President Trump said well these bureaucrats came at him from every side. They were all telling him what he had to do. He had the right instincts. He knew that he shouldn't close down the country. But he did it. He got rolled by his bureaucracy.

brownstone.org
(fair use applies)
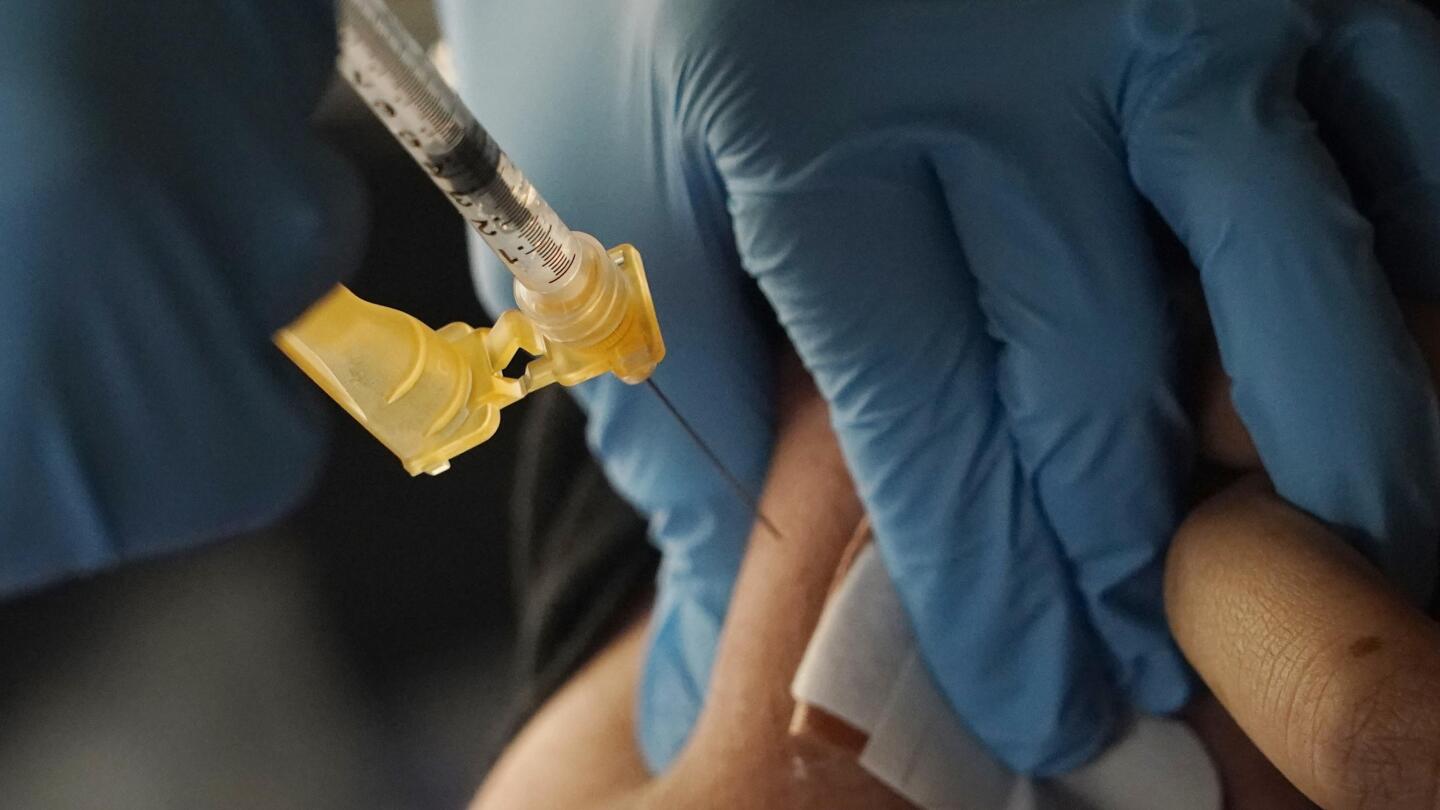
Robert F. Kennedy, Jr. on Lockdowns: Excerpt from the Announcement Speech
By Brownstone InstituteBrownstone Institute
April 22, 2023
On April 19, 2023, Robert F. Kennedy announced his intention to challenge Biden in the Democratic primary for president. As part of his announcement speech in Boston, he spoke bluntly about Covid lockdowns. What follows is the relevant excerpt of that speech.
You can read the full text here.
I want to move on to another topic that nobody’s going to want to talk about. But I’m going to talk about lockdowns. Nobody wants to talk about it. But we need to understand.
You know I grew up at a time that economists call the great prosperity. It’s when the American middle class between 1945 and 75. Grew to be the biggest economic engine on the face of the earth.
I mean we were the economy in the globe. We made everything and everybody looked to us not only for goods but for moral leadership and we became the most powerful country in the world. Unrivaled. It was because we had a stable democracy with institutions that people trusted the press that told us the truth.
Everybody knows it’s an economic and political economic rule. You cannot have democracy in a society where there is high concentrations of wealth and widespread poverty. You need a middle class or you don’t get democracy. That is a law. You cannot do it, you cannot do it unless you have a big middle class. We had that. But since the early 1980s there’s been a systematic attack on our middle class.
The coup de grace was a lockdown. Lockdown was the biggest shift in wealth in human history. I’m going to tell you about that in a second. I blame President Trump for the lockdown. President Trump gets blamed for a lot of things that he didn’t do and he gets blamed for some things that he did too. But the worst thing that he did to this country, to our civil rights, to our economy, and to the middle class in this country, was a lockdown.
In fairness let me just make this point. Trump will tell people, well the lockdown wasn’t my idea. It was my bureaucrats. They rolled me on it. I was saying we shouldn’t do it. But that’s not a good enough excuse. He was the president of the United States. As Harry Truman said, the buck stops here.
Six hundred doctors signed a letter to President Trump begging him not to do the lockdowns. They pointed out that at that time, all of the pandemic protocols anywhere in the world, the WHO, the CDC, everywhere, the European health agency, all said you never do mass lockdowns. It causes much worse havoc and deaths and injuries than if you do the standard protocol which is you lock down the sick, you protect the vulnerable, and you let everybody else go back to work.
Otherwise you are going to wreak havoc.
I wrote about it. On Instagram I was writing every day. I was citing these economic studies that showed every point in unemployment you get 37,000 excess deaths from heart attack, suicides, plus imprisonments.
I was writing about this and they dumped me from the platform. They said that’s misinformation. But it was not. People were saying it. People knew it. It wasn’t just me. We now know of course that it’s true. Now study after study and every comparison between the states and nations that locked down compared to those who didn’t has shown the ones who locked down had worse Covid death.
Numbers came out this week for Sweden, which was the only country in Europe that didn’t lock down. It had the lowest excess deaths in Europe, which is very predictable.
The nation that led lockdowns was the US and we had the highest body count of Covid on Earth. We have 4.2 percent of the world’s population yet 16 percent of the Covid deaths. At some point, even the media is going to have to stop saying that this was a success story.
The health issues were almost dwarfed by the economic cataclysm that befell our country. The IMF and Harvard study by Larry Summers showed that the cost of the lockdown to the United States was $16 trillion. $16 trillion for nothing!
We shifted $4 trillion from the middle class in this country to the super-rich. We created 500 new billionaires. The existing billionaires increased their wealth, according to the Oxfam study that came out three days ago, by 30 percent. This was a gift to the rich. And guess what? The ones who got rich were social media companies like Amazon and Facebook and Microsoft that were conspiring with President Trump’s White House to censor people like me.
So the very people who were profiting on those lockdowns were the ones who were strip-mining the wealth from the middle class in this country. Amazon got to close down all of its competitors. 3.3 million businesses shut down.
I’m in a lawsuit involving Amazon for censoring one of my books. They were censoring people who criticized the lockdowns while they were raking in the money from the lockdowns. And unfortunately, President Trump’s White House was colluding with them.
41 percent of black businesses shut down, most of them permanently.
I want to introduce you to somebody. This is Anthony Caldwell. Can you stand Anthony and Yvette? Just wave to people. Anthony Caldwell is from Boston. He was a chef, and a very very successful chef, in this town for 19 years. He saved every penny he had to build their dream, which was that he would have his own restaurant by the time he was 50 years old. It’s called 50 Kitchen.
It was the hottest spot in Dorchester, which is the town that my grandfather and grandmother lived. They were turning away crowds. Boston magazine called them a culinary genius.
It was a mix of Asian fusion food with soul food. Then the lockdowns came. Anthony told me his customers were gone. He was looking out the window staring out all day with this with the chairs stacked in his dining room and no customers.
The federal government gave him $17,000. They told him he had to spend it all within eight weeks or he had to pay it back. He said to me, how do I spend $17,000 with no customers? He had to let go of seven of his servers.
Finally he kept it open for a year without paying for himself. Then he closed it down and went bankrupt. He now owes $250,000.
That story can be told thousands upon thousands upon thousands of times in black communities all over this country. These lockdowns were a war on the poor and they were a war on American children. According to a Brown University study, children in this country, toddlers, lost 22 IQ points. One-third of children, throughout their school careers, are going to need remedial education.
Children all over the country miss their milestones. What is the CDC’s response? The CDC five months ago revised its milestones. Now a child no longer is expected to walk at one year. Now they have 18 months. And now a child does not have to have 50 words in 24 months. It’s 30 months. Instead of fixing the problem they are trying to cover it up.
The only indicia of social decline that actually improved during the pandemic was child abuse. It dropped but it was just an artifact of data gathering. Why? Because child abuse is reported by the schools. And the schools were closed. The kids were locked at home with their abusers. 55 percent of teenagers report being abused during the lockdowns, 13 percent physically abused.
It was also the schools were the places where people had hot lunches, where kids stayed at home watching screens or eating potato chips. We gained on average 29 pounds. And it was the obesity that killed you from Covid. We did the inverse of what you want to do.
Public Health authorities went to every black neighborhood and locked down the basketball courts so people couldn’t exercise. They could not even get in the sunlight. If they couldn’t lock down the courts, they removed the basketball hoops.
All of us suffered from it but the black communities, the minority communities, suffered the worst. 25 percent of teenagers reported going hungry. 20 percent had suicide ideation. 9 percent tried to commit suicide. Suicide is now the largest cause of death among black children.
These are just some of the horrifying data. And I could go on and on. But I’m not going to.
I want to talk about another issue which is the closing down of our rights. Not only did we start censoring people at the very very beginning. Hamilton and Adams said they put freedom of expression as the First Amendment because all the other rights depend on that. If you give a government license to silence its critics, it now has license for any atrocity.
So as soon as they knew they could censor us, they went after every other part of the First Amendment, including the freedom of worship. They closed every Church in this country without any scientific citation for a year.
They did it without any notice or comment. Rule-making democracy was simply abolished. Then they went after freedom of assembly. They told us we had to social distance. They went after our property rights in the Fifth Amendment. They closed 3.3 million businesses with no due process and no just compensation.
They got rid of Seventh Amendment jury trials. They said that if you’re involved with the countermeasure, no matter how egregious the injury you cause, no matter how negligent you are, no matter how reckless, you cannot be sued.
Here’s what the Seventh Amendment says. It says that no American shall be deprived the right of a trial before a jury of his peers in cases or controversies exceeding 25 dollars.
There’s no pandemic exception.
And by the way, the Framers knew all about pandemics. There were two epidemics during the Revolutionary War. One was a malaria epidemic in Virginia that decimated General Washington’s troops. There was a smallpox epidemic that disabled the armies of New England at the very moment they conquered Quebec. They had to withdraw. Otherwise today Canada would be part of the United States.
Between the end of the Revolution and the ratification of the Constitution, over nine years, there were epidemics in every city that killed tens of thousands of people. There were cholera epidemics, malaria epidemics, and smallpox epidemics, in Philadelphia, New York, Boston, and so on.
They knew all about them. But they didn’t put that in the Constitution. The Constitution was built for Hard Times. It wasn’t built for the easy times. During the Civil War, there were 659 000 soldiers who died. That’s the equivalent of 7,200,000 today.
Our country was this close from falling apart. It was a much worse crisis than this pandemic. Yet when Lincoln tried to prohibit habeas corpus, the court said you don’t. You can’t do that. You cannot do it. It doesn’t matter how bad the crisis is. You cannot do it. It’s in the Constitution. It’s the heart and soul of our country.
President Trump said well these bureaucrats came at him from every side. They were all telling him what he had to do. He had the right instincts. He knew that he shouldn’t close down the country. But he did it. He got rolled by his bureaucracy.
I’m going to tell you a quick story. During the Cuban Missile Crisis the ex-com committee – which was all the intelligence officials and military officials, and my father was on there, and so was Bob McNamara but so those are the exceptions – but all of the the doyens and the gurus, the old gray men…and the generals from the Joint Chiefs, all said we got to go in and bomb the the missile sites in Cuba.
My uncle said to them: well wait a minute. What’s going to happen? Who is on those gun crews? Are those Cubans or are they Russians? They said we don’t know. And he said, well if they’re Russians and we kill Russians, isn’t Russia then going to have to go into Berlin? They said, we don’t think they’ll do that.
My uncle said I want to see the aerial photographs.He looked at the aerial photographs and he said who is on the Cuban side? Who gives permission to fire? Does it come from Russia or does it come from Fidel? From the individual gun crews? Because if it comes from Fidel, he is going to fire. If it comes from the individual gun crews, then you’re putting the fate of the world in the hands of those commanders, 64 men.
They didn’t know. He said we’re not doing it. And he did something else.
All I’m saying is you need a president at this time in history who can stand up to his bureaucracy. The bureaucracies are owned by the industries. I’m talking about the NIH and EPA and CDC and FDA and DOC and USDA…..
Our food is terrible because the food companies and the pesticide companies own USDA. We’re in constant wars because the military industrial complex, the big contractors own CIA.
Now, I want to make this clear. I do not. Believe that everybody at the CIA is a bad person. My daughter in law, Amaryllis, who is one of the top officers on this campaign and her entire career is a clandestine agent for the CIA as a spy in the weapons of mass destruction programs in some of the most dangerous parts of the earth. And I have never met anybody with such courage. And that’s how most of the 22,000 people at CIA. They’re people who are patriots or people who are good public servants. And they’re people of enormous courage and idealism, as the same with most of our agencies.
The problem is the people who end up rising in those agencies generally are people who are in the tank with industry. And that’s how they get corrupted. And one of the things that I can do, I think better than any other political candidate, is I know how to fix something because I’ve spent so much time litigating and studying these agencies.
Very quickly, I want to just talk about the chronic disease epidemic, because to me, arguably, this is the worst attack on the middle class in this country. We have the worst health care system in the United States of America. What do I mean by that? I mean that we more on health care by far than any other country, and we have the worst health outcomes. We spend $4.3 trillion annually on health, 4.3 trillion, and about 84% of that goes to treating chronic disease.
And why is that? Because America has the highest chronic disease burden in the world. And we didn’t, we didn’t always in 1950’s and 60’s we had a really healthy population. We had only 6% of our people, of our citizens or children, had chronic disease. In 1988, that became 12.8%. So it doubled. Today, by 2006 it was 54%.
We have the sickest generation in American history. We have the sickest children on earth in this country. And by chronic disease, what do I mean? I mean obesity, but more importantly, neurological diseases, neurodevelopmental, A.D.D., ADHD, speech, language ticks, Tourette’s syndrome, ASD, and autism. Autism went from one in every 10,000 people in my generation to one in every 34 kids today.
Now, one of the talking points that the industry and their crooked legislative regulators will say is, oh, well, we just started noticing it for the first time. Missing autism is like missing a train wreck. So, it’s an absurd—but more importantly. There is study after study after study that shows that this epidemic is real. It is not the result of changing diagnostic criteria. It is not the result of better recognition.
It is an epidemic. And it’s common sense because if it was changing diagnostic criteria, you’d see people my age with full blown autism, 69 years old. I have never seen somebody my age with full blown autism. I mean, stimming, toe walking, head banging, nonverbal, non-toilet trained.
And I’ve been around at the spear tip of people with intellectual disabilities my whole life. My aunt founded Special Olympics. I worked in it from when I was a kid. My cousin, my dear cousin, Anthony Shriver, is the founder of Best Buddies. This has been in the DNA. I spent 200 hours working at (inaudible) home for the retarded in Hudson Valley when I was a teenager. I just I haven’t seen it somebody my age who looks like that and yet my kids’ schools—There are many, many children who look like that.
And why aren’t we asking the question: What happened? And by the way there was a report that came out a couple of weeks ago that shows that the cost of autism alone in the American economy will be—just of caring for people. As this group now ages, it will be $1,000,000,000,000 a year by 2040. The Congress said to EPA, tell us what year the autism epidemic began, and the EPA is a captive agency, but it’s captive by the oil, coal and pesticide industry, not by pharma.
So it actually came out with an honest study. And EPA said it’s a red line, 1989. Oh, something happened in 1989. And we know that it is an environmental insult because genes don’t cause epidemics. And the only thing is we just have to figure out what it is. There’s a limited number of culprits, of chemical toxins that became ubiquitous around 1989. And so, you know, that’s something that NIH is a $42 billion budget.
And by the way, it wasn’t just those neurological disorders that started then, it was all these autoimmune diseases. If you’re my age, you never saw anybody with rheumatoid arthritis or juvenile diabetes when you were younger. You know, the allergic diseases, food allergies, peanut allergies and eczema, anaphylaxis, which are ubiquitous, are at 27% of our school budgets are now going to special education.
This is crippling to the middle class in this country. And we need to figure out what it is. Let me tell you this when I am the President of the United States, I am going to end the chronic disease epidemic in this country. And if I have not significantly dropped the level of chronic disease in our children by the end of my first term, I do not want to get reelected.