counts Puerto Rico and DC when they do their counts of what's going on in the USA. So 50 states plus Puerto Rico and DC = 52. I was confused too when I first saw it. Then again, the CDC thinks men can give birth so why not have 52 states .... Apparently old definitions don't matter anymore...
. The CDC also counts Puerto Rico and DC when they do their counts of what's going on in the USA. So 50 states plus Puerto Rico and DC = 52. I was confused too when I first saw it. Then again, the CDC thinks men can give birth so why not have 52 states .... Apparently old definitions don't matter anymore...