It's sad that lately I've had to so often quote Mark Twain's famous truthful statement, "It is easier to fool

truthbasedmedia.com
 German Doctor Says If Anyone Should Be Locked Down and Restricted, It’s the Real Super-Spreaders: The ‘Vaccinated’
Despite the mainstream narrative, we are experiencing a pandemic of the vaccinated.
German Doctor Says If Anyone Should Be Locked Down and Restricted, It’s the Real Super-Spreaders: The ‘Vaccinated’
Despite the mainstream narrative, we are experiencing a pandemic of the vaccinated.
by
JD RUCKER
November 28, 2021
It’s sad that lately I’ve had to so often quote Mark Twain’s famous truthful statement, “It is easier to fool the people, than to convince them they have been fooled.”
This, more than anything else, is why this article will be labeled by the “fact-checkers” (aka the false-narrative-reinforcers) as misleading or even outright fake news. With billions of people worldwide having fallen for the Covid-19 “vaccine” con, it will take something catastrophic (God forbid) for the truth to finally come out. We’ve seen clear facts, unambiguous data, and trustworthy studies that have demonstrated three things beyond a shadow of a doubt:
- The “vaccinated” are just as likely as the “unvaccinated” to contract Covid-19 when they come in contact with the disease
- The “vaccinated” are just as likely as the “unvaccinated” to spread Covid-19 when others come in contact with them
- Many of the “vaccinated” have been lulled into a false sense of security that makes them more likely to engage in Covid-spreading activities and are therefore the real coronavirus super-spreaders
For those who have been watching with fascination and horror as the science gets butchered on a daily basis by government, mainstream media, Big Tech, academia, healthcare professionals, and all the various minions of Big Pharma, it’s abundantly clear that the agenda has superseded the truth. None of the “experts” such as Anthony Fauci or Rochelle Walensky even attempt to debunk any of the statements above because they cannot. Nevertheless, they continue to echo the vaxx-nanny mantras because they know far too many Americans refuse to look at the facts or think for themselves.
Perhaps the saddest realization for me in the era of Pandemic Panic Theater is seeing how reliant Americans are on the “experts” for information and direction. The data is available for anyone with an internet connection to see. But many if not most Americans have willfully stuck their collective heads in the sand and ignored the science in wholesale. Why? Because the “experts” deliver false conclusions from the science and most are simply too lazy to do some fact-checking on their own.
That’s a long build-up for the article below. But the build-up was necessary to frame what you’re about to read because it’s another example of a bombshell that will be actively and viciously suppressed by corporate media. Any doctor who echoes the sentiment below will likely lose their job and their license to practice. That’s how draconian the suppressors of the truth have become. Anything or anyone that counters their narrative must be fully destroyed, not just to keep the truth from getting out but also to set an example for anyone else who would be brave enough to disseminate it.
This article from
Free West Media details what most who read this site already know: We’re in the middle of a pandemic of the vaccinated, but since the vaxx-nannies control government, media, and the like, the false narrative of this all being a pandemic of the unvaccinated is still the dominant perception. We need to change that one article, video, or podcast a time. Spread the word, friends.
Vaccinated as the ‘Biggest Virus Spreaders’ Should Be Locked Down
Why should those vaccinated against Covid-19 be restricted in their movements and participation in society? Because vaccinated people are “the biggest virus spreaders”, German doctor Kenan Katmer from Bochum explained.
According to a report by the WAZ, the doctor runs a family doctor’s practice in Altenbochum, where he also offers Corona tests and vaccinations. From the results of the tests in his own practice and the four test centers in Bochum, he was able to conclude that “90 percent of the positive people who were tested by me were vaccinated.”
Katmer pointed out that “most of the vaccinated (…) think that with the vaccination the Coronavirus will no longer harm them, but that is a fallacy”.
The physician believes a
two-month lockdown only for vaccinated people should be declared by public health authorities. If these restrictions were then adhered to, the contacts reduced and the vaccination campaign continued, “the pandemic would then end quickly”.
Dr. Katmer apparently is not alone: Dr. Michael Tenholt from the Medical Quality Network in Bochum shared his colleague’s opinion. Instead of a lockdown, he spoke out in favor of additional compulsory testing for vaccinated people: “It is true that many people who are vaccinated feel too safe. Therefore, in my opinion, it is important to also test the vaccinated.”
In France, Professor Christian Perronne, one of the most renowned French experts on infectious diseases and long-standing government advisor, has long been a firm skeptic of the Covid-19 vaccination policy – and not just in his home country. With a view to the situation in Israel and Great Britain, Perronne has now publicly called for people vaccinated against Covid-19 to be quarantined and isolated from society.
The provocative demand is a reversal of the current narrative underscoring instead that the vaccinated are dangerous for others and not the unvaccinated. Especially in Israel and Great Britain, where the world’s largest vaccination programs are running, the most severe Covid cases are among vaccinated people in hospitals, according to
Report24.news.
Vaccine failure
The fact is that the vaccinations have not been doing what was promised for months. It has now been scientifically proven that “the effectiveness of the vaccine against symptomatic SARS-CoV-2 infection gradually decreases over time in all subgroups, but at a different rate depending on the type of vaccine and more quickly in men and especially in elderly, frail men.” The effectiveness against serious illnesses seems to remain high for nine months, “but not in men, elderly, frail people and people with comorbidities,” a
recent study from Sweden showed.
The authors concluded from this that only a further vaccination, or the “booster”, could help.
And here the real dilemma for vaccine pushers is revealed: Scientists, the manufacturers and governments had no idea what the vaccine, its effectiveness and side-effects would be. Despite not knowing, they were touting them as “safe and effective”.
The dilemma vaccine pushers are now facing
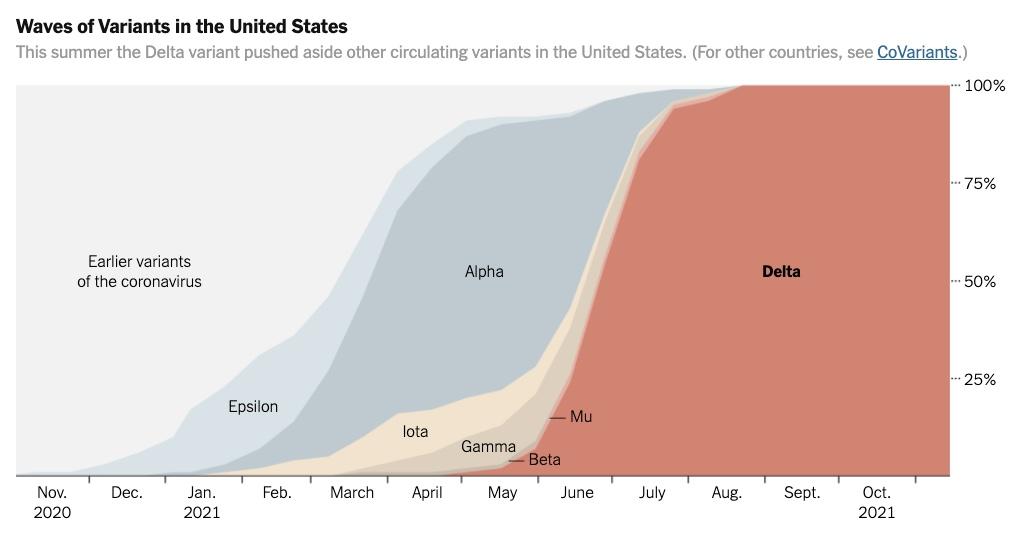
The mass experiment that the world has had to endure for almost a year now and which is called a “vaccination strategy” may be running out of “guinea pigs”. Essentially, if there is no control group, it would be more difficult to prove the negative effects of the shots. For that reason, compulsory vaccination is being discussed so that the test group of vaccinated people becomes even larger. And it is somehow ignored that the vaccine was developed against the “wild wet market” type of SARS-CoV-2, but not against the predominant Delta variant.
A new vaccine against Omicron is on the shelf, but would have to be approved again. It is not to be expected that the studies required for this will again show a fake “vaccination success rate” of 94 percent. Therefore, Pfizer and BioNtech are pushing for boosters containing the old ineffective vaccine against a new variant.
The ridiculous contradiction on the frontpage of Bild that Covid cultists choose to ignore. Via Twitter,
The lies continuously spouted by the mainstream are well-illustrated by two frontpages only days apart from the German tabloid
Bild. On November 21, the BioNtech founder declared that the “protection” of the shot was still “very high” after nine months. Four days later, the EU Commission announced the expiry of health passports… after nine months.

































")