(fair use applies)
EMPHASIS IN ORIGINAL ARTICLE (bolding is not mine)
The population’s antibody response to SARS2 is hanging by a thread
Radagast
October 28, 2024
I’ve said before that immunity to SARS-COV-2 in most people who were vaccinated now depends on a small number of loops in the N-Terminal Domain of Spike. This is why I wish to briefly go over
this study:
Omicron-specific ultra-potent SARS-CoV-2 neutralizing antibodies targeting the N1/N2 loop of Spike N-terminal domain
A multitude of functional mutations continue to emerge on the N-terminal domain (NTD) of the spike protein in SARS-CoV-2 Omicron subvariants. Understanding the immunogenicity of Omicron NTD and the properties of antibodies elicited by it is crucial for comprehending the impact of NTD mutations on viral fitness and guiding vaccine design. In this study, we find that most of NTD-targeting antibodies isolated from individuals with BA.5/BF.7 breakthrough infection (BTI) are ancestral (wildtype or WT)-reactive and non-neutralizing. Surprisingly, we identified five ultra-potent neutralizing antibodies (NAbs) that can only bind to Omicron but not WT NTD. Structural analysis revealed that they bind to a unique epitope on the N1/N2 loop of NTD and interact with the receptor-binding domain (RBD) via the light chain. These Omicron-specific NAbs achieve neutralization through ACE2 competition and blockage of ACE2-mediated S1 shedding. However, BA.2.86 and BA.2.87.1, which carry insertions or deletions on the N1/N2 loop, can evade these antibodies. Together, we provided a detailed map of the NTD-targeting antibody repertoire in the post-Omicron era, demonstrating their vulnerability to NTD mutations enabled by its evolutionary flexibility, despite their potent neutralization. These results revealed the function of the indels in the NTD of BA.2.86/JN.1 sublineage in evading neutralizing antibodies and highlighted the importance of considering the immunogenicity of NTD in vaccine design.
You don’t have to be a genius, to understand why this is bad news. This is an antibody response that quite literally hangs by a thread: Only the light chain of these new antibodies that emerged in the Omicron era still binds the receptor binding domain, the heavy chain has to bind to the N-Terminal Domain. This is not how any of this is supposed to work, as illustrated by the fact that it only happened as a way to deal with the Omicron variants.
To explain what we’re reading, let’s go back to the very beginning. People were vaccinated, to encourage the production of neutralizing antibodies. A neutralizing antibody blocks a viral particle from attaching to the receptor of a cell in which it can replicate itself.
The part of a Spike protein that binds to the receptor is called the Receptor-Binding domain. That’s where you expect to find neutralizing antibodies to bind that serve to develop immunity against a virus. Some vaccines against SARS2 didn’t even contain the rest of the Spike protein, they only injected people with the Receptor-Binding Domain.
Over time however, this part of the virus mutates. The immune system is then forced to use the antibodies it already developed against the RBD and change them, to fit the new RBD (somatic hypermutation). These tend to be of lower quality, than if it had the opportunity to develop a whole new antibody response from scratch.
This is what we call Original Antigenic Sin, a term that is exactly as intimidating as it should be, to warn humans that you have to be
really sure you know what you’re doing, when you want to intervene in a complex system like this.
In most of the human population, a second problem has by now emerged. These antibodies against the RBD are no longer part of the IgG3 class, which is able to bind very strongly. They class-shifted to IgG2 or IgG4. IgG antibodies have two identical arms (except IgG4), that can move separately and bind identical looking targets. Those two arms both contain a light chain and a heavy chain. IgG3 is unique in that it can form
cross-links: It’s a very bendy molecule, so its two arms can easily find two separate Spike proteins, thereby offering much stronger neutralization.
This means the immune system of most people is now stuck with antibodies against the Receptor Binding Domain, that have
poor affinity. You can think of this as a bunch of magnets floating in water, that very slowly move towards a piece of metal (the Spike protein) in the water. If it happens before the metal reaches its destination (generally the ACE2 receptor), the protein has been neutralized.
In the lab this works pretty well. You put these antibodies in your Petri dish, let them soak together with the Spike proteins. You wait for a while, then you add your cells, see if any get infected and then you say to yourself: “Well, good news, the Spike proteins are still being neutralized!” In the human lung, it doesn’t work like that of course. The Spike protein may find the ACE2 receptor before the antibody gets a chance to bind. In that case, the antibodies will look neutralizing to you in your petri dish, but in practice fail at neutralization in the body.
So the immune system can no longer rely on antibodies against the RBD, to neutralize viral particles. In a sense, you could say that it already “spent its ammunition”, on the receptor binding domain, so it’s now left with antibodies binding there that are just too slow to neutralize. And in response to that, the immune system becomes forced to come up with different antibodies, that still manage to achieve neutralization. This is the underlying problem.
So that’s what this study found. There are five loops in another part of the Spike protein, the N-Terminal Domain. Those loops are very immunogenic, that is, they look very different from our own proteins, so our body can produce antibodies against them without causing trouble for us. But just because they are immunogenic, does not necessarily mean that antibodies against these regions will be
neutralizing. Antibodies could bind to this part of the Spike protein, without blocking the Spike protein from performing its job.
In this case, they found that the vast majority of the antibodies made against the N-Terminal Domain, are not neutralizing. They found one exception however. The immune system is able to make antibodies against the N1 and N2 loops of the N-Terminal Domain, that bind with one part to these loops and with the other part, to the Receptor Binding domain.
This way, the immune system can still produce neutralizing antibodies: Instead of finding an entire region of the Receptor Binding to bind to, like a normal neutralizing antibody would, these new antibodies find a small region of the Receptor Binding Domain and a small region of the start of the N-Terminal Domain.
These are strange new antibodies, an abnormal way of neutralizing a viral particle. The immune system only started developing these antibodies once it ran out of ways to neutralize through the Receptor Binding Domain. We know this, because they’re only made against the Omicron variants, there are none of these antibodies seen against the original pre-Omicron variants of the virus. If it was a normal way to neutralize the virus, we would have seen it emerge before Omicron.
The result of course, is that huge pressure is placed on the virus, to change the region where these antibodies still manage to bind. Change that region and people are again left without potent neutralizing antibodies, that is, antibodies that will actually manage to beat the virus in a real human body, instead of just in a Petri dish.
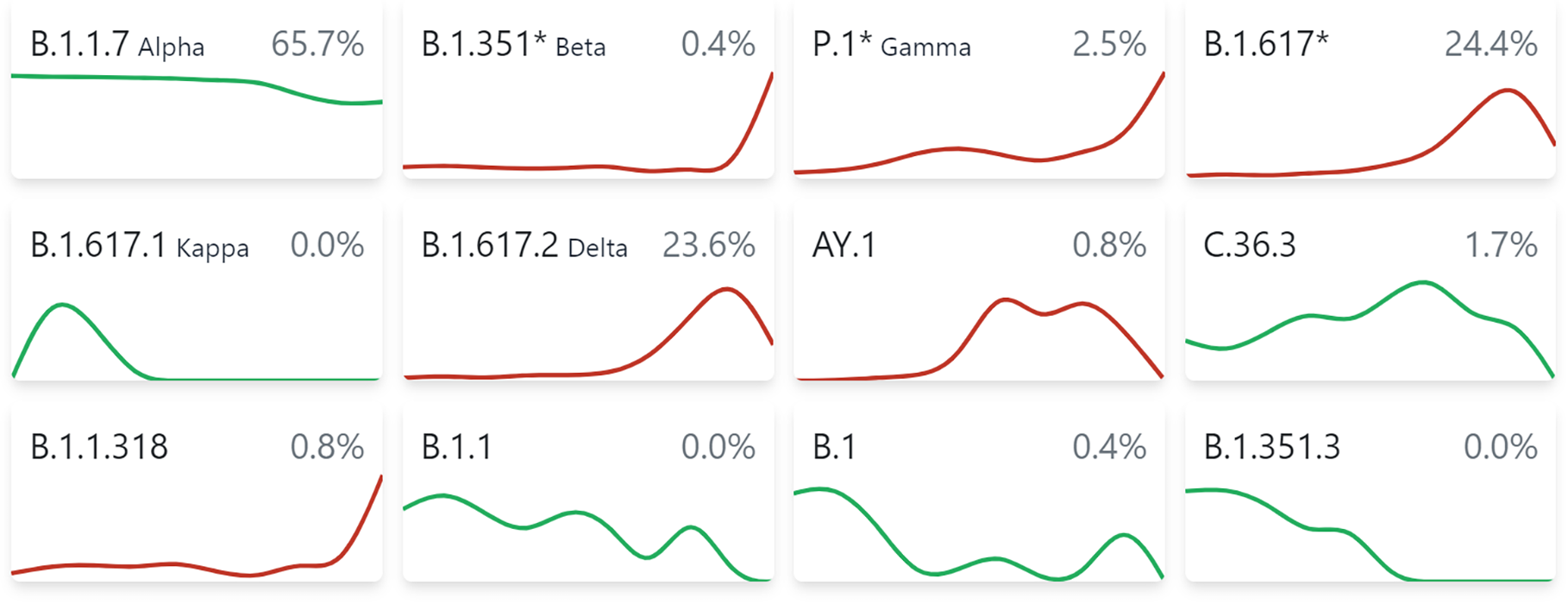
So that’s what happened. The virus responded by changing the N1 loop, with a new very different variant, called BA.2.86. This happened about a year ago. It added four new amino acids at position 16, right at the start of this N1 loop. This made the N1 loop look so different that most of these new antibodies would have become useless. All strains now circulating descend from this new variant.
The immune system responds to this, with new antibodies, that find some other part of the N1 and N2 loops, to bind to the new version of the virus. But those new versions of the antibodies, are forcing the virus to mutate yet again. And this time, things are looking very different.
Why? Because
now the virus is adding glycans, sugar molecules, to its N1 and N2 loops. When glycans are added to a part of a protein, it becomes very hard if not impossible, to neutralize a virus through that part of the protein, even with new antibodies.
Here’s what happened: One version put a glycan on S:30, just next to the N1 loop, by deleting amino acid S:31. This is what made most people sick this summer.
But another version, XEC, which is now taking over the world, went with a different solution: It puts a glycan on S:22, right in the middle of the N1 loop. These glycans are called N-linked glycans, they’re very big sugar molecules. There’s clearly huge pressure to get rid of these antibodies, because almost everything now has a glycan on either S:22 or S:30.
But there are other glycans, called O-linked glycans (because they attach to an Oxygen atom in an amino acid), that are smaller. In addition to S:22, on S:59, XEC put Serine, which should allow the virus to add an O-linked glycan there. This most likely blocks antibodies from binding to the N2 loop, which runs from amino acid 67 to 79.
You can see in the past few months, that the virus is under huge pressure to add these sugar molecules in this region, as a consequence of these strange new “last ditch effort” antibodies produced by the immune system.
The N1 loop has been dealt with, first by the insertion at position 16, followed by the glycans added at S:30 or S22. With S:59, it seems the virus deals with antibodies that can still use the N2 loop. But we see that this XEC variant is changing the inside of the N2 loop itself now too:
If it changes amino acid 72, that seems to be sufficient to interfere in the neutralizing antibodies that depend on the N2 loop. What it changes the amino acid into matters less, either R or D works.
It’s clear from these numbers, that this XEC variant is extremely eager to change the N2 loop, as we see mutations pop up at position 70, 72 and 75, all in recent weeks.
So people can’t make antibodies anymore that neutralize by binding the N1 loop and the RBD, the glycans have dealt with that. Antibodies that use the N2 loop and the RBD are now starting to suffer the same problem with the XEC variant, which is clearly very rapidly changing N2.
The question of course is: What happens after that, when all these antibodies using this exotic mechanism become unable to neutralize Spike?
It seems the immune system is running out of new ways to produce neutralizing antibodies. There might be some other mechanism for antibodies to neutralize viral particles that nobody is currently aware of. But the obvious target (RBD) has been exhausted and the new exotic mechanism that emerged with Omicron, is now being exhausted too.
So instead, people are now stuck with a wide range of low-affinity non-neutralizing antibodies. Those non-neutralizing antibodies won’t stop the viral particles from entering a new cell. Without neutralizing antibodies, the adaptive immune system can’t stop the cycle anymore, it can only clean up after the fact. These non-neutralizing antibodies also interfere in the innate immune system recognizing the virus, especially if they are IgG2 or IgG4 , but I have explained that before.
The incentives normally don’t favor the development of complete neutralizing antibody resistance in respiratory viruses. Consider the glycans a virus needs to achieve such resistance. They
tend to make it easier for the innate immune system to deal with a virus. Because in most people, the innate immune system would normally be doing most of the job, adding glycans would not have a clear benefit.
But in our case, the virus is now continually under huge abnormal antibody pressure in most of the population, against a very small part of its Spike protein. It then mutates that small part of the protein, the antibody pressure then shifts to another part of the protein, so then it mutates that small part. Right now, that small part is the N2 loop of the N-Terminal Domain, the N1 loop has already been dealt with and the RBD was dealt with long ago.
So the virus has by now dealt with the N1 loop and versions of the virus that have in addition dealt with the N2 loop are already here.
The question is really: What’s left after this?
A situation in which most of humanity
can’t develop a neutralizing antibody response anymore, would be new. But that seems to be where we’re now at, with the newest XEC lineages.
To summarize, what happened is roughly as following:
-Vaccination
-People develop antibodies against the RBD of Wuhan
-Delta emerges, which is faster
-Antibodies concentrations have to rise to stop Delta breakthrough infections (compensatory response #1)
-High concentrations of IgG3 antibodies lead to excessive inflammation, so class shift happens (compensatory response #2)
-Omicron emerges
-Antibodies undergo somatic hypermutation to bind the Omicron RBD (compensatory response #3)
-Omicron avoids those too.
-Unusual new antibodies develop that only bind partly to the RBD and partly to the N1 or N2 loops (compensatory response #4)
-BA.2.86 emerges and shakes most of those antibodies off.
-New antibodies develop that bind to the new version of the loops. (Compensatory response #5)
-The new version of the loops now starts adding glycans to N1, making it impossible for antibodies to bind here.
-Antibodies that use N2 have to do all the work now.
-XEC begins changing N2. (Compensatory response #6)
The question that’s now left for us, is whether there is any real way left, to develop new potently neutralizing antibodies against these new XEC lineages.
But it seems unlikely. The normal route (antibodies against the RBD) has been exhausted. This is the route the immune system normally pursues and it’s also the route that all the vaccines sought to use back in 2021. But that option has now been exhausted in most people.
So the immune system found an abnormal route, as part of a compensatory response. And that compensatory response is now nearing its end.
So what’s left after this?
You might think I’m “doom-mongering”. But the evidence is just pretty clear: The immune system was forced to develop an abnormal antibody response once Omicron emerged, because the original response could no longer achieve neutralization. That abnormal antibody response is now easily avoided by new mutations. There’s no real way to dispute this.
Human beings have an innate immune system that normally handles most of the viral load of respiratory viruses. When the innate immune system can’t handle such a virus on its own, the adaptive immune system has to join and develop antibodies that neutralize the virus. It normally picks small regions where it develops antibodies with high affinity. As time progresses, it improves those antibodies further (affinity maturation).
That puts a virus under certain molecular constraints, by disadvantaging the variants that provoke these antibodies. That’s for example why the 1918 flu never returned: The
survivors had very potent antibodies, that only worked against the 1918 influenza, but no other influenza viruses.
We didn’t let this process run its natural course with SARS-COV-2. Rather, we wanted the whole population to have very high concentrations of antibodies against this virus. We used our vaccines for this. The effect becomes that antibodies can’t discriminate against virulent variants of SARS-COV-2.
But more importantly, it means the innate immune system does not get to improve itself through successive reinfections. Instead, the body depends on these antibodies to protect itself. And because this is the case for most of the population, the virus is forced to evolve to get rid of these antibodies. It has been very successful at this, forcing the immune system to develop a strange compensatory response.
But the effect is that most of humanity is now about to lose the mechanism that normally allows the immune system to put a break on viral respiratory infections that the innate immune system can not handle on its own: Neutralizing antibodies.
In hindsight, it should have been obvious something went terribly wrong, when it became clear that the mRNA vaccinated had an IgG4 response to the receptor binding domain, with no IgG3 left, whereas all(!) of the unvaccinated still had a normal IgG3 response. That’s when all the alarm bells should have gone off.
But what people did instead, back when there was still time left to come up with a solution, was to come up with excuses. People said that there’s an IgG4 response seen to measles too. That merely illustrates the problem. Measles is known to interfere in the body’s immune system, by discouraging inflammation. That’s how it causes the IgG4 class shift. In practice it doesn’t matter, because you’re never reinfected by measles.
So now you have clear evidence that the immune system became forced to develop an abnormal compensatory antibody response that binds the N1/N2 loops and the RBD together, that has already been overcome by new XEC lineages.
What’s the answer to that going to be? More excuses of course. Once you have the needle in your own arm, or worse still, your children’s arms, you no longer want to see what you did.







:max_bytes(150000):strip_icc()/Health-GettyImages-1306165716-c24cbb81ceca4678bef8638e3f33e24b.jpg)