
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
CORONA Main Coronavirus thread
- Thread starter Heliobas Disciple
- Start date
-
- Tags
- coronavirus
Profit of Doom
Dismember
Cesium 137. Ok. So it’s radioactive. Is that supposed to power our nano bot supercomputer? The craycray Cray. Think somebody’s cheese has departed the cracker. I mean, attach a transistor to a cell, and that is supposed to control us?
vector7
Dot Collector
View: https://twitter.com/brixwe/status/1602395791963848747?s=20&t=M341oDl6DJ8Q45RnJd7wnA
Dr. Kirk Milhoan on myocarditis in children, teens and young adults. He got his BA from PLNU, PHD from UCSD, MD from Jefferson College in Philadelphia. Pediatric Cardiologist Fellowship at San Diego Children's Hospital.
RT 1:29secs
View: https://twitter.com/StellaEscoTV/status/1600601754415947776?s=20&t=AkZykn3Ti0pTnS4izE4T1w
Jim Jordan on gain of function research hearings
RT 7min
View: https://twitter.com/Jim_Jordan/status/1603035700479537157?s=20&t=jk04qAgXw1t70Ijr_rWfiA
Dr. Kirk Milhoan on myocarditis in children, teens and young adults. He got his BA from PLNU, PHD from UCSD, MD from Jefferson College in Philadelphia. Pediatric Cardiologist Fellowship at San Diego Children's Hospital.
RT 1:29secs
View: https://twitter.com/StellaEscoTV/status/1600601754415947776?s=20&t=AkZykn3Ti0pTnS4izE4T1w
Jim Jordan on gain of function research hearings
RT 7min
View: https://twitter.com/Jim_Jordan/status/1603035700479537157?s=20&t=jk04qAgXw1t70Ijr_rWfiA
Profit of Doom
Dismember
If you read the Twitter comments, note that Jack Spratt just joined in June. He needs a candlestick transplant.View: https://twitter.com/brixwe/status/1602395791963848747?s=20&t=M341oDl6DJ8Q45RnJd7wnA
Dr. Kirk Milhoan on myocarditis in children, teens and young adults. He got his BA from PLNU, PHD from UCSD, MD from Jefferson College in Philadelphia. Pediatric Cardiologist Fellowship at San Diego Children's Hospital.
RT 1:29secs
View: https://twitter.com/StellaEscoTV/status/1600601754415947776?s=20&t=AkZykn3Ti0pTnS4izE4T1w
Jim Jordan on gain of function research hearings
RT 7min
View: https://twitter.com/Jim_Jordan/status/1603035700479537157?s=20&t=jk04qAgXw1t70Ijr_rWfiA
Profit of Doom
Dismember
According to WaPo, Grant Wahl died at the World Cup from an aortic aneurism, said his wife. That’s a listed AE, isn’t it?
vector7
Dot Collector
Profit of Doom
Dismember
One of those girls could preach climate change. As I recall, Africa used HCQ/IVM and had drastically lower deaths. Other countries too.
northern watch
TB Fanatic

naegling62
Veteran Member
So my wife just got back from her hair appointment and the lady that owns the salon is very reliable. She said it is remarkable how many customers or family members of customers that are having strokes. She confirmed these are vaccinated individuals.
northern watch
TB Fanatic

Heliobas Disciple
TB Fanatic
THIS IS A REAL ARTICLE CITING A REAL STUDY -THIS IS NOT FROM THE ONION OR ANY OTHER SATIRE SITE!

People who skipped their COVID vaccine are at higher risk of traffic accidents, according to a new study
The findings could justify changes to driver insurance policies, the authors say.fortune.com
People who skipped their COVID vaccine are at higher risk of traffic accidents, according to a new study
Erin Prater
December 13, 2022, 1:31 PM EST
If you passed on getting the COVID vaccine, you might be a lot more likely to get into a car crash.
Or at least those are the findings of a new study published this month in The American Journal of Medicine. During the summer of 2021, Canadian researchers examined the encrypted government-held records of more than 11 million adults, 16% of whom hadn’t received the COVID vaccine.
They found that the unvaccinated people were 72% more likely to be involved in a severe traffic crash—in which at least one person was transported to the hospital—than those who were vaccinated. That’s similar to the increased risk of car crashes for people with sleep apnea, though only about half that of people who abuse alcohol, researchers found.
The excess risk of car crash posed by unvaccinated drivers “exceeds the safety gains from modern automobile engineering advances and also imposes risks on other road users,” the authors wrote.
Of course, skipping a COVID vaccine does not mean that someone will get into a car crash. Instead, the authors theorize that people who resist public health recommendations might also “neglect basic road safety guidelines.”
Why would they ignore the rules of the road? Distrust of the government, a belief in freedom, misconceptions of daily risks, “faith in natural protection,” “antipathy toward regulation,” poverty, misinformation, a lack of resources, and personal beliefs are potential reasons proposed by the authors.
The findings are significant enough that primary care doctors should consider counseling unvaccinated patients on traffic safety—and insurance companies might base changes to insurance policies on vaccination data, the authors suggest.
First responders may also consider taking precautions to protect themselves from COVID when responding to traffic crashes, the authors added, as it’s more likely that a driver is unvaccinated than vaccinated.
“The findings suggest that unvaccinated adults need to be careful indoors with other people and outside with surrounding traffic,” the authors concluded.
This isn’t the first time that researchers have examined the link between behavior and vaccination status. Among young adults, a 2021 study published in the Journal of Bioeconomics found a correlation between self-reported risky driving and having skipped their flu vaccine. It examined the survey responses of more than 100,000 Canadians.
Others are picking up this (idiotic) story. This from the Conservative Treehouse. Gateway Pundit also picked it up,

Canadian Research Group Finds Unvaccinated People More Likely to Have Severe Car Accidents - Paving Way for Insurance Rate Hikes for Unvaccinated - The Last Refuge
The logic within the research outline is silly. Unvaccinated people have a 72% higher rate of severe vehicle accidents than vaccinated drivers according to the study. Could it be the difference between rural vs metropolitan populations; one drives frequently, for longer durations and distances...
Canadian Research Group Finds Unvaccinated People More Likely to Have Severe Car Accidents – Paving Way for Insurance Rate Hikes for Unvaccinated
sundance
December 14, 2022
The logic within the research outline is silly. Unvaccinated people have a 72% higher rate of severe vehicle accidents than vaccinated drivers according to the study.
Could it be the difference between rural vs metropolitan populations; one drives frequently, for longer durations and distances, while the other does not?
Apparently, that type of commonsense possibility did not make it into the analysis. However, the authors of the study do suggest insurance companies should start considering insurance risk hikes based on vaccination status.
(Via Yahoo) – If you passed on getting the COVID vaccine, you might be a lot more likely to get into a car crash.
Or at least those are the findings of a new study published this month in The American Journal of Medicine. During the summer of 2021, Canadian researchers examined the encrypted government-held records of more than 11 million adults, 16% of whom hadn’t received the COVID vaccine.
They found that the unvaccinated people were 72% more likely to be involved in a severe traffic crash—in which at least one person was transported to the hospital—than those who were vaccinated. That’s similar to the increased risk of car crashes for people with sleep apnea, though only about half that of people who abuse alcohol, researchers found.
The excess risk of car crash posed by unvaccinated drivers “exceeds the safety gains from modern automobile engineering advances and also imposes risks on other road users,” the authors wrote.
Of course, skipping a COVID vaccine does not mean that someone will get into a car crash. Instead, the authors theorize that people who resist public health recommendations might also “neglect basic road safety guidelines.”
Why would they ignore the rules of the road? Distrust of the government, a belief in freedom, misconceptions of daily risks, “faith in natural protection,” “antipathy toward regulation,” poverty, misinformation, a lack of resources, and personal beliefs are potential reasons proposed by the authors.
The findings are significant enough that primary care doctors should consider counseling unvaccinated patients on traffic safety—and insurance companies might base changes to insurance policies on vaccination data, the authors suggest. (read more)
It’s a Canadian study, so start there.
Heliobas Disciple
TB Fanatic
BREAKING! COVID-19 News: Finally, U.S. NIH Warns SARS-CoV-2 Viral Persistence Is A Serious Issue That Is Also Affecting Long COVID! - Thailand Medical News
COVID-19 News: After yet another autopsy study, this time involving 44 patients who died from COVID-19 and Long COVID, the study team from the U.S. NIH and U.S. NIAID who found active SARS-CoV-2 RNA is various anatomic sites including the brain and various organs, have issued a warning that...
 www.thailandmedical.news
www.thailandmedical.news
COVID-19 News: Finally, U.S. NIH Warns SARS-CoV-2 Viral Persistence Is A Serious Issue That Is Also Affecting Long COVID
Thailand Medical News
Dec 14 2022
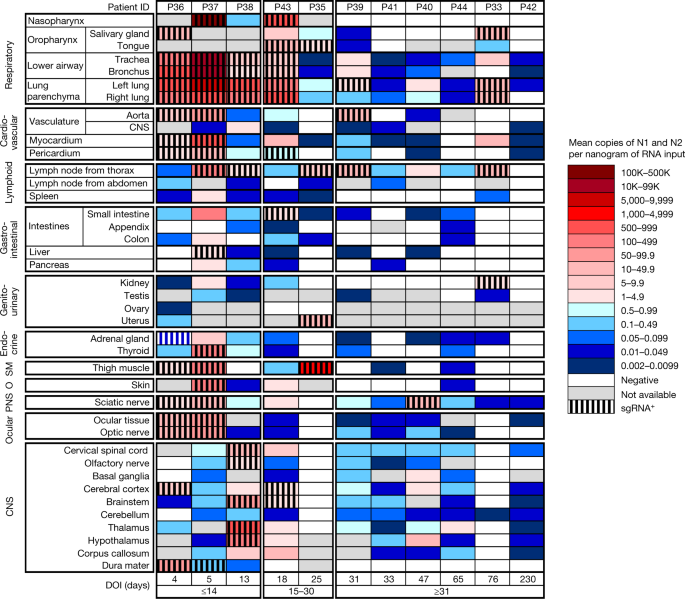
After yet another autopsy study, this time involving 44 patients who died from COVID-19 and Long COVID, the study team from the U.S. NIH and U.S. NIAID who found active SARS-CoV-2 RNA is various anatomic sites including the brain and various organs, have issued a warning that SARS-CoV-2 is more serious than thought and urgent research is needed to develop treatment protocols to address the issue.
The study findings were worrisome as in many cases, viral persistence was found months after initial symptom onset of COVID-19 or initial detection via standard test. Many do not display signs of inflammation caused by the virus presence and even other symptoms till severe damage materializes.
In one case, the study team detected active SARS-CoV-2 RNA in the brain of a patient 230 days following symptom onset.
The researchers found active replicative SARS-CoV-2 virus in cardiovascular, lymphoid, gastrointestinal, renal, endocrine, reproductive, muscle, brain and other tissue although none of these areas sustained significant inflammation compared to what they found in the respiratory tract!
According to the study team, COVID-19 is known to cause multi-organ dysfunction during acute infection with SARS-CoV-2, with some patients experiencing prolonged symptoms, termed post-acute sequelae of SARS-CoV-2.
However, the burden of infection outside the respiratory tract and time to viral clearance are not well characterized, particularly in the brain.
The study team carried out complete autopsies on 44 patients who died with COVID-19, with extensive sampling of the central nervous system in 11 of these patients, to map and quantify the distribution, replication and cell-type specificity of SARS-CoV-2 across the human body, including the brain, from acute infection to more than seven months following symptom onset.
Alarmingly, the study findings showed that SARS-CoV-2 is widely distributed, predominantly among patients who died with severe COVID-19, and that virus replication is present in multiple respiratory and non-respiratory tissues, including the brain, early in infection.
Shockingly, the study team detected persistent SARS-CoV-2 RNA in multiple anatomic sites, including throughout the brain, as late as 230 days following symptom onset in one case.
Worryingly, despite extensive distribution of SARS-CoV-2 RNA throughout the body, the study team observed little evidence of inflammation or direct viral cytopathology outside the respiratory tract.
The study findings indicate that in some patients SARS-CoV-2 can cause systemic infection and persist in the body for months.
The study findings were published in the peer reviewed journal: Nature.
SARS-CoV-2 infection and persistence in the human body and brain at autopsy - Nature
A study reports the distribution, replication and persistence of SARS-CoV-2 throughout the human body including in the brain at autopsy from acute infection to more than seven months following symptom onset.
 www.nature.com
www.nature.com
The study findings has serious implications as to how the COVID-19 pandemic has been wrongly managed in the last three years...starting with stupid diagnostics and protocols to determine that a person has "rec overed' from COVID-19 using only nasal or saliva tests and also the lack of any effective antivirals that can really help with total virus clearance in the human host.
Thailand Medical News had already been warning about SARS-CoV-2 viral persistence in our various COVID-19 News coverages since mid-2020 and that current approach to diagnostics and determining who has recovered form COVID-19 and also treatment protocols are all wrong as we are not completely clearing the virus out of the body.
COVID News: New York Scientists Find SARS-CoV-2 Viral Presence In The Lung Up To 359 Days After Acute Phase Of Disease Even In The Negative Tested! - Thailand Medical News
COVID News: A new study conducted by researchers from Weill Cornell Medicine, New York - USA has found SARS-CoV-2 viral presence in the lung up to 359 days after acute phase of disease, even in patients with negative nasopharyngeal swab tests! The study findings validate that SARS-CoV-2...
www.thailandmedical.news

World COVID-19 News: Global Deaths Crosses 1.6 Million Milestone, Infections Pass 71.8 Million. Why Are Authorities Downplaying Viral Persistence? - Thailand Medical News
World COVID-19 News: The COVID-19 crisis is escalating exponentially with the total COVID-19 deaths now crossing the 1.6 million milestone and reaching more than 1,607,900 as of Sunday (1700hrs Bangkok). The total number of global COVID-19 infections has now reached more than 71.8 million...
www.thailandmedical.news

BREAKING! U.S. NIH Study Shockingly Reveals SARS-CoV-2 Viral Persistence Throughout Human Body And In The Brain Even In Those Who Were Asymptomatic! - Thailand Medical News
SARS-CoV-2 Viral Persistence: A new study by scientists from the U.S. National Institute of Health (NIH) has found alarming evidence of SARS-CoV-2 viral persistence in the human host body and also in the brain even in those individuals that only had mild symptoms initially during infection and...
www.thailandmedical.news
BREAKING! SARS-CoV-2 Persists In Intestinal Enterocytes Up To 7 Months After Symptom Resolution. Viral Persistence Is Real And A Serious Issue! - Thailand Medical News
SARS-CoV-2 Viral Persistence: A study by researchers from Icahn School of Medicine at Mount Sinai -New York lead by Dr Minami Tokuyama has alarmingly found that the SARS-CoV-2 coronavirus persist in intestinal enterocytes up to 7 months after symptom resolution. The study which is still ongoing...
www.thailandmedical.news

BREAKING! Latest U.S. NIH Study Reveals Viral Persistence Is A Major Issue And That SARS-CoV-2 Replicates In Tissues For Months In Post-COVID Individuals! - Thailand Medical News
A new study by researchers from the NIH COVID-19 Autopsy Consortium has shocking revealed that SARS-CoV-2 viral persistence is a major issue and that the SARS-CoV-2 virus continues to still replicate in tissues of Post-COVID individuals for months! The study was led by Dr Daniel Chertow, a...
www.thailandmedical.news
COVID-19 News: Yale Study Shockingly Finds That PBMC Myeloid Cells Harbors SARS-CoV-2 Genomes With Implications For Viral Persistence And Misc Dangers! - Thailand Medical News
COVID-19 News: Scientists from Yale Medical School have made yet another alarming discovery that the human host’s blood mononuclear cells (PBMC) are able to harbor the SARS-CoV-2 genome with implications for viral persistence and dangers to various human organs over time. Various different...
www.thailandmedical.news
Viral Persistence: Georgia State University Study Indicates That SARS-CoV-2 May Hide In The Brain And Cause Relapses In ‘Recovered’ Patients! - Thailand Medical News
Viral Persistence: A new research by scientists from the Georgia State University involving animal models has demonstrated that mice being infected with the SARS-Cov-2 coronavirus through their nasal passages developed severe illness due to brain infection even after the virus had left their...
www.thailandmedical.news
COVID-19 Research: University of California Led Study Finds That Brain Pericytes Could Be Entry Points For SARS-CoV-2 And Are Potential Reservoirs - Thailand Medical News
COVID-19 Research: A news research led by scientist from University of California-San Diego along with researchers from Rady Children’s Hospital-San Diego, Rutgers State University-New Jersey and University of Wisconsin-Madison have found that the SARS-CoV-2 coronavirus is able to infect the...
www.thailandmedical.news

New COVID-19 Diagnostics Urgently Needed As The Current Nasal or Saliva Swabs Tests Are Unable To Detect Viral Persistence Let Alone New Variants! - Thailand Medical News
It is amazing and shocking as to how the global medical community has been addressing a global pandemic that has been plaguing the world for the last 31 months with a new pathogen outbreak that involves a novel virus that we still know little about and worse is constantly evolving and changing...
www.thailandmedical.news

Study In China Reveals Persistent Fecal Virus Shedding In Children Deemed ‘Recovered’ From COVID-19 After Testing Negative Via Nasal Swab Tests! - Thailand Medical News
While the Western world especially countries like the United States and the United Kingdom are trying to downplay issues about viral persistence in those that are deemed as ‘recovered’ from the COVID-19 disease , in other countries medical experts are focusing more studies on this issue. In the...
www.thailandmedical.news

Children’s Hospital Los Angeles Led Study Alarmingly Shows SARS-CoV-2 Causing Viral Persistence In Children And Young Adults With Cancer! - Thailand Medical News
A new study led by researchers from the Children’s Hospital Los Angeles along with scientists from New York Medical College, University of Southern California, Stanford University School of Medicine and Johns Hopkins Bloomberg School of Public Health has found alarmingly found that the new...
www.thailandmedical.news
COVID-19 News: WARNING! Millions Of Recovered COVID-19 Patients Could Be Walking Around With Residual Reservoirs Of The SARS-CoV-2 Virus In Them! - Thailand Medical News
COVID-19 News: The COVID-19 pandemic can be best described as one of the worst managed pandemics in history and without proper leadership. The WHO or World Health Organization has been so incompetent in the handling of the SARS-CoV-2 breakout in China and they literally helped the spread of the...
www.thailandmedical.news
BREAKING! Many Long COVID-19 Patients Have Higher Levels Of Circulating SARS-CoV-2 Viral RNA Compared To Those With Acute Infection! - Thailand Medical News
Long COVID-19 Research: A new study by researchers from the Division of Pulmonary and Critical Care Medicine at University of Kansas-USA has revealed that many Long COVID-19 patients have higher levels of circulating SARS-CoV-2 Viral RNA compared to individuals with acute COVID-19 infection...
www.thailandmedical.news
Yet Another Alarming Research Finding! Persistence of SARS CoV-2 S1 Protein Found in CD16+ Monocytes Of Post COVID-19 Patients Up To 15 Months After So-Called Recovery! - Thailand Medical News
SARS-CoV-2 Research: A new research by scientist from California, Massachusetts, New York, Orlando and also Costa Rican researchers have discovered that in patients having being deemed as recovered from COVID-19 but are still suffering from Long COVID conditions, it was found that even 15 months...
www.thailandmedical.news

NICE! Neurologists Find Replicable SARS-CoV-2 RNA In Cerebrospinal Fluid Of A Woman 114 Days After She Was Diagnosed With Asymptomatic COVID-19! - Thailand Medical News
SARS-CoV-2 Viral Persistence: The COVID-19 pandemic is the best thing that has happened to mankind so far as it shows how incompetent most medical researchers and physicians are and worst, those ignorant bureaucratic developing medical and treatment guidelines from diagnostics, treatments...
www.thailandmedical.news

BREAKING! Study Shows That COVID-19 Can Cause Intestinal Ischemia And Gastrointestinal Issues In Asymptomatic Individuals Who Continue To Test Negative! - Thailand Medical News
Contrary to the fallacy that most idiots and ignorant experts claim that those who were COVID-19 asymptomatic have nothing to worry about, in reality the fact that the virus is able to disrupt the host immune systen such that no symptoms appear while the virus is still persistent in some deeper...
www.thailandmedical.news

BREAKING! Brazilian And American Study Discovers That The Testes Of Males Could Be Viral Sanctuaries For The SARS-CoV-2 Virus! - Thailand Medical News
Alarming findings from a new study by researchers from Universidade Federal de Minas Gerais-Brazil, University of Texas Medical Branch-USA, University of Pittsburgh School of Medicine-USA, Faculdade de Medicina de São Jose do Rio Preto-Brazil, Universidade Estadual Paulista-Brazil and Clínica...
www.thailandmedical.news
BREAKING! Corpse Test Positive For SARS-CoV-2 Virus For 28 Times Six Weeks After Death Indicating Long Term Viral Persistence! - Thailand Medical News
SARS-CoV-2 Viral Persistence: Italian researchers from the University of Chieti-Pescara “G. d’Annunzio” have in a new case study reported of a corpse of a of a Ukrainian man who died from drowning in Italy testing positive for COVID-19 as many as 28 times in the six weeks after his death...
www.thailandmedical.news
BREAKING! Long COVID Is A Misnomer! The Conditions Are Being Caused By Viral Persistence And Viral Peptides Similar To Retrotransposons And Introns! - Thailand Medical News
We have been having lots of so-called experts…each claiming to have discovered the factors that is causing that Long COVID. Some say it is a condition caused by vasculitis triggered by the SARS-CoV-2, or it is because of the thrombotic state the body gain due to the effects of the virus while...
www.thailandmedical.news
BREAKING! Researchers Present Case Reports Of Long COVID Patients With Persistence Of Residual SARS-CoV-2 Antigen And RNA In Various Tissues! - Thailand Medical News
COVID-19 News: Researchers from the Institute of Molecular and Cell Biology (IMCB) at the Agency for Science, Technology and Research (ASTAR) - Singapore, Long Covid Autonomous Comm unities Together Spain (Research Group) Madrid -Spain, Vetcare Hospital Veterinario Madrid -Spain, Singapore...
www.thailandmedical.news
The latest study findings from the U.S. NIH and U.S. NIAD shows that the disease-causing SARS-CoV-2 virus is able to spread throughout the body ie beyond just being a respiratory disease and can remain in various tissues and organs for months.
The study findings hopefully help other researchers and scientists broaden their perspectives on where SARS-CoV-2 could cause infection and persist, including the brain.
Research findings from the autopsies, which took place between April 2020 and March 2021, confirmed that SARS-CoV-2 primarily infected and damaged the airway and lungs.
Alarmingly, scientists also found virus fragments (viral RNA) in 79 of 85 body locations, with some virus found up to 230 days after patient’s symptoms began.
The study team worryingly and found active SARS-CoV-2 virus in cardiovascular, lymphoid, gastrointestinal, renal, endocrine, reproductive, muscle, brain and other tissues and cell types although none of these areas sustained significant inflammation compared to what they found in the respiratory tract!
The study team comprising of scientists from NIH’s National Institute of Allergy and Infectious Diseases and Clinical Center led the work, closely collaborating with National Cancer Institute (NCI) pathologists, four other NIH institutes, the University of Maryland, and Maryland health care facilities in Salisbury and Towson.
Senior author, Dr Daniel Chertow from the Emerging Pathogens Section, Critical Care Medicine Department, Clinical Center, National Institutes of Health, Bethesda-USA told Thailand Medical News, “Our study findings show that the SARS-CoV-2 virus disseminates across the human body and brain early in infection at high levels and provide evidence of virus replication at multiple extrapulmonary sites during the first two weeks following symptom onset.”
He further added, “Worryingly, the SARS-CoV-2 virus can spread throughout the body and viral RNA may remain detectable for months even in cases with mild or no symptoms.”
He said, “The original thinking in the field was that SARS-CoV-2 was predominantly a respiratory virus. However, finding the viral fragments in tissue throughout the body and sharing those findings with colleagues a year ago, helped scientists explore a relationship between the viral fragments and Long COVID.”
The condition …Long COVID gets its name from the persistent symptoms some individuals experience after having COVID-19; symptoms can be debilitating, and the cause is not known.
Although the study team did not specifically explore Long COVID, finding the viral RNA throughout the body raised speculation that those fragments might contribute to the persistent symptoms.
Finding proper efficient antivirals that can truly eradicate SARS-CoV-2 reservoirs in the human body and also developing proper diagnostics to check for viral persistence is urgently warranted.
The current method of using nasal or saliva swabs to test and determine whether a person has recovered from COVID-19 is totally ridiculous and is laughable that this has been the standards in the last three years!
Thailand Medical News strongly believes that SARS-CoV-2 viral persistence is a contributing factor to Long COVID along with viral peptides persistence in the human host even after virus clearance along with the damages done to the various cellular pathways, genes, organs and tissues.
BREAKING! Long COVID Is A Misnomer! The Conditions Are Being Caused By Viral Persistence And Viral Peptides Similar To Retrotransposons And Introns! - Thailand Medical News
We have been having lots of so-called experts…each claiming to have discovered the factors that is causing that Long COVID. Some say it is a condition caused by vasculitis triggered by the SARS-CoV-2, or it is because of the thrombotic state the body gain due to the effects of the virus while...
www.thailandmedical.news
SARS-CoV-2 viral persistence will also contribute to excess deaths and will affect the health of many, some who are not even aware that they had been exposed to the SARS-CoV-2 virus!
Many will eventually succumb to various types of fatal outcomes ranging from heart failures, strokes organ failures sepsis etc.
Thailand Medical News also keeps on warning that many exposed to the SARS-CoV-2 virus will only have 5 to 8 years left while actually many might not even make it till then. Constant breakthrough infections and reinfections will even contribute to many having their lifespans even shortened.

BREAKING! Hypothesis That Majority Exposed To SARS-CoV-2 Will Have Shortened Lifespans Validated By Study Showing NSP2 Impairs Human 4EHP-GIGYF2 Complex! - Thailand Medical News
Since late March 2022, Thailand Medical News has been proposing our hypothesis that majority of individuals who have been exposed to the SARS-CoV-2 virus, irrespective of the initial conditions upon infection ie asymptomatic or mild to severely symptomatic, will have their lifespans reduced...
www.thailandmedical.news

Most Who Have Been Exposed To The Proteins Of The SARS-CoV-2 Virus Will Have Shortened Lifespans! Stop Using Fluvoxamine For BA.2 Infections! - Thailand Medical News
No this is not some April Day prank nor it is some fear porn to get everyone anxious, rather this is stark warning that everyone who has been exposed to the proteins of the SARS-CoV-2 virus through whichever means need to take it upon themselves to do frequent medical checkups and also to take...
www.thailandmedical.news
BREAKING! COVID-19 News: SARS-CoV-2 Infections Lead To Cellular m6A RNA Methylation Loss In Host Cells! Possible Implications For Cancer And Other Issues! - Thailand Medical News
COVID-19 News: A new international study has alarmingly found that SARS-CoV-2 infections lead to cellular m6A RNA methylation loss in host cells! The discovery is worrisome as accumulating evidence suggests that m6A RNA methylation modulates gene expression, thereby regulating cellular...
www.thailandmedical.news
Heliobas Disciple
TB Fanatic
Coronavirus Cure Breakthrough – Scientists Have Found a Potential Basis
They discovered that the organic compound can bind to many SARS-CoV-2 proteins. Researchers have discovered that salen can effectively bind a number of proteins of the coronavirus SARS-CoV-2. CoV-2's Scientists utilized molecular docking to reveal that salen binds to the non-structural protein nsp1
scitechdaily.com
Coronavirus Cure Breakthrough – Scientists Have Found a Potential Basis
By Ural Federal University
December 14, 2022
They discovered that the organic compound can bind to many SARS-CoV-2 proteins.
Researchers have discovered that salen can effectively bind a number of proteins of the coronavirus SARS-CoV-2. CoV-2’s Scientists utilized molecular docking to reveal that salen binds to the non-structural protein nsp14, which prevents the virus from being destroyed. The discovery may aid in the development of novel drugs and coronavirus infection treatments. The study’s findings were recently published in the journal Polycyclic Aromatic Compounds.
“Our study focused on a well-known compound, salen. We tried to assess the potential activity of this compound against a series of proteins of the SARS-CoV-2, which cause the COVID-19 disease. We found out that salen can potentially interact with the studied proteins, and the best results were obtained for the non-structural protein nsp14, which protects the virus from destruction,” says Damir Safin, Research Engineer at the Organic Synthesis Laboratory of Ural Federal University.
The term “salen” refers to a tetradentate Schiff base derived from salicylaldehyde and ethylenediamine. Salen and its derivatives are key ligands in a wide range of practical applications. This is an organic substance that has the ability to coordinate certain metals and keep them stable in various oxidation states. Metal complex compounds of salen derivatives are also used as catalysts.
Two “fluid” hydrogen atoms of hydroxyl groups are found in salen. Each of these hydrogen atoms has the ability to move to a nitrogen atom, therefore changing the shape of the molecule. This process is known as tautomerization, and the participants are tautomers or tautomeric forms.
“We’ve explored the potential interaction of various tautomers salen with SARS-CoV-2 proteins to identify the most preferred tautomeric form of the studied molecule in terms of the effectiveness in interaction with proteins. Of course, our research is only the first step towards understanding how salen can be used in the fight against COVID-19, much remains to be explored. However, the results we obtained inspire a certain optimism,” adds Damir Safin.
Reference: “Salen: Insight into the Crystal Structure, Hirshfeld Surface Analysis, Optical Properties, DFT, and Molecular Docking Studies” by Maria G. Babashkina, Elizaveta V. Panova, Larisa E. Alkhimova and Damir A. Safin, 22 July 2022, Polycyclic Aromatic Compounds.
DOI: 10.1080/10406638.2022.2097281
A study was carried out by scientists from the Innovation Center of Chemical and Pharmaceutical Technologies of Ural Federal University, Kurgan State University, and Tyumen State University.
Heliobas Disciple
TB Fanatic

Study finds surprising risks for COVID-19 infection
A new paper in Biology Methods & Protocols investigates risk factors and protections against contracting COVID-19, and also for suffering from severe COVID. Researchers have identified several characteristics—including male sex, lower age, blood group B, and larger household size—that increased...
Study finds surprising risks for COVID-19 infection
by Oxford University Press
December 15, 2022
A new paper in Biology Methods & Protocols investigates risk factors and protections against contracting COVID-19, and also for suffering from severe COVID. Researchers have identified several characteristics—including male sex, lower age, blood group B, and larger household size—that increased the risk of infection and many other characteristics—including mask-wearing and using vitamin D—that decreased it. They also identified the things that increased or decreased the risk of a severe course of COVID-19. Some of these findings are unexpected.
SARS-CoV-2 has infected more than 600 million people worldwide, resulting in 6.57 million confirmed deaths. But information about factors affecting the probability of infection or suffering from a severe course of the disease remains insufficient and often speculative. Preregistered longitudinal studies about the risk factors of infection are surprisingly rare. Many factors such as contact with animals have been suggested only on a theoretical basis or discussed in non-scientific sources.
Recruiting participants using sites like Facebook and Twitter, researchers ran a study on 30,000 internet users in the Czech Republic who shared information about their exposure to 105 risk factors for COVID-19. Study participants indicated which potential risks and protective factors applied to them. These included health and demographic characteristics as well as information about their behaviors, including keeping animals, taking vitamins and supplements, being actively engaged in sports, cold water swimming, frequent singing, marijuana use, tobacco smoking, living alone, walking in nature, and volunteering.
The study found that expectedly, some sociodemographic factors had a moderate effect on the risks of COVID-19. People who lived in larger cities and people with higher levels of education, especially women, had a lower risk of infection. Larger household sizes and the number of children under 20 years of age (in men), were associated with a higher risk of infection. People living on their own had a much lower risk of infection than those who shared a household. Singles also reported a less severe course of COVID-19. Education level and (in women) also household size had the strongest protective effects against a severe or long course of COVID-19.
Many predictable behaviors appeared to protect people against the infection, while three factors—being actively involved in sports, frequent singing, and cold-water swimming—increased the risk of infection. The most substantial protective factor against COVID-19 infection was strict adherence to mask-wearing. The second most substantial protective factor was the consumption of vitamins and supplements. This study found in particular that taking vitamin D provided significant protection against acquiring COVID-19.
Adherence to social distancing and frequent handwashing had only a weak protective effect. This study also indicated that having type B blood increased the risk for COVID-19 infection. Having cats or dogs as pets did not affect the risk of infection and had a mostly insignificant positive effect on the risk of someone experiencing a severe course of the disease.
The study also found that tobacco smoking and marijuana use (in women) provide a relatively strong protective effect against infection. The researchers found that marijuana use and tobacco smoking could also have some protective effects against a severe course of COVID-19. The protective effects of tobacco smoking against infection have been reported in previous studies. However, most studies show adverse effects of smoking on the risk of a severe course of COVID-19.
The most unexpected result of the study was a positive correlation between higher severity of the course of COVID-19 and adherence to wearing masks and respirators, and to a lesser extent, keeping social distance. The investigators speculate this is because people predisposed to a severe course of COVID-19 (those who are overweight, suffer from chronic obstructive pulmonary disease, or have diabetes) tried hard to avoid infection and more strictly adhered to public health recommendations about masks and social distancing. But when they did become infected, they often had a more severe course of the disease due to their underlying health problems.
Heliobas Disciple
TB Fanatic
THIS IS A REAL ARTICLE CITING A REAL STUDY -THIS IS NOT FROM THE ONION OR ANY OTHER SATIRE SITE!
People who skipped their COVID vaccine are at higher risk of traffic accidents, according to a new study
Erin Prater
December 13, 2022, 1:31 PM EST
If you passed on getting the COVID vaccine, you might be a lot more likely to get into a car crash.
Or at least those are the findings of a new study published this month in The American Journal of Medicine. During the summer of 2021, Canadian researchers examined the encrypted government-held records of more than 11 million adults, 16% of whom hadn’t received the COVID vaccine.
They found that the unvaccinated people were 72% more likely to be involved in a severe traffic crash—in which at least one person was transported to the hospital—than those who were vaccinated. That’s similar to the increased risk of car crashes for people with sleep apnea, though only about half that of people who abuse alcohol, researchers found.
The excess risk of car crash posed by unvaccinated drivers “exceeds the safety gains from modern automobile engineering advances and also imposes risks on other road users,” the authors wrote.
Of course, skipping a COVID vaccine does not mean that someone will get into a car crash. Instead, the authors theorize that people who resist public health recommendations might also “neglect basic road safety guidelines.”
Why would they ignore the rules of the road? Distrust of the government, a belief in freedom, misconceptions of daily risks, “faith in natural protection,” “antipathy toward regulation,” poverty, misinformation, a lack of resources, and personal beliefs are potential reasons proposed by the authors.
The findings are significant enough that primary care doctors should consider counseling unvaccinated patients on traffic safety—and insurance companies might base changes to insurance policies on vaccination data, the authors suggest.
First responders may also consider taking precautions to protect themselves from COVID when responding to traffic crashes, the authors added, as it’s more likely that a driver is unvaccinated than vaccinated.
“The findings suggest that unvaccinated adults need to be careful indoors with other people and outside with surrounding traffic,” the authors concluded.
This isn’t the first time that researchers have examined the link between behavior and vaccination status. Among young adults, a 2021 study published in the Journal of Bioeconomics found a correlation between self-reported risky driving and having skipped their flu vaccine. It examined the survey responses of more than 100,000 Canadians.
People who skipped their COVID vaccine are at higher risk of traffic accidents, according to a new study
The findings could justify changes to driver insurance policies, the authors say.
Study Claims Unvaccinated People More Likely To Be Reckless, Cause Traffic Accidents | ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
 www.zerohedge.com
www.zerohedge.com
Study Claims Unvaccinated People More Likely To Be Reckless, Cause Traffic Accidents
by Tyler Durden
Thursday, Dec 15, 2022 - 08:40 PM
A new study released this month by members of the Temerty Faculty of Medicine at Toronto University in Canada makes the bizarre claim that being unvaccinated is an indicator of psychological risk-taking and recklessness. The authors, Donald A. Redelmeier, MD, Jonathan Wang, MMASc, and Deva Thiruchelvam, Msc argue that data involving traffic accidents in which one or more people are admitted to the hospital for injuries shows a correlation between vaccination status and car wrecks.
Not surprisingly, the data sources involved in the study strongly support the original premise. But we'll get to that in a moment...
The first question one might ask is why in the world anyone would engage in such a study in the first place? The notion is out of left field and requires a couple initial assumptions – That unvaccinated people are a monolithic group that share the same psychological motivators, and that those motivators are dangerous. Without this rather biased assumption, it's unlikely that a group of doctors or scientists would dream up the study in the first place.
Of course, strange premises are not necessarily proof of rigged conclusions. So, let's get into motivations:
The authors of the study are all member of the University or Toronto Temerty Faculty and the Sunnybrooke Health Sciences Centre. This faculty and section of the university was funded by a $250 million grant from James C. Temerty and the Temerty Foundation in 2020; it was the single largest gift in Canadian history. The money was designated to various areas of the university, but a large portion went directly into Covid-19 research projects.
So who is James Temerty? He is a Ukrainian born citizen of Canada and the founder of Northland Power, but his non-profit foundation appears to be his primary focus. He is also on the advisory board of the Atlantic Council, a globalist think-tank out of Washington DC with many of the same ideological aims promoted by the World Economic Forum. In fact, members of the Atlantic Council are often invited to speak at WEF functions and none other than Klaus Schwab was the very first recipient of the Atlantic Council's “Global Citizen Award” several years ago.
The Atlantic Council advisory board is a long list of global elites and corporate heads. The institution also had previous connections to Charles Koch, though this relationship has apparently ended.
Does anyone in the vaccine industry and Big Pharma have a close relationship to the Atlantic Council? Of course. Albert Bourla, the Chairman and CEO of Pfizer. Bourla is often invited to speak at Atlantic Council events and was awarded the council's Global Citizen Award just last year.
As many people are now aware, the methodology of globalist think tanks is to use philanthropy (large sums of tax deductible money) as a means to control society by influencing (or corrupting) the top 10% in the professional class/academic class.
If you can buy the people that run the colleges, buy the people in suits and buy the people in lab coats then you can own the narrative and control the other 90% of people who simply “defer to the experts” without doing their research. The Temerty Foundation clearly has a high level of influence over the University of Toronto and their medical wing, and James Temerty is on the advisory board of a globalist institution that has aggressively supported the Pfizer narrative on covid mandates and vaccination.
Any covid based study funded by members of the Atlantic Council should be immediately treated as suspect.
But what about the science itself? How did the Temerty Faculty come to the conclusion that lack of covid vaccination indicates reckless behavior? Where did they get the vaccination data? Where did they get the traffic data? How did they tie it all together?
The study claims to have developed their reference points using encrypted identifiers from official government registries. In other words, they exploited private medical data tracked by the Canadian government. By cross referencing vaccination status with severe traffic accidents the group asserts that the unvaccinated are 72% more likely to harm themselves or others in the process of a car wreck.
There are two problems immediately evident from a scientific standpoint:
One, the group admits that a much larger portion of people who are unvaccinated were younger, ages 18-39. This makes perfect sense, because the vast majority of young people are at near zero risk of mortality from a covid infection. The median Infection Fatality rate of covid is a tiny 0.23%, and the younger you are, the more the IFR shrinks. Why get a vaccine for a virus that is no threat to your age group, and that doesn't prevent transmission to those around you anyway?
But beyond that, younger people are also statistically more likely to get into car accidents by virtue of age, inexperience and more reckless behavior. While teens are known for auto accidents, insurance companies rate people ages 25 – 34 as the deadliest drivers on the road. This age group, coincidentally, makes up the bulk of the Temerty Faculty's unvaccinated test case.
In other words, the study seems to ignore the age factor in an effort to support the unvaccinated factor. Maybe their vaccine status has nothing to do with their risky behavior and their younger age is the actual cause? Which is more likely given the circumstance?
Two, another problem with the study is the complete lack of peer review and the inability for independent analysis of their core data. The group claims to have used encrypted government medical data that is unavailable to the public (rather convenient, right?). While certain government officials might be able to get quick access, there is no way for the general public to look at this data to see if their claims are accurate or if the study is rigged. They could, frankly, say whatever they want about the unvaccinated being dangerous and no one would be able to disprove it for quite some time.
Perhaps a couple of years down the road the study will be debunked, but as in most cases of dubious and potentially politically motivated science the headlines stick in people's minds while no one notices the retractions.
But what would be the motive for exaggerating this kind of study other than to try to make the unvaccinated look bad? Consider the possibility of insurance as leverage.
Most people are required by law to have insurance of one kind or another, including car insurance, and the premiums they have to pay are based on a company's (or government's) determination of risk. Imagine if your insurance rates in every area skyrocketed because you are unvaccinated and are considered high risk? This is likely the root purpose of studies like the one in Toronto.
Punish the unvaccinated by institutionalizing vaccine status into every facet of life, including car insurance, health insurance, life insurance, home insurance, business insurance, etc. Another point of leverage would be credit. Many bank loans are also based the concept of low risk, but if you are unvaccinated and labeled high risk in life and in finances then you could be rejected for future access to funds.
The basic strategy is this: Use high costs to force the unvaccinated into compliance, and slowly whittle the public down. These people won't give up easily, and since the direct route of medical tyranny has failed, they have decided to use indirect chicanery to get what they want.
Heliobas Disciple
TB Fanatic

Senate passes defense bill rescinding COVID vaccine mandate
A bill to rescind the COVID-19 vaccine mandate for members of the U.S. military and provide nearly $858 billion for national defense has passed the Senate and now goes to President Joe Biden to be signed into law.
 apnews.com
apnews.com
Senate passes defense bill rescinding COVID vaccine mandate
By KEVIN FREKING
Dec 15, 2022
WASHINGTON (AP) — A bill to rescind the COVID-19 vaccine mandate for members of the U.S. military and provide nearly $858 billion for national defense passed the Senate on Thursday and now goes to President Joe Biden to be signed into law.
The bill provides for about $45 billion more for defense programs than Biden requested and roughly 10% more than last year’s bill as lawmakers look to account for inflation and boost the nation’s military competitiveness with China and Russia. It includes a 4.6% pay raise for servicemembers and the Defense Department’s civilian workforce.
The Senate passed the defense policy bill by a vote of 83-11. The measure also received broad bipartisan support in the House last week.
To win GOP support for the 4,408-page bill, Democrats agreed to Republican demands to scrap the requirement for service members to get a COVID-19 vaccination. The bill directs Defense Secretary Lloyd Austin to rescind his August 2021 memorandum imposing the mandate.
Before approving the measure, the Senate voted down a couple of efforts to amend it, including a proposal from Sen. Joe Manchin, D-W.Va., to speed the permitting process for energy projects. The effort had drawn fierce opposition from some environmental advocacy groups who worried it would accelerate fossil fuel projects such as gas pipelines and limit the public’s input on such projects.
Manchin, who chairs the Senate Energy Committee, secured a commitment from Biden and Democratic leaders last summer to support the permitting package in return for his support of a landmark law to curb climate change.
Machin’s legislation sets deadlines for completion of National Environmental Policy Act reviews for major energy and natural resource projects. It would require courts to consider litigation involving energy project permits on an expedited basis. It also directs federal agencies to permit the completion of a natural gas pipeline in his home state and Virginia “without further administrative or judicial delay or impediment.”
“We’re on the verge of doing something unbelievable, but let me tell you, most of it will be for naught. Because without permitting reform, the United States of America is more litigious than any nation on earth,” Manchin told colleagues.
Biden voiced his support for Manchin’s legislation a few hours before Thursday’s vote. He said far too many projects face delays and described Manchin’s amendment “as a way to cut Americans’ energy bills, promote U.S. energy security, and boost our ability to get energy projects built and connected to the grid.“
Not only did some environmental advocacy groups bash Manchin’s proposal, but so did many Republicans. Minority Leader Mitch McConnell, R-Ky., said it didn’t go far enough, calling it “reform in name only.”
The amendment fell short of the 60 votes needed for passage, 47-47.
An amendment from Sens. Ron Johnson, R-Wis., and Ted Cruz, R-Texas, also went down to defeat. It would have allowed for the reinstatement of those service members discharged for failing to obey an order to receive the COVID-19 vaccine and compensate them for any pay and benefits lost as a result of the separation.
“People serving our military are the finest among us. Over 8,000 were terminated because they refused to get this experimental vaccine, and so I’m urging all of my colleagues to support Senator Cruz’s and my amendment,” Johnson said.
But opponents worried about the precedent of rewarding members of the military who disobeyed an order. Rhode Island Sen. Jack Reed, the Democratic chairman of the Senate Armed Services Committee, said orders are not suggestions, they are commands.
“What message do we send if we pass this bill? It is a very dangerous one,” Reed said. “What we’re telling soldiers is, ‘if you disagree, don’t follow the order, and then just lobby Congress, and they’ll come along and they’ll restore your rank, or restore your benefits, or restore everything.’”
The amendment failed, with 40 senators supporting it and 54 opposing it.
The defense bill sets policy and provides a roadmap for future investments. Lawmakers will have to follow up with spending bills to bring many provisions to reality. It’s one of the final bills Congress is expected to approve before adjourning, so lawmakers were eager to attach their top priorities to it.
The directive to rescind the vaccine mandate for service members proved to be among the most controversial provisions, but Democrats agreed to it to allow the bill to advance.
As of early this month, about 99% of the active-duty troops in the Navy, Air Force and Marine Corps had been vaccinated, and 98% of the Army. Service members who are not vaccinated are not allowed to deploy, particularly sailors or Marines on ships. There may be a few exceptions to that, based on religious or other exemptions and the duties of the service member.
The vaccination numbers for the Guard and Reserve are lower, but generally all are more than 90%.
Heliobas Disciple
TB Fanatic


China Reports New Omicron Variant Spreading in 9 Provinces; Populace Fearful, Mortuaries Overwhelmed
By Alex Wu
December 15, 2022
COVID-19 cases have been increasing in China since the ruling communist regime eased its “zero-COVID” restrictions on Dec. 7.
Netizens have been reporting that hospitals and mortuaries are being overwhelmed by demand, particularly in nine provinces where the relatively new Omicron coronavirus subvariants BQ.1 and BQ.1.1 have been reported to be spreading quickly.
On Dec. 14, China’s Center for Disease Control and Prevention announced for the first time that 49 cases of BQ.1 had been found in nine Chinese provinces, as well as cases of BQ.1.1. However, authorities didn’t identify which provinces were affected.
BQ.1 and BQ.1.1 are descendants of Omicron variant BA.5, which was first detected by scientists in South Africa in April. They started taking over BA.5 as the dominant COVID-19 strains in the United States in October and have been detected in more than 50 countries.
Just days earlier, on Dec. 12, the Chinese Communist Party (CCP) official media outlet People’s Daily reported, citing Chinese experts, that the strains spreading in China were still Omicron BA.5.2 and BF.7. According to the report, most cases in Guangzhou were BA.5.2, with a high proportion of asymptomatic patients due to milder clinical condition than BF.7, which was said to be the cause of most of the infections in Beijing, which has been experiencing more severe cases.
But the Dec. 14 announcement has stirred distrust and fear in Beijing, made worse by the many claims on social media of residents experiencing allegedly more severe symptoms unlike the typical cold-like symptoms associated with previous Omicron variants.
Uncertainty in Beijing
Many had already suspected that a new variant was spreading in Beijing.
They had dubbed the virus “Hellhound,” a name they found fitting for the dire situation, following a sharp increase in cases and worsening symptoms, including high fevers and lung infections. “Hellhound” was first used in Europe by locals fearing a faster-spreading variant, in reference to the pet of Hades, the Greek god who was said to guard the gates of the underworld.
Many Beijing residents posted on social media that people have now been infected by the “Hellhound” variant, which many suspect is BQ.1.1, describing more severe symptoms and numerous deaths.
There have yet to be any reports to confirm which variant is actually related to the reports of worsening symptoms.
Authorities had earlier dropped their mandatory mass testing program, and the country’s National Health Commission stated on Dec. 14 that it would no longer be reporting asymptomatic cases.
Sean Lin, a U.S. virologist and former director of the Department of Virology at the U.S. Army Research Institute, told The Epoch Times on Dec. 14 that “many people in mainland China have symptoms such as fever and cough, but in addition to the mutated Omicron virus, there may be other factors, such as influenza.”
“How many people are now suffering severe respiratory symptoms, and what is the number of hospitalizations, critical patients, and deaths? The authorities need to be transparent and publicize the numbers. But like in the past three years, official data have been opaque,” he said.
In October, Dr. Maria Van Kerkhove, the WHO’s COVID-19 technical lead, said that at the time, the new BQ.1 and BQ.1.1 Omicron variants hadn’t yet been linked to a change in severity, although the assessment was based on very limited data.
Doctors in Beijing have posted videos on social media calling on patients with mild symptoms to not visit the emergency room. This isn’t only to avoid infecting the medical staff there, but also to avoid the spread of the flu, which can aggravate COVID-19 symptoms, they said.
Many patients in critical condition are described as having symptoms in the lower respiratory tract, which resemble the symptoms during the outbreak in 2020 rather than the typically mild cold-like symptoms of other Omicron strains.
A Beijing netizen posted that they know more than a dozen colleagues in a company in Chaoyang district who have been infected with “Hellhound,” and all of them are seriously ill. A 27-year-old colleague ran a high fever of 40 degrees Celsius (104 degrees Fahrenheit) for five consecutive days, which left two of his organs inflamed and caused him to vomit blood. He’s currently on a ventilator.
This netizen also said several patients in the ward “have infections affecting the lungs, and some are suffering COVID + hyperemia.”
Current affairs commentator Li Muyang said on his NTD talk show on Dec. 13, “Judging from the information provided in these posts on social media, Hellhound is terrifying, with a high infection rate, severe symptom rate, and high death rate,” he said of the netizenry’s description of the situation in the Chinese capital, lacking information from official channels.
“If this is the virus that is spreading in Beijing, it’s not hard to understand the situation in the hospitals and mortuaries.”
Overwhelmed Hospitals, Mortuaries
The wave of likely COVID-19 infections has hit services in large cities hard, especially in Beijing and Guangzhou.
Patients have been reportedly flooding fever clinics and paralyzing local hospitals, with a large number of doctors and nurses also falling ill. Those showing moderate symptoms have been asked by authorities to keep working.
Dr. Li from Beijing Chaoyang Hospital told The Epoch Times on Dec. 9 that the ballooning number of COVID-19 infections has also led to a severe shortage of manpower among medical staff.
“We are seriously understaffed now. Many doctors and nurses are infected, and they cannot go to work. The same is true in other hospitals. There are many infections and a shortage of manpower. Several departments in our hospital have closed [because of it],” Li said.
The head nurse from a top-tier hospital in Beijing, Wan Ling (pseudonym), told state media: “At present, the symptoms of the infected colleagues in the hospital are relatively serious. Almost all of them have a high fever of 39 degrees and are sore all over their bodies. None of them are asymptomatic.”
Ms. Zhang, a Beijing resident, told The Epoch Times on Dec. 14 that residents know it’s now very difficult to expect ambulances to respond to calls for help.
According to a Beijing 120 emergency call dispatcher, the emergency system is collapsing. People who called at 7 a.m. for an ambulance didn’t see it arrive until 1 p.m., according to an incident reported by Radio Free Asia.
Ms. Zhang said delivery services have also been paralyzed in Beijing with many couriers being infected.
“[The goods] are piled up like mountains,” she said.
Several mortuary staff members in Beijing have also reported infections.
According to screenshots from netizen “Dolphin Peipei” on Chinese social media platform Weibo, medical workers at the Oriental Hospital of Beijing University of Traditional Chinese Medicine recently said: “Because the funeral home employees have tested positive one after another in the past two days, there is a serious shortage of staff. Due to the recent increase in the death rate in Beijing, the scheduled cremation time is at least 5 to 7 days, and the accumulation of remains is serious.” [...]
Mr. Lin, a staff member of Beijing Babaoshan Funeral Home, told The Epoch Times on Dec. 14 that the number of people who died in recent days was particularly high.
“Every day is very busy now,” he said. “I have never been so busy. I can’t answer the appointment calls, and many people are waiting in line.”
Mr. Liu, a staff member of Tongzhou Funeral Home in Beijing, said: “The farewell ceremony is all canceled now. The whole of Beijing is like this, it’s a city-wide regulation. The cremation appointment has been scheduled until Dec. 22.”
As for the reasons for the backlog, he said: “It is related to the COVID epidemic. But I don’t know whether the deaths are directly caused by the underlying diseases or COVID.”
Xiao Lusheng, Luo Ya, Zhao Fenghua, Hong Ning, and Reuters contributed to the report.
Heliobas Disciple
TB Fanatic

Omicron BQ, XBB subvariants are a serious threat to boosters and knock out antibody treatments, study finds
The latest omicron subvariants could cause a surge of breakthrough infections and reinfections, a new study finds.
 www.cnbc.com
www.cnbc.com
Omicron BQ, XBB subvariants are a serious threat to boosters and knock out antibody treatments, study finds
by Spencer Kimball
Published Wed, Dec 14 20224:26 PM EST | Updated Thu, Dec 15 20226:32 PM EST
KEY POINTS
- Scientists, in a study published online in the journal Cell, found that the BQ and XBB subvariants are "barely susceptible to neutralization" by the vaccines, including the new omicron boosters.
- This could result in a surge of breakthrough infections and reinfections, though the vaccines have been shown to hold up against severe disease, they wrote.
- Key antibody drugs, Evusheld and bebtelovimab, were "completely inactive" against the new subvariants, according to the study.
The omicron subvariants that have become dominant in recent months present a serious threat to the effectiveness of the new boosters, render antibody treatments ineffective and could cause a surge of breakthrough infections, according to a new study.
The BQ.1, BQ.1.1, XBB and XBB.1 omicron subvariants are the most immune evasive variants of Covid-19 to date, according to scientists affiliated with Columbia University and the University of Michigan. These variants, taken together, are currently causing 72% of new infections in the U.S., according to data from the Centers for Disease Control and Prevention.
The scientists, in a study published online Tuesday in the peer-reviewed journal Cell, found that these subvariants are "barely susceptible to neutralization" by the vaccines, including the new omicron boosters. The immune response of people who were vaccinated and had breakthrough infections with prior omicron variants also was weaker against the subvariants.
"Together, our findings indicate that BQ and XBB subvariants present serious threats to current COVID-19 vaccines, render inactive all authorized antibodies, and may have gained dominance in the population because of their advantage in evading antibodies," the scientists wrote.
Although these subvariants are more likely to cause breakthrough infections, the vaccines have been shown to remain effective at preventing hospitalization and severe disease from omicron, the scientists wrote.
The study examined blood samples from people who received three or four shots of the original vaccines, those who received the new omicron boosters after three shots of the original vaccines, and individuals vaccinated with the original shots who also had breakthrough infections from the BA.2 or BA.5 subvariants.
For people who received the omicron boosters, antibodies that block infection were 24 times lower against BQ.1, 41 times lower against BQ.1.1, 66 times lower against XBB and 85 times lower against XBB.1 compared to their performance against the ancestral strain that emerged in Wuhan, China, in 2019.
However, people who received the omicron boosters had modestly higher antibody levels against all of these subvariants compared with people who received three or four shots of the original vaccines, according to the study.
People who were vaccinated and had breakthrough infections had the highest antibody levels of any group in the study, though neutralization was also much lower against the subvariants than the ancestral strain.
The subvariants have evolved away from previous versions of omicron in dramatic fashion. BQ.1.1, for example, is about as different from omicron BA.5 as the latter subvariant is from ancestral Covid strain, according to the study.
"Therefore, it is alarming that these newly emerged subvariants could further compromise the efficacy of current COVID-19 vaccines and result in a surge of breakthrough infections, as well as re-infections," the scientists wrote.
XBB.1, however, presents the biggest challenge. It is about 49 times more resistant to antibody neutralization than the BA.5 subvariant, according to the study. XBB.1, fortunately, is currently causing no more than 1% of infections in the U.S., according to CDC data.
BQ.1.1 and BQ.1 represent 37% and 31% of new infections respectively, while XBB is causing 4.7% of new infections, according to CDC data.
Antibodies ineffective
Key antibody drugs, Evusheld and bebtelovimab, were "completely inactive" against the new subvariants, according to the study. These antibodies are used primarily by people with weak immune systems.
Evusheld is an antibody cocktail used to prevent Covid in people with weak immune systems who don't respond strongly to the vaccines. Bebtelovimab is used to prevent Covid from progressing to severe disease in organ transplant patients and other individuals who cannot take other treatments.
"This poses a serious problem for millions of immunocompromised individuals who do not respond robustly to COVID-19 vaccines," the scientists wrote. "The urgent need to develop active monoclonal antibodies for clinical use is obvious."
The Food and Drug Administration has already pulled its authorization of bebtelovimab nationwide because it is no longer effective against the dominant omicron variants in the U.S. Evusheld remains authorized as the only option for pre-exposure prophylaxis.
New Covid infections increased by about 50% to 459,000 for the week ended Dec. 7, according to CDC data. Covid deaths increased 61% to nearly 3,000 during the same week. Hospital admissions have plateaued at 4,700 per day on average after rising in November, according to the data.
White House chief medical advisor Dr. Anthony Fauci, in a press briefing last month, said U.S. health officials are hoping there's enough immunity in the population from vaccination, infection or both to prevent the massive surge of infections and hospitalizations the U.S. suffered last winter when omicron first arrived
Heliobas Disciple
TB Fanatic
BREAKING! Cambridge Study Finds That Cheap Generic Drug Ursodeoxycholic Acid Could Be Repurposed As A Prophylactic And Therapeutic Against COVID-19! - Thailand Medical News
COVID-19 Drugs: A new breakthrough study led by researchers from Cambridge University-UK has found that the commonly available cheap generic drug used to treat a type of liver disease ie Ursodeoxycholic Acid (UDCA), could be repurposed to not only treat COVID-19 but also act as an effective...
www.thailandmedical.news
Cambridge Study Finds That Cheap Generic Drug Ursodeoxycholic Acid Could Be Repurposed As A Prophylactic And Therapeutic Against COVID-19
Thailand Medical News
Dec 15 2022
A new breakthrough study led by researchers from Cambridge University-UK has found that the commonly available cheap generic drug used to treat a type of liver disease ie Ursodeoxycholic Acid (UDCA), could be repurposed to not only treat COVID-19 but also act as an effective prophylactic.
The drug is also not only effective against all existing SARS-CoV-2 variants but also against future emerging SARS-CoV-2 variants.
The study findings showed that Ursodeoxycholic Acid (UDCA), an existing drug used to treat a type of liver disease is able to ‘lock’ the doorway by which SARS-CoV-2 enters our cells, a receptor on the cell surface known as ACE2.
As the drug targets the host cells and not the virus, it should protect against future new variants of the virus as well as other coronaviruses that might emerge.
Once confirmed in larger clinical trials, this breakthrough discovery could provide a vital drug for protecting those individuals for whom vaccines are ineffective or inaccessible as well as individuals at increased risk of infection.
Dr Fotios Sampaziotis, from the Wellcome-MRC Cambridge Stem Cell Institute at the University of Cambridge -UK and Addenbrooke’s Hospital-UK led the study in collaboration with Professor Dr Ludovic Vallier from the Berlin Institute of Health at Charité-Germany.
The study team previously discovered an important molecule that regulates ACE2 ‘binding capabilities.’
The study team used organoids which are clusters of cells that can grow and proliferate in culture, taking on a 3D structure that has the same functions as the part of the organ being studied, in this case being “mini bile-ducts.”
Utilizing these, the study team found rather that a molecule known as FXR or farnesoid X receptor, which is present in large amounts in these bile duct organoids, directly regulates the viral ‘doorway’ ACE2, effectively opening and closing it.
The researchers went on to discover that ursodeoxycholic acid (UDCA), an off-patent drug used to treat a form of liver disease known as primary biliary cholangitis, ‘turns down’ FXR and closes the ACE2 doorway.
In this new study, the research team showed that they could use the same approach to close the ACE2 doorway in organoids representing ‘mini-lungs’ and ‘mini-guts’ ie representing the two main targets of SARS-CoV-2 and prevent viral infection.
The study team next progressed to animal studies to validate vivo capabilities of ursodeoxycholic acid (UDCA).
The COVID-19 Drugs study team teamed up with Professor Dr Andrew Owen from the University of Liverpool-UK to show that the drug prevented infection in hamsters exposed to the virus, which are used as the ‘gold-standard’ mod el for pre-clinical testing of drugs against SARS-CoV-2.
Importantly, the hamsters treated with ursodeoxycholic acid or UDCA were protected from the delta variant of the virus, which was new at the time and was partially resistant to existing vaccines.
The study team next worked with Professor Dr Andrew Fisher from Newcastle University-UK and Professor Dr Chris Watson from Addenbrooke’s hospital-UK to see if their findings in hamsters held true in human lungs exposed to the SARS-CoV-2 virus.
The study team took a pair of donated lungs not suitable for transplantation, keeping them breathing outside the body with a ventilator and using a pump to circulate blood-like fluid through them to keep the organs functioning while they could be studied.
For the study, one lung was given the drug, but both were exposed to SARS-CoV-2.
Significantly, the lung that received the drug ursodeoxycholic acid (UDCA), did not become infected, while the other lung did.
Dr Sampaziotis told Thailand Medical News, “This is one of the first studies to test the effect of a drug in a whole human organ while it’s being perfused. This could prove important for organ transplantation, given the risks of passing on COVID-19 through transplanted organs, it could open up the possibility of treating organs with drugs to clear the virus before transplantation.”
The study team next moved to human clinical trials.
For this, the COVID-19 Drugs study team at Cambridge team collaborated with Professor Dr Ansgar Lohse from the University Medical Centre Hamburg-Eppendorf in Germany.
The combined study team recruited eight healthy volunteers to receive the drug. When the researchers swabbed the noses of these volunteers, they found lower levels of ACE2, suggesting that the SARS-COv-2 virus would have fewer opportunities to break into and infect their nasal cells which are the main gateway for the virus.
The study team also studied data on COVID-19 outcomes from two independent cohorts of patients, comparing those individuals who were already taking ursodeoxycholic acid (UDCA) for their liver conditions against patients not receiving the drug.
The researchers found that patients receiving ursodeoxycholic acid or UDCA were less likely to develop severe COVID-19 and be hospitalized.
The study team said that the drug could be an affordable and effective way of protecting those for whom the COVID-19 vaccine is ineffective or inaccessible.
Dr Sampaziotis said, “We have used ursodeoxycholic acid or UDCA in clinic for many years, so we know it’s safe and very well tolerated, which makes administering it to individuals with high COVID-19 risk straightforward. This tablet costs little, can be produced in large quantities fast and easily stored or shipped, which makes it easy to rapidly deploy during outbreaks – especially against vaccine-resistant variants, when it might be the only line of protection while waiting for new vaccines to be developed. We are optimistic that this drug could become an important weapon in our fight against COVID-19.”
The study team is hoping to next find the necessary financial funding and support to conduct large randomized clinical trials.
The study team are the first to identify FXR ((farnesoid X receptor) as a direct regulator of angiotensin-converting enzyme-2 (ACE2) transcription among respiratory and gastrointestinal tissues impacted by COVID-19.
According to the study team, prevention of SARS-CoV-2 infection through the modulation of viral host receptors, such as ACE2, could represent a new chemoprophylactic approach for COVID-19.
To date however, the mechanisms controlling ACE2 expression remain elusive.
The study team identified farnesoid X receptor (FXR) as a direct regulator of ACE2 transcription in multiple COVID19-affected tissues, including the gastrointestinal and respiratory systems.
The COVID-19 Drugs study team then used the over-the-counter compound z-guggulsterone (ZGG) and the off-patent drug ursodeoxycholic acid (UDCA) to reduce FXR signaling and downregulate ACE2 in human lung, cholangiocyte and intestinal organoids and in the corresponding tissues in mice and hamsters.
They demonstrated that UDCA-mediated ACE2 downregulation reduces susceptibility to SARS-CoV-2 infection in vitro, in vivo and in human lungs and livers perfused ex situ.
The study team showed that ursodeoxycholic acid or UDCA reduces ACE2 expression in the nasal epithelium in humans and also showed a correlation between UDCA treatment and positive clinical outcomes following SARS-CoV-2 infection using retrospective registry data, and further confirmed these findings in an independent validation cohort of liver transplant recipients.
The study findings were published in the peer reviewed journal: Nature.
FXR inhibition may protect from SARS-CoV-2 infection by reducing ACE2 - Nature
Prevention of SARS-CoV-2 infection through the modulation of viral host receptors, such as ACE21, could represent a new chemoprophylactic approach for COVID-19 complementing vaccination2,3. However, the mechanisms controlling ACE2 expression remain elusive. Here, we identify the farnesoid X...
www.nature.com
The study team predicted that chenodeoxycholic acid (CDCA) might regulate ACE2 expression via FXR.
In order to test their theory, it was verified that FXR is expressed in vivo in gallbladder cholangiocytes and associated gallbladder cholangiocytes organoids (GCO) in vitro after activation by CDCA therapy.
To confirm whether FXR is required for CDCA-induced upregulation of ACE2, the team knocked down FXR among cholangiocyte organoids with short hairpin ribonucleic acid (shRNA), which blocked CDCA-induced upregulation of small heterodimer partner (SHP) and ACE2.
Next, to determine if FXR could interact with the ACE2 gene and possibly regulate its transcriptional activity, the study team assessed the ACE2 promoter region and noted the existence of an FXR-responsive element.
The COVID-19 Drugs study team examined in vitro whether FXR-mediated downregulation of ACE2 could diminish susceptibility to COVID-19.
The study team also subjected airway, gallbladder cholangiocyte, and intestine organoids to physiological amounts of CDCA to imitate the base level of FXR activation noted in vivo. These tissues were then infected with SARS-CoV-2, collected from a patient's nasopharyngeal swab with or without the presence of z-guggulsterone (ZGG) or ursodeoxycholic acid (UDCA).
Subsequently, the research team determined if the observed decrease in SARS-CoV-2 infection was a direct consequence of FXR-mediated ACE-2 downregulation.
In order to assess whether ACE2 regulation is the sole mechanism through which ZGG and UDCA inhibit SARS-CoV-2 infection, HEK293T cells were modified to over-express ACE2 irrespective of FXR with ZGG or UDCA followed by SARS-CoV-2 infection. The potential effects of UDCA treatment on COVID-19 patient outcomes were also tested by querying the COVID-Hep/SECURELiver registries. These registries provide information on patients with chronic liver disease who also tested COVID-19-positive and those with cholestatic liver diseases who received ursodeoxycholic acid (UDCA).
The COVID-19 Drugs study team using chromatin immunoprecipitation, confirmed that active FXR could bind directly to the ACE2 promoter. Significantly, site-specific mutation of the IR-1 region decreased the luciferase signal, revealing the FXR binding site specificity to the ACE2 promoter.
Importantly, in contrast, inhibition of FXR signaling with the FXR antagonist ZGG or ursodeoxycholic acid (UDCA) decreased FXR activity, as indicated by lowered levels of SHP, reduced FXR levels on ACE2 promoter, and ACE-2 downregulation at the protein and transcript. Collectively, the findings indicate that FXR directly regulates ACE2 expression in cholangiocytes.
Significantly, the study also noted that inhibiting FXR signaling with U.S, FDA approved drug ursodeoxycholic acid (UDCA) decreases ACE2 expression in many cell types.
Ursodeoxycholic acid (UDCA) mediated inhibition of FXR signaling lowered SARS-CoV-2 infection in all three types of organoids, demonstrating that knocking down FXR with shRNAs reduces ACE2 expression and suppresses viral infection among cholangiocyte organoids regardless of the presence of UDCA/ZGG or CDCA. Thus, after knockdown, neither UDCA nor ZGG affected viral infection.Without ACE2 regulation, neither UDCA nor ZGG affected viral replication.
The research findings demonstrate that Ursodeoxycholic acid (UDCA) decrease susceptibility to COVID-19 in several cell types in vitro by regulating ACE2 via FXR.
Utilizing multivariable logistic regression, the study team noted that Ursodeoxycholic acid (UDCA) exposure was related to a 46% decreased risk of contracting COVID-19. The connection was detected across the COVID-19 spectrum concerning symptomatic disease.
Future large randomized clinical trials should validate the effectiveness of Ursodeoxycholic acid (UDCA) as a COVID-19 prophylactic and therapeutic agent.
Zoner
Veteran Member
psychgirl
Has No Life - Lives on TB
How sad none of this will not only be seen by most of the population, but even if they do?
Not a soul will believe it because it’s not been spouted off as fact by the fake media.
Zoner
Veteran Member
How true and how sad and yet hopefully people they trusted will wake up and help others to do the same.How sad none of this will not only be seen by most of the population, but even if they do?
Not a soul will believe it because it’s not been spouted off as fact by the fake media.
I got to go back and read the mers thread
psychgirl
Has No Life - Lives on TB
Yes, that MERS thread is…well, I’m getting ready for a long 12 hr shift and the information posted there will take more time to digest.How true and how sad and yet hopefully people they trusted will wake up and help others to do the same.
I got to go back and read the mers thread
It’s not painting a pretty picture.

Where is the Mers thread?Yes, that MERS thread is…well, I’m getting ready for a long 12 hr shift and the information posted there will take more time to digest.
It’s not painting a pretty picture.
Zoner
Veteran Member
Where is the Mers thread?
HEALTH - MERS in Qatar?
Big sporting event, deadly outbreak. I can't keep up. 1.2 million at risk?? https://weather.com/en-IN/india/health/news/2022-11-29-camel-flu-threat-over-fifa-world-cup-symptom-causes-faq MERS is more dangerous than COVID19. As per the WHO, the mortality rate of this disease is a whopping...
Zoner
Veteran Member
Heliobas Disciple
TB Fanatic
The substack article referred to in those tweets; it's very long, it would take multiple posts and a lot of formatting to bring the whole thing over so I just posted the beginning of it; go to the link to read the whole thing if you are interested in reading the whole article (which I recommend).
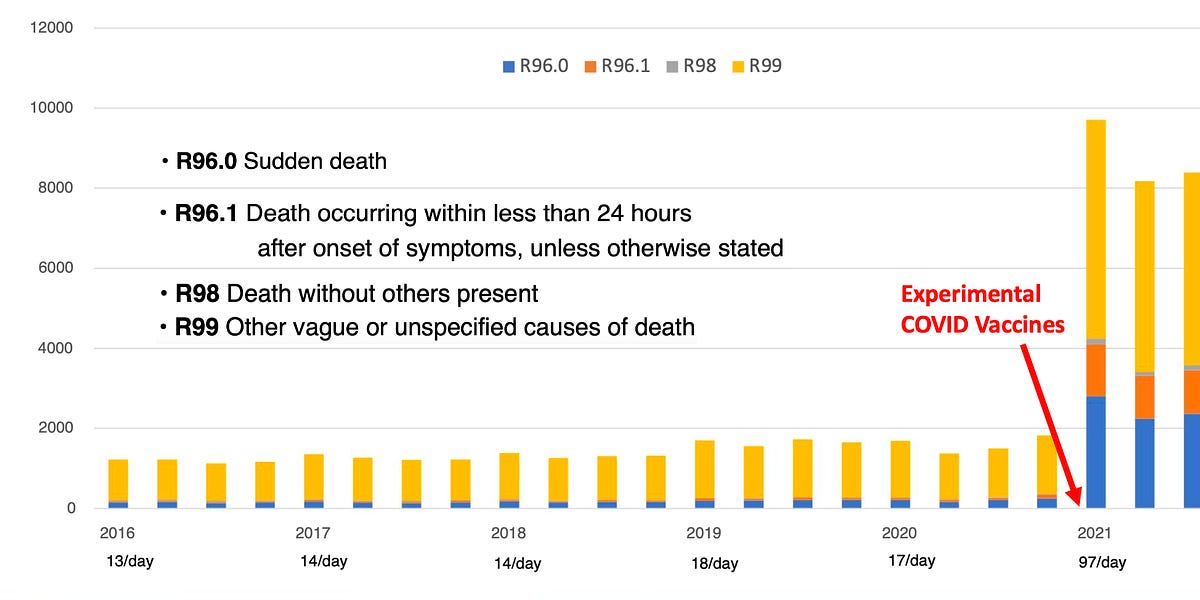
The Most Important Dataset of the Pandemic Was Just Released
Germany Has Provided The Means To Quantify The Human Cost Of The Experimental Vaccination Program
The Most Important Dataset of the Pandemic Was Just Released
Germany Has Provided The Means To Quantify The Human Cost Of The Experimental Vaccination Program
A Midwestern Doctor
Dec 13
Most sane people believe that the burden of proving safety should lie on the party conducting a questionable action, rather than their victim. For example, if a criminal shot someone, the prosecution would not be required to prove that the victim’s sudden death after the gunshot wound was not just a spontaneous coincidence, a result of extreme stress from the situation, or due to a pre-existing medical condition.
Unfortunately, the pharmaceutical industry has been able to establish a special type of privilege within the legal system and has made it very difficult to demonstrate that vaccines (along with many other pharmaceuticals) can ever be at fault for anything. Because of this, we recently had a flood of experimental vaccines mandated upon the population, which were never tested for safety (despite many serious concerns with their design), whose (likely fraudulent) clinical trial data was never made accessible to the public. We then had, as far as I know, the most aggressive propaganda campaign in history, and I watched the majority of my colleagues lose the ability to recognize any problems related to the vaccines. Instead, they developed an almost surreal religious devotion to the coming salvation (the vaccines becoming available).
Once the vaccines entered the market, a variety of red flags began going off indicating that these vaccines were killing people, and rather than address these concerns, the government—in concert with the media—chose to deny any of this was occurring. Instead they mandated the vaccines upon the entire population. I was understandably worried that the vaccines would cause problems and tried to do my part to head this off in 2020, but I did not expect anything on the scale of what we have encountered since then.
I personally became involved in all of this because soon after the vaccines entered the market, I began to have many friends and patients reach out to ask me if the vaccine could kill, because someone they knew had had a tragic sudden death after vaccination. Once the magnitude of the problem dawned on me, I realized that even though my available options were limited, I could at least do my best to document each case sent my way so that someone would bear witness to what had happened. Otherwise, the dead had no voice. Other than knowing I had a duty to compile this list, I was not sure what to do with it. Later after someone kindly helped launch this Substack, I decided to post it, it ended up being seen by a lot of people…and that is how I ended up writing here.
Because of how long it took to verify each case, I realized that I had to end it a year in (at which point I knew of 45 individuals who had either critical or fatal injuries of a similar nature in close proximity to vaccination). Since that time, I still continue to hear reports I periodically document and discuss.
For example, a good friend is a nurse in a cardiac unit and has told me many of the patients she sees now with heart failure are much younger than they were a few years ago. I previously advised her against getting the vaccine due to her history of rheumatic fever (a condition where the immune system attacks and damages part of the heart). This was because I had noticed both COVID-19 and especially its vaccine seemed to cause inflammatory flares at previous sites of injuries or inflammation (Lyme is also known for doing this). The vaccine also has a remarkably high rate of exacerbating pre-existing autoimmune conditions—such as the 24.2% rate found in a recent Israeli survey which is comparable to what a few colleagues have observed, and I suspect exacerbation of preexisting inflammation in the circulatory system, like what this study of 566 patients found, is a key mechanism behind vaccine deaths.
A month ago, that same friend I had advised against vaccinating informed me that she had developed a heart condition from the vaccine, her mother had as well ), and that her sibling's partner is suffering longterm complication from a stroke that immediately followed a booster.
Looking back on it, the thing I found the most disappointing about my own documentation project was that once it went viral, it should have triggered the drug regulators evaluating the vaccines to take preventative action. Instead, due to the meticulously planned campaign of mass censorship that we all found ourselves in, more red flags than I can count were ignored by the “very rigorous” vaccination surveillance systems that were allegedly ensuring there were no safety issues with these vaccines.
Because of the immense power behind the medical-industrial complex, those debating this program have been stuck fighting an uphill battle. However, despite the immense degree of corruption, withholding of critical data, and censorship, these vaccines are dangerous enough that more and more evidence is nonetheless emerging of their danger, and the public is beginning to recognize it. The previous article that was posted detailed how this appears to be happening:
After it was published, I was informed by a reader that possibly the most important dataset over the last two years was released today. For those interested, much of the context for today’s article can be found in the article above.German Data
One of the depressing realizations one gains from studying the evidence-based literature is discovering how many issues exist within it and how difficult it is to know which data sources can be trusted. One of my favorite authors, Dr. Malcom Kendrick, devoted a book to addressing this subject and shared a pertinent anecdote for today’s events:
“In truth, the figures on vaccine damage are exceedingly difficult to analyse, because causality is very difficult to prove on a case by case basis. However, when it comes to negative findings I always like to go to Germany. It has been demonstrated many times that the Germans are the most likely to report negative findings accurately. Yes I know, terrible racial stereotyping, but a fact is a fact. What do the Germans have to say on the matter?
“Between 1978 and 1993 approx. 13,500 cases of undesired effects resulting from medications for vaccinations was reported to the Paul Ehrlich-Institute (PEI)…the majority was reported by the pharmaceutical industry. In 40% [5,400] of these cases the complications were severe, 10% [1,350] pertained to fatalities on account of effects.”
Additionally, as I learned from Kendrick, since early 2001, the federal infection protection law has mandated that specific severe vaccine injuries be immediately reported directly to the PEI (Germany’s equivalent of the FDA for vaccines and biologics). The German’s list of reportable injuries is much broader than what I have seen acknowledged by many other countries (e.g. those which are possible to receive compensation for within the United States) and includes the previously discussed complications of DPT along with many of the reactions typically associated with the COVID-19 vaccines. However, while that historical trend exists, Germany has not been one of the best countries for reporting COVID vaccine injuries (which I suspect is due to the political direction their government has moved in).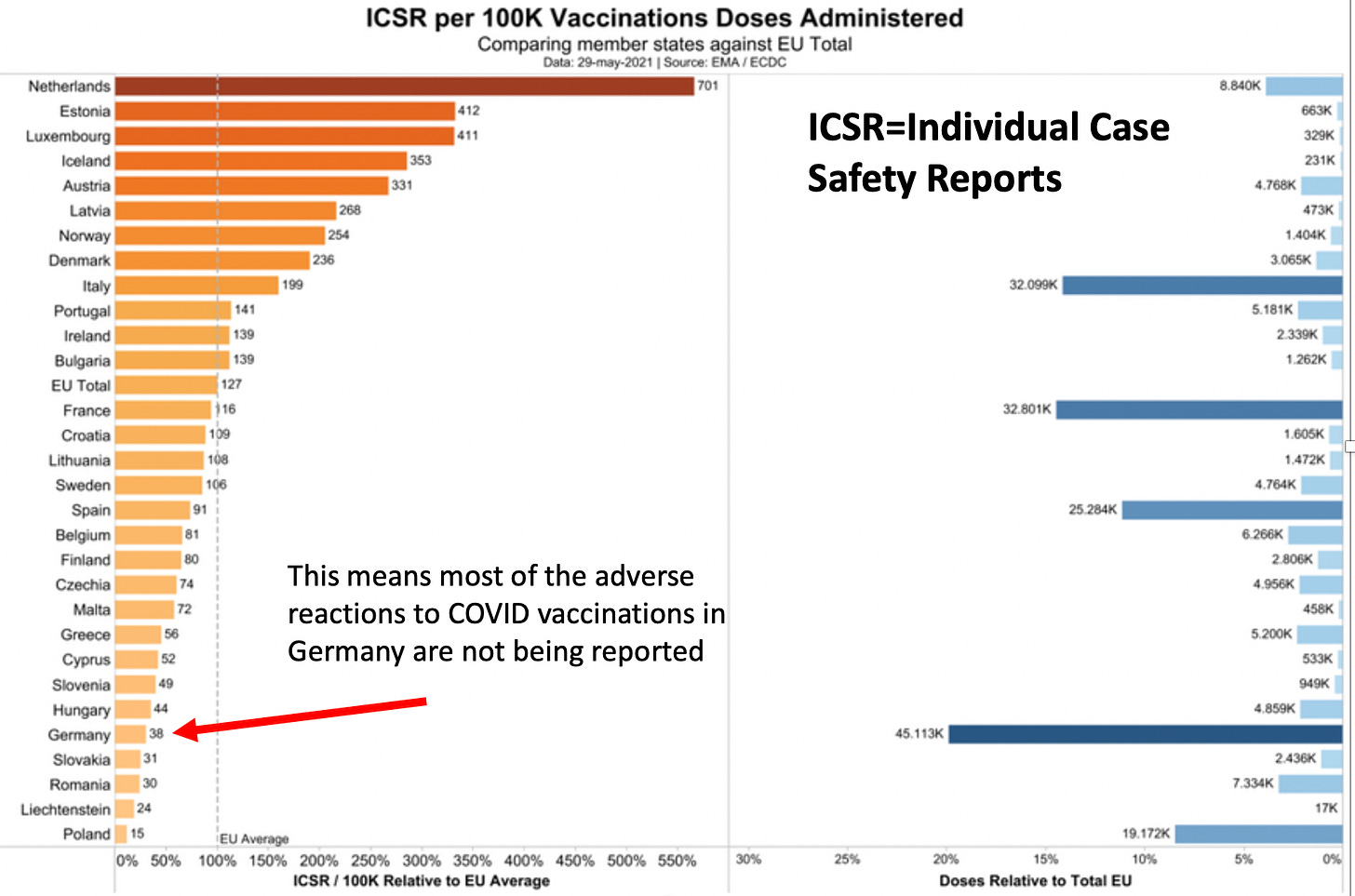
(The above graph illustrates why many of my German friends are not happy with their government)
SNIP [go to link for rest of very long article]
Heliobas Disciple
TB Fanatic
Some more information on BF7 in China, which with an R0 of around 15, should sweep through the cities in the next week or so
Remember the origin of the SARS-COV2 virus that causes C19 disease was in China. Maybe it’s a signpost (probably not) maybe it’s a forecast. We need to keep an eye on developments to see if there is a new variant forced by the interaction with the “whole inactivated” SInoVac vaccine - or whether...
Some more information on BF7 in China, which with an R0 of around 15, should sweep through the cities in the next week or so
Peter Halligan
13 hr ago
Remember the origin of the SARS-COV2 virus that causes C19 disease was in China. Maybe it’s a signpost (probably not) maybe it’s a forecast. We need to keep an eye on developments to see if there is a new variant forced by the interaction with the “whole inactivated” SInoVac vaccine - or whether the current R0 of up to 18.6 (!!!!) is reduced by the SinoVac intervention.
What happens in China could stay in China (unlike the original Wuhan virus) so it does not mean that the US, UK and EU will follow what is occurring in China, (or vice versa).
Here is a link to a video released yesterday 15 December 2022 by Dr John Campbell
The variant about to explode across the Middle Kingdom is BF7 (Actually, BA.5.2.1.7)
Referenced in the video is Dr Li Tongzeng, a medical expert at Beijing's Xiaotangshan Hospital cited in a Global Times article dated 28 November 2022 and a China Daily article of 29 November 2022 here:
Q&A: Beijing's latest COVID-19 outbreak - Chinadaily.com.cn
Some details on the BF7 (B.5.2.1.7) Omicron Outbreak About to Infect 1.4 billion Chinese people ahead of their New Year of the Rabbit on January 2023.
“The Omicron BF.7 was from outside Beijing, and is different to other sub-variants circulating in other parts of China. Compared with the BA.1, BA.2 and BA.5 variants detected previously, Omicron BF.7 has more immune escape capability, a shorter incubation period and faster transmission rate, said.”
BF7 represents 5% of SARS-COV2 variants of concern estimated to be circulating in the US, BQ.1 (41%) and BQ.1.1 (22%) total 74%.
Here’s a take on BF.7 from Health Site News on 12 October 2022
From the Asia Times dated 14 December 2022.
“BF.7 has been detected in several other countries around the world including India, the US, the UK. and several European countries such as Belgium, Germany, France and Denmark.”
Bullet points from a Chinese virologist, Dr Li as quoted in China Daily on 29 November 2022, who is dealing with patients.
- Lower immunity, R0 (how many other people does an infected person infect) – original “wild” strain = 2.4, Delta around 6, “Old” Omicron 5, BF7 – up to 18.6 – each infected person infects 18.6 others (unmitigated by any interventions). By way of illustration, an R0 of 15 would infect all of China in just over a week, maybe all of the US a day sooner. However, note that BF7 has been present for a while in the US and it is not replacing BQ.1 and BQ.1.1 (I have no source for variants of concern circulating in China).
- Shorter incubation – “People begin viral shedding one day after contracting an Omicron subvariant. The second-generation cases may appear within two or three days.”
- Recovery time – “The time for infected people to turn negative is still about seven to 10 days.”
- Symptoms – “Major symptoms of the Omicron variant BF.7 include fever, coughing, sore throat and decreased sense of smell and taste. A small number of people may suffer from diarrhea and vomiting.”
Heliobas Disciple
TB Fanatic
Study: Vaccines 'barely' neutralize newest COVID variants
Even "recent" boosting offers little protection, scientists claim.
Study: Vaccines 'barely' neutralize newest COVID variants
Even "recent" boosting offers little protection, scientists claim.
By Just the News staff
Updated: December 16, 2022 - 12:39pm
A scientific study is sounding an alarm bell regarding the latest COVID-19 variants, claiming that vaccines and boosters offer little protection against the newest mutations of the virus.
The study, published this week in the peer-reviewed journal Cell, claim that the BQ and XBB variants of COVID are "barely susceptible to neutralization by sera from vaccinated individuals."
The lack of vaccine effectiveness against the virus was observed in patients "with or without prior infection," the scientists said, including in "persons recently boosted with the new bivalent mRNA vaccines."
"[It is alarming that these newly emerged subvariants could further compromise the efficacy of current COVID-19 vaccines and result in a surge of breakthrough infections, as well as re-infections," the researchers said.
They noted that, though the data regarding the newest COVID variants were troubling, "it is important to emphasize that although infections may now be more likely, COVID-19 vaccines have been shown to remain effective at preventing hospitalization and severe disease even against Omicron."
Kewpie
Senior Member
It’s called HIPAA. And yes, certain information can not only get you fired, but lose your license. Im pretty damn skeptical of this information for SEVERAL reasons.I really hope that screenshot about the myocarditis cases at the pediatric hospital was fake because 1) I don't want bad things happening to kids and 2) That moron gave out so much identifying info that his friend (if real) will probably get fired.
Primarily; one of my besties who LOVES my child works in anesthesia for Cook Children’s Medical Center, one of the largest freestanding pediatric medical centers for children in the US. I’ve had many conversations with not only her but other people who are employed by Cooks. They’re not seeing anything like that. So either that’s a localized issue, or more than likely, a flat out lie.
It’s freaking shameful that people are so highly invested in identity politics they are willing to LIE about easily verified medical information to push an agenda. If you knew the name of the hospital, you can easily verify how many ICU beds they have and how many are occupied.
Oh, that’s right, when the hospital publishes that information, it’s automatically assumed disinformation and some random YouTuber or vague Twitter photo is given more credence because of confirmation bias. *insert eye roll here*
vector7
Dot Collector
That awkward silence in America right now is the vaccinated realizing the unvaccinated were right.
View: https://twitter.com/EmeraldRobinson/status/1604117209076404225?s=20&t=K3VVnhWm3su9Tm-Q4Ey69w
Just a few words on behalf of Americans that didn't take the jab
RT 2min
View: https://twitter.com/miguelifornia/status/1598460857750781952?s=20&t=NadjxVs5TYAv2p0dnW0-HQ
View: https://twitter.com/EmeraldRobinson/status/1604117209076404225?s=20&t=K3VVnhWm3su9Tm-Q4Ey69w
Just a few words on behalf of Americans that didn't take the jab
RT 2min
View: https://twitter.com/miguelifornia/status/1598460857750781952?s=20&t=NadjxVs5TYAv2p0dnW0-HQ
Heliobas Disciple
TB Fanatic
SARS-CoV-2 Variants: Ongoing Onslaught Of COVID-19 Infections Soon To Be Lead By New Cluster Of Sub-Lineages Including CH.1.1, CH.3, XAY.2, XBC, XBF, BE.10! - Thailand Medical News
SARS-CoV-2 Variants: The current global continuous onslaught of COVID -19 infections that is led by various BA.5 sub-lineages, the BQ.1, BQ.1.1BQ.1.1.4, BQ.1.12, BQ.1.22 subvariants, the XBB recombined variant including some of its newer spawns such as XBB.1, XBB.1.5, the BN.1.4, BN.1.3.1...
www.thailandmedical.news
SARS-CoV-2 Variants: Ongoing Onslaught Of COVID-19 Infections Soon To Be Lead By New Cluster Of Sub-Lineages Including CH.1.1, CH.3, XAY.2, XBC, XBF, BE.10
Thailand Medical News
Dec 18 2022
The current global continuous onslaught of COVID -19 infections that is led by various BA.5 sub-lineages, the BQ.1, BQ.1.1BQ.1.1.4, BQ.1.12, BQ.1.22 subvariants, the XBB recombined variant including some of its newer spawns such as XBB.1, XBB.1.5, the BN.1.4, BN.1.3.1 subvariants and BR.2 variants among the more than 500 new SARS-CoV-2 Variants and sub-lineages alongside recombinant variants that have emerged over the last 6 months is currently contributing to increased hospitalizations and excess deaths (COVID-19 deaths are strangely going down though) across many countries despite various health authorities and governments saying these new variants are mild and that we should learn to live with it.
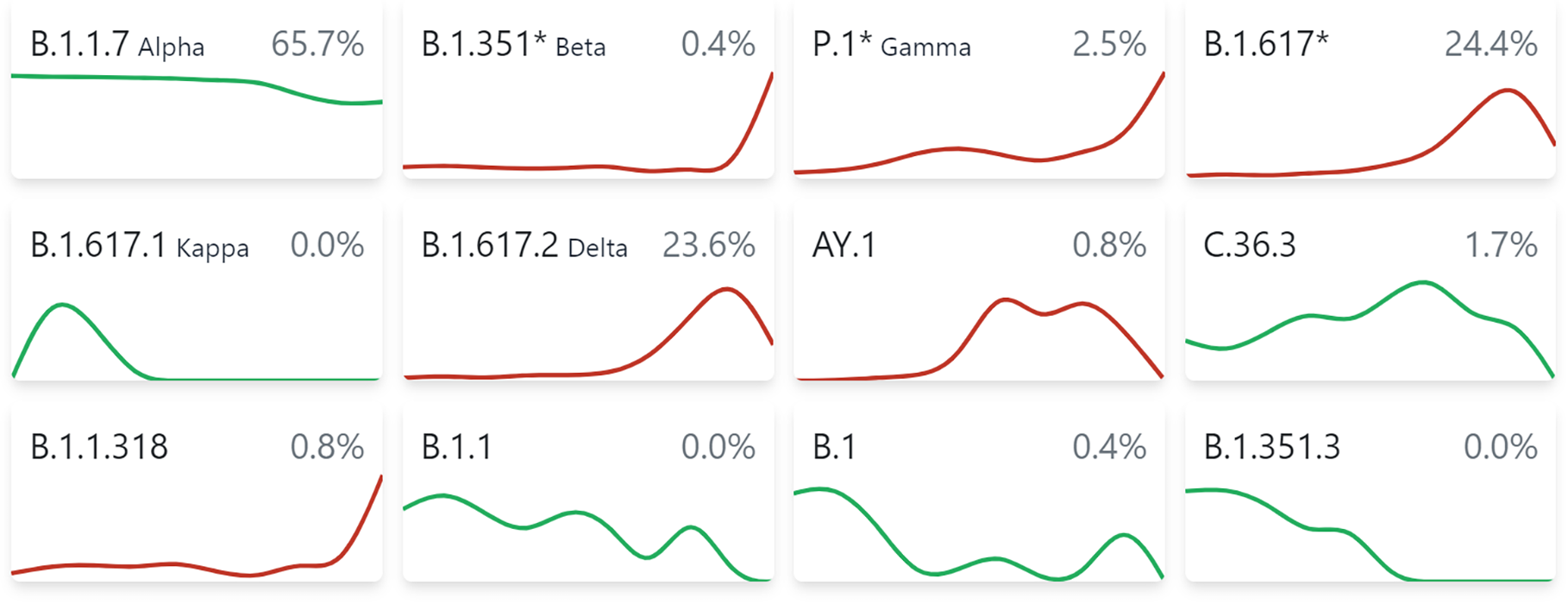
covSPECTRUM
covSPECTRUM is an interactive platform aiming to help scientists investigate and identify variants of SARS-CoV-2.
 cov-spectrum.org
cov-spectrum.org
Coronavirus (COVID-19) latest insights - Office for National Statistics
The latest data and trends about the coronavirus (COVID-18) pandemic from the Office for National Statistics and other sources.
www.ons.gov.uk
Excess mortality - statistics - Statistics Explained
This article examines the evolution of the number of deaths that occurred each month in the European Union, compared with a baseline of the average number of deaths for a particular month over the 4 years from 2016 to 2019.
 ec.europa.eu
ec.europa.eu
Deaths registered weekly in England and Wales, provisional - Office for National Statistics
Provisional number of deaths registered in England and Wales, including deaths involving coronavirus (COVID-19), in the latest weeks.
www.ons.gov.uk

COVID-19 News: Australian Bureau of Statistics Finds An Excess Death Rate Of 17 Percent For January 1 to August 31, 2022! Why Are So Many Australians Dying? - Thailand Medical News
COVID-19 News: The Australian Bureau of Statistics last month released the latest mortality data that alarmingly showed that there had been 128,797 deaths from January 1 to August 31, which was 17 per cent higher than the historical average...
www.thailandmedical.news
Do take note that most COVID-19 statistical data and excess deaths data are not reliable as many governments are deliberately trying to conceal actual data and impact of the ongoing crisis and in reality, the actual figures could be much higher.
Regime type and Data Manipulation: Evidence from the COVID-19 Pandemic
Autocratic and democratic leaders have an incentive to misreport data that may reveal policy failure. However, it is easier for autocratic leaders to fabricate data because they are not subject to scrutiny from media, opposition parties, and civil society. This suggests that autocratic...
 www.medrxiv.org
www.medrxiv.org
Most of the current SARS-CoV-2 Variants and sub-lineages in circulation are more immune evasive and trans missible and are causing breakthrough infections and constant reinfections in many.

Alarming antibody evasion properties of rising SARS-CoV-2 BQ and XBB subvariants
Recent BQ and XBB subvariants of SARS-CoV-2 demonstrate dramatically increased ability to evade neutralizing antibodies, even those from people who received the bivalent mRNA booster or who are immunized and had previous breakthrough Omicron infection. Additionally, both BQ and XBB are...
www.cell.com
Constant reinfections can in fact increase disease severity and also increase the risk of mortality.
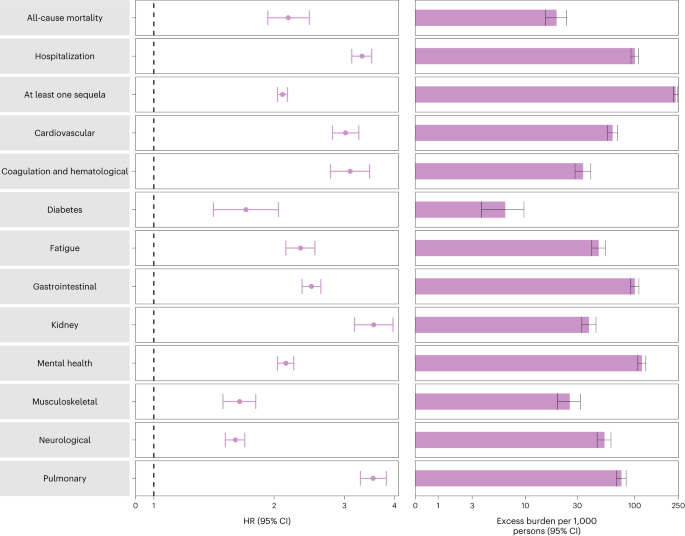
Acute and postacute sequelae associated with SARS-CoV-2 reinfection - Nature Medicine
A new analysis using US Department of Veterans Affairs databases showed that reinfection is associated with increased risk of all-cause mortality, hospitalization and a wide range of long COVID complications in individuals who have had SARS-CoV-2 compared to those with no reinfection.
 www.nature.com
www.nature.com
In fact, new studies are also indicating that the new bivalent boosters being promoted extensively by health authorities are literally hopeless against these new variants and sub-lineages though some are claiming that they reduce disease severity and lower risk of mortality!
COVID-19 News: Hybrid Immunity And Bivalent Boosters Have Little Effect On New Omicron Sub-Lineages BQ.1.1 And BA.2.75.2 Due To Immune Imprinting! - Thailand Medical News
COVID-19 News: Despite various governments, health authorities and mainstream media are trying to downplay the dire situation we are in with regards to the COVID-19 pandemic and are concealing COVID-19 statistics and also implications of long term catastrophic issues while making stupid claims...
www.thailandmedical.news
It is projected that in a matter of weeks, most of the predominant variants and sub-lineages in circulation will be quickly superseded by a new cluster of SARS-CoV-2 variants that have better growth advantage and are also more immune evasive.
Unlike in the past, when we have specific periodic surges driven by one or tow variants of concern with periods of respite, we will no longer see such surges anymore, rather, the world will be faced by a continuous onslaught of COVID-19 infections driven by clusters consisting of numerous variants and sub-lineages that are quickly displaced by newer clusters.

SARS-CoV-2 Variant Soup Means No More Waves Or Surges But Rather Constant Onslaught And Reinfections! China Reports Record COVID-19 Infections! - Thailand Medical News
COVID-19 News: While governments and health authorities along with paid mainstream media around the world try to downplay rising COVID-19 infections and the seriousness and dangers of Long COVID-19, the good news is that as a result of the SARS-CoV-2 Omicron variants and sub-lineages along with...
www.thailandmedical.news
The SARS-CoV-2 is rapidly evolving and spawning newer mutations and subvariants and sub-lineages at an unprecedented phase that has never been witnessed in the annals of virology.
The next clusters are expected to be head by the CH.1.1, CH.3, XAY.2, XBC, XBF, BE.10, CH.3.1, XBK, BQ.1.15, BR.2.1 variants and sub-lineages among many others.
All these newer variants are likely to be also more immune evasive and also more transmissible with enhanced growth advantage.
New Emerging SARS-CoV-2 Variants And Sub-lineages Such As BQ1.1.10, XBB.3, BA.4.6.3 and CH.1.1 Are Taking Immune Evasion To A Newer Level! - Thailand Medical News
COVID-19 News: Researchers are sounding alarms that while the SARS-CoV-2 coronavirus is evolving rapidly and spawning a variety of variants and sub-lineages, some of these such as the BQ1.1.10, XBB.3, BA.4.6.3 and CH.1.1 sub-lineages are literally taking immune evasion to a whole new level. It...
www.thailandmedical.news
New SARS-CoV-2 Variants BR.2 And XBF Expected To Become Dominant Midway In Winter Surge. Current Surges Not Severe, Rather Will Kill Slowly! - Thailand Medical News
COVID-19 News: Scientist are predicting that the new SARS-CoV-2 Omicron variant called BR.2.1 and also a new recombinant variant XBF is expected to be become dominant in circulation sometime midway in the winter surge and will join other newly emerging variants in creating non-stop COVID-19...
www.thailandmedical.news
covSPECTRUM
covSPECTRUM is an interactive platform aiming to help scientists investigate and identify variants of SARS-CoV-2.
cov-spectrum.org
covSPECTRUM
covSPECTRUM is an interactive platform aiming to help scientists investigate and identify variants of SARS-CoV-2.
cov-spectrum.org
covSPECTRUM
covSPECTRUM is an interactive platform aiming to help scientists investigate and identify variants of SARS-CoV-2.
cov-spectrum.org
covSPECTRUM
covSPECTRUM is an interactive platform aiming to help scientists investigate and identify variants of SARS-CoV-2.
cov-spectrum.org
The XBK variant is a BA.5.2 and CJ.1 recombinant that first emerged in Netherlands but has since seems to be growing in circulation in various parts of Europe including Belgium, Austria, Denmark and even Japan now.
BA.5.2/CJ.1 recombinant, 46 samples from Denmark and 8 other countries · Issue #1418 · cov-lineages/pango-designation
Description: Sub-lineage of BM.1.1 with S:F490S, S:F486P and C1627T or BA.5.2/CJ.1 recombinant Nucleotide mutations: C1627T (and T23031C, T23018C) Earliest sequence: 2022-10-07 from the Netherlands...
 github.com
github.com
covSPECTRUM
covSPECTRUM is an interactive platform aiming to help scientists investigate and identify variants of SARS-CoV-2.
cov-spectrum.org
The XAY.2 recombinant variant is the most concerning variant as besides being a Delta and BA.2 recombinant variant, it seems to be having enhanced growth advantage and is now found in many countries already and is expected to becoming dominant very fast.
There are speculations that it has enhanced pathogenesis which contributes to increased disease severity and hospitalizations along with increased mortality risk.
It is now found in Denmark, Philippines, Sweden, South Korea South Africa, New Zealand, Germany, Australia but so far in small clusters but that is expected to change in coming weeks as it becomes predominant.
Worrying, it is also anticipated that some of these variants and sub-lineages as they continue to evolve, might start ‘picking up’ mutations around the 680-699 regions of the spike and also unique 839 or 486 (through reverse zoonotic infections especially by minks, coinfections or recombinant events) mutations. All of which are expected to contribute to disease severity through syncytia formation.
It Takes Two: Bimodal interactions between the SARS-CoV-1 fusion peptide and Ca2+ ions promote membrane insertion and viral entry
In coronaviruses, the fusion peptide (FP) is situated within the membrane fusion domain of the spike protein, becoming exposed following proteolytic cleavages at the S1/S2 and S2’ sites. After receptor binding-induced conformational changes, the FP penetrates the host cell membrane and mediates...
 www.biorxiv.org
www.biorxiv.org

BREAKING NEWS! Study Confirms P681R Mutation Found On Delta Variant Has Special Infection Strategy And Can Evade Immunity Induced By Vaccination Or Natural Infection! - Thailand Medical News
Variant News: Japanese scientists have conducted a new research in which the findings show that the B.1.617 lineage of the SARS-CoV-2 coronavirus that emerged in India has evolved a unique strategy to facilitate infection and evade the immunity induced by vaccination or natural infection...
www.thailandmedical.news
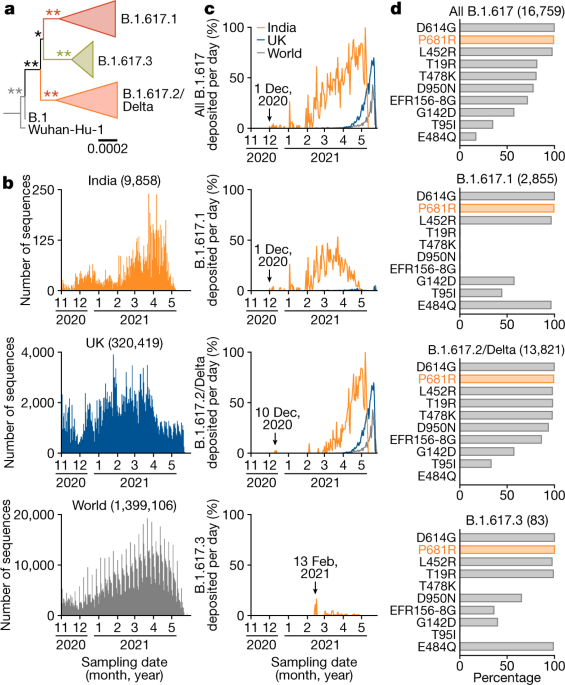
Enhanced fusogenicity and pathogenicity of SARS-CoV-2 Delta P681R mutation - Nature
The P681R mutation in the spike protein renders the Delta variant more pathogenic than prototypic SARS-CoV-2 in infected hamsters, and facilitates spike protein cleavage and enhances viral fusogenicity.
www.nature.com
SARS-CoV2 spike protein gene variants with N501T and G142D mutation–dominated infections in mink in the United States
Large numbers of mink have been infected with SARS-CoV2 containing the spike protein Y453F mutation in Europe, causing zoonosis concerns. To evaluate the genetic characteristics of the U.S. and Canadian mink–derived SARS-CoV2 sequences, we analyzed ...
 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
While we are fortunate to a certain degree that most of the current new variants and sub-lineages in circulation are only causing mild symptomatic infections in the otherwise general healthy populations except those in the vulnerable groups (ie the aged, the young, the obese, the immunocompromised those with existing comorbidities and those with certain ‘genetic-makeup’), that is expected to change drastically in coming weeks.
Also, it should be noted that it is a complete fallacy to assume that even an asymptomatic or mild infection is ok as these new variants are not only more immune evasive but they have adapted so well to disarm most of the human host immune responses so as to accommodate it ‘plans’ for longer periods of viral persistence in the human host.
Viral persistence is a major health threat and even more concerning is that latest studies are showing that during its presence in the human host in various viral reservoir areas such as deep tissues or various organs etc, it is able to control or even decrease inflammatory levels so that its presence is not easily detectable until stages where sufficient damage has been done to those particular tissues or organs.
BREAKING! COVID-19 News: Finally, U.S. NIH Warns SARS-CoV-2 Viral Persistence Is A Serious Issue That Is Also Affecting Long COVID! - Thailand Medical News
COVID-19 News: After yet another autopsy study, this time involving 44 patients who died from COVID-19 and Long COVID, the study team from the U.S. NIH and U.S. NIAID who found active SARS-CoV-2 RNA is various anatomic sites including the brain and various organs, have issued a warning that...
www.thailandmedical.news
That is why, we are now seeing so many sudden fatal outcomes contributing to excess deaths from heart failures, kidney failures, other organ failures, strokes and sepsis etc.
The coming weeks will be more fun as these many new variants become predominant and we expect that 2023 will even be more interesting as it is very likely more lethal and pathogenic SARS-CoV-2 variants and even SARS-CoV-3 might debut along with newer strains of other pathogens while the masses continue to have their immune systems depleted via constant reinfections.
Without even considering China, the IHME model at University of Washington is predicting on an optimistic and conservative level that up to a million people are expected to die from COVID-19 for the next three months ie from now to the 1st Of April 2023.
IHME | COVID-19 Projections
Explore forecasts of COVID-19 cases, deaths, and hospital resource use.
 covid19.healthdata.org
covid19.healthdata.org
We at Thailand Medical News rather believe that without the advent of any other new more pathogenic or lethal variant besides those we already mentioned, there should be at least 3 to 6 million COVID-19 deaths including considering China till the Ist of April 2023, taking into account the current kinetics of the pandemic. This figure does not include excess deaths or deaths due to “long COVID” issues. We do hope that we are wrong.
Heliobas Disciple
TB Fanatic
I have been posting article about what is happening in China because they are starting to have massive outbreaks. In the next post the article states that lifting the zero covid policy didn't cause the outbreak, they lifted the policy because it couldn't stop it. Either way - the zero policy didn't provide the Chinese people with the same natural immunity from constant exposure that Geert talks about. But the variants now have a huge population to defeat immune pressure and that can bring about the "Geert variant".

 news.yahoo.com
(fair use applies)
news.yahoo.com
(fair use applies)
COVID-19 is about to explode in China. What that could mean for the United States.
Karen Weintraub, USA TODAY
Sat, December 17, 2022, 12:11 PM EST
China is likely to see an explosion of COVID-19 cases in coming weeks, experts say, as the country lifts its long-standing and highly unpopular zero-COVID-19 policy.
China is extremely vulnerable right now because its population – especially older adults, who are the most likely to suffer severe disease – is undervaccinated, has no natural immunity from infection and a limited supply of treatments.
Experts predict hundreds of millions of infections and as many as 1.5 million to 2 million deaths.
"I think China is going to blow in the next six to 12 weeks," said Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, in a Thursday webinar. "Instead of falling off a 5-foot cliff, we're going to watch them fall off a 1,000-foot cliff."
A raging epidemic in China could be bad news for controlling the virus in the U.S., he and other experts said, because travelers will arrive sick and the chances of mutation increase anytime a virus infects a lot of people.
China lifts zero-COVID policy. How will the US be impacted?
Any time a virus rages out of control, especially in a population as large as China's, there is a good chance that new variants will develop, said Dr. Jeremy Luban, an expert in viruses at the UMass Chan Medical School.
The variants now circulating in China seem to be the ones that have been most prevalent here, including the omicron subvariants BA.5 and BQ.1.
"There's no specific reason to be concerned other than that a lot of infections are bad for evolution of new things that we can't predict," Luban said Wednesday on a Massachusetts Consortium on Pathogen Readiness media call. "The more the rate of infection can be controlled in China, the better."
The U.S. carefully monitors for infections and variants among travelers, using wastewater and other means, said Dr. Ashish Jha, the White House coronavirus response coordinator, in a Thursday news conference.
"If new variants emerge, I'm confident we'll be able to address them," he said.
What's likely to happen in China?
One model predicts China will see 100 million symptomatic cases, 5 million hospital admissions and up to 1.6 million deaths, just from COVID-19, not counting the strain on the health system that will lead to even more tragedies, said Jennifer Bouey, a RAND epidemiologist.
She said there are not enough intensive care units in the country to handle this level of demand and she expects the health care system will be overwhelmed. Blood banks are already seeing a shortage of donations, she said.
If mainland China were to see the same death rate as Hong Kong did during an outbreak in February and March, more than 2 million Chinese people would be predicted to die in the coming months, said William Hanage, an epidemiologist at the Harvard T.H. Chan School of Public Health, on the call with Luban.
Why is China so vulnerable to COVID-19 right now?
'A very hard road ahead' for China
Following widespread public protests, the Chinese government lifted its zero-COVID-19 restrictions on Dec. 1.
Bouey said she's seen little evidence that the Chinese government was prepared to suddenly lift its restrictions. A booster campaign this summer would have made a big difference, along with a substantial pre-purchase of antiviral treatments.
"We see the government just starting the last couple of days talking about boosters and antivirals," she said.
Heath said reversing course now "will further fuel distrust and skepticism among the Chinese people who are not sure how much truth the government is really telling."
Both he and Bouey said they don't think the government is accurately reporting COVID-19 cases right now. Official reports say infections are falling, while social media, empty streets and shops, medication shortages, and long lines at hospitals tell a different story.
Still, Hanage predicts China will have fewer deaths per capita than the U.S. because it delayed its outbreak until after the arrival of vaccines. "China has a very, very hard road ahead of it in the coming months, don't get me wrong, but in the absence of vaccination, it would be much, much worse."
COVID-19 is about to explode in China. What that could mean for the United States.
Experts are predicting COVID cases in China will explode after the country ended its strict zero-COVID policy. Here's how the US may be affected.
COVID-19 is about to explode in China. What that could mean for the United States.
Karen Weintraub, USA TODAY
Sat, December 17, 2022, 12:11 PM EST
China is likely to see an explosion of COVID-19 cases in coming weeks, experts say, as the country lifts its long-standing and highly unpopular zero-COVID-19 policy.
China is extremely vulnerable right now because its population – especially older adults, who are the most likely to suffer severe disease – is undervaccinated, has no natural immunity from infection and a limited supply of treatments.
Experts predict hundreds of millions of infections and as many as 1.5 million to 2 million deaths.
"I think China is going to blow in the next six to 12 weeks," said Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, in a Thursday webinar. "Instead of falling off a 5-foot cliff, we're going to watch them fall off a 1,000-foot cliff."
A raging epidemic in China could be bad news for controlling the virus in the U.S., he and other experts said, because travelers will arrive sick and the chances of mutation increase anytime a virus infects a lot of people.
China lifts zero-COVID policy. How will the US be impacted?
Any time a virus rages out of control, especially in a population as large as China's, there is a good chance that new variants will develop, said Dr. Jeremy Luban, an expert in viruses at the UMass Chan Medical School.
The variants now circulating in China seem to be the ones that have been most prevalent here, including the omicron subvariants BA.5 and BQ.1.
"There's no specific reason to be concerned other than that a lot of infections are bad for evolution of new things that we can't predict," Luban said Wednesday on a Massachusetts Consortium on Pathogen Readiness media call. "The more the rate of infection can be controlled in China, the better."
The U.S. carefully monitors for infections and variants among travelers, using wastewater and other means, said Dr. Ashish Jha, the White House coronavirus response coordinator, in a Thursday news conference.
"If new variants emerge, I'm confident we'll be able to address them," he said.
What's likely to happen in China?
One model predicts China will see 100 million symptomatic cases, 5 million hospital admissions and up to 1.6 million deaths, just from COVID-19, not counting the strain on the health system that will lead to even more tragedies, said Jennifer Bouey, a RAND epidemiologist.
She said there are not enough intensive care units in the country to handle this level of demand and she expects the health care system will be overwhelmed. Blood banks are already seeing a shortage of donations, she said.
If mainland China were to see the same death rate as Hong Kong did during an outbreak in February and March, more than 2 million Chinese people would be predicted to die in the coming months, said William Hanage, an epidemiologist at the Harvard T.H. Chan School of Public Health, on the call with Luban.
Why is China so vulnerable to COVID-19 right now?
- Natural immunity: Because of the zero-COVID-19 policy, few Chinese people have been infected so they lack natural immune protection, Bouey said.
- Vaccine protection has waned: About 90% of the Chinese population got a first round of vaccinations but far fewer received boosters and most of those shots were more than six months ago, she said.
- Lack of trust: Early in the pandemic, there were some scandals where patients were given fake or adulterated COVID-19 vaccines, reducing public faith in them, said Timothy Heath, a senior international defense researcher at RAND.
- Vaccine misconceptions: The government also prioritized vaccinating young, healthy people, which fostered a public belief that the vaccine could be dangerous for older people.
'A very hard road ahead' for China
Following widespread public protests, the Chinese government lifted its zero-COVID-19 restrictions on Dec. 1.
Bouey said she's seen little evidence that the Chinese government was prepared to suddenly lift its restrictions. A booster campaign this summer would have made a big difference, along with a substantial pre-purchase of antiviral treatments.
"We see the government just starting the last couple of days talking about boosters and antivirals," she said.
Heath said reversing course now "will further fuel distrust and skepticism among the Chinese people who are not sure how much truth the government is really telling."
Both he and Bouey said they don't think the government is accurately reporting COVID-19 cases right now. Official reports say infections are falling, while social media, empty streets and shops, medication shortages, and long lines at hospitals tell a different story.
Still, Hanage predicts China will have fewer deaths per capita than the U.S. because it delayed its outbreak until after the arrival of vaccines. "China has a very, very hard road ahead of it in the coming months, don't get me wrong, but in the absence of vaccination, it would be much, much worse."
Last edited:
Heliobas Disciple
TB Fanatic

One million people could die from COVID-19 in China next year, according analysis of a new report
New research from the Institute of Health Metrics and Evaluation predicts China could experience a sharp increase in COVID-19 deaths in 2023.
One million people could die from COVID-19 in China next year, according analysis of a new report
Bethany Dawson - Business Insider
Sat, December 17, 2022, 8:17 AM EST
2023 could see over 1 million COVID-19 deaths in China, per Reuters' analysis of a new report.
The projected surge in deaths comes in the wake of China's rollback of its zero-COVID policies earlier this month.
The report predicts that the COVID-19 death toll in China could reach over 300,000 by April 2023.
According to Reuters' analysis of a new report released by the US-based Institute of Health Metrics and Evaluation, also known as IHME, China could see more than one million COVID-19 deaths in 2023.
This projected surge in cases and deaths comes after the sudden relaxation of China's zero-COVID policy coinciding with the Chinese New Year festivities next month.
The IHME has suggested that the virus would peak at the start of April 2023, when they believe the country's COVID-19 deaths will soar to 322,000.
Currently, China has reported 5,235 fatalities related to the virus, according to Our World in Data, an organization from the University of Oxford.
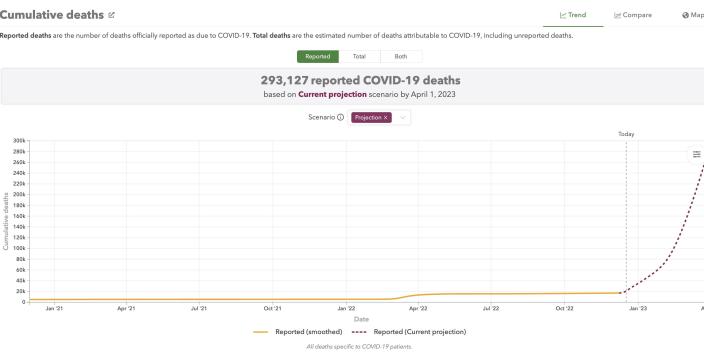
Death projections in China from the Institute of Health Metrics and Evaluation
COVID-19 death toll projections in China from the Institute of Health Metrics and Evaluation.Institute of Health Metrics and Evaluation
The zero-COVID measures were lifted last month following widespread protests.
Experts are most concerned about the elderly population in China, who are vulnerable to the virus due to age, but also have lower vaccine take-up when compared to other demographic groups in China, IHME Director Chris Murray said in a video statement earlier this month.
Speaking about the year ahead, Murray suggested that many places will see waning immunity against the more recent Omicron variants worldwide, but China was the biggest concern. "It's not as if the only place in the world that's at great risk is China. It's just that that's the biggest concentration right now for that at-risk population," Murray said of the over-80 population.
Murray said China has not indicated that it will provide better vaccines, more vaccinations, or anti-virals in the wake of its zero-COVID policy becoming unsustainable.
China has refused to use western vaccines in its fight against COVID-19, instead relying on its homegrown inoculations. However, according to Politico, the Chinese vaccines have done little to curb the latest coronavirus variants, including the highly transmissible omicron variant.
Public health experts told Insider that China's lockdown policies should have been used to increase vaccination rates as much as possible, but failed to do so. Now, there are large swathes of China's over-80s population that are at risk of dying from COVID-19.
Heliobas Disciple
TB Fanatic

US, German Embassies in China Suspend Visa Services as COVID Infections Soar
U.S. and German embassies in China's capital of Beijing announced on Dec. 15 the suspension of routine visa services ...
 www.theepochtimes.com
www.theepochtimes.com
US, German Embassies in China Suspend Visa Services as COVID Infections Soar
By Alex Wu
December 17, 2022
U.S. and German embassies in China’s capital of Beijing announced on Dec. 15 the suspension of routine visa services due to the city’s COVID-19 outbreak that is also being seen in other large cities in China, following dozens of countries who have already suspended their visa applications in China.
Meanwhile, concerns have been rising that the COVID-19 outbreak in Beijing will spread to the countryside during travel for the Chinese new year in January.
The recent outbreak started before the communist regime lifted its “zero-COVID” restrictions last month, the World Heath Organization’s (WHO) emergencies chief noted.
Foreign Embassies and Visa Centers Suspend Services in China
The U.S. Embassy in China announced on Dec. 15 on its website that due to the surge in COVID infections across China, all routine visa services have been suspended except for some pre-scheduled visa services in the Shanghai Consulate. All regular appointments at the Beijing embassy and other Consulates General have been cancelled. The offices said that only passport and emergency citizen and consular services would continue to be provided.
The German embassy in Beijing also announced that due to the epidemic situation in Beijing, its consular office and visa office will be closed until Jan. 6, 2023.
German ambassador to China Patricia Flor expressed concern about the medical capacity of mainland China on Dec. 15, “We don’t know, are there enough intensive care unit (ICU) beds?”
She warned, “Nobody is really prepared, mentally, for this situation. So we cannot be excluded. There will be further disruptions here.”
More than a dozen countries had already closed their visa centers in China in late November.
VFS Global, authorized by many countries’ governments to provide visa services in China, temporarily closed their visa centers for some countries in Beijing from Nov. 22 until further notice. Those countries include: Austria, Canada, Croatia, Czech Republic, Estonia, Finland, Greece, Hungary, Italy, Latvia, Poland, Portugal, Slovenia, Iceland, Norway, Sweden, Switzerland, Ukraine, and others.
Concerns for COVID-19 Spread as Holidays Near
The Chinese lunar New Year, the biggest holiday in China, falls on Jan. 22, 2023, and the Chinese countryside expects massive influxes of people returning home as well as tourists as the holiday approaches. However, rural China has had little exposure to the various strains of the COVID-19 virus in the past three years, prompting concerns about a large wave of infections and deaths.
China’s national health commission said on Dec. 16 that it was ramping up vaccinations and stocking up on ventilators, essential medicines, and testing kits in rural areas. It is also advising Chinese new year travelers to reduce their contact with elderly relatives.
According to mainland Chinese media, Henan Province, with a large population whose majority are in the countryside, has announced that it has entered the first level of preparations for a spike in COVID-19 cases. Authorities have cancelled holiday leave for all employees in the health system in the province from now until the end of March next year.
Infections Exploding Long Before ‘Zero-COVID’ Policy Dropped
Michael Ryan, the WHO emergencies chief, said at a press briefing on Dec. 14 that COVID-19 infections were exploding in China well before the Chinese regime abandoned its strict “zero-COVID” policy.
He said that there’s a false perception going around about China’s COVID-19 situation.
“There’s a narrative at the moment that China lifted the restrictions and all of a sudden the disease is out of control.”
He pointed out that the lifting of restriction in China is not the cause of the infection surge but a response to it, as it happened way before.
“The disease was spreading intensively because I believe the control measures in themselves were not stopping the disease,” he said. “And I believe China decided strategically that was not the best option anymore.”
Heliobas Disciple
TB Fanatic
A New Drug Could Fight Both COVID and Cancer
University of Southern California and the Cleveland Clinic Florida Research and Innovation Center researchers have published new research on GRP78, a protein implicated in both COVID-19 and numerous forms of cancer, as well as a new drug that interferes with its effects. While vaccination can pro
scitechdaily.com
A New Drug Could Fight Both COVID and Cancer
By Keck School of Medicine of USC
December 18, 2022
University of Southern California and the Cleveland Clinic Florida Research and Innovation Center researchers have published new research on GRP78, a protein implicated in both COVID-19 and numerous forms of cancer, as well as a new drug that interferes with its effects.
While vaccination can provide potentially life-saving protection against COVID-19, researchers are still looking for effective ways to treat severe infections, including in those who cannot get the vaccine or in the event that dangerous new virus strains emerge that could bypass vaccine protection.
A new study led by Amy S. Lee, Ph.D., professor of biochemistry and molecular medicine at the University of Southern California’s Keck School of Medicine, finds that GRP78, a chaperone protein involved in the spread of other viruses, plays a critical role in the spread of SARS-CoV-2, the virus that causes COVID-19. The research also demonstrates that SARS-CoV-2 replication was significantly decreased by preventing GRP78 production or by inhibiting it through the use of a new targeted drug.
According to the study, which was recently published in the journal Nature Communications, this drug may potentially offer a new type of protection against COVID-19, one that might remain effective even as new strains develop.
“A major problem in fighting SARS-CoV-2 is that it is constantly mutating and adapting itself to more efficiently infect and multiply in its host cells,” said Lee, also the Judy and Larry Freeman Chair in basic science research. “If we keep chasing the virus around, this could become quite challenging and unpredictable.”
GRP78’s role in the spread of viruses
In search of a more stable way to combat COVID-19, Lee and her colleagues at USC’s Keck School of Medicine and the Cleveland Clinic Florida Research and Innovation Center began investigating the role of GRP78, a key cellular chaperone protein that helps regulate the folding of other cellular proteins. While healthy cells need a fraction of GRP78 to function normally, cells under stress need more GRP78 to cope. The Keck School of Medicine researchers demonstrated in a 2021 study that when SARS-CoV-2 enters the scene, GRP78 is hijacked to operate in tandem with other cellular receptors to bring the SARS-CoV-2 virus into cells, where it can then multiply and spread.But questions remained about whether GRP78 is “necessary and essential” for SARS-CoV-2 replication inside human lung cells. Examining human lung epithelial cells infected with SARS-CoV-2, the research team observed that as the viral infection intensifies, the infected cells produce higher levels of GRP78.
The power of inhibiting GRP78
Then Lee and her team used a special messenger RNA tool to suppress the production of the GRP78 protein in human lung epithelial cells in cell culture, without interrupting other cellular processes. When those cells were later infected with SARS-CoV-2, they produced a lower amount of the viral spike protein and released much less of the virus to infect other cells, proving that GRP78 was necessary and essential for viral replication and production.“We now have direct evidence that GRP78 is a proviral protein that is essential for the virus to replicate,” Lee said.
To further explore whether targeting GRP78 could work to treat COVID-19, the researchers tested a recently identified small molecule drug, known as HA15 on the infected lung cells. This drug, developed for use against cancer cells, specifically binds GRP78 and inhibits its activity.
“Lo and behold, we found that this drug was very effective in reducing the number and size of SARS-CoV-2 plaques produced in the infected cells, in safe doses which had no harmful effect on normal cells,” Lee said.
The researchers then tested HA15 in the body of mice that were genetically engineered to express a human SARS-CoV-2 receptor and infected with SARS-CoV-2, finding that the drug greatly reduced viral load in the lungs.
Drugs that target GRP78
Separately, Lee and her colleagues at the Keck School of Medicine are studying the efficacy of HA15 in cancer, as well as another GRP78 inhibitor, YUM70, in collaboration with researchers at the University of Michigan. They discovered that HA15 and YUM70 can suppress the production of mutant KRAS proteins—a common mutation that tends to resist drug treatment—and reduce the viability of cancer cells bearing such mutations in pancreatic, lung, and colon cancer. Those findings, recently published in the journal Neoplasia, suggest targeting GRP78 may help combat these deadly cancers.These are basic proof of principle studies; further research, including clinical trials, is needed to establish that HA15 and YUM70 are safe and effective for use in humans. These and other GRP78 inhibitors are now being tested as treatments for both COVID-19 and cancer. These drugs may also prove useful for treating future coronaviruses that depend on GRP78 for entry and replication, Lee said.
References: “The stress-inducible ER chaperone GRP78/BiP is upregulated during SARS-CoV-2 infection and acts as a pro-viral protein” by Woo-Jin Shin, Dat P. Ha, Keigo Machida and Amy S. Lee, 14 November 2022, Nature Communications.
DOI: 10.1038/s41467-022-34065-3
“Targeting GRP78 suppresses oncogenic KRAS protein expression and reduces viability of cancer cells bearing various KRAS mutations” by Dat P. Ha, Bo Huang, Han Wang, Daisy Flores Rangel, Richard Van Krieken, Ze Liu, Soma Samanta, Nouri Neamati and Amy S. Lee, 24 September 2022, Neoplasia.
DOI: 10.1016/j.neo.2022.100837
The research was funded by the National Institutes of Health, the W. M. Keck Foundation, and the Korea Research Institute of Bioscience and Biotechnology.
This research is facilitated by USC’s Biosafety-Level 3 containment laboratory, allowing the team to safely study the SARS-CoV-2 infection in genetically engineered mice.
vector7
Dot Collector
I’m hoping that Elon did this poll as a honeypot to catch all the deep state bots. The dataset for this poll will contain most of them. Some good data-mining and he could kill them all in one go
RT 30secs
View: https://twitter.com/bennyjohnson/status/1604943195057840129?s=20&t=9VdgNT_ue9uRH2HWHYzaEA
RT 30secs
View: https://twitter.com/bennyjohnson/status/1604943195057840129?s=20&t=9VdgNT_ue9uRH2HWHYzaEA
Makes you wonder if there is a "racial component" to this bug as well as the at large general health of the Chinese mainland's population.....
Posted for fair use.....

 www.theedgemarkets.com
www.theedgemarkets.com
/
Bloomberg
December 19, 2022 19:42 pm +08
(Dec 19): Police and security guards were stationed outside a Beijing crematorium reportedly designated to handle Covid fatalities, as questions over China’s virus death toll mount.
Guards pushed journalists to the back of the Beijing Dongjiao Funeral Parlor’s parking lot on Monday, as a line of about a dozen black minivans entered the site on Beijing’s eastern outskirts, used to prepare and process bodies for cremation. The vans appeared to be dropping off bodies and were surrounded at one point by what seemed to be mourners or relatives.
The crematorium has drawn scrutiny after workers told foreign media including the Financial Times and the Wall Street Journal that they were overwhelmed with bodies since China scrapped most Covid restrictions and Beijing experienced a surge in cases. That contrasts with the official virus death count, which saw just two Covid fatalities recorded for Beijing this weekend, the first in almost a month.
Photographs taken earlier on Monday showed rows of cars — some adorned with ribbons often used in China to signify a vehicle is part of a funeral procession — entering Dongjiao, and employees in full PPE moving a coffin.
The crematorium has been designated to handle Covid-positive cases and has been working around the clock, with about 200 bodies arriving daily, from 30 to 40 on a typical day, an employee told the Journal on Friday. Meanwhile, staff told the FT that the bodies of at least 30 Covid victims were cremated on Wednesday, when no fatalities were recorded for all of China, let alone Beijing.
The disparity comes as China embarks on a complete pivot away from its stringent Covid Zero policy, which has been dragging on the economy all year and stoking popular unrest. After painting Covid as a lethal threat the population needed to be protected from for most of the pandemic, officials are now saying it’s not dangerous, with one top adviser saying Omicron could be likened to a “cold”.
The inevitable rise in deaths that comes from reopening doesn’t fit with that messaging, especially with some experts predicting almost one million fatalities from this coming wave alone.
Other countries that made a similar shift from containing Covid to living with it, like Singapore and New Zealand, saw much bigger increases in deaths when they reopened, and they had higher vaccination rates, especially among the elderly. China’s booster rate for those over 80 is just 40%.
Read also:
China reports first two Covid-19 deaths since easing rules, but numbers don’t stack up
Posted for fair use.....
Police guard Beijing crematorium as Covid-19 deaths questioned
(Dec 19): Police and security guards were stationed outside a Beijing crematorium reportedly designated to handle Covid fatalities, as questions over China’s virus death toll mount.Guards pushed journalists to the back of the Beijing Dongjiao Funeral Parlor’s parking lot on Monday, as a line of...
Police guard Beijing crematorium as Covid-19 deaths questioned
Bloomberg/
Bloomberg
December 19, 2022 19:42 pm +08
(Dec 19): Police and security guards were stationed outside a Beijing crematorium reportedly designated to handle Covid fatalities, as questions over China’s virus death toll mount.
Guards pushed journalists to the back of the Beijing Dongjiao Funeral Parlor’s parking lot on Monday, as a line of about a dozen black minivans entered the site on Beijing’s eastern outskirts, used to prepare and process bodies for cremation. The vans appeared to be dropping off bodies and were surrounded at one point by what seemed to be mourners or relatives.
The crematorium has drawn scrutiny after workers told foreign media including the Financial Times and the Wall Street Journal that they were overwhelmed with bodies since China scrapped most Covid restrictions and Beijing experienced a surge in cases. That contrasts with the official virus death count, which saw just two Covid fatalities recorded for Beijing this weekend, the first in almost a month.
Photographs taken earlier on Monday showed rows of cars — some adorned with ribbons often used in China to signify a vehicle is part of a funeral procession — entering Dongjiao, and employees in full PPE moving a coffin.
The crematorium has been designated to handle Covid-positive cases and has been working around the clock, with about 200 bodies arriving daily, from 30 to 40 on a typical day, an employee told the Journal on Friday. Meanwhile, staff told the FT that the bodies of at least 30 Covid victims were cremated on Wednesday, when no fatalities were recorded for all of China, let alone Beijing.
The disparity comes as China embarks on a complete pivot away from its stringent Covid Zero policy, which has been dragging on the economy all year and stoking popular unrest. After painting Covid as a lethal threat the population needed to be protected from for most of the pandemic, officials are now saying it’s not dangerous, with one top adviser saying Omicron could be likened to a “cold”.
The inevitable rise in deaths that comes from reopening doesn’t fit with that messaging, especially with some experts predicting almost one million fatalities from this coming wave alone.
Other countries that made a similar shift from containing Covid to living with it, like Singapore and New Zealand, saw much bigger increases in deaths when they reopened, and they had higher vaccination rates, especially among the elderly. China’s booster rate for those over 80 is just 40%.
Read also:
China reports first two Covid-19 deaths since easing rules, but numbers don’t stack up