
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
CORONA Main Coronavirus thread
- Thread starter Heliobas Disciple
- Start date
-
- Tags
- coronavirus
psychgirl
TB Fanatic
We’ll see how this goes.
Honestly, I’m skeptical of anyone even pays attention. Didn’t another country already try that?
Heliobas Disciple
TB Fanatic
Just posting the summary and intro to this long article authored by Fauci and two others. I will post two substacks discussing it following this post.
 (fair use applies)
(fair use applies)
Rethinking next-generation vaccines for coronaviruses, influenzaviruses, and other respiratory viruses
David M. Morens
Jeffery K. Taubenberger
Anthony S. Fauci
Volume 31, ISSUE 1, P146-157, January 11, 2023
Until the emergence of COVID-19, influenza had for many decades been the deadliest vaccine-preventable viral respiratory disease, one for which only less than suboptimal vaccines are available. Surprisingly, little has changed with influenza vaccines since 1957 when they were first administered in US national vaccination programs. Over the years, influenza vaccines have never been able to elicit durable protective immunity against seasonal influenza virus strains, even against non-drifted strains. Although current influenza vaccines reduce the risk of severe disease, hospitalization, and death to some degree, their effectiveness against clinically apparent infection is decidedly suboptimal, ranging from 14% to 60% over the past 15 influenza seasons.
Furthermore, the duration of vaccine-elicited immunity is measured only in months. Current vaccines require annual re-vaccination with updated formulations that are frequently not precisely matched to circulating virus strains.Although annual influenza vaccinations are strongly recommended for most of the general public and especially for persons in high-risk groups, including the elderly, those with chronic diseases, and pregnant women, vaccine acceptance by the general public is not ideal. As of 2022, after more than 60 years of experience with influenza vaccines, very little improvement in vaccine prevention of infection has been noted. As pointed out decades ago, and still true today, the rates of effectiveness of our best approved influenza vaccines would be inadequate for licensure for most other vaccine-preventable diseases.
Even decades-long efforts to develop better, so-called “universal” influenza vaccines—vaccines that would create more broadly protective immunity, preferably lasting over longer time periods—have not yet resulted in next-generation, broadly protective vaccines, although a large number of experimental vaccines are in preclinical or early clinical development.
During the COVID-19 pandemic, the rapid development and deployment of SARS-CoV-2 vaccines has saved innumerable lives and helped to achieve early partial pandemic control.
However, as variant SARS-CoV-2 strains have emerged, deficiencies in these vaccines reminiscent of influenza vaccines have become apparent. The vaccines for these two very different viruses have common characteristics: they elicit incomplete and short-lived protection against evolving virus variants that escape population immunity.
Considering that vaccine development and licensure is a long and complex process requiring years of preclinical and clinical safety and efficacy data, the limitations of influenza and SARS-CoV-2 vaccines remind us that candidate vaccines for most other respiratory viruses have to date been insufficiently protective for consideration of licensure, including
parainfluenzaviruses, endemic coronaviruses, and many other “common cold” viruses that cause significant morbidity and economic loss.
More than 50 years ago, the development of successful vaccines against some of the most important respiratory viruses, including measles, mumps, and rubella, led to the hope that vaccines could soon be developed for all other respiratory viruses. However, natural infections with these three vaccine-controlled respiratory viruses, as well as smallpox and varicella zoster virus (VZV), are not representative of infections caused by most respiratory viruses. They differ in at least three critically important ways that are related to their successful control with vaccines (Table 1):
similar to studies of influenza RNAemia.
As a result, the non-systemically replicating respiratory viruses, apparently including SARS-CoV-2, tend to repeatedly re-infect people over their lifetimes without ever eliciting complete and durable protection.
Another important factor to consider is that although RNA viruses share a similar inherent RNA-dependent RNA polymerase error rate different viruses (and different open reading frames within their genomes) differ in their tolerance for mutation. Mutational constraints can be related to frequent overlapping open reading frames or functional constraints on the acquisition of nonsynonymous mutations as is the case, for example, with measles virus.
In contrast, the external influenza A virus hemagglutinin and neuraminidase proteins are comparatively plastic, and positively selected nonsynonymous mutations result in immunologically significant antigenic drift, by the acquisition of nonsynonymous mutations in antigenic epitopes, as well as by altering the N-linked glycosylation patterns.
Rapid antigenic drift affects the control of annual influenza epidemics and complicates the effort to produce broadly protective, “universal” influenza vaccines. The SARS-CoV-2 spike protein has shown a similar plasticity, with the emergence of multiple variants with altered antigenicity that has complicated its control through current vaccination strategies.
Although rapid evolution of antigenically variable mucosal viruses like influenza A viruses and SARS-CoV-2 complicate next-generation vaccine design, other mucosal-only respiratory viruses, such as RSV, have shown much less antigenic plasticity; however, it still causes repeated infections over a lifetime without the development of long-term protective immunity.
Thus, although genetic and antigenic variability of viruses like influenza and SARS-CoV-2 make vaccine design more challenging, these factors by themselves cannot fully explain the lack of elicitation of long-term protective immunity against other respiratory mucosal viruses like the more phenotypically stable RSV.
Taking all of these factors into account, it is not surprising that none of the predominantly mucosal respiratory viruses have ever been effectively controlled by vaccines. This observation raises a question of fundamental importance: if natural mucosal respiratory virus infections do not elicit complete and long-term protective immunity against reinfection, how can we expect vaccines, especially systemically administered non-replicating vaccines, to do so? This is a major challenge for future vaccine development, and overcoming it is critical as we work to develop “next-generation” vaccines.
Key challenges (summarized in Table 2) are discussed below, along with ways to confront them in the pursuit of new and improved vaccines for respiratory viruses.
[SNIP - GO TO LINK FOR MUCH LONGER ARTICLE]
Rethinking next-generation vaccines for coronaviruses, influenzaviruses, and other respiratory viruses
Despite the successful deployment of vaccines during the SARS-CoV2 pandemic, viruses replicating in the respiratory mucosal environment continue to present a particular challenge for developing effective vaccines with strong protection. Morens et al. discuss approaches that need to be...
www.cell.com
Rethinking next-generation vaccines for coronaviruses, influenzaviruses, and other respiratory viruses
David M. Morens
Jeffery K. Taubenberger
Anthony S. Fauci
Volume 31, ISSUE 1, P146-157, January 11, 2023
Summary
Viruses that replicate in the human respiratory mucosa without infecting systemically, including influenza A, SARS-CoV-2, endemic coronaviruses, RSV, and many other “common cold” viruses, cause significant mortality and morbidity and are important public health concerns. Because these viruses generally do not elicit complete and durable protective immunity by themselves, they have not to date been effectively controlled by licensed or experimental vaccines. In this review, we examine challenges that have impeded development of effective mucosal respiratory vaccines, emphasizing that all of these viruses replicate extremely rapidly in the surface epithelium and are quickly transmitted to other hosts, within a narrow window of time before adaptive immune responses are fully marshaled. We discuss possible approaches to developing next-generation vaccines against these viruses, in consideration of several variables such as vaccine antigen configuration, dose and adjuventation, route and timing of vaccination, vaccine boosting, adjunctive therapies, and options for public health vaccination polices.Introduction
Effective vaccines and vaccine prevention strategies against endemic and emerging respiratory viruses are of critical importance, as these pathogens kill as many as 5 million people worldwide every year. For example, over the past decade, influenza killed 12,000–52,000 people in the United States each year and ranks among the leading causes of years of productive life lost (YPLL). Endemic respiratory viruses such as respiratory syncytial virus (RSV) and the parainfluenzaviruses take many additional lives, and previously unrecognized respiratory viruses such as SARS-CoV-2, the cause of COVID-19, have emerged unexpectedly. SARS-CoV-2 thus far has killed more than one million people in the United States. The increasing frequency of emergences of such pandemic respiratory viruses may be a key feature of a new pandemic era, forcing us to consider anew the state of respiratory virus vaccinology.Until the emergence of COVID-19, influenza had for many decades been the deadliest vaccine-preventable viral respiratory disease, one for which only less than suboptimal vaccines are available. Surprisingly, little has changed with influenza vaccines since 1957 when they were first administered in US national vaccination programs. Over the years, influenza vaccines have never been able to elicit durable protective immunity against seasonal influenza virus strains, even against non-drifted strains. Although current influenza vaccines reduce the risk of severe disease, hospitalization, and death to some degree, their effectiveness against clinically apparent infection is decidedly suboptimal, ranging from 14% to 60% over the past 15 influenza seasons.
Furthermore, the duration of vaccine-elicited immunity is measured only in months. Current vaccines require annual re-vaccination with updated formulations that are frequently not precisely matched to circulating virus strains.Although annual influenza vaccinations are strongly recommended for most of the general public and especially for persons in high-risk groups, including the elderly, those with chronic diseases, and pregnant women, vaccine acceptance by the general public is not ideal. As of 2022, after more than 60 years of experience with influenza vaccines, very little improvement in vaccine prevention of infection has been noted. As pointed out decades ago, and still true today, the rates of effectiveness of our best approved influenza vaccines would be inadequate for licensure for most other vaccine-preventable diseases.
Even decades-long efforts to develop better, so-called “universal” influenza vaccines—vaccines that would create more broadly protective immunity, preferably lasting over longer time periods—have not yet resulted in next-generation, broadly protective vaccines, although a large number of experimental vaccines are in preclinical or early clinical development.
During the COVID-19 pandemic, the rapid development and deployment of SARS-CoV-2 vaccines has saved innumerable lives and helped to achieve early partial pandemic control.
However, as variant SARS-CoV-2 strains have emerged, deficiencies in these vaccines reminiscent of influenza vaccines have become apparent. The vaccines for these two very different viruses have common characteristics: they elicit incomplete and short-lived protection against evolving virus variants that escape population immunity.
Considering that vaccine development and licensure is a long and complex process requiring years of preclinical and clinical safety and efficacy data, the limitations of influenza and SARS-CoV-2 vaccines remind us that candidate vaccines for most other respiratory viruses have to date been insufficiently protective for consideration of licensure, including
parainfluenzaviruses, endemic coronaviruses, and many other “common cold” viruses that cause significant morbidity and economic loss.
More than 50 years ago, the development of successful vaccines against some of the most important respiratory viruses, including measles, mumps, and rubella, led to the hope that vaccines could soon be developed for all other respiratory viruses. However, natural infections with these three vaccine-controlled respiratory viruses, as well as smallpox and varicella zoster virus (VZV), are not representative of infections caused by most respiratory viruses. They differ in at least three critically important ways that are related to their successful control with vaccines (Table 1):
- (1) after first replicating mucosally, these systemic respiratory viruses all cause significant viremia that seeds an enormous number of infectious virions throughout the body, putting them in contact with multiple immune compartments and immune competent cell types,
- (2) they have relatively long incubation periods that reflect initial mucosal replication and the subsequent systemic spread of infectious virions, which allows time for the induction of the full force of adaptive immunity, and
- (3) they elicit long-term or lifetime protective immunity (Table 1).
similar to studies of influenza RNAemia.
As a result, the non-systemically replicating respiratory viruses, apparently including SARS-CoV-2, tend to repeatedly re-infect people over their lifetimes without ever eliciting complete and durable protection.
Another important factor to consider is that although RNA viruses share a similar inherent RNA-dependent RNA polymerase error rate different viruses (and different open reading frames within their genomes) differ in their tolerance for mutation. Mutational constraints can be related to frequent overlapping open reading frames or functional constraints on the acquisition of nonsynonymous mutations as is the case, for example, with measles virus.
In contrast, the external influenza A virus hemagglutinin and neuraminidase proteins are comparatively plastic, and positively selected nonsynonymous mutations result in immunologically significant antigenic drift, by the acquisition of nonsynonymous mutations in antigenic epitopes, as well as by altering the N-linked glycosylation patterns.
Rapid antigenic drift affects the control of annual influenza epidemics and complicates the effort to produce broadly protective, “universal” influenza vaccines. The SARS-CoV-2 spike protein has shown a similar plasticity, with the emergence of multiple variants with altered antigenicity that has complicated its control through current vaccination strategies.
Although rapid evolution of antigenically variable mucosal viruses like influenza A viruses and SARS-CoV-2 complicate next-generation vaccine design, other mucosal-only respiratory viruses, such as RSV, have shown much less antigenic plasticity; however, it still causes repeated infections over a lifetime without the development of long-term protective immunity.
Thus, although genetic and antigenic variability of viruses like influenza and SARS-CoV-2 make vaccine design more challenging, these factors by themselves cannot fully explain the lack of elicitation of long-term protective immunity against other respiratory mucosal viruses like the more phenotypically stable RSV.
Taking all of these factors into account, it is not surprising that none of the predominantly mucosal respiratory viruses have ever been effectively controlled by vaccines. This observation raises a question of fundamental importance: if natural mucosal respiratory virus infections do not elicit complete and long-term protective immunity against reinfection, how can we expect vaccines, especially systemically administered non-replicating vaccines, to do so? This is a major challenge for future vaccine development, and overcoming it is critical as we work to develop “next-generation” vaccines.
Key challenges (summarized in Table 2) are discussed below, along with ways to confront them in the pursuit of new and improved vaccines for respiratory viruses.
[SNIP - GO TO LINK FOR MUCH LONGER ARTICLE]
Heliobas Disciple
TB Fanatic

Dr. Fauci Knew Covid Vaccines Would Never Give Us Herd Immunity
Is Tony trying to "explain his mistakes" and ask for pandemic amnesty?
 igorchudov.substack.com
igorchudov.substack.com
Dr. Fauci Knew Covid Vaccines Would Never Give Us Herd Immunity
Is Tony trying to "explain his mistakes" and ask for pandemic amnesty?
Igor Chudov
Feb 6
A new scientific study is out, and Anthony Fauci co-authored it.
What is remarkable about that study is the derogatory language Fauci et al. employ towards influenza and Covid vaccines.
Until the emergence of COVID-19, influenza had for many decades been the deadliest vaccine-preventable viral respiratory disease, one for which only less than suboptimal vaccines are available.
Less than suboptimal vaccines is a term that leaves little to the imagination. Suboptimal means “not good.” Less than suboptimal means “useless at best.”
The article presumably discusses “next-generation vaccines.” However, the next-generation talk is empty and speculative, without specific mentions of any new technology that Dr. Fauci and his coauthors can recommend. The substance of the Cell article only explains why current influenza vaccines cannot prevent influenza and why Covid vaccines cannot prevent Covid.
Although current influenza vaccines reduce the risk of severe disease, hospitalization, and death to some degree, their effectiveness against clinically apparent infection is decidedly suboptimal, ranging from 14% to 60% over the past 15 influenza seasons.1 Furthermore, the duration of vaccine-elicited immunity is measured only in months. Current vaccines require annual re-vaccination with updated formulations that are frequently not precisely matched to circulating virus strains.8 Although annual influenza vaccinations are strongly recommended for most of the general public and especially for persons in high-risk groups, including the elderly, those with chronic diseases, and pregnant women, vaccine acceptance by the general public is not ideal.9
As of 2022, after more than 60 years of experience with influenza vaccines, very little improvement in vaccine prevention of infection has been noted.
The above sounds like this article by yours truly:
After retiring, Fauci does not mince words on Covid vaccines either:
During the COVID-19 pandemic, the rapid development and deployment of SARS-CoV-2 vaccines has saved innumerable lives and helped to achieve early partial pandemic control.
However, as variant SARS-CoV-2 strains have emerged, deficiencies in these vaccines reminiscent of influenza vaccines have become apparent. The vaccines for these two very different viruses have common characteristics: they elicit incomplete and short-lived protection against evolving virus variants that escape population immunity.
Fauci Knew Why Covid Vaccine Could Never WorkFauci and his co-authors explain why Covid vaccine had no chance of working.
First, he asks a question that many vaccine skeptics brought up many times before:
This observation raises a question of fundamental importance: if natural mucosal respiratory virus infections do not elicit complete and long-term protective immunity against reinfection, how can we expect vaccines, especially systemically administered non-replicating vaccines, to do so?
Then Tony goes on to explain why the respiratory nature of Sars-Cov-2 does not lead to even a possibility of encountering a bloodborne immune response.
In stark contrast, the non-systemic respiratory viruses such as influenza viruses, SARS-CoV-2, and RSV tend to have significantly shorter incubation periods (Table 1) and rapid courses of viral replication. They replicate predominantly in local mucosal tissue, without causing viremia, and do not significantly encounter the systemic immune system or the full force of adaptive immune responses, which take at least 5–7 days to mature, usually well after the peak of viral replication and onward transmission to others. SARS-CoV-2 “RNAemia” (circulation of viral RNA in the bloodstream, as is seen with most mucosal respiratory virus infections, as distinct from viremia, in which infectious viruses can be cultured from the blood), has been reported, and RT-PCR levels of viral RNA have been linked to severe disease,23,24 similar to studies of influenza RNAemia.25,26 As a result, the non-systemically replicating respiratory viruses, apparently including SARS-CoV-2,13,14,15 tend to repeatedly re-infect people over their lifetimes without ever eliciting complete and durable protection.27
Regrettably, many of my unvaccinated readers report repeat infections with Covid-19. Even though I have had only one Covid so far, in Nov 2020, I am very cognizant that my natural immunity is far from perfect.
Another important factor to consider is that although RNA viruses share a similar inherent RNA-dependent RNA polymerase error rate,28 different viruses (and different open reading frames within their genomes) differ in their tolerance for mutation. Mutational constraints can be related to frequent overlapping open reading frames28 or functional constraints on the acquisition of nonsynonymous mutations as is the case, for example, with measles virus.29 In contrast, the external influenza A virus hemagglutinin and neuraminidase proteins are comparatively plastic, and positively selected nonsynonymous mutations result in immunologically significant antigenic drift,30,31 by the acquisition of nonsynonymous mutations in antigenic epitopes, as well as by altering the N-linked glycosylation patterns.32 Rapid antigenic drift affects the control of annual influenza epidemics8 and complicates the effort to produce broadly protective, “universal” influenza vaccines. The SARS-CoV-2 spike protein has shown a similar plasticity, with the emergence of multiple variants with altered antigenicity33 that has complicated its control through current vaccination strategies.34
Great, right? Fauci and his “science” are still injecting the original Wuhan strain-encoding mRNA, well into the fifth calendar year of the pandemic, while being fully aware that mutations have rendered those injections to be “less than suboptimal.” (the bivalent booster contains equal doses of Ba.5 and Wuhan variant-encoding mRNA)
Fauci Again Shows Knowledge of Immune Tolerance
Dr. Fauci shows great familiarity with “immune tolerance,” a condition affecting recipients of multiple mRNA vaccines:
The terms “disease tolerance” and “immune tolerance” refer to the still-incompletely characterized but distinct category of mammalian immune defense mechanisms that allow hosts to “accept” infection and other antigenic stimuli to optimize survival (reviewed in Medzhitov et al. and Iwasaki et al.). Because humans inhale and ingest enormous quantities of exogenous proteins with every breath and mouthful, the respiratory and gastrointestinal immune compartments have evolved to deal with continual and massive antigenic assaults from the outside world. (Immune responses to viral infection of the gastrointestinal mucosa have recently been reviewed, and are not discussed here.) Inhaled and ingested proteins must be identified and either tolerated or attacked and eliminated.
This is not the first time we caught Fauci being aware of immune tolerance and yet continuing to push tolerance-inducing mRNA Covid vaccines:
Fauci then speculates on what can be done to make a “new generation of vaccines.” His and his coauthors’ talk is very lame and exposes them as quacks who want to try out anything without a theoretical basis.Appreciate the lack of any sense this passage makes:
For example, during times of significant viral circulation within human populations, can better protection be achieved with repeat dosing, or by sequential mucosal and systemic vaccination? Is frequent re-boosting a viable vaccine option, e.g., via self-administered home nasal vaccines? Also to be considered are possible ancillary roles for prophylactic antivirals, including “programmable antivirals” targeting conserved structures, antibodies, including therapeutic IgA and innate immunity stimulators as adjuncts to imperfect vaccines. It remains to be seen if vaccination and prophylaxis can be effectively combined at the population level.
It is disheartening that, during a man-made pandemic still taking hundreds of lives daily and still playing a role in excess mortality, we are led by people officially pushing for vaccines that they know to be “less than sub-optimal.”Fauci Knew Covid Vaccine Would Never Stop the Pandemic
Fauci explained in the study cited above why a vaccine-induced blood (humoral) response to Sars-Cov-2 would never stop respiratory infections. And yet, he lied to us for THREE YEARS about how vaccines would be the key to “getting out of the pandemic” and getting to herd immunity.
Witness this video from 2020, where Fauci promises us herd immunity:
It is very regrettable that our health leaders, realizing that Covid vaccine could never possibly stop the Covid pandemic, preached to us that we could reach herd immunity.
As a result, we have a dumpster fire of a pandemic and excess mortality not even explainable by official Covid death counts.
Tony, meanwhile, is collecting hefty “speaking engagement” fees:

Will Dr. Fauci Admit “Mistakes” and Ask for Amnesty?
Why would Dr. Fauci lie to us about “herd immunity” when he knew, based on very basic properties of coronaviruses, that sterilizing immunity was impossible?
Is his article a clever way to prepare us for him asking for a “pandemic amnesty” and “recognizing his mistakes”?
How can we accept his actions as “mistakes” when he knew he was lying to us in furtherance of his goals? A mistake implies honesty, after all.
Let us know what you think!
Heliobas Disciple
TB Fanatic
Fauci now today in a published paper (CELL) says the COVID gene injection vaccine & similar respiratory vaccines were problematic to begin & likely DO NOT WORK & CANNOT work, NOT as is; What? AMNESTY?
I need to take up very heavy drinking to keep up with the absurdity & duplicity of this guy; Fauci is likely the most inept & destructive health official in America's history, he causes DEATH!
Fauci now today in a published paper (CELL) says the COVID gene injection vaccine & similar respiratory vaccines were problematic to begin & likely DO NOT WORK & CANNOT work, NOT as is; What? AMNESTY?
I need to take up very heavy drinking to keep up with the absurdity & duplicity of this guy; Fauci is likely the most inept & destructive health official in America's history, he causes DEATH!
Dr. Paul Alexander
4 hr ago

TITLE:
Rethinking next-generation vaccines for coronaviruses, influenza viruses, and other respiratory viruses
This CELL paper by Fauci is actually a real headache for him and implicates him in very destructive activities. I think it can help incarcerate him, Francis Collins, Bourla, Bancel, Walensky etc. Why? They know what they did, they know the vaccine failed day one! They knew about the risk of original antigenic sin (immune imprinting, immune fixation), paradoxical priming (auto-immunity), viral immune escape, and antibody-dependent enhancement of infection and/or disease.
There were never any randomized controlled trials to show the shot reduced hospitalization, death etc. and the observational studies have been poorly conducted, short duration, small sample sizes, small event outcome numbers, did not control effectively for natural immunity across comparative groups, nor early treatment, nor baseline differences, nor co-morbidities, and did not control for the ‘healthy vaccinee effect bias’ where vaccinated people are typically healthier to begin with.
To date, we have no definitive evidence that these shots ever reduced hospitalizations, severity, death. None.
Is Fauci now pleading for amnesty like Oster and this eugenics proponent and time fame grifter Kevin Bass? This paper tells us that vaccines on the whole CANNOT work against respiratory infections like common cold, flu, COVID. CANNOT. And those bringing it know and knew this, including Fauci. Fauci and Francis Collins knew that the flu vaccine was pure garbage and does not work, and that it is an annual lie perpetrated on people, especially to elderly.
This CELL paper by Fauci really tells us that the nation and world were taken on a Clown car ride by CDC, FDA, NIH etc. and that they are all frauds and malfeasants for the damage they have done. Fauci and Bourla and Bancel and Francis Collins pushed vaccines that drive and drove immune tolerance and damaged underlying immune systems. They knew. I repeat, the COVID gene injections must be removed from market and all players involved, all, from mRNA to vaccine, must be thoroughly investigated and must be jailed once definitive wrong is shown!
SOURCE:
https://www.cell.com/cell-host-microbe/fulltext/S1931-3128(22)00572-8?utm_source=substack&utm_medium=email#%20
Let me begin this mind-blowing review of this CELL paper and I will highlight in italics, lines or passages that are important:
Abstract
Viruses that replicate in the human respiratory mucosa without infecting systemically, including influenza A, SARS-CoV-2, endemic coronaviruses, RSV, and many other “common cold” viruses, cause significant mortality and morbidity and are important public health concerns. Because these viruses generally do not elicit complete and durable protective immunity by themselves, they have not to date been effectively controlled by licensed or experimental vaccines. In this review, we examine challenges that have impeded development of effective mucosal respiratory vaccines, emphasizing that all of these viruses replicate extremely rapidly in the surface epithelium and are quickly transmitted to other hosts, within a narrow window of time before adaptive immune responses are fully marshaled. We discuss possible approaches to developing next-generation vaccines against these viruses, in consideration of several variables such as vaccine antigen configuration, dose and adjuventation, route and timing of vaccination, vaccine boosting, adjunctive therapies, and options for public health vaccination polices.
Because these viruses generally do not elicit complete and durable protective immunity by themselves, they have not to date been effectively controlled by licensed or experimental vaccines.
Did you read this statement by Fauci in the abstract and thus immediately, how this opens key questions about the COVID vaccine?
Until the emergence of COVID-19, influenza had for many decades been the deadliest vaccine-preventable viral respiratory disease, one for which only less than suboptimal vaccines are available. Over the years, influenza vaccines have never been able to elicit durable protective immunity against seasonal influenza virus strains, even against non-drifted strains…their effectiveness against clinically apparent infection is decidedly suboptimal, ranging from 14% to 60% over the past 15 influenza seasons.
What about that, does not give you any confidence in the flu shot, does it?
During the COVID-19 pandemic, the rapid development and deployment of SARS-CoV-2 vaccines has saved innumerable lives and helped to achieve early partial pandemic control. However, as variant SARS-CoV-2 strains have emerged, deficiencies in these vaccines reminiscent of influenza vaccines have become apparent. The vaccines for these two very different viruses have common characteristics: they elicit incomplete and short-lived protection against evolving virus variants that escape population immunity.
Basically the COVID vaccine is junk.
In stark contrast, the non-systemic respiratory viruses such as influenza viruses, SARS-CoV-2, and RSV tend to have significantly shorter incubation periods (Table 1) and rapid courses of viral replication. They replicate predominantly in local mucosal tissue, without causing viremia, and do not significantly encounter the systemic immune system or the full force of adaptive immune responses, which take at least 5–7 days to mature, usually well after the peak of viral replication and onward transmission to others. SARS-CoV-2 “RNAemia” (circulation of viral RNA in the bloodstream, as is seen with most mucosal respiratory virus infections, as distinct from viremia, in which infectious viruses can be cultured from the blood), has been reported, and RT-PCR levels of viral RNA have been linked to severe disease, similar to studies of influenza RNAemia. As a result, the non-systemically replicating respiratory viruses, apparently including SARS-CoV-2, tend to repeatedly re-infect people over their lifetimes without ever eliciting complete and durable protection.
Here Fauci tells you in his own words that the systemic vaccinal antibodies (adaptive response) e.g. circulating IgG (neutralizing) have near zero chance of bumping up against virus residing in the respiratory mucosal layers (in nostrils, upper respiratory tract etc.). In other words, a vaccine-induced humoral response (in your blood stream after leaving injection site) cannot abrogate respiratory infections.
Taking all of these factors into account, it is not surprising that none of the predominantly mucosal respiratory viruses have ever been effectively controlled by vaccines. This observation raises a question of fundamental importance: if natural mucosal respiratory virus infections do not elicit complete and long-term protective immunity against reinfection, how can we expect vaccines, especially systemically administered non-replicating vaccines, to do so?
Again, Fauci, this after helping mandate these fraud injections on millions of people, is saying how could we expect vaccines like the COVID vaccine to work? It is administered systemically (deltoid muscle and vaccinal antibodies enters the systemic circulation) while the virus lands in the mucosa (nose mouth etc.). In short, they could have never worked and Bhakdi said this from day one!
Another important factor to consider is that although RNA viruses share a similar inherent RNA-dependent RNA polymerase error rate, different viruses (and different open reading frames within their genomes) differ in their tolerance for mutation. Mutational constraints can be related to frequent overlapping open reading frames or functional constraints on the acquisition of nonsynonymous mutations as is the case, for example, with measles virus. In contrast, the external influenza A virus hemagglutinin and neuraminidase proteins are comparatively plastic, and positively selected nonsynonymous mutations result in immunologically significant antigenic drift, by the acquisition of nonsynonymous mutations in antigenic epitopes, as well as by altering the N-linked glycosylation patterns. Rapid antigenic drift affects the control of annual influenza epidemics and complicates the effort to produce broadly protective, “universal” influenza vaccines. The SARS-CoV-2 spike protein has shown a similar plasticity, with the emergence of multiple variants with altered antigenicity that has complicated its control through current vaccination strategies.
So Fauci is saying here that there are extensive mutations and thus a mismatch between induced vaccinal antibodies and the circulating sub-variants. Then why do and did they push vaccine that cannot work? For example, the now failed bivalent booster (contains original Wuhan strain and BA.5 sub-variant clade that is not predominant now e.g. XBB 1.5 is). Same with influenza vaccine. Failures. Then why force it and lie to the public?
The terms “disease tolerance” and “immune tolerance” refer to the still-incompletely characterized but distinct category of mammalian immune defense mechanisms that allow hosts to “accept” infection and other antigenic stimuli to optimize survival (reviewed in Medzhitov et al. and Iwasaki et al.)…The immunologic “Faustian bargain” between tolerance versus infection control, which permits transient, moderated infection by respiratory agents of low or intermediate pathogenicity to restrain the destructive forces of an immune elimination response may be problematic for vaccine control of respiratory viruses, not only in the local and systemic sensing of vaccine antigens but also in eliciting optimal immune responses.
Did Fauci know about ‘tolerance’ by the immune system and how destructive it could be? You bet he did!
As of 2022, after more than 60 years of experience with influenza vaccines, very little improvement in vaccine prevention of infection has been noted. As pointed out decades ago, and still true today, the rates of effectiveness of our best approved influenza vaccines would be inadequate for licensure for most other vaccine-preventable diseases.
Inspires confidence, does it not?
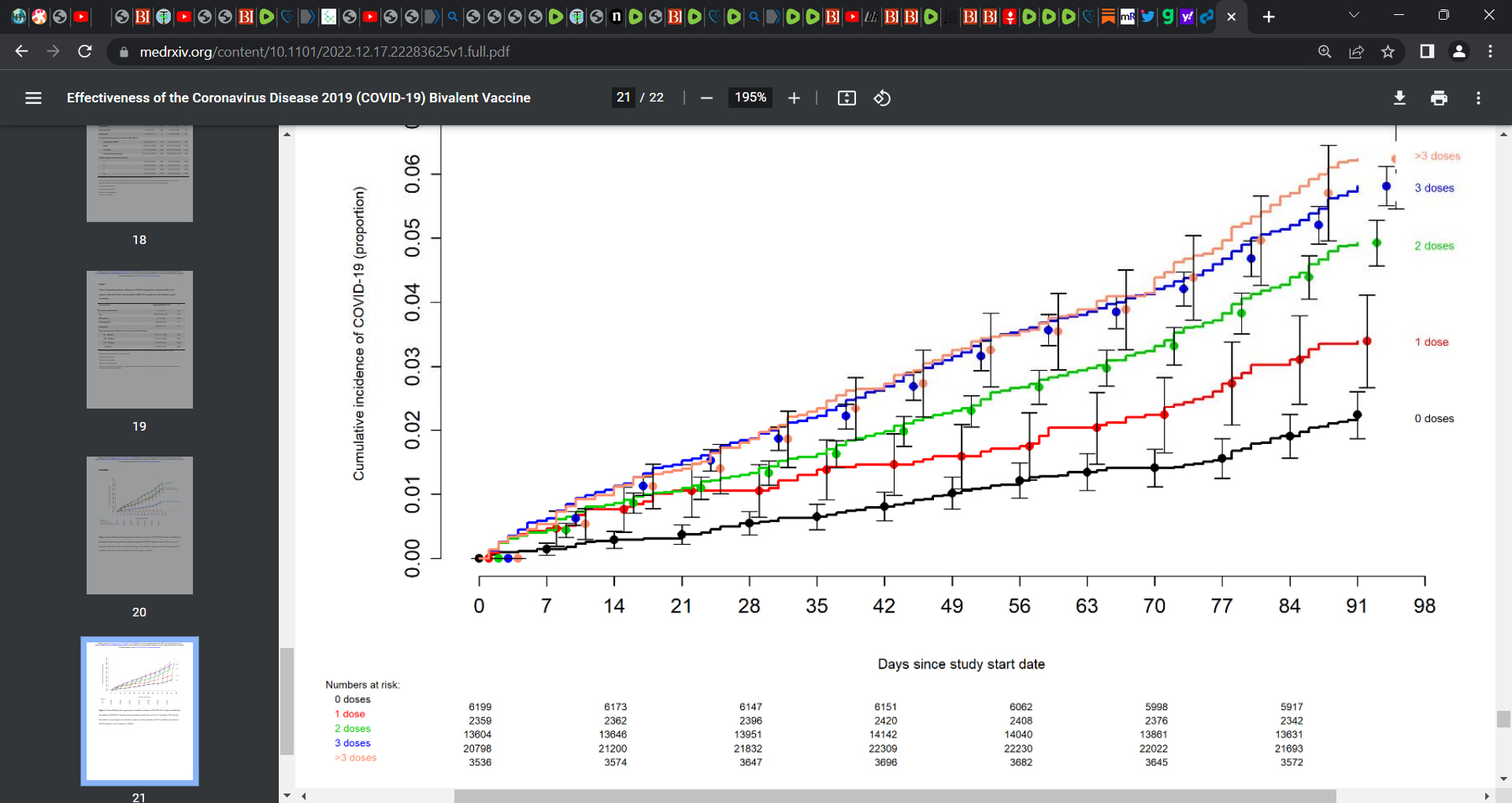
Remember this recent publication by Shrestha et al.? Its showed that the more doses you had, the more COVID and the unvaccinated (0 doses) fared best, see graph below.
https://substackcdn.com/image/fetch/f_auto,q_auto:good,fl_progressive:steep/https://substack-post-media.s3.amazonaws.com/public/images/6842622b-0159-4f42-8071-602e861bb7f7_150x50.png
Heliobas Disciple
TB Fanatic
Another article about the Fauci Cell article.
 www.theepochtimes.com
(fair use applies)
www.theepochtimes.com
(fair use applies)
Just How Hard Were We Trolled?
Jeffrey A. Tucker
February 6, 2023 | Updated: February 8, 2023
Commentary
What if Dr. Anthony Fauci co-authored an article on vaccines that would have gotten you and me blocked and banned at any point in the past three years? That just happened.
His article in Cell—“Rethinking next-generation vaccines for coronaviruses, influenzaviruses, and other respiratory viruses”—says it as plainly as possible: the COVID vaccine did not work because it could not work.
First some review from what we knew before this whole fiasco began.
Vaccines aren’t suitable for coronaviruses. Such respiratory viruses spread and mutate too quickly. This is why there has never been a vaccine for the common cold and why the flu shot is predictably suboptimal. Vaccines can only be sterilizing and contribute to public health when the virus is a stable pathogen such as smallpox and measles. For coronaviruses, there is really only one way forward: better antivirals, therapeutics, and acquired immunity.
The above paragraph has been repeated to me countless times in my life, especially after COVID hit. Every expert was on the same page. There was simply no question about it. Anything that would be called a vaccine would lack the features of vaccines past. It wouldn’t stop infection or transmission, much less end a bad season for respiratory viruses. This is why the FDA has never approved one. It would not and could not make it through trials, especially given the safety risks associated with every vaccine.
Maybe, maybe, there exists the possibility that you can come up with one variant but it isn’t likely to be approved in time to be effective. It might provide temporary protection against severe outcomes from one variant but it will be useless against further mutations. In addition, vaccine-induced protection is not as broad as natural immunity, so it is likely that the person would get infected later. Boosting is likely only to pertain to last month’s mutation, and raises dangers of itself: imprinting the immune system in ways that make it less effective.
Sadly, posting those three paragraphs on social media at any point in the past three years would likely get you censored or even banned. Normal science was suppressed. Common knowledge among experts was verboten. Everything we’ve learned for a century or even two millennia was thrown out. The job of censorship was tasked to a gaggle of ill-educated tech workers obeying the FBI overlords, so they went along.
And here we are two years after the vaccine rollout and the truth is rather well known. The vaccines were an enormous flop. At best. At worst, they caused tremendous amounts of injury and death as compared to any vaccine ever approved for the market. That they were forced on people in many professions—and backed by a Stalinesque media frenzy—is simply incredible. Several cities even locked themselves down for the vaccinated only. Even now, unvaccinated non-Americans cannot travel to the United States, unless they come across the southern border.
And yet only now does Fauci choose to lay out the science that we knew long ago. There is nothing particularly interesting in his article. Only the timing is interesting: following trillions in pharma profits, millions displaced by mandates, and suffering from injury all over the world. Now he says that there was really no chance that the vaccine would be either effective or necessarily safe.
This is a level of trolling that is truly unthinkable and indescribable.
Here is the summary of the article:
“Viruses that replicate in the human respiratory mucosa without infecting systemically, including influenza A, SARS-CoV-2, endemic coronaviruses, RSV, and many other ‘common cold’ viruses, cause significant mortality and morbidity and are important public health concerns. Because these viruses generally do not elicit complete and durable protective immunity by themselves, they have not to date been effectively controlled by licensed or experimental vaccines.
“In this review, we examine challenges that have impeded development of effective mucosal respiratory vaccines, emphasizing that all of these viruses replicate extremely rapidly in the surface epithelium and are quickly transmitted to other hosts, within a narrow window of time before adaptive immune responses are fully marshaled.”
There are profound safety issues to consider too. It takes a very long time to assure that. Fauci says:
“Considering that vaccine development and licensure is a long and complex process requiring years of preclinical and clinical safety and efficacy data, the limitations of influenza and SARS-CoV-2 vaccines remind us that candidate vaccines for most other respiratory viruses have to date been insufficiently protective for consideration of licensure …”
Further, vaccines certainly cannot improve on what even natural immunity cannot do:
“Taking all of these factors into account, it is not surprising that none of the predominantly mucosal respiratory viruses have ever been effectively controlled by vaccines. This observation raises a question of fundamental importance: if natural mucosal respiratory virus infections do not elicit complete and long-term protective immunity against reinfection, how can we expect vaccines, especially systemically administered non-replicating vaccines, to do so?”
This is why the flu vaccines “have never been able to elicit durable protective immunity against seasonal influenza virus strains, even against non-drifted strains…. their effectiveness against clinically apparent infection is decidedly suboptimal, ranging from 14 percent to 60 percent over the past 15 influenza seasons.”
Now, it’s not as if Fauci admits that the vaccine was a complete flop. Of course, he has to engage in the usual incantations of the glories of the COVID vaccination.
“During the COVID-19 pandemic, the rapid development and deployment of SARS-CoV-2 vaccines has saved innumerable lives and helped to achieve early partial pandemic control.”
Note the word “innumerable.” It means there is no number and no possibility of a number. Exactly. Also note “early partial”—weasel words to cover the reality of egregious failure.
If you click through the citation to this dubious claim, it is from April 2021, early in the mutation process when we hardly had any data at all to justify such celebration. Why is Fauci citing a two-year-old piece in defense of the vaccine? Because that’s all there is to cite: two-year-old hagiographies without meaningful data.
How precisely can we account for this fiasco? If they knew, and they did know, how is it that they put us through this horrible upheaval? The most dreadful theory is that they knew for sure that the virus would become endemic through exposure. But the point of “slowing the spread” and “flattening the curve” (lockdowns and masking), while trashing and nearly banning other therapeutics, was to preserve the customer base for the new experimental product.
That product was mRNA which is supposed to be a platform for future vaccines. This is why the Johnson & Johnson vaccine was taken off market.
Under this theory, they wanted to prolong the pandemic for as long as possible so they could collect data on how well the vaccine worked. And they wanted to try it universally, which is why we did not hear much at all about the risk gradient of the vaccine itself. This also accounts for the deliberate drumming up of disease panic and forced distancing.
So let that sink in. They utterly smashed the world as we knew it—violating all human rights—in order to test out a new technology at great profit to themselves. In other words, they treated us all as lab rats.
An entire generation of politicians needs to be toppled from power all over the world. The same goes for media professionals, tech CEOs, and public-health officials. They all have to go. And we need a thorough accounting not to mention guarantees that nothing like this will ever happen again. As for Moderna and Pfizer, one could easily make a case for forcing their immediate end as corporate entities.
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of
The Epoch Times.
Just How Hard Were We Trolled?
www.theepochtimes.com
Just How Hard Were We Trolled?
Jeffrey A. Tucker
February 6, 2023 | Updated: February 8, 2023
Commentary
What if Dr. Anthony Fauci co-authored an article on vaccines that would have gotten you and me blocked and banned at any point in the past three years? That just happened.
His article in Cell—“Rethinking next-generation vaccines for coronaviruses, influenzaviruses, and other respiratory viruses”—says it as plainly as possible: the COVID vaccine did not work because it could not work.
First some review from what we knew before this whole fiasco began.
Vaccines aren’t suitable for coronaviruses. Such respiratory viruses spread and mutate too quickly. This is why there has never been a vaccine for the common cold and why the flu shot is predictably suboptimal. Vaccines can only be sterilizing and contribute to public health when the virus is a stable pathogen such as smallpox and measles. For coronaviruses, there is really only one way forward: better antivirals, therapeutics, and acquired immunity.
The above paragraph has been repeated to me countless times in my life, especially after COVID hit. Every expert was on the same page. There was simply no question about it. Anything that would be called a vaccine would lack the features of vaccines past. It wouldn’t stop infection or transmission, much less end a bad season for respiratory viruses. This is why the FDA has never approved one. It would not and could not make it through trials, especially given the safety risks associated with every vaccine.
Maybe, maybe, there exists the possibility that you can come up with one variant but it isn’t likely to be approved in time to be effective. It might provide temporary protection against severe outcomes from one variant but it will be useless against further mutations. In addition, vaccine-induced protection is not as broad as natural immunity, so it is likely that the person would get infected later. Boosting is likely only to pertain to last month’s mutation, and raises dangers of itself: imprinting the immune system in ways that make it less effective.
Sadly, posting those three paragraphs on social media at any point in the past three years would likely get you censored or even banned. Normal science was suppressed. Common knowledge among experts was verboten. Everything we’ve learned for a century or even two millennia was thrown out. The job of censorship was tasked to a gaggle of ill-educated tech workers obeying the FBI overlords, so they went along.
And here we are two years after the vaccine rollout and the truth is rather well known. The vaccines were an enormous flop. At best. At worst, they caused tremendous amounts of injury and death as compared to any vaccine ever approved for the market. That they were forced on people in many professions—and backed by a Stalinesque media frenzy—is simply incredible. Several cities even locked themselves down for the vaccinated only. Even now, unvaccinated non-Americans cannot travel to the United States, unless they come across the southern border.
And yet only now does Fauci choose to lay out the science that we knew long ago. There is nothing particularly interesting in his article. Only the timing is interesting: following trillions in pharma profits, millions displaced by mandates, and suffering from injury all over the world. Now he says that there was really no chance that the vaccine would be either effective or necessarily safe.
This is a level of trolling that is truly unthinkable and indescribable.
Here is the summary of the article:
“Viruses that replicate in the human respiratory mucosa without infecting systemically, including influenza A, SARS-CoV-2, endemic coronaviruses, RSV, and many other ‘common cold’ viruses, cause significant mortality and morbidity and are important public health concerns. Because these viruses generally do not elicit complete and durable protective immunity by themselves, they have not to date been effectively controlled by licensed or experimental vaccines.
“In this review, we examine challenges that have impeded development of effective mucosal respiratory vaccines, emphasizing that all of these viruses replicate extremely rapidly in the surface epithelium and are quickly transmitted to other hosts, within a narrow window of time before adaptive immune responses are fully marshaled.”
There are profound safety issues to consider too. It takes a very long time to assure that. Fauci says:
“Considering that vaccine development and licensure is a long and complex process requiring years of preclinical and clinical safety and efficacy data, the limitations of influenza and SARS-CoV-2 vaccines remind us that candidate vaccines for most other respiratory viruses have to date been insufficiently protective for consideration of licensure …”
Further, vaccines certainly cannot improve on what even natural immunity cannot do:
“Taking all of these factors into account, it is not surprising that none of the predominantly mucosal respiratory viruses have ever been effectively controlled by vaccines. This observation raises a question of fundamental importance: if natural mucosal respiratory virus infections do not elicit complete and long-term protective immunity against reinfection, how can we expect vaccines, especially systemically administered non-replicating vaccines, to do so?”
This is why the flu vaccines “have never been able to elicit durable protective immunity against seasonal influenza virus strains, even against non-drifted strains…. their effectiveness against clinically apparent infection is decidedly suboptimal, ranging from 14 percent to 60 percent over the past 15 influenza seasons.”
Now, it’s not as if Fauci admits that the vaccine was a complete flop. Of course, he has to engage in the usual incantations of the glories of the COVID vaccination.
“During the COVID-19 pandemic, the rapid development and deployment of SARS-CoV-2 vaccines has saved innumerable lives and helped to achieve early partial pandemic control.”
Note the word “innumerable.” It means there is no number and no possibility of a number. Exactly. Also note “early partial”—weasel words to cover the reality of egregious failure.
If you click through the citation to this dubious claim, it is from April 2021, early in the mutation process when we hardly had any data at all to justify such celebration. Why is Fauci citing a two-year-old piece in defense of the vaccine? Because that’s all there is to cite: two-year-old hagiographies without meaningful data.
How precisely can we account for this fiasco? If they knew, and they did know, how is it that they put us through this horrible upheaval? The most dreadful theory is that they knew for sure that the virus would become endemic through exposure. But the point of “slowing the spread” and “flattening the curve” (lockdowns and masking), while trashing and nearly banning other therapeutics, was to preserve the customer base for the new experimental product.
That product was mRNA which is supposed to be a platform for future vaccines. This is why the Johnson & Johnson vaccine was taken off market.
Under this theory, they wanted to prolong the pandemic for as long as possible so they could collect data on how well the vaccine worked. And they wanted to try it universally, which is why we did not hear much at all about the risk gradient of the vaccine itself. This also accounts for the deliberate drumming up of disease panic and forced distancing.
So let that sink in. They utterly smashed the world as we knew it—violating all human rights—in order to test out a new technology at great profit to themselves. In other words, they treated us all as lab rats.
An entire generation of politicians needs to be toppled from power all over the world. The same goes for media professionals, tech CEOs, and public-health officials. They all have to go. And we need a thorough accounting not to mention guarantees that nothing like this will ever happen again. As for Moderna and Pfizer, one could easily make a case for forcing their immediate end as corporate entities.
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of
The Epoch Times.
Heliobas Disciple
TB Fanatic
Maryland Considering Bill That Would Allow The Vaccination Of Children Without Parent's Consent | ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
 www.zerohedge.com
www.zerohedge.com
Maryland Considering Bill That Would Allow The Vaccination Of Children Without Parent's Consent
by Tyler Durden
Wednesday, Feb 08, 2023 - 04:40 PM
The State of Maryland has introduced a bill for consideration (Senate Bill 378) that would allow healthcare workers to vaccinate a child who is deemed "able to understand the benefits and potential consequences of getting vaccinated" without parental consent. The determined age of consent for a child to "choose" to be vaccinated is 14, though, such laws are often a slippery slope as guidelines and goalposts can be adjusted once a bill is passed to include even younger people.
It should be noted that Maryland law prevents children of 14 or older to refuse vaccination ordered by parents. In other words, they are considered competent enough to get vaccinated without parent's knowledge, but not competent enough to refuse vaccination with parent's knowledge. The push among some states to provide or legalize medical procedures on minors without advising parents has been growing in multiple sectors of healthcare the past few years, from abortions to gender affirmation surgeries.
It sounds like a remnant from two years ago when Democrat run states like New York were talking seriously about the forced internment of people who were "potential dangers" to public health. The concept of constitutional rights were going out the window and the US barely dodged an Orwellian end. Parental rights are often considered a vital barrier to state interference with vulnerable children who are easily manipulated into accepting procedures that could affect their rest of their lives.
The potential consequences are obvious - Schools and other government institutions could very easily exploit medical personnel to convince children that they MUST submit to vaccination. They could also influence minors to believe it was "all their idea." The same scenario could involve overzealous doctors or nurses in a hospital setting. With the informed parental shield removed, the sky is the limit in terms of what the state can do to the younger generation.
Though the bill mentions that decisions by minors be made "without coercion", a child may not be able to identify coercion when it happens. Not all manipulation requires open and obvious threats.
Democratic State Sen. Cheryl Kagan introduced Bill 378 on Wednesday. The bill is set to go before a hearing in the Senate Finance Committee on Feb. 22. The language is broad and seems to include all possible vaccinations rather than a set list.
Even in the case of a child voluntarily asking for medical treatments without deception, it is the job of parents to sometimes protect their kids from themselves. Without developed critical thinking skills minors require guidance to avoid rash decisions. When peer pressure is coming from officials with a perceived authority, children are less likely to say no. The Maryland bill ignores these factors and opens the door to a wide range of abuses.
Heliobas Disciple
TB Fanatic
Scientists Discover Small Molecules That Successfully Target COVID Spike Proteins
Using Small Molecules To Keep SARS-CoV-2 Closed for Business The infamous spike proteins on the surface of SARS-CoV-2 help it bind to and enter human cells. Because of their important role in spreading infection, these spike proteins are one of the main targets for COVID-19 vaccines and treatments.
scitechdaily.com
Scientists Discover Small Molecules That Successfully Target COVID Spike Proteins
By American Chemical Society
February 8, 2023
Using Small Molecules To Keep SARS-CoV-2 Closed for Business
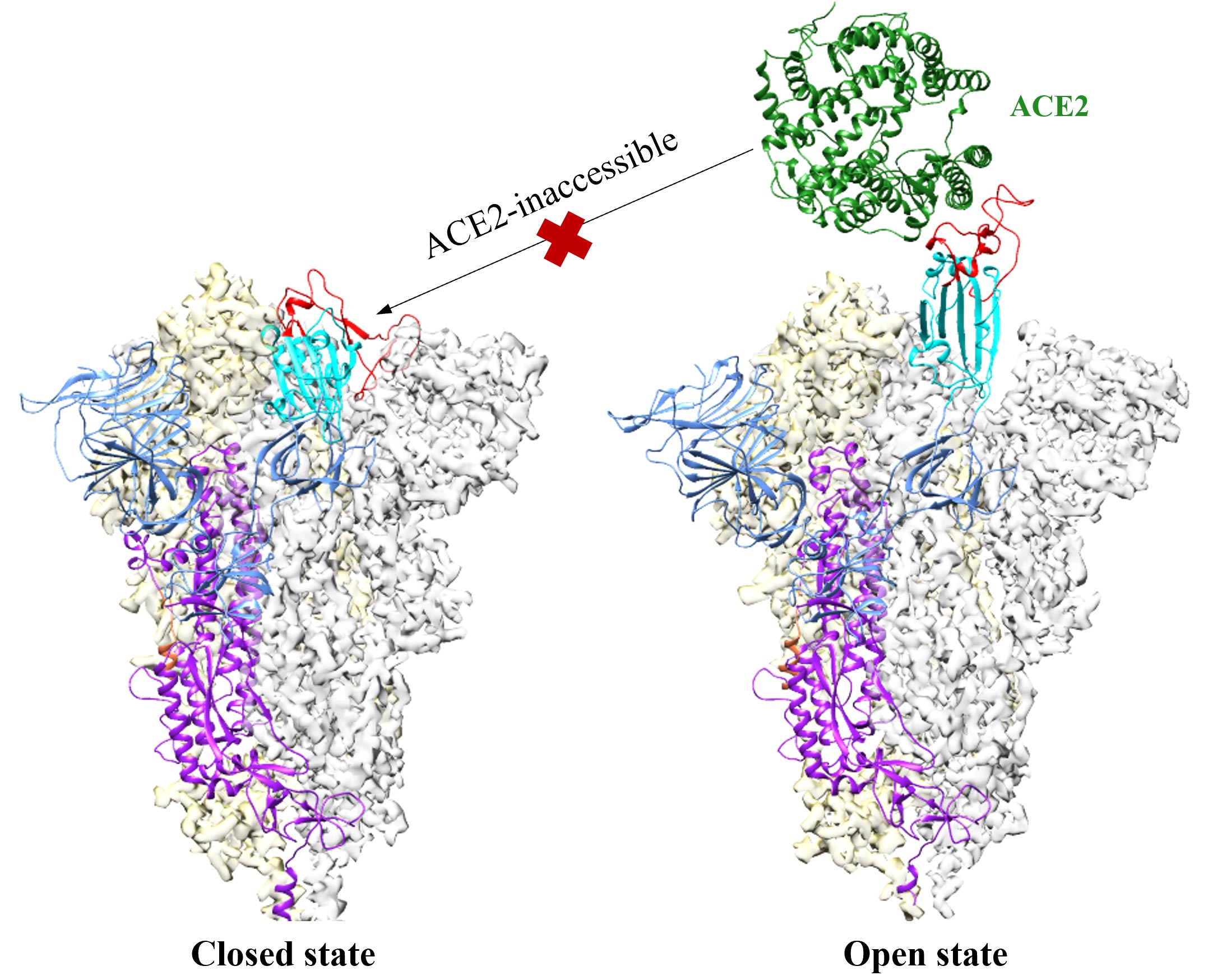
The infamous spike proteins on the surface of SARS-CoV-2 help it bind to and enter human cells. Because of their important role in spreading infection, these spike proteins are one of the main targets for COVID-19 vaccines and treatments. But those remedies gradually lose effectiveness when certain segments of the spike proteins mutate. Now, researchers report in ACS Central Science that they have discovered small molecules that successfully target other segments that mutate less.
Spike proteins change shape when they attack a cell. In their “open” structure, they expose a section known as the receptor-binding domain (RBD) so it can attach to the ACE2 protein on human cells. In the “closed” structure, this RBD segment is tucked inside the spike protein and can’t bind to human cells. Antibodies contained in some COVID-19 therapies or stimulated by vaccines or infection target the RBD domain so it can’t bind to ACE2. However, some emerging variants of the coronavirus contain mutations in the RBD fragment. That means vaccines and antibody therapies designed to target that fragment could become less effective as the virus mutates.
To get around this problem, other, less mutation-prone parts of the spike protein could be targeted instead. One possibility is a pocket in the spike protein that has been dubbed the Achilles’ heel of the virus. When this cranny is occupied by free fatty acids (FFAs) or a few other compounds, the protein remains locked in its closed, harmless configuration. However, those compounds aren’t suitable treatments because they aren’t stable or they bind weakly. So, Jianhui Huang, Niu Huang, and colleagues decided to look for other potential treatments that lack these flaws.
Using computer modeling, the team screened a library of small molecules, seeking ones that could slip into this pocket and stick firmly to the spike protein, keeping it in the closed shape. The researchers then used surface plasmon resonance and other techniques to evaluate analogs of these molecules for improved binding and solubility. The resulting compounds, which can bind to spike proteins from the original coronavirus as well as the omicron BA.4 variant, could serve as a starting point for developing broad-spectrum treatments for COVID-19, the team says.
Reference: “In Silico Discovery of Small Molecule Modulators Targeting the Achilles' Heel of SARS-CoV-2 Spike Protein” 8 February 2023, ACS Central Science.
DOI: 10.1021/acscentsci.2c01190
The authors acknowledge support from the Beijing Municipal Science & Technology Commission and Tsinghua University.
Heliobas Disciple
TB Fanatic
Single-dose treatment reduces COVID-19 hospitalization risk by half for high-risk patients in phase 3 trial
A single-dose of the antiviral drug peginterferon lambda reduced by half the risk of hospitalization or a visit to the Emergency Department due to COVID-19, according to a study published today in the New England Journal of Medicine.
Single-dose treatment reduces COVID-19 hospitalization risk by half for high-risk patients in phase 3 trial
by University Health Network
February 8, 2023
A single-dose of the antiviral drug peginterferon lambda reduced by half the risk of hospitalization or a visit to the Emergency Department due to COVID-19, according to a study published today in the New England Journal of Medicine.
The multi-center phase 3 TOGETHER clinical trial—designed to test a new therapy in a real setting—evaluated the use of this drug in more than 1,900 outpatients at high risk of developing complications from COVID-19.
Patients who received a single-dose subcutaneous injection of peginterferon lambda within seven days of their first COVID-19 symptom had a 50 percent lower risk of needing to be admitted to hospital when compared to people who received a placebo.
The trial was one of the first to test treatment in a largely vaccinated population. The research team found that a similar effect was seen in those who had received the vaccine—84 percent—as in those who were unvaccinated. The team also saw the benefits of treatment across multiple COVID-19 variants, including the highly transmissible omicron variant.
This study follows a previous phase 2 trial performed at UHN that showed that peginterferon lambda accelerated clearance of the virus.
"This much larger trial shows us that the antiviral benefits we previously observed translate to clinical benefit. The results conclusively show that this is an effective therapy to treat COVID-19 to reduce the risk of complications," says Dr. Jordan Feld, one of the lead authors of the study, Interim Director of the Toronto Center for Liver Disease and Co-Director of the Schwartz Reisman Liver Research Center and the R. Phelan Chair in Translational Liver Research at UHN.
"An important feature of this treatment is that it is not affected by changes or mutations in the virus, because it works by stimulating the body's own response to viral infection," added Dr. Feld, who is also a Senior Scientist at the Toronto General Hospital Research Institute at UHN and a professor in the Department of Medicine at the University of Toronto.
Study participants reported few or no side effects, with no significant differences seen between the group that received the actual treatment and the group that received a matching placebo.
"This could be an important addition to our arsenal to fight COVID-19, especially for high-risk patients who may not be able to use currently available treatments because of side effects or drug interactions with medications they take," says Dr. Feld.
All participants were either aged 50 or older or had a health condition that put them at higher risk for severe COVID-19, such as diabetes, hypertension, obesity, being a transplant recipient, cancer patient, among other conditions. The effect of the treatment was even more pronounced in people who received the drug within three days of symptom onset, consistent with other antiviral medications for COVID-19.
The study was done in partnership with the Pontifical Catholic University of Minas Gerais, Brazil, where first author Dr. Gilmar Reis and his team recruited the majority of participants and helped analyze the data. The study was also done in collaboration with Dr. Edward Mills, at McMaster University, and Professor Jeffrey Glenn at Stanford University.
The TOGETHER Study is a phase 3 trial that was based on the phase 2 study led by Dr. Feld in Toronto last year.
Heliobas Disciple
TB Fanatic

No new variants emerged from China’s Covid outbreak, study finds
Analysis of Covid-19 cases in Beijing suggests that no new variants emerged from China’s recent outbreak, according to a study in The Lancet on Wednesday.
No new variants emerged from China’s Covid outbreak, study finds
Jennifer Jett - NBC News
Wed, February 8, 2023, 12:37 PM EST
HONG KONG — Analysis of Covid-19 cases in Beijing suggests that no new variants emerged from China’s recent outbreak, according to a study published Wednesday.
Facing rare mass unrest after nearly three years of strict “zero-Covid” policies, the Chinese government dropped most restrictions on Dec. 7. The sudden change unleashed the coronavirus over the winter on a population of 1.4 billion people who had barely been exposed to it, raising fears that the outbreak could produce a new variant of concern and leading dozens of countries, including the United States, to impose testing and other curbs on travelers from China.
But the Chinese-funded study, which was published in The Lancet, found that of 413 sampled infections in Beijing, all belonged to existing Covid variants. The most common were omicron subvariants BA.5.2 and BF.7, which together accounted for more than 90% of local infections.
The samples were randomly selected for genomic sequencing from a larger group of 2,881 high-quality samples collected in Beijing from Nov. 14 to Dec. 20, 2022.
George Gao, the study’s lead author and a professor at the Institute of Microbiology in the Chinese Academy of Sciences, said it was important to investigate whether any new variants had emerged during China’s outbreak given the impact that others like delta and omicron have had on the course of the pandemic.
“Our analysis suggests two known omicron subvariants — rather than any new variants — have chiefly been responsible for the current surge in Beijing, and likely China as a whole,” Gao, the former director of the Chinese Center for Disease Control and Prevention, said in a news release.
“However, with ongoing large-scale circulation of Covid-19 in China, it is important we continue to monitor the situation closely so that any new variants that might emerge are found as early as possible.”
Although the study covered a short period early in the outbreak and the sampling was limited to Beijing, its findings are in line with reports from Italy and other countries that have been testing arrivals from China for Covid and sequencing the results, said Tongai Maponga, a researcher in the Division of Medical Virology at the University of Stellenbosch in South Africa.
“Whatever they are detecting in travelers originating from China is the same as what we already know to be in circulation elsewhere,” said Maponga, who was not involved in the Beijing study.
The study was also limited by the fact that China ended mandatory large-scale testing in December, making it difficult to know the total number of cases in the outbreak and thus what percentage of total cases the samples represent.
After being kept at bay for most of the pandemic, the virus appears to have torn through China much faster than in many other countries, starting to pick up speed last fall even before the Covid restrictions were lifted. Beijing and other major cities experienced some of the earliest outbreaks.
Zeng Guang, former chief epidemiologist at the Chinese CDC, said in late December that more than 80% of Beijing residents had most likely contracted the virus. A study published in January by researchers at the University of Hong Kong said it could be more than 92% by Jan. 31.
Chinese officials say a feared surge during the Lunar New Year holiday period, when hundreds of millions of people travel to their hometowns to visit family and which began in mid-January, did not materialize. But the outbreak has still been a huge source of anxiety for Chinese who had been taught to fear Covid-19 and devastating for those who lost loved ones to the disease.
Global fears that a new variant might emerge were compounded by what the World Health Organization and others said was a lack of data from China about its outbreak. China has defended its data and criticized the travel measures as unscientific and discriminatory.
Chinese officials have released more data in recent weeks, saying hospitals have recorded about 80,000 Covid-related deaths since early December. Many experts say the true number is far higher, with the British forecaster Airfinity estimating 608,000 deaths from Dec. 1 to Jan. 17.
The Chinese CDC most recently reported 3,278 Covid-related deaths nationwide from Jan. 27 to Feb. 2, about half the number from the week before. It says daily Covid infections peaked at 6.94 million on Dec. 22 and have since fallen to about 24,000 as of Jan. 30.
Maponga pointed out that a new variant of concern could still emerge anywhere in the world, underlining the need for continued testing, genomic surveillance and transparent sharing of data.
“As long as it continues circulating, infecting people as well as animals, the virus will always be developing mutations because that is the nature of viruses,” he said.
Heliobas Disciple
TB Fanatic
Pfizer vax chief advised government on gain-of-function guidelines 4 years before COVID: Report
Director participated in National Academies panel on rule revision advice.
Pfizer vax chief advised government on gain-of-function guidelines 4 years before COVID: Report
Director participated in National Academies panel on rule revision advice.
By Just the News staff
Updated: February 7, 2023 - 2:08pm
A leading vaccine researcher at Pfizer helped advise a U.S. federal advisory board on its revision of guidelines overseeing dangerous "gain-of-function" virology research years before the pandemic, documents show.
Philip Dormitzer, then the chief scientific officer for vaccine research and development at Pfizer, "advised the National Science Advisory Board for Biosecurity during the group’s deliberation over redrafting government policies concerning gain of function research," according to a Tuesday report by Natalie Winters at War Room.
"Gain-of-function" research involves experiments to increase the pathogenicity and/or lethality of viruses in order to study their potential for infecting human hosts. Experts have for years criticized these experiments as too risky relative to their potential scientific payoffs.
In 2014 the U.S. government issued an unprecedented pause on gain-of-function research, clamping down on funding for the experiments amid concerns of the risks associated with them. The National Academies subsequently convened two symposiums to discuss potential revisions to the U.S.'s gain-of-function guidelines in order to reinstate funding for the experiments.
Dormitzer was a member of the planning committee of the second symposium, Winters reports, citing documentation from the National Academies Press.
In at least one instance during the symposium, the documents show, Dormitzer expressed "concern about unintended consequences, for example from the 'blowback' onto vaccine production from the controversies over [gain-of-function] studies of concern—or GOF research more generally—in academia.”
The National Academies, Winters notes, "were the most influential advisor to the NSABB, which, in turn, was responsible drafting the government’s new gain of function research policy."
The National Institutes of Health's Office of Science Policy notes on its website that the U.S. government "considered the NSABB’s findings and recommendations during the development of policy on gain-of-function research."
psychgirl
TB Fanatic
I can’t say enough how important this is, as are the previous articles HD posted last night.Another article about the Fauci Cell article.
(fair use applies)Just How Hard Were We Trolled?
Just How Hard Were We Trolled?
Jeffrey A. Tucker
February 6, 2023 | Updated: February 8, 2023
Commentary
What if Dr. Anthony Fauci co-authored an article on vaccines that would have gotten you and me blocked and banned at any point in the past three years? That just happened.
His article in Cell—“Rethinking next-generation vaccines for coronaviruses, influenzaviruses, and other respiratory viruses”—says it as plainly as possible: the COVID vaccine did not work because it could not work.
First some review from what we knew before this whole fiasco began.
Vaccines aren’t suitable for coronaviruses. Such respiratory viruses spread and mutate too quickly. This is why there has never been a vaccine for the common cold and why the flu shot is predictably suboptimal. Vaccines can only be sterilizing and contribute to public health when the virus is a stable pathogen such as smallpox and measles. For coronaviruses, there is really only one way forward: better antivirals, therapeutics, and acquired immunity.
The above paragraph has been repeated to me countless times in my life, especially after COVID hit. Every expert was on the same page. There was simply no question about it. Anything that would be called a vaccine would lack the features of vaccines past. It wouldn’t stop infection or transmission, much less end a bad season for respiratory viruses. This is why the FDA has never approved one. It would not and could not make it through trials, especially given the safety risks associated with every vaccine.
Maybe, maybe, there exists the possibility that you can come up with one variant but it isn’t likely to be approved in time to be effective. It might provide temporary protection against severe outcomes from one variant but it will be useless against further mutations. In addition, vaccine-induced protection is not as broad as natural immunity, so it is likely that the person would get infected later. Boosting is likely only to pertain to last month’s mutation, and raises dangers of itself: imprinting the immune system in ways that make it less effective.
Sadly, posting those three paragraphs on social media at any point in the past three years would likely get you censored or even banned. Normal science was suppressed. Common knowledge among experts was verboten. Everything we’ve learned for a century or even two millennia was thrown out. The job of censorship was tasked to a gaggle of ill-educated tech workers obeying the FBI overlords, so they went along.
And here we are two years after the vaccine rollout and the truth is rather well known. The vaccines were an enormous flop. At best. At worst, they caused tremendous amounts of injury and death as compared to any vaccine ever approved for the market. That they were forced on people in many professions—and backed by a Stalinesque media frenzy—is simply incredible. Several cities even locked themselves down for the vaccinated only. Even now, unvaccinated non-Americans cannot travel to the United States, unless they come across the southern border.
And yet only now does Fauci choose to lay out the science that we knew long ago. There is nothing particularly interesting in his article. Only the timing is interesting: following trillions in pharma profits, millions displaced by mandates, and suffering from injury all over the world. Now he says that there was really no chance that the vaccine would be either effective or necessarily safe.
This is a level of trolling that is truly unthinkable and indescribable.
Here is the summary of the article:
“Viruses that replicate in the human respiratory mucosa without infecting systemically, including influenza A, SARS-CoV-2, endemic coronaviruses, RSV, and many other ‘common cold’ viruses, cause significant mortality and morbidity and are important public health concerns. Because these viruses generally do not elicit complete and durable protective immunity by themselves, they have not to date been effectively controlled by licensed or experimental vaccines.
“In this review, we examine challenges that have impeded development of effective mucosal respiratory vaccines, emphasizing that all of these viruses replicate extremely rapidly in the surface epithelium and are quickly transmitted to other hosts, within a narrow window of time before adaptive immune responses are fully marshaled.”
There are profound safety issues to consider too. It takes a very long time to assure that. Fauci says:
“Considering that vaccine development and licensure is a long and complex process requiring years of preclinical and clinical safety and efficacy data, the limitations of influenza and SARS-CoV-2 vaccines remind us that candidate vaccines for most other respiratory viruses have to date been insufficiently protective for consideration of licensure …”
Further, vaccines certainly cannot improve on what even natural immunity cannot do:
“Taking all of these factors into account, it is not surprising that none of the predominantly mucosal respiratory viruses have ever been effectively controlled by vaccines. This observation raises a question of fundamental importance: if natural mucosal respiratory virus infections do not elicit complete and long-term protective immunity against reinfection, how can we expect vaccines, especially systemically administered non-replicating vaccines, to do so?”
This is why the flu vaccines “have never been able to elicit durable protective immunity against seasonal influenza virus strains, even against non-drifted strains…. their effectiveness against clinically apparent infection is decidedly suboptimal, ranging from 14 percent to 60 percent over the past 15 influenza seasons.”
Now, it’s not as if Fauci admits that the vaccine was a complete flop. Of course, he has to engage in the usual incantations of the glories of the COVID vaccination.
“During the COVID-19 pandemic, the rapid development and deployment of SARS-CoV-2 vaccines has saved innumerable lives and helped to achieve early partial pandemic control.”
Note the word “innumerable.” It means there is no number and no possibility of a number. Exactly. Also note “early partial”—weasel words to cover the reality of egregious failure.
If you click through the citation to this dubious claim, it is from April 2021, early in the mutation process when we hardly had any data at all to justify such celebration. Why is Fauci citing a two-year-old piece in defense of the vaccine? Because that’s all there is to cite: two-year-old hagiographies without meaningful data.
How precisely can we account for this fiasco? If they knew, and they did know, how is it that they put us through this horrible upheaval? The most dreadful theory is that they knew for sure that the virus would become endemic through exposure. But the point of “slowing the spread” and “flattening the curve” (lockdowns and masking), while trashing and nearly banning other therapeutics, was to preserve the customer base for the new experimental product.
That product was mRNA which is supposed to be a platform for future vaccines. This is why the Johnson & Johnson vaccine was taken off market.
Under this theory, they wanted to prolong the pandemic for as long as possible so they could collect data on how well the vaccine worked. And they wanted to try it universally, which is why we did not hear much at all about the risk gradient of the vaccine itself. This also accounts for the deliberate drumming up of disease panic and forced distancing.
So let that sink in. They utterly smashed the world as we knew it—violating all human rights—in order to test out a new technology at great profit to themselves. In other words, they treated us all as lab rats.
An entire generation of politicians needs to be toppled from power all over the world. The same goes for media professionals, tech CEOs, and public-health officials. They all have to go. And we need a thorough accounting not to mention guarantees that nothing like this will ever happen again. As for Moderna and Pfizer, one could easily make a case for forcing their immediate end as corporate entities.
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of
The Epoch Times.
That Fauxi himself is an authors on them is astounding.
The gall of him!
There are truly no words.
northern watch
TB Fanatic

Covid related?
northern watch
TB Fanatic
Alexander COVID News-Dr. Paul Elias Alexander's Newsletter
Natural exposure immunity evidence existed even historically from the Athenian plague of 430 BC whereby historical documents showed that recovered persons were protected when re-exposed to infection
'The same man was never attacked twice and certainly not fatally', this was known dating back 430 BC; this is natural immunity (natural acquired-adaptive immunity) that doctors disregarded for COVID
February 9 2023
SOURCE:
The Project Gutenberg eBook of The History of the Peloponnesian War, by Thucydides

Natural exposure immunity evidence existed even historically from the Athenian plague of 430 BC whereby historical documents showed that recovered persons were protected when re-exposed to infection
'The same man was never attacked twice and certainly not fatally', this was known dating back 430 BC; this is natural immunity (natural acquired-adaptive immunity) that doctors disregarded for COVID
Heliobas Disciple
TB Fanatic
Surprised MSM is reporting on this. Blaming covid not the vaccine, but the numbers must be indisputable now if MSM is reporting on it.

 news.yahoo.com
(fair use applies)
news.yahoo.com
(fair use applies)
Since COVID, more young people are dying of heart attacks. Here's what we know
Maura Hohman - TODAY
Thu, February 9, 2023, 4:47 PM EST
When Demi Washington, a basketball player at Vanderbilt University came down with COVID-19 in late 2020, her symptoms were mild, just a runny nose. But to ensure her safe return to the court, the school required her to undergo an MRI.
The results brought Washington to tears.
Following the infection, the now college senior had developed myocarditis — when the heart muscle becomes inflamed, which can decrease the heart's ability to pump blood. The condition can lead to stroke or heart attack, according to Mayo Clinic. Washington was not vaccinated against COVID-19 at the time.
"I was scared because any internal organ, you’re like, 'Oh, my gosh, I need that to live,'" she recalled to TODAY. "I didn’t really know what was going to come of it, how long was it going to take for it to resolve."
Washington had to skip the rest of the 2020 to 2021 season, but ultimately she was grateful. "I think about the fact that Vanderbilt does do the MRI and a lot of other schools didn’t," she told TODAY in a segment aired Feb. 9. "The fact that I could have played if we didn’t is hard and scary to think about."
Washington's doctor never told her that she was at risk of dying, but he did stress the importance of rest and keeping her heart rate under a certain pace. She had to wear a watch to track her activity. Even though COVID was especially new at the time, Washington said her doctor felt confident her condition was due to the coronavirus, as he'd seen something similar other college athletes.
Washington said she felt no symptoms or signs that her heart had become inflamed, nor did she have a genetic predisposition. "It (just) happened to be me," she said. "I still don't really know why."
Washington has since recovered and is back to playing ball. But her experience sheds light on the thousands of young adults infected with COVID-19 whose health hasn't rebounded as successfully.
COVID-19, heart attacks and young people
Since the COVID-19 pandemic began, heart attack deaths across all age groups have become more common in the U.S., according to a September 2022 study by Cedars Sinai hospital in Los Angeles.
The age group hit the hardest? People between 25 and 44, who saw a 29.9% relative increase in heart attack deaths over the first two years of the pandemic (which means the actual number of heart attack deaths were almost 30% higher than the predicted number).
“Young people are obviously not really supposed to die of heart attack. They’re not really supposed to have heart attacks at all,” Dr. Susan Cheng, a cardiologist at Cedars Sinai and co-author of the study, told TODAY in a segment aired Feb. 9.
Adults between 45 and 64 saw a 19.6% relative increase in heart attack deaths, and those 65 and older saw a 13.7% relative increase, according to a press release from Cedars Sinai. The increase in U.S. heart attack deaths continued through the omicron surge, even though the variant is thought to cause milder illness, and spikes of heart attack deaths have aligned with the timing of COVID-19 surges in the U.S.
Los Angeles County paramedic Romeo Robles told TODAY in the Feb. 9 segment that upticks in COVID-19 would often lead to more 911 calls related to heart issues in his community.
"Surprisingly, people my age ... we would find them in cardiac arrest, and it was all predicted by these waves," he said.
Cheng called the connection "more than coincidental, that is for sure." Explaining why, she pointed out that COVID-19 can greatly impact the cardiovascular system.
"It appears to be able to increase the stickiness of the blood and increase ... the likelihood of blood clot formation," Cheng said. "It seems to stir up inflammation in the blood vessels. It seems to also cause in some people, an overwhelming stress, whether it’s related directly to the infection or situations around the infection, that can also cause a spike in blood pressure."
The reason for the relative rise in young people in particular is unclear, but one theory, Cheng said, is that the virus's impact on the cardiovascular system in some people may be due to an excessive immune system response and that young people are more likely to have stronger immune systems..
COVID-19 and heart disease
For COVID-19 survivors, the risk of developing a heart condition even a year after the infection, regardless of how severe the initial symptoms were, is "substantial," according to a February 2022 study of more than 150,000 individuals with COVID-19. The risk increases even for people who don't have any other risk factors for heart disease.
Dr. Ziyad Al-Aly, a physician-scientist ad Washington University School of Medicine in St. Louis and co-author of the study, estimated that about 4% of people who have COVID-19 will develop a heart problem, such as irregular heartbeat, heart failure, inflammation or heart attacks.
"It’s a small number, but really, it’s not as you multiply that number by the huge number of people in the United States and throughout the world who had COVID-19," he told TODAY.
What's more, the risk of developing long COVID, including heart problems, increases with each COVID-19 infection an individual has, Al-Aly pointed out. As a result, Latino and Black communities, which have higher rates of reinfection, are especially high risk for heart problems post-COVID, Cheng said.
As doctors and other researchers continue to wade through the data on COVID-19 and heart disease, the best course of action is to avoid infection as best you can, Cheng and Al-Aly said. To do so:
"I'd love to say we're ... coming out on the other side and we can think of COVID more so like the common cold. Unfortunately, that is not the case. ... That is eminently clear from all of the data," Cheng said. "This is not even just like the flu. ... This virus is still very different from any other virus we have seen in our lifetime."
.
Since COVID, more young people are dying of heart attacks. Here's what we know
When Demi Washington, a basketball player at Vanderbilt University came down with COVID-19 in late 2020, her symptoms were mild, just a runny nose.
Since COVID, more young people are dying of heart attacks. Here's what we know
Maura Hohman - TODAY
Thu, February 9, 2023, 4:47 PM EST
When Demi Washington, a basketball player at Vanderbilt University came down with COVID-19 in late 2020, her symptoms were mild, just a runny nose. But to ensure her safe return to the court, the school required her to undergo an MRI.
The results brought Washington to tears.
Following the infection, the now college senior had developed myocarditis — when the heart muscle becomes inflamed, which can decrease the heart's ability to pump blood. The condition can lead to stroke or heart attack, according to Mayo Clinic. Washington was not vaccinated against COVID-19 at the time.
"I was scared because any internal organ, you’re like, 'Oh, my gosh, I need that to live,'" she recalled to TODAY. "I didn’t really know what was going to come of it, how long was it going to take for it to resolve."
Washington had to skip the rest of the 2020 to 2021 season, but ultimately she was grateful. "I think about the fact that Vanderbilt does do the MRI and a lot of other schools didn’t," she told TODAY in a segment aired Feb. 9. "The fact that I could have played if we didn’t is hard and scary to think about."
Washington's doctor never told her that she was at risk of dying, but he did stress the importance of rest and keeping her heart rate under a certain pace. She had to wear a watch to track her activity. Even though COVID was especially new at the time, Washington said her doctor felt confident her condition was due to the coronavirus, as he'd seen something similar other college athletes.
Washington said she felt no symptoms or signs that her heart had become inflamed, nor did she have a genetic predisposition. "It (just) happened to be me," she said. "I still don't really know why."
Washington has since recovered and is back to playing ball. But her experience sheds light on the thousands of young adults infected with COVID-19 whose health hasn't rebounded as successfully.
COVID-19, heart attacks and young people
Since the COVID-19 pandemic began, heart attack deaths across all age groups have become more common in the U.S., according to a September 2022 study by Cedars Sinai hospital in Los Angeles.
The age group hit the hardest? People between 25 and 44, who saw a 29.9% relative increase in heart attack deaths over the first two years of the pandemic (which means the actual number of heart attack deaths were almost 30% higher than the predicted number).
“Young people are obviously not really supposed to die of heart attack. They’re not really supposed to have heart attacks at all,” Dr. Susan Cheng, a cardiologist at Cedars Sinai and co-author of the study, told TODAY in a segment aired Feb. 9.
Adults between 45 and 64 saw a 19.6% relative increase in heart attack deaths, and those 65 and older saw a 13.7% relative increase, according to a press release from Cedars Sinai. The increase in U.S. heart attack deaths continued through the omicron surge, even though the variant is thought to cause milder illness, and spikes of heart attack deaths have aligned with the timing of COVID-19 surges in the U.S.
Los Angeles County paramedic Romeo Robles told TODAY in the Feb. 9 segment that upticks in COVID-19 would often lead to more 911 calls related to heart issues in his community.
"Surprisingly, people my age ... we would find them in cardiac arrest, and it was all predicted by these waves," he said.
Cheng called the connection "more than coincidental, that is for sure." Explaining why, she pointed out that COVID-19 can greatly impact the cardiovascular system.
"It appears to be able to increase the stickiness of the blood and increase ... the likelihood of blood clot formation," Cheng said. "It seems to stir up inflammation in the blood vessels. It seems to also cause in some people, an overwhelming stress, whether it’s related directly to the infection or situations around the infection, that can also cause a spike in blood pressure."
The reason for the relative rise in young people in particular is unclear, but one theory, Cheng said, is that the virus's impact on the cardiovascular system in some people may be due to an excessive immune system response and that young people are more likely to have stronger immune systems..
COVID-19 and heart disease
For COVID-19 survivors, the risk of developing a heart condition even a year after the infection, regardless of how severe the initial symptoms were, is "substantial," according to a February 2022 study of more than 150,000 individuals with COVID-19. The risk increases even for people who don't have any other risk factors for heart disease.
Dr. Ziyad Al-Aly, a physician-scientist ad Washington University School of Medicine in St. Louis and co-author of the study, estimated that about 4% of people who have COVID-19 will develop a heart problem, such as irregular heartbeat, heart failure, inflammation or heart attacks.
"It’s a small number, but really, it’s not as you multiply that number by the huge number of people in the United States and throughout the world who had COVID-19," he told TODAY.
What's more, the risk of developing long COVID, including heart problems, increases with each COVID-19 infection an individual has, Al-Aly pointed out. As a result, Latino and Black communities, which have higher rates of reinfection, are especially high risk for heart problems post-COVID, Cheng said.
As doctors and other researchers continue to wade through the data on COVID-19 and heart disease, the best course of action is to avoid infection as best you can, Cheng and Al-Aly said. To do so:
- Wear a mask in crowded settings, and consider socializing outdoors with people outside your household.
- Stay up to date on your vaccinations. Research shows that you're 11 times more likely to develop myocarditis from COVID itself versus the vaccine, NBC News senior medical correspondent Dr. John Torres said during a TODAY segment on Feb. 9.
- Take a COVID-19 test as soon as you start to develop any symptoms and stay home when you're sick.
- Chest pain or discomfort, such as pressure, squeezing or fullness.
- Weakness, light-headedness or fainting.
- A cold sweat.
- Pain or discomfort in the jaw, neck or back.
- Shortness of breath, either at the same time as or before chest discomfort.
"I'd love to say we're ... coming out on the other side and we can think of COVID more so like the common cold. Unfortunately, that is not the case. ... That is eminently clear from all of the data," Cheng said. "This is not even just like the flu. ... This virus is still very different from any other virus we have seen in our lifetime."
.
Heliobas Disciple
TB Fanatic

More Than 217,000 Americans Killed by the COVID Jab: Survey Estimate
You'll never guess how many have been killed or seriously injured in just the first year. Yet, the ...
 www.theepochtimes.com
www.theepochtimes.com
More Than 217,000 Americans Killed by the COVID Jab: Survey Estimate
Joseph Mercola
Feb 7 2023
You’ll never guess how many have been killed or seriously injured in just the first year. Yet, the FDA and CDC keep pushing the shots, despite their own trial data showing they have no benefit in terms of reducing your risk of hospitalization or death.
- According to a December 2021 survey of 2,840 Americans, between 217,330 and 332,608 people died from the COVID jabs in 2021.
- Survey results also show that people who got the jab were more likely to know someone who experienced a health problem from COVID-19 infection, whereas those who knew someone who experienced a health problem after getting the jab were less likely to be jabbed.
- Of the respondents, 34 percent knew one or more people who had experienced a significant health problem due to the COVID-19 illness, and 22 percent knew one or more people who had been injured by the shot.
- Fifty-one percent of the survey respondents had been jabbed. Of those, 13 percent reported experiencing a “serious” health problem post-jab. Compare that to Pfizer’s six-month safety analysis, which claimed only 1.2 percent of trial participants experienced a serious adverse event.
- In December 2022, Rasmussen Reports polled 1,000 Americans. In this poll, 34 percent reported experiencing minor side effects from the jab and seven percent reported major side effects.
While it’s clear that the experimental COVID shots have killed a considerable number of people, the total death toll remains elusive, thanks to U.S. health agencies obfuscating, hiding, and manipulating data.
That said, the most recent survey1,2—published in the peer-reviewed journal BMC Infectious Diseases—puts the death toll from the COVID jabs somewhere between 217,330 and 332,608 in 2021 alone. As noted by Steve Kirsch:3
“[We’ve] killed at least 217,000 Americans and seriously injured 33 million … in just the first year, and the CDC [Centers for Disease Control and Prevention] and FDA [U.S. Food and Drug Administration] want to give you more shots … Since deaths from the vaccine were higher in 2022, most experts would estimate the all-cause mortality death toll from the COVID vaccines to be in the range of 500K to 600K.
“So the global cost of life from these vaccines is on the order of 10 to 12 million people … These [data] are consistent with the numbers I’ve been saying for a long time. It’s not a coincidence.”
Survey: Why People Did or Did Not Get the Jab
Now, the slant of this paper is kind of interesting. The primary aim of it was to “identify the factors associated by American citizens with the decision to be vaccinated against COVID-19.”
The author was curious about why 31 percent of the U.S. population had declined the jab or not completed the primary series by November 2022, nearly two years into a massively advertised “vaccination” campaign.
Calculating the proportion of fatal events from the jab was secondary. As explained by the author, Mark Skidmore,4 Ph.D., an economics professor at Michigan State University:5
- “A largely unexplored factor is the degree to which serious health problems arising from the COVID-19 illness or the COVID-19 vaccines among family and friends influences the decision to be vaccinated.
- “Serious illness due to COVID-19 would make vaccination more likely; the perceived benefits of avoiding COVID-19 through inoculation would be higher.
- "On the other hand, observing major health issues following COVID-19 inoculation within one’s social network would heighten the perceived risks of vaccination. Previous studies have not evaluated the degree to which experiences with the disease and vaccine injury influence vaccine status.
- “The main aim of this online survey of COVID-19 health experiences is to investigate the degree to which the COVID-19 disease and COVID-19 vaccine adverse events among friends and family, whether perceived or real, influenced inoculation decisions. The second aim of this work is to estimate the total number of COVID-19 vaccine-induced fatalities nationwide from the survey.”
Here’s an excerpt describing the methodology:6
“An online survey of COVID-19 health experiences was conducted. Information was collected regarding reasons for and against COVID-19 inoculations, experiences with COVID-19 illness, and COVID-19 inoculations by survey respondents and their social circles. Logit regression analyses were carried out to identify factors influencing the likelihood of being vaccinated.”
Survey Findings
A total of 2,840 people completed the survey between Dec. 18 and Dec. 23, 2021. The mean age was 47, and the gender ratio was 51 percent women, 49 percent men. Just over half, 51 percent, had received one or more COVID jabs.
As Skidmore suspected, results showed that people who got the jab were more likely to know someone who experienced a health problem from COVID-19 infection, whereas those who knew someone who experienced a health problem after getting the jab were less likely to be jabbed.
Of the respondents, 34 percent knew one or more people who had experienced a significant health problem due to the COVID-19 illness, and 22 percent knew one or more people who had been injured by the shot. So, as noted by to the author:7
“Knowing someone who reported serious health issues either from COVID-19 or from COVID-19 vaccination are important factors for the decision to get vaccinated.”
As for the types of side effects experienced by people within the respondents’ social circles, they included (but were not limited to) the “usual suspects,” such as:
- Heart and cardiovascular problems.
- Severe COVID infection or other respiratory illness.
- Feeling generally unwell, weak, fatigued, and out of breath for weeks.
- Blood clots and stroke.
- Death.
Hundreds of Thousands Killed for No Reason
Based on these survey data, Skidmore estimates:
“… the total number of fatalities due to COVID-19 inoculation may be as high as 278,000 (95 percent CI 217,330-332,608) when fatalities that may have occurred regardless of inoculation are removed.”
Were COVID-19 an infection with an extremely high mortality rate, perhaps high rates of death from a vaccine would be acceptable. But COVID-19 has an exceptionally low mortality rate, on par with or lower than influenza, hence the risk associated with the COVID jabs ought to be equally low.
The global cost of life from these vaccines is on the order of 10 to 12 million people.
— Steve Kirsch
As it stands, the risks of the shots are very high, while Pfizer’s own trial data, with more than 40,000 participants, show they offer no benefit in terms of your risk of hospitalization and/or death. The absolute risk reduction is so minute as to be inconsequential.8
High Rates of Side Effects
The death toll from the jabs isn’t the only disturbing part of this paper, though. Skidmore’s findings also suggest side effects from the jab may be more common than previously suspected.
As mentioned, 51 percent of the respondents had been jabbed. Of those, 15 percent reported experiencing a new health problem post-jab and 13 percent deemed it “serious.” Compare that to Pfizer’s six-month safety analysis,9 which claimed only 1.2 percent of trial participants reported a serious adverse event.
Now, as suggested by Kirsch,10 “we need to discount that by a factor of two because people report less severe adverse events as adverse events.” Still, that means serious adverse events from the jab are five times higher than what Pfizer reported.
“This is why the FDA never does after-market surveys on the drugs it approves. Because reality hurts,” Kirsch writes.11 “It is the FDA that should have discovered this before Mark Skidmore. The FDA is asleep at the wheel and they just believe everything the drug companies tell them, hook, line, and sinker. This is a major miss. Why aren’t they doing surveys like this to see if the reality matches the study?”
More Side Effect Rate Comparisons
For additional comparison, here are the findings of several other investigations:
- Rasmussen Reports12: In December 2022, Rasmussen Reports polled 1,000 Americans. In this poll—taken one year after Skidmore’s survey—34 percent reported experiencing minor side effects from the jab and seven percent reported major side effects.
- CDC’s V-Safe data13: In October 2022, ICAN [Informed Consent Action Network] obtained the Centers for Disease Control and Prevention’s V-Safe data. This is a voluntary program to monitor adverse vaccine reactions. Of the 10.1 million COVID jab recipients who used the app, 7.7 percent had to seek medical care post-jab.
- Kirsch-funded survey14: A June 2022 U.S. survey by the market research company Pollfish found that 16.3 percent of COVID jabbed respondents experienced an injury, and 9.7 percent required medical care.
The graphic below, which visually compares Skidmore’s findings to the findings of the Rasmussen, V-Safe, and Pollfish surveys, was created by InfoGame on Substack.15 As noted by InfoGame:
“Skidmore’s article serves as another sign that the rate of COVID-19 side effects is extremely high and that the COVID-19 vaccines are an unprecedently risky medical product.”
Menstrual Irregularities Are Common Post-Jab
While we’re on the topic of reported side effects, several surveys have also focused on the frequency of abnormal menses in women who got the jab, which could be indicative of reproductive harm. For example:
- A British survey published in early December 2021 found 20 percent of women experienced menstrual disturbances following their jab.16
- A study published in Science Advances in mid-July 2022 found 66 percent of “fully vaccinated” postmenopausal women experienced abnormal breakthrough bleeding. In total, 42.1 percent reported heavier menstrual flow post-jab (this included women of all ages, as well as transgenders on hormone treatments).17
- An Italian peer-reviewed study published in March 2022 found that “50-60 percent of reproductive-age women who received the first dose of the COVID-19 vaccine reported menstrual cycle irregularities, regardless of the type of administered vaccine.” After the second dose, abnormal menses were reported by 60 percent to 70 percent.18
People in High Places Seek Retraction
Not surprisingly, people in high places are already trying to force a retraction of the paper. A special notice from the editor, dated just two days post-publication, states:
“Readers are alerted that the conclusions of this paper are subject to criticisms that are being considered by editors. Specifically, that the claims are unsubstantiated and that there are questions about the quality of the peer review.”
As noted by Kirsch:19
“They are actively trying to get the paper retracted because it destroys the narrative. I’m certain they will succeed because journals are under intense pressure to censor any anti-narrative paper. The problem is that Mark’s survey was entirely consistent with my surveys.
“If they want to have the paper retracted they need to show us THEIR surveys. But of course, they don’t have any surveys because they are too afraid of the results.
“So they will use hand-waving arguments like “I don’t like the methodology” or some nonsense like that instead of gathering their own data. They will NEVER show us survey data that supports their narrative because it isn’t there.
“That’s why there are no success anecdotes. NOBODY can give me the name of a U.S. geriatric practice where all-cause deaths plummeted after the vaccines rolled out. In every case, they went the wrong way. The narrative is unraveling at an accelerated pace but the medical community is still fighting the truth.”
Originally published Feb. 07, 2023, on Mercola.com
1, 5, 6, 7 BMC Infectious Diseases 2023; 23 article number 51
2 Jean Marc Benoit MD Substack Jan. 24, 2023
3, 10, 11, 19 Steve Kirsch Substack Jan. 25, 2023
4 Michigan State University Mark Skidmore
8 Steve Kirsch Substack Jan. 24, 2023
9 NEJM Nov. 4, 2021; 385: 1761-1773
12 Rasmussen Reports Dec. 7, 2022
13 ICANdecide.org Oct. 3, 2022
14 SKirsch.com July 1, 2022
15 Infogame Substack Jan. 25, 2023
16 MedRxiv Dec. 6, 2021
17 Science Advances July 15, 2022; 8(28)
18 Open Med March 9, 2022; 17(1): 475-484
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times. Epoch Health welcomes professional discussion and friendly debate. To submit an opinion piece, please follow these guidelines and submit through our form here.
Heliobas Disciple
TB Fanatic

Scientists Find Natural Protein That Blocks COVID-19 Infection
The human body has a natural defence against COVID-19 which scientists at the University of Sydney say could ...
www.theepochtimes.com
Scientists Find Natural Protein That Blocks COVID-19 Infection
Daniel Y. Teng
Feb 9 2023
The human body has a natural defence against COVID-19 which scientists at the University of Sydney say could pave the path for future vaccines against newer strains.
The team discovered that the body contains a naturally occurring protein, the leucine-rich repeat-containing protein 15 (LRRC15), which ties itself to the COVID-19 virus and does not pass it on to other cells.
“For me, as an immunologist, the fact that there’s this natural immune receptor that we didn’t know about, that’s lining our lungs and blocks and controls virus, that’s crazy interesting,” said Professor Greg Neely, who conducted the research along with PhD researcher Lipin Loo and Matthew Waller from the Charles Perkin Centre.
“We can now use this new receptor to design broad-acting drugs that can block viral infection or even suppress lung fibrosis.”
Loo said, “We think this newly identified protein could be part of our body’s natural response to combating the infection, creating a barrier that physically separates the virus from our lung cells most sensitive to COVID-19.”
Neely told The Epoch Times the amount of LRRC15 in a person’s body determined how serious a person’s COVID symptoms could be, noting the new research could potentially be used to deal with long COVID.
“We are hoping to take this knowledge and use it to create new therapies for long COVID that involve lung fibrosis,” he said in an email.
He also noted that it might not help Long COVID sufferers with the “brain fog component yet.”
The team worked with the researchers at Oxford University in the United Kingdom, as well as Yale and Brown Universities in the United States.
What Does LRRC15 Do to COVID?
The COVID-19 virus infects humans through a spike protein called the angiotensin-converting enzyme 2 (ACE2) receptor which allows it to enter human cells.
Lung cells tend to have high levels of the ACE2 receptors, which is why the virus targets and causes problems for people in this area.
LRRC15 is similar to ACE2 in that it is also a receptor for the COVID-19 virus.
However, the difference with LRRC15 is that it does not support infection. In fact, it sticks to the virus and immobilises it while also preventing other, more vulnerable cells from being infected.
“We think it acts a bit like Velcro, molecular Velcro, in that it sticks to the spike of the virus and then pulls it away from the target cell types,” Loo said.
“Basically, the virus is coated in the other part of the Velcro, and while it’s trying to get to the main receptor, it can get caught up in this mesh of LRRC15,” said Waller from the Charles Perkin Centre.
LRRC15 is common in several parts of the body, including the lungs, skin, tongue, fibroblasts, placenta, and lymph nodes.
Researchers found, however, that it was the lungs that responded most prominently to infection.
“When we stain the lungs of healthy tissue, we don’t see much of LRRC15, but then in COVID-19 lungs, we see much more of the protein,” Loo said.
The team hope the finding of the gene could push further development of antiviral and antifibrotic medicines to deal with future strains or potential lung fibrosis.
“For fibrosis, there are no good drugs: for example, idiopathic pulmonary fibrosis is currently untreatable,” Neely said.
COVID-19 can cause fibrosis to occur by inflaming the lungs leaving them scarred and thickened, resulting in breathing difficulties.
Heliobas Disciple
TB Fanatic

Messenger RNA Sequences Found in Blood 28 Days After COVID-19 Vaccination
Messenger RNA sequences from the Pfizer and Moderna COVID-19 vaccines were found in the blood of multiple individuals ...
www.theepochtimes.com
Messenger RNA Sequences Found in Blood 28 Days After COVID-19 Vaccination
Zachary Stieber
Feb 9 2023
Messenger RNA sequences from the Pfizer and Moderna COVID-19 vaccines were found in the blood of multiple individuals weeks after vaccination, according to a new study.
Researchers in Denmark analyzed samples from the vaccinated and detected partial or even full sequences of the messenger RNA (mRNA) following vaccination. The sequences were found as late as 28 days after vaccination, or the longest time period the study analyzed.
The findings mean that the mRNA, which is situated in lipid nanoparticles for deliverance into the body, lingers for much longer than authorities in the United States and elsewhere acknowledge.
The U.S. Centers for Disease Control and Prevention, for instance, has claimed that the mRNA is broken down “within a few days.” The Infectious Diseases Society of America says the mRNA “is quickly metabolized and eliminated via cellular processing mechanisms.”
Henrik Westh, a professor of clinical microbiology at the University of Copenhagen, and co-authors of the new study described being surprised by the findings.
“We surprisingly found fragments of COVID-19 vaccine mRNA up to 28 days postvaccination in blood from chronic HCV patients vaccinated with mRNA vaccines from both Pfizer-BioNTech and Moderna,” they wrote.
The study featured taking samples from 108 vaccinated people with chronic hepatitis C virus, or HCV, and examining them for up to 28 days after vaccination.
Ten of the samples, or 9.3 percent, had partial or full sequences of the mRNA sequence.
The vaccines deliver mRNA inside lipid nanoparticles.
The researchers said that the detected mRNA was likely still inside the nanoparticles, which “have been slowly released from the injection site either directly to the blood or through the lymph system.” Without the nanoparticles, the mRNA “would rapidly degrade.”
They claimed that the new data “does not in any way change the conclusion that both mRNA vaccines are safe and effective.”
That conclusion shows bias and it overlooks how pseudouridine, which is used to modify the RNA in the vaccines, “alters the stability of RNA considerably,” Dr. Robert Malone told The Epoch Times. Documents leaked in 2022 showed European regulators expressed concern about truncated and modified RNA in the vaccines.
The researchers also said the mRNA lingering in the blood “allows pro-longed spike protein production giving an advantage for a continuous immune response in some persons.”
If true, that would amount to chronic low-level boosting, which would exacerbate immune imprinting, or focusing one’s body on the outdated strains the vaccines target, according to Malone, who helped develop the mRNA technology.
Malone said the difficulty in identifying mRNA specifically from the vaccines, particularly as time goes on, means there may have been RNA from the vaccines in the blood of some of the other samples.
Westh, Pfizer, and Moderna did not respond to a request for comment.
The paper was published by the Journal of Pathology, Microbiology, and Immunology. No funding sources were listed.
Research on mice has detected the spread of the mRNA beyond the injection site and lymph nodes. One previous paper described the finding of mRNA in lymph node germinal centers up to 60 days following vaccination with the Pfizer and Moderna vaccines. Another set of researchers detected mRNA from the vaccines two weeks following vaccination. Research on mice has detected the spread of the mRNA beyond the injection site and lymph nodes.
The papers highlight how “we really don’t know how long this RNA persists,” Malone said. “The true implications of all of this is that the assumption that adverse events occurring later than two to three weeks cannot be associated with the drug product once again is clearly false.”
The mRNA delivers instructions to the body to produce the spike protein, which is meant to protect people against COVID-19.
Experts have raised concerns that the circulating spike protein is toxic and contributes to myocarditis, a form of heart inflammation caused by the vaccines, and other adverse events following vaccination.
“You have the spike causing inflammation, the spike causing clotting, the spike causing amyloid and prion disease, and you have the spike causing all of this autoimmune disease,” Dr. Paul Marik, co-founder of the Front Line COVID-19 Critical Care Alliance, previously told The Epoch Times. “It’s a total onslaught from every angle, and that’s just the beginning of what spike does. It seems the more spike you have, the more inflammation you have.”
In January, U.S. researchers reported discovering high levels of spike protein in people who had been vaccinated and suffered myocarditis.
Several months prior, Colorado researchers reported finding “nearly identical alterations in gene expression” in people with myocarditis after COVID-19 or vaccination, with the alterations detected up to 137 days after infection and 182 days after vaccination. They said that more studies are needed “to define the full extent of the molecular pathology of COVID-19—and mRNA vaccine-associated myocardial injury, including the extent that and how these are triggered by exposure to S[pike] protein.”
Wow. As a child, my family lived in third world countries, so we had to have vaccines that most people don't get. Many of the vaccines were series of three shots over a period on weeks or months, but we had nowhere near 100 shots by the age of 18. What are they doing to our kids?
northern watch
TB Fanatic
Is the following story bs?
February 9 2023
The American Dossier
The global “elite” are attacking eggs by calling them dangerous and deadly after it was revealed that the high-protein superfood is a natural cure for covid.
The World Economic Forum (WEF) tweeted a lie stating that eating eggs “increases the risk of heart attacks and strokes,” the suggestion being that people should stop eating them for their own safety.
We know the truth that covid “vaccines” are responsible for the sudden uptick in heart attacks and strokes being observed all around the world, but the WEF is trying to convince everyone that eggs, which are currently in short supply, are worse than crack cocaine or heroin.
Globalist-aligned “scientists” claim that eating eggs could cause blood clots leading to death – a convenient cover story for the hordes of “fully vaccinated” people who are dying every single day from the injections.
Source: Natural News

 theamericandossier.com
theamericandossier.com
WEF promises to ban “dangerous” eggs following scientific discovery that eating them cures covid naturally
by Ethan HuffFebruary 9 2023
The American Dossier
The global “elite” are attacking eggs by calling them dangerous and deadly after it was revealed that the high-protein superfood is a natural cure for covid.
The World Economic Forum (WEF) tweeted a lie stating that eating eggs “increases the risk of heart attacks and strokes,” the suggestion being that people should stop eating them for their own safety.
We know the truth that covid “vaccines” are responsible for the sudden uptick in heart attacks and strokes being observed all around the world, but the WEF is trying to convince everyone that eggs, which are currently in short supply, are worse than crack cocaine or heroin.
Globalist-aligned “scientists” claim that eating eggs could cause blood clots leading to death – a convenient cover story for the hordes of “fully vaccinated” people who are dying every single day from the injections.
Source: Natural News
WEF promises to ban “dangerous” eggs following scientific discovery that eating them cures covid naturally | The American Dossier
The global “elite” are attacking eggs by calling them dangerous and deadly after it was revealed that the high-protein su...
theamericandossier.com
Heliobas Disciple
TB Fanatic
Is the following story bs?
WEF promises to ban “dangerous” eggs following scientific discovery that eating them cures covid naturally
by Ethan Huff
February 9 2023
The American Dossier
eggs on table by Priscilla Du Preez is licensed under unsplash.com
The global “elite” are attacking eggs by calling them dangerous and deadly after it was revealed that the high-protein superfood is a natural cure for covid.
The World Economic Forum (WEF) tweeted a lie stating that eating eggs “increases the risk of heart attacks and strokes,” the suggestion being that people should stop eating them for their own safety.
We know the truth that covid “vaccines” are responsible for the sudden uptick in heart attacks and strokes being observed all around the world, but the WEF is trying to convince everyone that eggs, which are currently in short supply, are worse than crack cocaine or heroin.
Globalist-aligned “scientists” claim that eating eggs could cause blood clots leading to death – a convenient cover story for the hordes of “fully vaccinated” people who are dying every single day from the injections.
Source: Natural News
WEF promises to ban “dangerous” eggs following scientific discovery that eating them cures covid naturally | The American Dossier
The global “elite” are attacking eggs by calling them dangerous and deadly after it was revealed that the high-protein su...
I think it's BS. I looked through the tweets from the WEF through around Jan 20 and didn't find any such tweet.
There was a study published where the scientists said eggs can cause blood clots though. And we reported here on the thread that there was also a study that eggs are a good remedy for COVID. I remember growing up eggs were great for breakfast, and then eggs were terrible and to be avoided because of cholesterol. For the last 60+ years they haven't been able to make their mind up eggs. Personally I love them and think they're a great source of protein. I have been ignoring the 'studies' since they cholesterol bruhaha. Not a doctor; ymmv....
If you follow the trail of links from the article you posted, you find this article about eggs and choline and blood clots.

Scientists Warn Eggs Are Causing Thousands of People to ‘Suddenly’ Form Blood Clots
Scientists are now warning the public that consuming eggs could cause blood clots, strokes and heart attacks.
 newspunch.com
newspunch.com
Heliobas Disciple
TB Fanatic
The CDC Lied: The mRNA Wasn’t Meant to “Stay in the Arm” ⋆ Brownstone Institute
Why has the CDC been lying about this for the last two years and insisting that the mRNA “stays in the arm?”
The CDC Lied: The mRNA Wasn’t Meant to “Stay in the Arm”
By Robert Kogon
February 10, 2023
The CDC’s information page on Covid-19 vaccines contains the following bullet points on “How mRNA COVID-19 vaccines work:”
First, mRNA COVID-19 vaccines are given in the upper arm muscle or upper thigh, depending on the age of who is getting vaccinated.
After vaccination, the mRNA will enter the muscle cells. Once inside, they use the cells’ machinery to produce a harmless piece of what is called the spike protein…. After the protein piece is made, our cells break down the mRNA and remove it, leaving the body as waste.
Or, in other words, as we have long been told, “it” – the mRNA – “stays in the arm.” And then, after having instructed the muscle cells to produce the spike, is disposed of.But look at the below picture from a recent presentation on mRNA vaccination at the European Parliament. The picture was posted on Twitter by Virginie Joron, a French member of the parliament. The speaker is no less an authority than Özlem Türeci, the Chief Medical Officer of BioNTech: the German biotech company that developed what has come to be known to most of the world as the “Pfizer” Covid-19 vaccine.

Have a closer look at Türeci’s slide, which tells a very different story than that which the CDC has been telling Americans for the last two years.
Far from “staying in the arm” and entering the muscle cells at the injection site, the injection site is only the point of departure for a journey that is supposed to take the mRNA rather to the lymph nodes. The subtitle of the slide is “Bringing mRNA to the right cells at the right places.” The deltoid is not the right place; the lymph nodes are.
Once in the lymph nodes, a specific sort of cell, the dendritic cells, is supposed to manufacture the spike protein: here colorfully described as the “wanted poster” that will help the immune system to identify the SARS-CoV-2 virus in case of subsequent exposure.
A passage from The Vaccine, the book that Türeci and her husband, BioNTech CEO Ugur Sahin, wrote which journalist Joe Miller, explains why BioNTech’s platform specifically targets the lymph nodes:
What Ugur learnt was that the location to which a vaccine delivers its ‘wanted poster’ really mattered. The reason for this, the couple’s team in Mainz later realised, was that not all dendritic cells … were created equal. The ones that resided in lymph nodes – of which the spleen is the largest – were particularly adept at capturing mRNA and making sure the instructions it carried were acted upon. These kidney-bean shaped organs, found under our armpits, in our groins, and at several other outposts in the body, are the information hubs of the immune system. (p. 98)
Indeed, Sahin and Türeci were so determined to get their mRNA into the lymph nodes that they had an earlier mRNA construct injected directly into the patient’s lymph nodes in the groin (p. 104).Needless to say, such an approach was not likely to obtain wide acceptance as a vaccine! This is why the couple, as explained in their book, needed to package the mRNA in lipid nanoparticles, in order to ensure that mRNA administered by way of an intramuscular injection would, nonetheless, be widely distributed around the body and thus reach the lymph nodes.
This is to say that the wide biodistribution of the mRNA that came to light after rollout was never a bug. It is a feature of BioNTech’s mRNA technology. Having elicited an immune response by way of injection into the groin, Sahin is even said to have wondered, “How substantial could the immune response be if a vaccine got into all lymphatic tissues around the body, and recruited all the resident DCs [dendritic cells] into action?” (p. 105)
So, why has the CDC been lying about this for the last two years and insisting that the mRNA “stays in the arm?” Well, the obvious answer is that the idea of the mRNA staying at the injection site is reassuring, since otherwise we could fear systemic adverse effects of precisely the sort that have emerged since rollout.
It is worth noting, moreover, that in developing its vaccine, as discussed in my earlier article here, BioNTech simply skipped the so-called safety pharmacology studies whose purpose is precisely to test a candidate vaccine for potential systemic adverse effects – and regulators, including the FDA, let the company do it.
Heliobas Disciple
TB Fanatic

Extracts From Common Wild Plants Can Block COVID From Entering Human Cells: Study
Two plants that can be found throughout North American wilderness contain ingredients that can block COVID-19 virus from entering human cells, a study says.
www.theepochtimes.com
Extracts From Common Wild Plants Can Block COVID From Entering Human Cells: Study
Bill Pan
Feb 10 2023
Two plants that can be found throughout North American wilderness contain ingredients that can block the virus that causes COVID-19 from entering human cells, a recent study says.
After testing 1,867 samples extracted from different parts of 660 plant and fungal species, a team of scientists at Emory University in Georgia reported that extracts from the flowers of tall goldenrod (Solidago altissima) and the rhizomes of the eagle fern (Pteridium aquilinum) each prevented the viral spike protein of SARS-CoV-2 from attaching to human cells in lab settings.
Both plants are native to North America. In fact, they are known to be used by Native American peoples as herbal remedies, the scientists noted.
Tall goldenrod flowers were reported to be used as burn dressings and applied to ulcers by the Ojibwe tribe, according to the study. Meanwhile, eagle fern is part of the diet across many indigenous tribes and has a long history of varied uses including antiseptic and anthelminthic.
With that said, the scientists advised against people trying to treat COVID with the plants, considering that actually effective compounds are only present in minuscule quantities in the plants. Not to mention that all parts of eagle fern are toxic.
“It’s very early in the process, but we’re working to identify, isolate and scale up the molecules from the extracts that showed activity against the virus,” Cassandra Quave, the study’s co-author and a botanist specialized in traditional medicine at Emory University, said in a press release. “Once we have isolated the active ingredients, we plan to further test for their safety and for their long-range potential as medicines against COVID-19.”
Studies show that COVID enters by binding its spike protein to a receptor, called ACE2, on the surface of the host cell. “The viral spike protein uses the ACE2 protein almost like a key going into a lock, enabling the virus to break into a cell and infect it,” Quave said.
For their experiment, Emory scientists used virus-like particles (VLPs), which are COVID-based viruses stripped of the genetic information needed to cause infection; and human cells programmed to overexpress ACE2 on their surface. The VLP was programmed in a way that once it successfully bonded to an ACE2 protein and made entry, it would produce a fluorescent green protein.
Scientists added a plant extract to the cells in a petri dish before introducing the VLPs. They then shined a fluorescent light on the dish to see if the VLP had made it into the cells and produced the green protein.
Tall goldenrod and eagle fern extract both “demonstrated robust activity at lower concentrations, as well as minimal cytotoxicity at higher concentrations,” according to the study. They also showed antiviral effects in COVID-infected cell culture.
“Plants have such chemical complexity that humans probably couldn’t dream up all the botanical compounds that are waiting to be discovered,” said Caitlin Risener, the study’s leading author. “The vast medicinal potential of plants highlights the importance of preserving ecosystems.”
The study was published in Scientific Reports on Jan. 23.
Heliobas Disciple
TB Fanatic
View: https://twitter.com/Baklava_USA/status/1624203591627182080
ʟᴇғᴛ ᴄᴏᴀˢᴛ ᴠᴀɢʀᴀɴᴛ@Baklava_USA
7:28 PM · Feb 10, 2023
Dr. Ryan Cole’s Biopsy Results May Explain The Shocking Rise In “Mysterious” Cancers — He Explains There Is Spike Protein “Inside Every Single Cancer Cell” “What’s inside of every cancer cell? Spike protein. Every malignant B-cell has spike protein in it.”
VIDEO AT LINK: 55 seconds
ʟᴇғᴛ ᴄᴏᴀˢᴛ ᴠᴀɢʀᴀɴᴛ@Baklava_USA
7:28 PM · Feb 10, 2023
Dr. Ryan Cole’s Biopsy Results May Explain The Shocking Rise In “Mysterious” Cancers — He Explains There Is Spike Protein “Inside Every Single Cancer Cell” “What’s inside of every cancer cell? Spike protein. Every malignant B-cell has spike protein in it.”
VIDEO AT LINK: 55 seconds
Heliobas Disciple
TB Fanatic

“Failure” of COVID-Era Air Travel Measures Revealed Through Plane Wastewater Testing
Almost all planes arriving at three UK airports during a period of COVID restrictions had the SARS CoV-2 virus in their wastewater, according to newly published research. Almost all planes arriving at three UK airports during a period of Covid restrictions had the SARS CoV-2 virus in their wastew
scitechdaily.com
"Failure” of COVID-Era Air Travel Measures Revealed Through Plane Wastewater Testing
By Bangor University
February 10, 2023
Almost all planes arriving at three UK airports during a period of COVID restrictions had the SARS CoV-2 virus in their wastewater, according to newly published research.
Almost all planes arriving at three UK airports during a period of Covid restrictions had the SARS CoV-2 virus in their wastewater, according to newly published research. The virus was also found in wastewater at arrival terminals.
Bangor University scientists, who pioneered the use of wastewater testing to track SARS-CoV2 in the UK, wanted to find out whether wastewater testing could be used as a way of monitoring the general health of passengers on flights coming into the country in future. The study was funded by the UK’s Health Security Agency and is published in PLOS Global Public Health.
The team tested the toilet tank water taken from long haul and short haul flights entering the UK at Heathrow, Edinburgh and Bristol airports over a three-week period between 8-31 March 2022. Samples were also collected from sewers connected to the arrival halls in the airport terminals and at a wastewater treatment plant in the vicinity of each airport.
The COVID-19 restrictions were lifted in England on March 18th, 2022, removing the requirement for unvaccinated passengers to take a pre-departure test and a day 2 post arrival test to prove their Covid status. But the researchers found little difference in the concentrations of SARS-CoV-2 in wastewater before and after that date.
Professor Davey Jones from Bangor University’s School of Natural Sciences, said,“Despite all the intervention measures that the UK had in place to try to stop people with the illness getting on flights to the UK, almost every single plane we tested contained the virus, and most of the terminal sewers too. That might have been because people developed symptoms after testing negative; or were evading the system, or for some other reason. But it showed that there was essentially a failure of border control in terms of Covid surveillance.”
Earlier research by the team may explain why. In a poll of 2000 adults, 23% of respondents admitted that they had previously boarded a flight back to the UK while feeling ill. That survey also asked respondents about their toilet habits on flights, and found that 13% of individuals catching a short haul flight would be likely to defecate on the plane; with a higher proportion seen in long haul passengers, at around 36% of the total. Based on this information, together with Covid shedding rates, the team estimated that if wastewater sampling was set up at airports in future, it could capture 8-14% of SARS-CoV-2 cases entering the UK via air travel.
The researchers believe wastewater sampling could form part of a future infectious disease surveillance system for the UK. Future sampling could also pick up other infections, such as Norovirus or Enterovirus, potentially giving a clearer picture of what pathogens are entering the country.
Researcher Dr Kata Farkas said: “This is about getting an overall picture to help UK health systems to be prepared, or, if possible, have an advance warning, of emerging diseases. It wouldn’t be feasible to test every flight arriving, but taking wastewater from arrivals at a single airport terminal used for long-haul arrivals may provide an estimate of diseases entering the country.”
She added: “At the moment we have no idea how many people come into the country carrying different diseases, partly because no one wants to be tested on the spot. Wastewater monitoring gives us a snapshot of the infectious diseases passengers may carry upon arrival.”
Reference: “Wastewater-based monitoring of SARS-CoV-2 at UK airports and its potential role in international public health surveillance” by Kata Farkas, Rachel Williams, Natasha Alex-Sanders, Jasmine M. S. Grimsley, Igor Pântea, Matthew J. Wade, Nick Woodhall and Davey L. Jones, 19 January 2023, PLOS Global Public Health.
DOI: 10.1371/journal.pgph.0001346
Heliobas Disciple
TB Fanatic

VSS Scientific Updates During Pandemic Times #52 | Voice for Science and Solidarity
VSS Scientific Updates During Pandemic Times #52 : How Does SARS-CoV-2 Affect Other Respiratory Diseases? Geert RespondsFrom Geert: The auth
 www.voiceforscienceandsolidarity.org
www.voiceforscienceandsolidarity.org
VSS Scientific Updates During Pandemic Times #52
By Geert Vanden Bossche
February 10, 2023
1. How Does SARS-CoV-2 Affect Other Respiratory Diseases? Geert Responds
From Geert: The author of this article lacks a basic understanding of how our immune system fights off acute, self-limiting diseases. They are so obsessed with intervening in the immune system that they have completely forgotten about the crucial role of our first line of defense, the innate immune system. They have no understanding that the cell-based innate immune system can be strengthened by exposure to several different viruses causing acute, self-limiting diseases. Don't they realize that this type of immune defense is virus-nonspecific and that exposure to SARS-CoV-2 also strengthens our first line of defense against other respiratory diseases? Have they never wondered why childhood vaccines, all of which are live attenuated, are so successful that they have never been replaced by "modern" vaccines, such as those using subunit or recombinant vaccine technologies? For many months, people have not been respecting social distancing, wearing masks, or adhering to other infection-prevention measures. For many months, circulating variants have been highly infectious. Nevertheless, this author has cherry-picked some cheap data to make people believe that precisely these measures, at a time when they are no longer respected, have caused reduced transmission of highly transmissible circulating variants and this is now responsible for an "immunity gap" and promoting the occurrence of other infectious diseases.Of course, this must be true, as even mathematical modeling, which we all know fails miserably over and over again due to uninformed assumptions, has proven this! How can this immunity gap be more pronounced in babies and children? Aren't they immunologically naïve anyway? The author is even invoking the hygiene theory and suggesting that the sterile environment generated by the no longer existing infection-prevention measures are causing a lack of exposure. What the author seems to be unaware of is that the bulk of other respiratory diseases consists of RSV and flu infections. It is unlikely that this juvenile author has any understanding of how highly activated cytolytic T cells enable C-19 vaccinees to spread RSV and influenza asymptomatically, whereas both infections usually cause symptoms. This has to do with CTL-mediated targeting of a shared (‘universal’) T cell peptide in host cells infected by these enveloped glycosylated viruses. Asymptomatic shedding of RSV and influenza by C-19 vaccinees is causing high infectious pressure in highly vaccinated countries. It is therefore not surprising that those who are immunologically naïve (children are typically not vaccinated against RSV or flu for different reasons) and not equipped with C-19 activated CTLs have a higher chance of being infected because of enhanced exposure! The surge of respiratory infections in immunologically naïve individuals is therefore to be considered a direct consequence of a high rate of C-19 vaccination and not a lack of exposure. As I have predicted, these waves will calm down as natural immunity in babies and children will be strengthened and ultimately protect them from disease. Although C-19 vaccination provides temporary relief from these diseases, this protection is temporary and very fragile. The unbelievers can read my upcoming book or wait and see. In addition, C-19 vaccination sidelines the cell-based innate immune system, which is key to enabling full-fledged natural immunity against a multitude of other acute, self-limiting viral infections.
This is yet another example of how blatant immunological illiteracy drives young and inexperienced scientists (https://www.ibt.unam.mx/perfil/4311/mc-alicia-helena-marquez-bandala) to swallow the narrative and erroneously advise parents to vaccinate their young children:
“In the case of COVID-19, it is not planned to vaccinate children under 5 years of age, and if we do not vaccinate children under 5 years of age, that gap will exist. In addition, this winter season will be important to know whether we are already endemic or not”.
Not having any relevant immunological insight and blindly citing other scientists who believe that endemicity is still within reach speaks volumes about the value of this article. We have no choice but to continue destroying this simplistic but dangerous line of reasoning.
https://www.medscape.com/viewarticle/987277?icd=login_success_email_match_norm#vp_2
2. U.S. Investigating First Cases of "Concerning" New Drug-resistant Gonorrhea Strain
“The Massachusetts cases are the first confirmed in the lab to have developed the ability to sidestep six of the seven drugs that health authorities track for potential resistance. It carries a change to the "penA60 allele" – a gene mutation – which has been linked to previous ceftriaxone-resistant cases in Nevada, the United Kingdom, and Asia.”U.S. investigating first cases of "concerning" new drug-resistant gonorrhea strain
3. Relatives Angry as Covid Kept Off Chinese Death Certificates
“It’s absurd. Someone dies and we can’t even accurately write the cause,” the 23-year-old said, asking to be identified only by her surname.Subscribe to read | Financial Times
4. Alarming Antibody Evasion Properties of Rising SARS-CoV-2 BQ and XBB Subvariants
“considering the extensive herd immunity built up in the population over the last three years from infections and vaccinations.”From Geert: “This publication illustrates once more the immunological illiteracy of mutation spotters who continue to make people believe that the population has established herd immunity! They are confusing population-level immune PRESSURE (‘herd immune pressure’) on the virus with herd immunity! No population establishing herd immunity breeds immune escape variants that dominantly (co-)circulate! An immune escape pandemic can never generate herd immunity and vice versa! This is a contradictio in terminis! Their immunological ignorance is an insult to the science.”
Alarming antibody evasion properties of rising SARS-CoV-2 BQ and XBB subvariants - PubMed
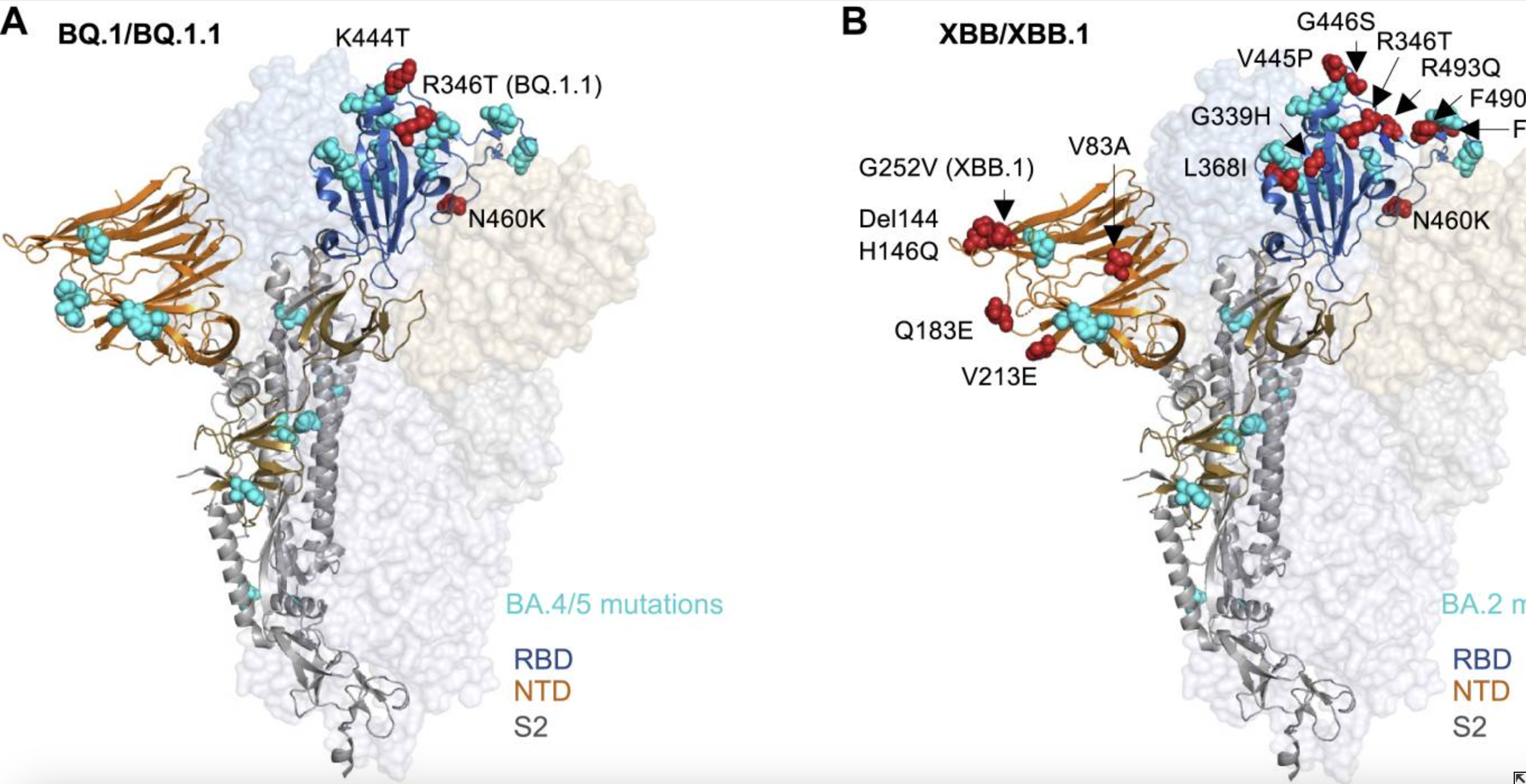
5. Covid Booster Jabs for Elderly to Continue This Year
“Government also prepares to launch emergency surge vaccinations if novel variant of sufficient concern emerges”Covid booster jabs for elderly to continue this year
6. The FAA Has Very Quietly Tacitly Admitted that the EKGs of Pilots are No Longer Normal
“In the October 2022 version of the FAA Guide for Aviation Medical Examiners, the FAA quietly widened the EKG parameters beyond the normal range (from a PR max of .2 to unlimited). And they didn’t widen the range by a little. They widened it by a lot. It was done after the vaccine rollout.”The FAA has very quietly tacitly admitted that the EKGs of pilots are no longer normal. We should be concerned. Very concerned.
7. Do COVID-19 RNA-Injections Affect Male Fertility? Latest Facts and Perspective
"Unexplained" significant decline in fertility exactly 9 months after the start of the vaccination campaign.Male fertility and Covid vaccine: New german study • Pure Fertility
Heliobas Disciple
TB Fanatic
Geert spoke at a conference and he posted the slides he used during the presentation at the following link. There are way too many to bring over so I am only copying over the ones that advertise the conference. Go to the link to see all the ones he used while he spoke. Hopefully a video will show up of his presentation too....
 www.voiceforscienceandsolidarity.org
(fair use applies)
www.voiceforscienceandsolidarity.org
(fair use applies)
Pandemic Strategies: Lessons and Consequences – International Conference in Stockholm
By Geert Vanden Bossche
February 10, 2023


Pandemic Strategies: Lessons and Consequences – International Conference in Stockholm | Voice for Science and Solidarity
Pandemic Strategies: Lessons and Consequences – International Conference in Stockholm
www.voiceforscienceandsolidarity.org
Pandemic Strategies: Lessons and Consequences – International Conference in Stockholm
By Geert Vanden Bossche
February 10, 2023
Tristan
TB Fanatic
Don't know if this has been posted yet, but here's an interview Russel Brand did with Dr. John Campbell posted to Rumble on Feb. 10th. Discusses many issues regarding the pandemic, the responses especially, and the control mechanism which were used to stifle actual scientific discussion... among other things.
 rumble.com
rumble.com
rt: 1:08:02
Dr John Campbell: You Were Right! - #078 - Stay Free With Russell Brand
Russell chats to Dr John Campbell, a retired nurse educator who holds a Master of Science in health science and Ph.D. in nursing. John came to prominence on YouTube during the pandemic, with audiences
rumble.com
rt: 1:08:02
Heliobas Disciple
TB Fanatic

New York lets COVID-19 health care mask requirements lapse
ALBANY, N.Y. (AP) — New York state officials said they will allow COVID-19-related masking requirements for staff and visitors in hospitals and other health care facilities to lapse on Sunday. Acting Health Commissioner Dr.
 apnews.com
apnews.com
New York lets COVID-19 health care mask requirements lapse
February 11, 2023
ALBANY, N.Y. (AP) — New York state officials said they will allow COVID-19-related masking requirements for staff and visitors in hospitals and other health care facilities to lapse on Sunday.
Acting Health Commissioner Dr. James McDonald said that while the pandemic is not over, “we are moving to a transition.”
“As we do, and with safe and effective vaccines, treatments, and more, we are able to lift the state’s masking requirement in health care settings,” McDonald said in a statement.
The decision announced Thursday comes as governments continue to relax rules enacted during the most intense days of the pandemic.
Earlier this week New York City announced it would no longer require COVID-19 vaccinations for police, firefighters, teachers and other municipal employees.
The statewide number of COVID-19 hospitalizations has been steadily dropping this year and as of Thursday stood at 2,176.
Health officials advised hospitals, nursing homes, treatment centers and other facilities to enact their own masking rules in accordance with guidance form the Centers for Disease Control.
___
This story has been corrected to remove a reference that said the masking requirement had applied to patients, which it did not.
Heliobas Disciple
TB Fanatic

Top US Officials Discussed 'Adverse Event Issue' With COVID-19 Vaccines and Pregnancy: Emails
Top U.S. health officials were concerned with an "adverse event issue" concerning COVID-19 vaccines being injected during pregnancy, ...
www.theepochtimes.com
Top US Officials Discussed ‘Adverse Event Issue’ With COVID-19 Vaccines and Pregnancy: Emails
Zachary Stieber
Feb 11 2023
Top U.S. health officials were concerned with an “adverse event issue” concerning COVID-19 vaccines being injected during pregnancy, according to newly disclosed emails.
On May 14, 2021, officials with the U.S. Food and Drug Administration (FDA) and U.S. Centers for Disease Control and Prevention (CDC) were exchanging emails about language concerning the co-administration of COVID-19 vaccines with other vaccines during pregnancy.
“Please let me know if you want to connect about the adverse event issue later today. Seems like work is still ongoing, but let me know,” Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, wrote to colleagues at both agencies.
Dr. Amanda Cohn, chief medical officer of the CDC’s National Center for Immunizations and Respiratory Diseases, replied.
“We have a meeting with Rochelle at 3:30 about if we should say anything or wait until we have more definitive information … I will let you know where we land,” Cohn wrote. Dr. Rochelle Walensky is the head of the CDC.
“I’m not sure there is a right answer,” Cohn added.
The emails (pdf) were obtained by the nonprofit Judicial Watch, which sued the U.S. government for failing to appropriately respond to a Freedom of Information Act request for messages regarding adverse events, deaths, and/or injuries caused by the COVID-19 vaccines.
Adverse events include health issues such as arthritis or heart inflammation.
No other emails about the “adverse event issue” were included in the latest tranche obtained by the nonprofit.
“I respectfully decline to comment,” Marks told The Epoch Times in an emailed statement when asked what the issue was.
Cohn and the CDC did not respond to requests for comment.
The CDC currently recommends virtually all Americans aged 6 months and older, including pregnant women, get a COVID-19 vaccine and multiple booster shots.
The original trials did not include enough information “to make conclusions about the safety of the” vaccines from Pfizer, Moderna, and Johnson & Johnson, according to FDA documents.
Authorities have relied on observational data, including a study from the CDC, a corrected version of which was published in October 2021.
Pfizer conducted a post-authorization trial of its vaccine in pregnant women that was labeled completed in mid-2022 but results have not been reported publicly as of yet.
“We think that part of the reason is because the results are so bad,” Linda Wastila, a professor at the University of Maryland, told The Epoch Times.
Pfizer did not respond to a request for comment.
Confidentiality Agreement
The FDA vaccine advisory committee met on Dec. 10, 2020, to consider whether to advise the FDA to authorize Pfizer’s vaccine.
During the meeting, officials revealed that two postvaccination cases of severe allergic shock (anaphylaxis) had been recorded in the United Kingdom out of 6,000 doses administered on the day the events occurred.
“At this point, we are seeking further information from the MHRA under our confidentiality agreement to learn more about this and to really tease that out,” Marion Gruber, an FDA official at the time, told the panel.
The Medicines and Healthcare products Regulatory Agency (MHRA) is the British equivalent of the FDA.
The newly obtained set of emails showed U.S. and UK officials discussing the cases of anaphylaxis throughout December, including as early as Dec. 9, 2020.
Marks wrote that it would “be very helpful if our Office of Vaccines could receive additional details” from MHRA “under the terms of our mutual confidentiality agreement.” Jonathan Mogford, a UK official, sent back data, adding, “If I can just remind—information shared under our confidentiality agreement.”
The MHRA declined to provide a copy of the confidentiality agreement, and the FDA did not respond to emailed questions about the pact.
“It again took a lawsuit for the Biden administration to hand over, albeit heavily redacted, information regarding the safety of the COVID vaccines that the public has every right to know,” Judicial Watch President Tom Fitton said in a statement. “This disturbing batch of new documents have uncovered a secret confidentiality agreement tied to COVID vaccine safety issues and emails that raise new questions about the vaccines and pregnancy.”
The Epoch Times has submitted Freedom of Information Act requests to try to uncover more information about the adverse event issue and the confidentiality agreement. Previous requests have unearthed secret data on COVID-19 vaccines, including showing how the CDC identified hundreds of potential safety issues with the Pfizer and Moderna vaccines.
People with a history of severe allergic reaction to any vaccine were excluded from Pfizer’s trial and people with a history of allergic reactions to any components of the Moderna vaccine were excluded from Moderna’s trial. No such exclusions were reported for the Johnson & Johnson trial.
The fact sheets for all three vaccines in the United States were updated to include warnings about severe allergic shock, including saying the vaccine should not be administered to people with a known history of severe allergic reaction to any components of the shot.
Heliobas Disciple
TB Fanatic

Scientists Discover Protein in the Lungs That Blocks COVID-19 Infection – “Natural Protective Barrier”
The protein receptor found in the lungs sticks to the virus and pulls it away from the target cells. University of Sydney scientists have discovered a protein in the lung that blocks SARS-CoV-2 infection and forms a natural protective barrier in the human body. This protein, the leucine-rich r
scitechdaily.com
Scientists Discover Protein in the Lungs That Blocks COVID-19 Infection – “Natural Protective Barrier”
By University of Sydney
February 11, 2023
Immunofluorescent staining shows expression of the new SARS-CoV-2 Spike-receptor LRRC15 (green) in post-mortem lung tissue section from individual with COVID-19. Credit: The University of Sydney
The protein receptor found in the lungs sticks to the virus and pulls it away from the target cells.
University of Sydney scientists have discovered a protein in the lung that blocks SARS-CoV-2 infection and forms a natural protective barrier in the human body.
This protein, the leucine-rich repeat-containing protein 15 (LRRC15), is an inbuilt receptor that binds the SARS-CoV-2 virus without passing on the infection.
The research opens up an entirely new area of immunology research around LRRC15 and offers a promising pathway to develop new drugs to prevent viral infection from coronaviruses like COVID-19 or deal with fibrosis in the lungs.
The study was published on February 9, 2023, in the journal PLOS Biology. It was led by Professor Greg Neely with his team members Dr. Lipin Loo, a postdoctoral researcher, and PhD student Matthew Waller at the Charles Perkins Centre and the School of Life and Environmental Sciences.
The University study is one of three independent papers that reveal this specific protein’s interaction with COVID-19.
“Alongside two other groups, one at Oxford, the other at Brown and Yale in the USA, we found a new receptor in the LRRC15 protein that can stop SARS-CoV-2. We found that this new receptor acts by binding to the virus and sequestering it which reduces infection,” Professor Neely said.
“For me, as an immunologist, the fact that there’s this natural immune receptor that we didn’t know about, that’s lining our lungs and blocks and controls virus, that’s crazy interesting.
“We can now use this new receptor to design broad-acting drugs that can block viral infection or even suppress lung fibrosis.”
What is LRRC15?
The COVID-19 virus infects humans by using a spike protein to attach to a specific receptor in our cells. It primarily uses a protein called the angiotensin-converting enzyme 2 (ACE2) receptor to enter human cells. Lung cells have high levels of ACE2 receptors, which is why the COVID-19 virus often causes severe problems in this organ of infected people.
Like ACE2, LRRC15 is a receptor for coronavirus, meaning the virus can bind to it. But unlike ACE2, LRRC15 does not support infection. It can, however, stick to the virus and immobilize it. In the process, it prevents other vulnerable cells from becoming infected.
“We think it acts a bit like Velcro, molecular Velcro, in that it sticks to the spike of the virus and then pulls it away from the target cell types,” Dr. Loo said.
“Basically, the virus is coated in the other part of the Velcro, and while it’s trying to get to the main receptor, it can get caught up in this mesh of LRRC15,” Mr. Waller said.
LRRC15 is present in many locations such as lungs, skin, tongue, fibroblasts, placenta and lymph nodes. But the researchers found human lungs light up with LRRC15 after infection.
“When we stain the lungs of healthy tissue, we don’t see much of LRRC15, but then in COVID-19 lungs, we see much more of the protein,” Dr. Loo said.
“We think this newly identified protein could be part of our body’s natural response to combating the infection creating a barrier that physically separates the virus from our lung cells most sensitive to COVID-19.”
Implications of the research
“When we studied how this new receptor works, we found that this receptor also controls antiviral responses, as well as fibrosis, and could link COVID-19 infection with lung fibrosis that occurs during long COVID,” Mr. Waller said.
“Since this receptor can block COVID-19 infection, and at the same time activate our body’s anti-virus response, and suppress our body’s fibrosis response, this is a really important new gene,” Professor Neely said.
“This finding can help us develop new antiviral and antifibrotic medicines to help treat pathogenic coronaviruses, and possibly other viruses or other situations where lung fibrosis occurs.
“For fibrosis, there are no good drugs: for example, idiopathic pulmonary fibrosis is currently untreatable.”
Fibrosis is a condition in which lung tissue becomes scarred and thickened, causing breathing difficulties. COVID-19 can cause inflammation and damage to the lungs, leading to fibrosis.
The authors said they are developing two strategies against COVID-19 using LRRC15 that could work across multiple variants – one which targets the nose as a preventative treatment, and another aimed at the lungs for serious cases.
The researchers also said that the presence or lack of LRRC15, which is involved in lung repair, is an important indication of how severe a COVID-19 infection might become.
“A group at Imperial College London independently found that absence of LRRC15 in the blood is associated with more severe COVID, which supports what we think is happening.” Dr. Loo said. “If you have less of this protein, you likely have serious COVID. If you have more of it, your COVID is less severe.
“We are now trying to understand exactly why this is the case.”
The research involved screening human cell cultures for genes and investigating the lungs of human COVID-19 patients.
Reference: “Fibroblast-expressed LRRC15 is a receptor for SARS-CoV-2 spike and controls antiviral and antifibrotic transcriptional programs” by Lipin Loo, Matthew A. Waller, Cesar L. Moreno, Alexander J. Cole, Alberto Ospina Stella, Oltin-Tiberiu Pop, Ann-Kristin Jochum, Omar Hasan Ali, Christopher E. Denes, Zina Hamoudi, Felicity Chung, Anupriya Aggarwal, Jason K. K. Low, Karishma Patel, Rezwan Siddiquee, Taeyoung Kang, Suresh Mathivanan, Joel P. Mackay, Wolfram Jochum, Lukas Flatz, Daniel Hesselson, Stuart Turville and G. Gregory Neely, 8 February 2023, PLOS Biology.
DOI: 10.1371/journal.pbio.3001967
Funding: National Health and Medical Research Council, New South Wales Government, Australian Government
Heliobas Disciple
TB Fanatic
Good News: Most Long COVID Effects Resolve Within a Year After a Mild Infection
Researchers found that most infected individuals do not experience significant long-term illness as a result of a mild case of the disease. According to a large study from Israel published in The BMJ, most symptoms or conditions that arise following a mild case of COVID-19 tend to persist for sever
scitechdaily.com
Good News: Most Long COVID Effects Resolve Within a Year After a Mild Infection
By BMJ
February 12, 2023
Long COVID refers to the phenomenon of people continuing to experience symptoms of the disease long after the initial infection has cleared. This can include symptoms such as fatigue, brain fog, and shortness of breath, among others. While the exact cause of Long COVID is still not fully understood, researchers believe it may be related to lingering inflammation in the body or ongoing damage to certain organs.
Researchers found that most infected individuals do not experience significant long-term illness as a result of a mild case of the disease.
According to a large study from Israel published in The BMJ, most symptoms or conditions that arise following a mild case of COVID-19 tend to persist for several months, but typically return to normal within a year.
Specifically, the study found that individuals who have been vaccinated are at a reduced risk of developing breathing difficulties, the most prevalent effect to occur following a mild case of COVID-19, compared to those who have not been vaccinated.
These findings suggest that, although the long covid phenomenon has been feared and discussed since the beginning of the pandemic, the vast majority of mild disease cases do not suffer serious or chronic long-term illness, say the researchers.
Long covid is defined as symptoms persisting or new symptoms appearing more than four weeks after initial infection. In March 2022, an estimated 1.5 million people in the UK (2.4% of the population) reported long covid symptoms, mainly fatigue, shortness of breath, loss of smell, loss of taste, and difficulty concentrating.
But the clinical effects of long covid one year after mild infection and their association with age, sex, covid-19 variants, and vaccination status are still unclear.
To address this, researchers compared the health of uninfected individuals with those who had recovered from mild covid-19 for a year after infection.
They used electronic records of a large public healthcare organization in Israel, in which almost 2 million members were tested for covid-19 between 1 March 2020 and 1 October 2021. Over 70 long covid conditions were analyzed in a group of infected and matched uninfected members (average age 25 years; 51% female).
They compared conditions in unvaccinated people, with and without covid-19 infection, controlling for age, sex, and covid-19 variants, during early (30-180 days) and late (180-360 days) time periods after infection. Conditions in vaccinated versus unvaccinated people with covid-19 were also compared over the same time periods.
To ensure only mild disease was assessed, they excluded patients admitted to hospitals with more serious illnesses. Other potentially influential factors, such as alcohol intake, smoking status, socioeconomic level, and a range of pre-existing chronic conditions were also taken into account.
Covid-19 infection was significantly associated with increased risks of several conditions including loss of smell and taste, concentration and memory impairment, breathing difficulties, weakness, palpitations, streptococcal tonsillitis, and dizziness in both early and late time periods, while hair loss, chest pain, cough, muscle aches and pains and respiratory disorders resolved in the late period.
For example, compared with non-infected people, mild covid-19 infection was associated with a 4.5-fold higher risk of smell and taste loss (an additional 20 people per 10,000) in the early period and an almost 3-fold higher risk (11 per 10,000 people) in the late period.
The overall burden of conditions after infection across the 12-month study period was highest for weakness (an additional 136 people per 10,000) and breathing difficulties (107 per 10,000).
When conditions were assessed by age, breathing difficulties were the most common, appearing in five of the six age groups but remaining persistent throughout the first year post-infection in the 19-40, 41-60, and over 60 years age groups.
Weakness appeared in four of the six age groups and remained persistent in the late phase only in the 19-40 and 41-60 age groups.
Male and female patients showed minor differences, and children had fewer outcomes than adults during the early phase of covid-19, which mostly resolved in the late period. Findings were similar across the wild-type, Alpha, and Delta covid-19 variants.
Vaccinated people who became infected had a lower risk of breathing difficulties and similar risk for other conditions compared with unvaccinated infected patients.
The researchers point to some limitations, such as incomplete measurement within medical records, so data might not fully reflect diagnoses and outcomes reported. And they can’t rule out the possibility that covid-19 patients may use healthcare services more frequently, resulting in higher reporting and increased screening for potential covid-related outcomes in these patients.
Nevertheless, this was a large detailed analysis of health records across a diverse population, representing one of the longest follow-up studies in patients with mild covid-19 to date. And findings should apply to similar western populations worldwide.
“Our study suggests that mild covid-19 patients are at risk for a small number of health outcomes and most of them are resolved within a year from diagnosis,” say the researchers.
“Importantly, the risk for lingering dyspnoea was reduced in vaccinated patients with breakthrough infection compared with unvaccinated people, while risks of all other outcomes were comparable,” they add.
Reference: “Long covid outcomes at one year after mild SARS-CoV-2 infection: nationwide cohort study” by Barak Mizrahi, Tamar Sudry, Natalie Flaks-Manov, Yoav Yehezkelli, Nir Kalkstein, Pinchas Akiva, Anat Ekka-Zohar, Shirley Shapiro Ben David, Uri Lerner, Maytal Bivas-Benita and Shira Greenfeld, 11 January 2023, The BMJ.
DOI: 10.1136/bmj-2022-072529
Hfcomms
EN66iq
One of my employees now has cancer. I told him when those vaccine first rolled out to stay away from them but he is a type-2 diabetic and basically hangs on every word his doctor says. The doctor said he should get the vaccine and I know he got the first and second shots but I don't think he got the booster.
I know he had a colonoscopy and had a few polyps that needed to be removed and also had a hernia that needed repair so he went into the hospital last Monday. They were going to do both procedures laparoscopically and found out today he is still in the hospital and has 'complications' which I don't know the extent of. But, I was also told he has cancer and will at least have to do some mild chemo.
So I'm guessing that when they took the polyps that they were cancerous or pre-cancerous but I don't know for sure. Of course there is no way to directly link this to his shots but every since he received them he has been a little bit off at times with not being able to finish a sentence or losing his train of thought and he is only in his early 60's and never had that issue before the shots.
So, time will tell but the shots have already attrited his immune system and adding any chemo to the mix isn't going to help much I don't think.
I know he had a colonoscopy and had a few polyps that needed to be removed and also had a hernia that needed repair so he went into the hospital last Monday. They were going to do both procedures laparoscopically and found out today he is still in the hospital and has 'complications' which I don't know the extent of. But, I was also told he has cancer and will at least have to do some mild chemo.
So I'm guessing that when they took the polyps that they were cancerous or pre-cancerous but I don't know for sure. Of course there is no way to directly link this to his shots but every since he received them he has been a little bit off at times with not being able to finish a sentence or losing his train of thought and he is only in his early 60's and never had that issue before the shots.
So, time will tell but the shots have already attrited his immune system and adding any chemo to the mix isn't going to help much I don't think.
Zoner
Veteran Member
Sorry HfOne of my employees now has cancer. I told him when those vaccine first rolled out to stay away from them but he is a type-2 diabetic and basically hangs on every word his doctor says. The doctor said he should get the vaccine and I know he got the first and second shots but I don't think he got the booster.
I know he had a colonoscopy and had a few polyps that needed to be removed and also had a hernia that needed repair so he went into the hospital last Monday. They were going to do both procedures laparoscopically and found out today he is still in the hospital and has 'complications' which I don't know the extent of. But, I was also told he has cancer and will at least have to do some mild chemo.
So I'm guessing that when they took the polyps that they were cancerous or pre-cancerous but I don't know for sure. Of course there is no way to directly link this to his shots but every since he received them he has been a little bit off at times with not being able to finish a sentence or losing his train of thought and he is only in his early 60's and never had that issue before the shots.
So, time will tell but the shots have already attrited his immune system and adding any chemo to the mix isn't going to help much I don't think.
I just said a prayer for him. May he know the LORD.
northern watch
TB Fanatic
Judicial Watch: Records Show U.S. and UK ‘Confidentiality Agreement’ Tied to Vaccine Adverse Events
February 10 2023
(Washington, DC) – Judicial Watch announced today it received 57 pages of heavily redacted records from the U.S. Department of Health and Human Services (HHS) that show, just two days prior to FDA approval of the Pfizer-BioNTech COVID-19 vaccine, a discussion between U.S. and UK health regulators regarding the COVID shot and “anaphylaxis,” with the regulators emphasizing their “mutual confidentiality agreement.”
Judicial Watch obtained the records through a Freedom of Information Act (FOIA) lawsuit against HHS (Judicial Watch v. U.S. Department of Health and Human Services (No. 1:22-cv-00660)) after the Food and Drug Administration (FDA), which is an agency of HHS, failed to respond to an August 30, 2021, FOIA request for:
All emails sent to and from members of the Vaccines and Related Biological Products Advisory Committee regarding adverse events, deaths and/or injuries caused by investigatory vaccines for the prevention or treatment of SARS-CoV-2 and/or COVID-19 currently produced by Pfizer/BioNTech, Moderna and/or Johnson & Johnson.
The Vaccines and Related Biological Products Advisory Committee (VRBPAC) is the U.S. Government’s central advisory body, along with Advisory Committee on Immunization Practices (ACIP), advising whether to approve COVID vaccines.
A lengthy, heavily redacted December 2020 email exchange shows U.S. and UK health officials placing a heavy emphasis on their “mutual confidentiality agreement” in a discussion regarding “anaphylactoid reactions” to the COVID vaccine.
The exchange is initiated by Jonathan Mogford, policy director of the UK’s Medicines and Healthcare Products Regulatory Agency and is sent to Acting FDA Commissioner Janet Woodcock as well as Peter Marks, director of the Center for Biologics Evaluation and Research (CBER). The subject line and body of the email are fully redacted under FOIA Exemption B3 (relating to statutory prohibitions).
As background, Mogford includes information on “two cases of anaphylactoid reactions in individuals with a strong past history of allergic reactions….” Marks replies to Mogford: “It would be very helpful if our Office of Vaccines could receive additional details [redacted] from MHRA [UK Medicines and Healthcare Products Regulatory Agency] under the terms of our mutual confidentiality agreement.” Mogford later replies, “… attached are [redacted] hope that’s helpful in the meantime. If I can just remind – information shared under our confidentiality agreement.”
Marion Gruber, head of the Office of Vaccines Research and Review (OVRR), then replies to Mogford, “Thank you so much for this information. Our emails crossed. If possible, would be available for a t-con [teleconference] today?” The exchange concludes with OVRR Deputy Director Phil Krause advising UK Medicines and Healthcare Products Regulatory Agency official Jamie Convisser, “Your summary is correct. I’m cc:ing Amanda Cohn at CDC who can provide the most up-to-date details about [redacted]. Obviously, [redacted], not all of this is public so please hold these details confidential.” Cohn then replies to Mogford, and includes an attachment titled “Anaphylaxis CLARK Dec 19 2020 Final”. She writes, “I am adding my colleagues Tom Clark and Stacey Martin, we are happy to share more information with you. Attached are slides that were presented at a public meeting on Saturday. [Redacted].”
The FDA issued its Emergency Use Authorization for the Pfizer-BioNTech COVID vaccine for individuals 16 years of age and older on December 11, 2020.
On May 14, 2021, the CDC’s Dr. Amanda Cohn emailed Office of Vaccines Research and Review Director Marion Gruber and Center for Biologics Evaluation and Research Director Peter Marks with the subject line “Coadministration of COVID-19 Vaccines with Other Vaccines During Pregnancy.”
Gruber writes, “I am fine with this language.” Marks then responds to Cohn and her CDC colleague, Sarah Mbaeyi, “I can live with this too. Please let me know if you want to connect about the adverse event issue later today. Seems like work is still ongoing, but let me know. Thanks.” Cohn replies, “We have a meeting with Rochelle [presumably CDC Director Rochelle Walensky] at 3:30 about if we should say anything or wait until we have more definitive information. I will let you know where we land. I’m not sure there is a right answer.”
“It again took a lawsuit for the Biden administration to hand over, albeit heavily redacted, information regarding the safety of the COVID vaccines that the public has every right to know,” said Judicial Watch President Tom Fitton. “This disturbing batch of new documents have uncovered a secret confidentiality agreement tied to COVID vaccine safety issues and emails that raise new questions about the vaccines and pregnancy.”
Judicial Watch is pursuing challenges against the agency’s redactions under FOIA.
In a previous production from this FOIA lawsuit, Judicial Watch received 1,081 pages of records from HHS detailing internal discussions about myocarditis and the COVID vaccine. Other documents detailed adverse “events for which a contributory effect of the vaccine could not be excluded.”
Through FOIA, Judicial Watch has uncovered a substantial amount of information about COVID-19 issues:
- HHS records regarding data Moderna submitted to the FDA on its mRNA COVID-19 vaccine, indicated a “statistically significant” number of rats were born with skeletal deformations after their mothers were injected with the vaccine. The documents also reveal Moderna elected not to conduct a number of standard pharmacological studies on the laboratory test animals.
- FDA records detailed pressure for COVID-19 vaccine booster approval and use.
- NIH records revealed an FBI “inquiry” into the NIH’s controversial bat coronavirus grant tied to the Wuhan Institute of Virology. The records also show National Institute of Allergy and Infectious Diseases (NIAID) officials were concerned about “gain-of-function” research in China’s Wuhan Institute of Virology in 2016. The Fauci agency was also concerned about EcoHealth Alliance’s lack of compliance with reporting rules and use of gain-of-function research in the NIH-funded research involving bat coronaviruses in Wuhan, China.
- HHS records revealed that from 2014 to 2019, $826,277 was given to the Wuhan Institute of Virology for bat coronavirus research by the NIAID.
- NIAID records showed that it gave nine China-related grants to EcoHealth Alliance to research coronavirus emergence in bats and was the NIH’s top issuer of grants to the Wuhan lab itself. The records also included an email from the vice director of the Wuhan Lab asking an NIH official for help finding disinfectants for decontamination of airtight suits and indoor surfaces.
- HHS records included an “urgent for Dr. Fauci ” email chain, citing ties between the Wuhan lab and the taxpayer-funded EcoHealth Alliance. The government emails also reported that the foundation of U.S. billionaire Bill Gates worked closely with the Chinese government to pave the way for Chinese-produced medications to be sold outside China and help “raise China’s voice of governance by placing representatives from China on important international counsels as high level commitment from China.”
- HHS records included a grant application for research involving the coronavirus that appears to describe “gain-of-function” research involving RNA extractions from bats, experiments on viruses, attempts to develop a chimeric virus and efforts to genetically manipulate the full-length bat SARSr-CoV WIV1 strain molecular clone.
- HHS records showed the State Department and NIAID knew immediately in January 2020 that China was withholding COVID data, which was hindering risk assessment and response by public health officials.
- University of Texas Medical Branch (UTMB) records showed the former director of the Galveston National Laboratory at the University of Texas Medical Branch (UTMB), Dr. James W. Le Duc warned Chinese researchers at the Wuhan Institute of Virology of potential investigations into the COVID issue by Congress.
- HHS records regarding biodistribution studies and related data for the COVID-19 vaccines showed a key component of the vaccines developed by Pfizer/BioNTech, lipid nanoparticles (LNPs), were found outside the injection site, mainly the liver, adrenal glands, spleen and ovaries of test animals, eight to 48 hours after injection.
- Records from the Federal Select Agent Program (FSAP) revealed safety lapses and violations at U.S. biosafety laboratories that conduct research on dangerous agents and toxins.
- HHS records included emails between National Institutes of Health (NIH) then-Director Francis Collins and Anthony Fauci, the director of National Institute of Allergy and Infectious Diseases (NIAID), about hydroxychloroquine and COVID-19.
- HHS records showed that NIH officials tailored confidentiality forms to China’s terms and that the World Health Organization (WHO) conducted an unreleased, “strictly confidential” COVID-19 epidemiological analysis in January 2020.
- Fauci emails included his approval of a press release supportive of China’s response to the 2019 novel coronavirus.

Judicial Watch: Records Show U.S. and UK ‘Confidentiality Agreement’ Tied to Vaccine Adverse Events - Judicial Watch
(Washington, DC) – Judicial Watch announced today it received 57 pages of heavily redacted records from the U.S. Department of Health and Human Services (HHS) that show, just two days prior to FDA approval of the Pfizer-BioNTech COVID-19 vaccine, a discussion between U.S. and UK health...
www.judicialwatch.org
Heliobas Disciple
TB Fanatic
Geert has a new article today - it's a reprint of an article he did from Aug 2015 about the Ebola vaccine. I don't know why he posted it now, I'm guessing because of the news of Marburg in W Africa. Or maybe for another reason???? 
Anyway - here's the link. Since it's off topic (not directly covid related (I don't think...)) I won't paste the article, but it's from Geert and could be he's hinting at something so posting the link for anyone interested:
 www.voiceforscienceandsolidarity.org
www.voiceforscienceandsolidarity.org
Anyway - here's the link. Since it's off topic (not directly covid related (I don't think...)) I won't paste the article, but it's from Geert and could be he's hinting at something so posting the link for anyone interested:
Guinea – The Ebola vaccine trial and the reported interim results | Voice for Science and Solidarity
In response to the challenging circumstances, and desires to fast-track Ebola vaccine research, investigators studying rVSV-ZEBOV did not us
www.voiceforscienceandsolidarity.org
Heliobas Disciple
TB Fanatic
Far-Reaching Implications: Scientists Shed Light on the “Original Antigenic Sin”
According to the theory of original antigenic sin (OAS), our immune systems react most strongly to the viral strains we encountered in our childhoods. This first encounter with a virus such as influenza or COVID-19 is referred to as the "original sin" that influences our immune response to newer str
scitechdaily.com
Far-Reaching Implications: Scientists Shed Light on the “Original Antigenic Sin”
By The Rockefeller UniversityFebruary 13, 2023
According to the theory of original antigenic sin (OAS), our immune systems react most strongly to the viral strains we encountered in our childhoods. This first encounter with a virus such as influenza or COVID-19 is referred to as the “original sin” that influences our immune response to newer strains. As a result, even after receiving flu vaccines or COVID boosters, our bodies may still produce outdated antibodies against an outdated strain of the virus. Instead, the OAS theory suggests that our immune system has a persistent bias toward the first strain of a virus it encountered.
A recent study published in Nature sheds new light on the otherwise hazy phenomenon, providing some of the clearest evidence to date of when OAS occurs and how it functions in a laboratory setting. These findings could have significant implications for the creation of effective vaccines against influenza and COVID-19.
“Our goal was to understand the basic principles that underlie OAS so that researchers making these vaccines can keep the potential effects in mind,” says Rockefeller’s Gabriel D. Victora. “With a novel technique, we lay out the basics of how OAS should be looked at from an experimental perspective and answer a question we believe to be key to vaccine development.”
Antigenic Sin
OAS was initially described in the 1950s by Thomas Francis Jr., a legendary virologist who isolated the first human influenza strain in the U.S. The son of a Presbyterian minister, Francis chose decidedly religious terminology to capture his frustration with the immune system’s tendency to imprint on the first antigen it encounters, even to its own detriment. “Francis realized that you could figure out someone’s age by looking at their antibodies against flu,” Victora says. “People’s strongest antibodies were usually to the strains circulating when they were young.”“Love it or hate it, the term has stuck and become a staple in conversations about viral vaccination.”
If OAS were strictly true, it would be difficult for a vaccine program to overcome the body’s resistance to change. Upon exposure to a new flu strain via seasonal vaccines, the body would just repeatedly reuse its original cohort of B cells and suppress the formation of new ones. “According to the OAS idea, your body wouldn’t be able to develop new immune responses to evolving variants of a virus, because it would be addicted to the first strain you encountered,” Victora says.
Despite half a century of epidemiological evidence of this frustrating phenomenon, however, the precise extent of OAS proved difficult to measure in a laboratory setting. “It was not easy to generate good experimental data on OAS,” Victora says. “Prior experiments have given discrepant results—sometimes researchers see it, and sometimes they don’t.”
In an attempt to better understand OAS and its impacts on seasonal vaccines and booster shots, Victora and colleagues developed molecular fate-mapping, a technique which allowed the team to clearly distinguish old antibodies from new ones in serum. They then exposed mice to one immunization after another, while tracking the progress of every last antibody. The findings confirmed, experimentally, that, when the antigen was kept the same, the mice were “addicted” to the first B cells they produced, and that these B cells were preventing the formation of new B cells to respond to novel threats.
“We estimate that the mice would have made 55-fold more new antibodies were their old antibodies not around to suppress the formation of new ones,” Victora says.
Antigenic Redemption
On the surface, these findings would appear to imply that seasonal shots and boosters are exercises in futility. The body is doomed to produce B cells attuned to everyone’s first COVID or flu exposure, ignoring and even suppressing inoculations against new strains.“But there’s a twist,” Victora says. If the booster shot contains an antigen sufficiently different from the original antigen, OAS steps into the sidelines. Indeed, Victora and colleagues demonstrate in mice infected with a variety of influenza virus and SARS-CoV-2 strains that once two antigens are even a few amino acids apart, that 55-fold deficit falls to a manageable three-fold.
“This work provides a basic understanding of the way B cells respond to a series of booster vaccines and underscores the ingenuity and adaptability of the immune system,” says first author Ariën Schiepers, a graduate student in Victora’s lab and the first author on the paper. “When boosting with a variant antigen, we begin to see new, variant-specific antibodies that enable the subversion of OAS.”
Although the findings are confined to mice, Victora suspects the message may be universal. Should the trend hold in humans, the team’s findings would imply that boosting against a new strain of SARS-CoV-2 will bear the most fruit if the new strain is sufficiently different from the one covered by the previous vaccine (which, by the way, is clearly the case for the case bivalent COVID vaccines currently in clinical use). “It may well be a matter of waiting to update vaccines until the virus is sufficiently divergent. That would be just the right time to develop a booster.”
Reference: “Molecular fate-mapping of serum antibody responses to repeat immunization” by Ariën Schiepers, Marije F. L. van ’t Wout, Allison J. Greaney, Trinity Zang, Hiromi Muramatsu, Paulo J. C. Lin, Ying K. Tam, Luka Mesin, Tyler N. Starr, Paul D. Bieniasz, Norbert Pardi, Jesse D. Bloom and Gabriel D. Victora, 16 January 2023, Nature.
DOI: 10.1038/s41586-023-05715-3