
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
CORONA Main Coronavirus thread
- Thread starter Heliobas Disciple
- Start date
-
- Tags
- coronavirus
Heliobas Disciple
TB Fanatic
Here is the article referred to in that tweet:
New SARS-CoV-2 KP.2 variant defies vaccines with higher spread, study warns
Study on the bioRxiv server reports that the SARS-CoV-2 KP.2 variant, despite lower infectivity, shows significant immune resistance and higher transmissibility compared to other variants, potentially impacting global public health and vaccine efficacy.
 www.news-medical.net
www.news-medical.net
New SARS-CoV-2 KP.2 variant defies vaccines with higher spread, study warns
By Vijay Kumar Malesu - Reviewed by Susha Cheriyedath, M.Sc.
Apr 29 2024
In a recent preprint* study posted to the bioRxiv server, a team of researchers analyzed the virological characteristics and epidemiological impact of the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) FLiRT variant KP.2, which has demonstrated increased transmissibility and immune resistance.
Background
The rapid emergence and diversification of the JN.1 variant and its descendant, KP.2, which shows significant alterations in spike (S) protein structure and increased resistance to existing vaccines, underscore the necessity for further research to understand the implications for public health and vaccine development.
About the study
The present study was initiated by analyzing the genomic sequences of the KP.2 variant from surveillance data across the United States of America (USA), United Kingdom, and Canada, where over 30 sequences were reported. The relative effective reproduction number (Re) was calculated using a Bayesian multinomial logistic regression model, adjusting for various covariates that could influence transmission dynamics.
Subsequently, virological assays were conducted to evaluate the infectivity and immune evasion capabilities of KP.2. Lentivirus-based pseudovirus assays were performed using Human Osteosarcoma cells (HOS)- Angiotensin-Converting Enzyme 2 (ACE2)/Transmembrane Protease, Serine 2 (TMPRSS2) cells infected with pseudoviruses bearing the S proteins of KP.2, JN.1, and other relevant variants. The quantity of input virus was standardized against the Human Immunodeficiency Virus Type 1 (HIV-1) Protein 24 (p24) capsid protein. Statistical analysis was carried out using two-sided Student's t-tests to determine significant differences in infectivity between the variants.
For the neutralization assays, serum samples were collected from individuals in various immunization and infection states. These included vaccinated individuals both with and without prior infections and those who had recovered from specific variant infections. Each serum sample was tested in quadruplicate against pseudoviruses harboring different S protein mutations. The 50% neutralization titers (NT50) were calculated and compared across all serum samples to assess the degree of neutralization resistance posed by KP.2. Statistical significance of the differences in NT50 values was evaluated using two-sided Wilcoxon signed-rank tests.
Study results
The study revealed that the KP.2 variant, a descendant of the JN.1 lineage, demonstrates significantly enhanced epidemiological fitness compared to its predecessors, including the dominant XBB lineage. This finding is confirmed by the Re estimated for KP.2 in the USA, United Kingdom, and Canada, where it was observed to be 1.22, 1.32, and 1.26 times higher than JN.1, respectively. The spread of KP.2 has been rapid, with its variant frequency reaching 20% in the United Kingdom as of early April 2024, suggesting a potential to become the predominant lineage globally.
Further virological investigation into KP.2 using a lentivirus-based pseudovirus assay highlighted a paradox wherein, despite its higher transmissibility, the infectivity of KP.2 was found to be significantly lower (10.5-fold) than that of JN.1. This reduced infectivity might suggest different mechanisms or pathways for KP.2's enhanced spread and establishment in the host populations.
In addition to infectivity, resistance to neutralization was assessed through assays using sera from individuals vaccinated with the monovalent XBB.1.5 vaccine and those who had breakthrough infections with various SARS-CoV-2 variants. KP.2 exhibited significant resistance to neutralization, with a 3.1-fold reduction in susceptibility to neutralization by sera from vaccines without infection and a 1.8-fold reduction from those with prior infections. This increased resistance could partially explain the higher Re of KP.2, indicating an enhanced ability to evade immune responses compared to JN.1 and other previous variants.
Journal reference:
- Preliminary scientific report. Yu Kaku, Keiya Uriu, Yusuke Kosugi, et al. Virological characteristics of the SARS-CoV-2 KP.2 variant, bioRxiv (2024), doi: 10.1101/2024.04.24.590786, Virological characteristics of the SARS-CoV-2 KP.2 variant
*Important notice: bioRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
Heliobas Disciple
TB Fanatic

CDC: Hospitals No Longer Mandated to Report COVID-19 Data
The CDC says that hospitals no longer have to report COVID-19 hospital admissions, hospital capacity, or related information.
 www.theepochtimes.com
www.theepochtimes.com
CDC: Hospitals No Longer Mandated to Report COVID-19 Data
The CDC says that hospitals no longer have to report COVID-19 hospital admissions, hospital capacity, or related information.
By Jack Phillips
5/2/2024
Hospitals no longer have to report COVID-19 hospital admissions, hospital capacity, or related information to the U.S. Centers for Disease Control and Prevention (CDC), according to the agency.
The CDC said the change went into effect on May 1 and that the “data will be archived as of May 10, 2024, and available at United States COVID-19 Hospitalization Metrics by Jurisdiction, Timeseries,” according to its website.
The statement further said that it still encourages hospitals to engage in “voluntary reporting” of hospitalizations.
Officials have said they will use other data sources such as wastewater, laboratory tests, and emergency department information to report on the spread of COVID-19.
“A key lesson we learned from the COVID-19 pandemic is the importance of having reporting systems in place before an active emergency,” a CDC spokesperson told news outlets about the change. “These data have a significant and ongoing value for protecting patient health and safety as well as public health,” the statement added.
Since the COVID-19 pandemic was declared in March 2020, federal officials have been mandated to collect virus-related data from hospitals and states. The COVID-19 public health emergency officially expired in May 2023, but the hospital reporting was extended.
Meanwhile, CDC data shows that COVID-19 hospitalizations have appeared to hit a record low in the United States, years after virus spread to the United States in early 2020.
There were 5,615 COVID-19 hospitalizations in the most recent week where data is available, said the agency. There were more than 150,000 weekly admissions during the peak in January 2022, according to the agency’s historical data.
Reported COVID-19 deaths have also been on the decline this year, hitting new lows, according to the CDC’s tracking website. An estimated 231 deaths were confirmed in the most recent week of data that was made available.
It comes as the CDC again called on older Americans to receive another, updated dose of the COVID-19 vaccine. On April 25, the agency wrote in a report that people aged 65 and older “should receive an additional dose of the updated COVID-19 vaccine to enhance their immunity and decrease the risk for severe COVID-19-associated illness.”
The agency added that officials believe COVID-19 “remains an important public health threat, despite overall decreases in COVID-19-related severe disease since the start of the COVID-19 pandemic.” That’s because, according to the agency’s data, COVID-19-related hospitalizations were higher among adults aged 65 and older.
Several weeks ago, a survey released by the Pew Research Center found that 20 percent of Americans think COVID-19 is a “major threat to the health of the U.S. population,” while 10 percent are “very concerned they will get it and require hospitalization.”
“This data represents a low ebb of public concern about the virus that reached its height in the summer and fall of 2020, when as many as two-thirds of Americans viewed COVID-19 as a major threat to public health,” Pew’s article said.
Data from the CDC showed that about 22.6 percent of adults and 14 percent of children in the U.S. have received the latest vaccine. A larger number of Americans, meanwhile, have received the influenza vaccine in the past six months, as compared with the updated COVID-19 shot.
“Almost half of those who received a flu shot from a health care provider chose not to get the updated COVID-19 vaccine,” the report found.
The CDC in March changed its longstanding guidance that Americans who test positive for COVID-19 no longer need to stay in isolation for five days, saying that people can return to work or regular activities if their symptoms are mild and improving and it’s been a day since they’ve had a fever.
However, the CDC guidance for workers at nursing homes and other health care facilities is staying the same. That includes a recommendation that medical personnel stay home at least seven days after symptoms first appear, and that they test negative within two days of returning to work.
The CDC had originally advised 10 days of isolation, but in late 2021 cut it to five days for Americans who catch the virus and have no symptoms or only brief illnesses. Under that guidance for the general public, isolation only ended if a person had been fever-free for at least 24 hours without the use of fever-reducing medications and if other symptoms were resolving.
Heliobas Disciple
TB Fanatic

Moderna’s sales from its only product, the COVID-19 vaccine, fell 91% from last year
The drugmaker is optimistic about higher sales with new vaccines and a little help from AI in the coming years.
Moderna’s sales from its only product, the COVID-19 vaccine, fell 91% from last year
Sunny Nagpaul - FORTUNE
Thu, May 2, 2024, 5:21 PM EDT
The dark days of the pandemic are finally in the past for most of us—and that seems to be reflected in the earnings for Moderna, whose revenue is dependent on sales of its COVID-19 vaccine.
In the first quarter of the year, Moderna reported $167 million in sales of its only product on the market, its COVID-19 vaccine called Spikevax. The company’s first quarter revenue is down 91% from the $1.9 billion it reported in the same quarter last year.
The plummeting revenue makes sense, considering the demand for the vaccine has been dropping since 2021, but it’s not all bad news for the vaccine maker: Its revenue surpassed Wall Street’s expectation of $97.5 million, and in turn, shares of Moderna jumped 7% on Thursday. Near the end of April, the company also announced a new innovation to integrate AI and ChatGPT in its operations as part of an ongoing partnership with OpenAI since 2023, according to OpenAI’s press release, and also has plans to roll out a new RSV vaccine this fall.
Moderna's first quarter net loss of $1.18 billion was also stronger than Wall Street expectations of $1.4 billion in net losses, and the company now anticipates $4 billion in full-year sales.
In its first-quarter earnings report, the Massachusetts-based biopharmaceutical company said its sales decline “aligns with the anticipated transition to a seasonal COVID-19 vaccine market,” which makes the market for the vaccine similar to that of the flu shot, and said that its revenue sales in 2023 were bolstered primarily by “delivered doses deferred from 2022.”
It’s important to note that the vaccine maker, which employs about 5,100 people as of June 2023 and was founded in 2010, is in a very different category than some other pharmaceutical giants that made bank during the pandemic, like Pfizer, which was founded in 1849 and reported first-quarter sales of $14.88 billion; or Johnson and Johnson, which was founded in 1886 and posted $21.4 billion in first-quarter revenue.
One reason for Moderna’s low sales is because Americans aren’t getting booster vaccines as frequently in the last few years. According to the Centers for Disease Control and Prevention, as of the end of April this year, just over 22% of American adults reported getting an updated COVID-19 vaccine since mid-September. What’s more, about 28% of adults report receiving the most up-to-date vaccine, according to a Pew Research Center report, which also found that despite a public-health push encouraging adults to get both flu and COVID-19 vaccines at the same time, almost half of those who received a flu shot from a health care provider chose not to get the updated COVID-19 vaccine.
Moderna’s next focus is to continue rolling out mRNA vaccines, which teaches cells how to make the proteins that will trigger an immune response inside our bodies; up next will be its aforementioned RSV vaccine, and a seasonal flu vaccine. The company’s RSV vaccine entered the third of five clinical research phases the Food and Drug Administration requires of new medications, according to the earnings report, and expects initial regulatory approvals for the vaccine in the first half of this year, with the launch of the vaccine expected in fall 2024, just in time for cold-and-flu season.
With its OpenAI partnership, Moderna hopes to implement AI across its business, with a goal to bring 15 new products to market in the next five years, according to a statement by OpenAI. Those products could range from RSV vaccines to individualized cancer treatments, which will help diversify the company’s future revenue.
“This is the start of a banner year for our vaccine platform as we continue to advance mRNA medicines for patients,” Moderna CEO Stéphane Bancel said in the earnings call. “This is just the beginning.”
Heliobas Disciple
TB Fanatic

Long COVID symptoms in children can vary by age
Symptoms associated with Long COVID in children differ based on the child's age, according to a nationwide, multi-site study. The research will be presented at the Pediatric Academic Societies (PAS) 2024 Meeting, held May 2–6 in Toronto.
Long COVID symptoms in children can vary by age
by American Pediatric Society
May 3, 2024
Symptoms associated with Long COVID in children differ based on the child's age, according to a nationwide, multi-site study. The research will be presented at the Pediatric Academic Societies (PAS) 2024 Meeting, held May 2–6 in Toronto.
Experts say that the study findings allow clinicians to recognize and manage Long COVID in children more accurately based on common symptoms. The study characterized pediatric Long COVID symptoms and how they differ based on a child's age.
The study identifies symptoms in different age groups including young children, such as infants, toddlers, and preschool-age children (birth to five years); school-age children (6 to 11 years); adolescents (12 to 17 years); and young adults (18 to 25 years). Researchers compared prolonged symptoms in participants with and without a history of a COVID-19 infection to identify symptoms mostly highly linked with Long COVID.
According to the findings, school-age children, adolescents, and young adults with a history of a COVID-19 infection had many prolonged symptoms in common, including low energy; tiring after walking; headaches; body, muscle, and joint pains; lightheadedness or dizziness; trouble concentrating or focusing; and gastrointestinal symptoms, like nausea and vomiting.
Some symptoms varied by age with school-age children having more prolonged phobias or fears of specific things and school refusal, and adolescents having more fears of crowds or enclosed spaces and panic attacks compared to similarly aged children without a COVID-19 infection history.
Research showed that change in smell or taste was more commonly described by adolescents and young adults, and chest pain and palpitations were more common in young adults, but not in the younger age groups.
The study found that young children between birth and 5 years old with a prior COVID-19 infection were more likely to have general symptoms, including poor appetite, trouble sleeping, and fussiness, and prolonged respiratory symptoms like stuffy nose and cough, compared to young children without a known prior COVID-19 infection.
"These findings underscore the importance of characterizing Long COVID in children while researchers are still discovering the long-term effects of COVID-19 infection in this age group," said Rachel Gross, MD, MS, associate professor of pediatrics and population health at New York University Grossman School of Medicine and presenting author.
"This research is important because clinicians can appropriately diagnose and treat Long COVID when they better understand how different age groups are affected by the condition."
Researchers surveyed 7,229 caregivers and children enrolled in the National Institutes of Health's Researching COVID to Enhance Recovery (RECOVER)-Pediatrics study, 75% of whom had reported having had a COVID-19 infection.
More information: Abstract: Spectrum of Clinical Symptoms Identified as Long COVID from Infancy Through Young Adulthood: First Look Results from the NIH-Funded RECOVER (Researching COVID to Enhance Recovery) Initiative.
Provided by American Pediatric Society
Heliobas Disciple
TB Fanatic
AstraZeneca Admits Their COVID Vaccine Can Cause Clotting
Drbeen Medical Lectures
May 2, 2024
20 min 44 sec
UK's vaccine giant AstraZeneca has finally admitted in a court filing that their COVID-19 vaccine in very rare cases can cause thrombosis with thrombocytopenia syndrome (TTS). They still will not admit that they know the mechanism or will not entertain the usage of the term vaccine-induced immune thrombotic thrombocytopenia (VITT). Interestingly their own scientists participated in research about VITT with scientists from Cardiff University and Arizona State University. In this research scientists actually came back with a proposed mechanism of VITT. Let's review.
URL list from Thursday, May. 2 2024
AstraZeneca admits its Covid vaccine can cause rare side effect in court documents for first time
Scientists may have solved an important part of the mystery of ultra-rare blood clots linked to adenovirus COVID-19 vaccines - News - Cardiff University
Pathogenesis of vaccine-induced immune thrombotic thrombocytopenia (VITT) - PMC
Trigger of rare blood clots with COVID vaccines found - - Diamond Light Source
ChAdOx1 interacts with CAR and PF4 with implications for thrombosis with thrombocytopenia syndrome | Science Advances
Platelet factor 4 - Wikipedia
Heliobas Disciple
TB Fanatic

Bird flu virus circulated in cows for four months before outbreak confirmed by USDA, analysis shows
A USDA analysis shows the spread in cattle started from a single spillover event from birds in the Texas panhandle that may have happened in early December.
 www.statnews.com
www.statnews.com
Bird flu virus circulated in cows for four months before outbreak confirmed by USDA, analysis shows
By Megan Molteni
May 2, 2024
As agricultural authorities and epidemiologists try to get their arms around the scope of the latest confounding chapter in the decades-long story of the H5N1 avian influenza virus — its jump into U.S. herds of dairy cattle — they’re turning to the genetic breadcrumbs the virus leaves behind in the animals’ nose, lungs, and, primarily, milk.
On Wednesday, U.S. Department of Agriculture scientists released a preprint — a study that has not yet been peer-reviewed — describing for the first time what their investigations of 220 viral genomes from infected cows have so far turned up. The study’s authors suggest that the spread in cattle started from a single spillover event from birds in the Texas panhandle that may have happened in early December. The USDA didn’t confirm the presence of H5N1 in a Texas herd until March 25.
“These data support a single introduction event from wild bird origin virus into cattle, likely followed by limited local circulation for approximately 4 months prior to confirmation by USDA,” the authors wrote.
The findings add more precision to what had previously been reported by academic scientists. Reading viral genomes can provide clues to the origins of the outbreak and allows researchers to monitor how the virus, which primarily infects wild and farmed birds, is changing as it finds a foothold in bovine hosts.
In an initial analysis of USDA genome sequence data released last week, academic DNA sleuths had revealed that the outbreak in dairy cows has likely been going on for months longer than previously realized, and has probably spread more widely than official numbers would suggest. So far, the USDA has reported 36 herds in nine states have tested positive for the virus.
The new analysis also offers a window into how the bird flu is changing as it spends time in the bodies of cattle.
In the last few years, H5N1 has spread from wild birds to a variety of carnivorous mammals, including foxes, bears, and seals, but in each of those instances, the virus has hit a dead end. The outbreak in dairy cows represents one of the first times that this bird flu virus has demonstrated the ability to efficiently transmit between mammals, said Thomas Mettenleiter, a virologist who served as the director of the Friedrich Loeffler Institut — Germany’s leading animal disease research center — from 1996 until he stepped down last year. The other instance was a number of outbreaks at mink farms in Spain and Finland in 2022 and 2023, respectively.
“These spillover events don’t usually lead to transmission chains,” he said. “This situation is definitely an eye-opener for me.”
The USDA’s analysis found about two dozen mutations that have arisen in the H5N1 virus as it has circulated in dairy cattle that are known to make influenza viruses more deadly or more likely to be able to infect humans.
“It’s still really difficult to draw a risk map out of that, but there seems to be ongoing evolution,” Mettenleiter said. “This is not surprising but it’s good to know. All these mammal-to-mammal passages, as we would do experimentally, put an evolutionary pressure on the virus to mutate and this is what we see with the increase of these known mammalian adaptation markers.”
Vivien Dugan, director of the influenza division at the Centers for Disease Control and Prevention, told STAT Thursday that the mutations found so far did not raise any immediate red flags for increased risk to human health.
“I think based on our analysis of the consensus and some of that raw [sequence] data — because we have a good data-sharing relationship with USDA — we’ve not seen anything that would be concerning to us for mammalian adaptation, at this point,” Dugan said.
The CDC has been testing existing H5 vaccines in ferrets, and found that vaccination appears to offer cross-protection against the virus from the man who was infected in Texas.
Scientists who have been frustrated by the slow drip of data from the USDA’s investigations hailed the preprint on social media as progress. “Really grateful to this research team for sharing this, though I hope they weren’t holding on to the data solely to ensure they published first,” Angela Rasmussen, a virologist who studies pathogens that jump from animals to people at the Vaccine and Infectious Disease Organization at the University of Saskatchewan, in Saskatoon, Canada, posted on X on Thursday.
For weeks, the agency has been facing criticism from scientists and pandemic experts for a lack of transparency and timely sharing of data about the outbreak that has slowed down efforts to track its progress. When the USDA finally uploaded a large tranche of genetic sequences of the pathogen to a public database, researchers eager to analyze the sequences to determine if the H5N1 virus has been changing as it is transmitted from cow to cow quickly discovered that the sequences didn’t include necessary information about when and where the samples were collected. All are simply labeled with “USA” and “2024.”
The USDA has denied taking that basic information — called metadata — off the sequence files. The agency’s Animal and Plant Health Inspection Service has said it is sharing raw sequence data as quickly as it is available and plans to upload “consensus sequences,” which are more thoroughly edited and contain the metadata scientists are seeking, when they are ready.
Heliobas Disciple
TB Fanatic

Tracking bird flu virus changes in cows is stymied by missing data, scientists say
Scientists are frustrated that the USDA again failed to include basic information about H5N1 genetic sequences from cows when the data were released this week.
www.statnews.com
Tracking bird flu virus changes in cows is stymied by missing data, scientists say
By Helen Branswell
May 2, 2024
Another upload of genetic sequence data from the H5N1 bird flu outbreak in dairy cattle has exacerbated the scientific community’s frustration with the U.S. Department of Agriculture after the agency again failed to include basic information needed to track how the virus is changing as it spreads.
Like a large tranche of sequences that the USDA uploaded to a public database on April 21, this week’s data dump did not include information about where and when the sequenced samples were obtained from cows or other sequenced animals. All are simply labeled with “USA” and “2024.”
A key goal of monitoring genetic sequences in an outbreak is to track the evolution of a spreading virus, in this case to see if transmission among a new mammalian species is leading to changes that could make H5N1 more transmissible to and among people. Without the equivalent of a time stamp on the individual sequences, that’s much more difficult to do, scientists told STAT.
“We know what was happening a month ago, but we don’t know what’s happening now. Or it’s less clear what’s happening now,” said Thomas Peacock, an influenza virologist at the Pirbright Institute, a British organization that focuses on controlling viral illnesses in animals.
Cows in 36 herds in nine states are known to have tested positive for the virus. But it is widely believed the outbreak, which may have begun late last year, is more widespread than the number of confirmed outbreaks would suggest.
In fact, the USDA said as much in a preprint the agency posted on BioRxiv on Wednesday. The paper, which has not yet been peer reviewed, is based on an analysis of sequence data from the outbreak. The authors suggest the spillover event that started the spread in cattle may have happened in early December. The first detection that something was amiss with some cattle herds in the Texas panhandle dates to late January, but it took until March 25 before USDA confirmed the presence of H5N1 in a Texas herd.
In the paper, the authors say they have posted the sequence data they used online. A link in the article did not initially lead to a cache of data and to the supplementary materials — additional charts and figures that flesh out a paper — but that was later fixed.
In scientific publishing, researchers often try to hold on to their sequence data until they can get a paper published, for fear of being scooped by other scientists. But during public health emergencies, there is heavy pressure to share data as it becomes available, because to withhold it until publication can hamstring good decision making.
“Really grateful to this research team for sharing this, though I hope they weren’t holding on to the data solely to ensure they published first,” Angela Rasmussen, a virologist who studies emerging zoonotic pathogens — disease threats that jump from animals to humans — posted on Twitter on Thursday. Rasmussen, who is among those who have been frustrated at the USDA’s data sharing approach, works at the Vaccine and Infectious Disease Organization at the University of Saskatchewan, in Saskatoon, Canada.
Many of the 87 new sequences that were uploaded to the database of the National Center for Biotechnology Information — run by the National Institutes of Health’s National Library of Medicine — are from samples retrieved from poultry and wild birds, and may not pertain to the dairy cow outbreak. But 10 of the new viral sequences are from cattle, two more are from cats, and another is from a pigeon. These sequences are all believed to be part of the outbreak.
The fact that basic information — called metadata — isn’t being shared about the samples “hinders our efforts a lot,” said Gytis Dudas, a senior researcher in genomic epidemiology and metagenomics at the Vilnius University Life Sciences Center in Lithuania. Dudas is working with a group of U.S. and international researchers to try to make sense of what the genetic sequences say about the H5N1 outbreak in cows.
A number of scientists have openly questioned whether the USDA is deliberately withholding these data, or even removing more specific information.
“I can’t imagine that they’d be getting these samples, running the sequences, and not somehow recording that data for themselves, for what state it came from and what date it was sampled. That’s really extremely basic data,” said Rasmussen.
A USDA spokesman denied that the department is taking metadata off the sequence files before uploading them. In an email exchange with STAT, he said samples it receives contain only laboratory information numbers when they are sequenced. “Metadata is added by [Animal and Plant Health Inspection Service] staff after the sequencing occurs,” he said. “APHIS adds ‘USA’ and ‘2024’ as metadata tags and posts the sequences as they become available, in order to expedite public access to sequence data.”
The department has committed to sharing raw sequence data as quickly as it is available and has said it will upload what are called “consensus sequences” in an internationally used database, GISAID — the Global Initiative on Sharing All Influenza Data — when they are ready. Consensus sequences are more thoroughly edited and contain the metadata scientists are seeking.
It’s not just academic scientists who are seeking it, Peacock said, noting international public health agencies that are trying to assess the risk the U.S. outbreak poses are keen to get more data too. “They’re just being much more quiet about it. But you know they’re all requesting this and not getting it as well, as far as I’m aware.”
The USDA has only posted consensus sequences to GISAID from this outbreak once, in late March. It’s clear, though, that they have many more than they have shared to date. At an online symposium last week, Rosemary Sifford, the USDA’s chief veterinary officer, showed a phylogenetic tree featuring dozens of sequences, using the figure to explain that the department believes the outbreaks across the country are all linked and began from one spillover of the virus from wild birds to cows, likely in Texas.
A phylogenetic tree is like a family tree of a virus, showing how it is changing over time, but also providing a sense of when the virus spilled over from wild birds into cattle. The genetic sequence data available so far suggest that it occurred in late 2023 or early 2024.
The sequences featured in the phylogenetic tree in Sifford’s presentation would have been consensus sequences, Peacock said. “It does suggest they have them and they’re just not uploading them.”
The group of scientists Peacock, Dudas, and Rasmussen are part of quickly went through the sequences on the slide Sifford showed, harvesting from it the metadata the USDA has to date failed to provide. “That was less than ideal,” Dudas said.
psychgirl
Has No Life - Lives on TB
And again, this sounds all too familiar; weren’t there accusations of missing sequences for Covid in the very beginning, as well?(fair use applies)Tracking bird flu virus changes in cows is stymied by missing data, scientists say
Scientists are frustrated that the USDA again failed to include basic information about H5N1 genetic sequences from cows when the data were released this week.
Tracking bird flu virus changes in cows is stymied by missing data, scientists say
By Helen Branswell
May 2, 2024
Another upload of genetic sequence data from the H5N1 bird flu outbreak in dairy cattle has exacerbated the scientific community’s frustration with the U.S. Department of Agriculture after the agency again failed to include basic information needed to track how the virus is changing as it spreads.
Like a large tranche of sequences that the USDA uploaded to a public database on April 21, this week’s data dump did not include information about where and when the sequenced samples were obtained from cows or other sequenced animals. All are simply labeled with “USA” and “2024.”
A key goal of monitoring genetic sequences in an outbreak is to track the evolution of a spreading virus, in this case to see if transmission among a new mammalian species is leading to changes that could make H5N1 more transmissible to and among people. Without the equivalent of a time stamp on the individual sequences, that’s much more difficult to do, scientists told STAT.
“We know what was happening a month ago, but we don’t know what’s happening now. Or it’s less clear what’s happening now,” said Thomas Peacock, an influenza virologist at the Pirbright Institute, a British organization that focuses on controlling viral illnesses in animals.
Cows in 36 herds in nine states are known to have tested positive for the virus. But it is widely believed the outbreak, which may have begun late last year, is more widespread than the number of confirmed outbreaks would suggest.
In fact, the USDA said as much in a preprint the agency posted on BioRxiv on Wednesday. The paper, which has not yet been peer reviewed, is based on an analysis of sequence data from the outbreak. The authors suggest the spillover event that started the spread in cattle may have happened in early December. The first detection that something was amiss with some cattle herds in the Texas panhandle dates to late January, but it took until March 25 before USDA confirmed the presence of H5N1 in a Texas herd.
In the paper, the authors say they have posted the sequence data they used online. A link in the article did not initially lead to a cache of data and to the supplementary materials — additional charts and figures that flesh out a paper — but that was later fixed.
In scientific publishing, researchers often try to hold on to their sequence data until they can get a paper published, for fear of being scooped by other scientists. But during public health emergencies, there is heavy pressure to share data as it becomes available, because to withhold it until publication can hamstring good decision making.
“Really grateful to this research team for sharing this, though I hope they weren’t holding on to the data solely to ensure they published first,” Angela Rasmussen, a virologist who studies emerging zoonotic pathogens — disease threats that jump from animals to humans — posted on Twitter on Thursday. Rasmussen, who is among those who have been frustrated at the USDA’s data sharing approach, works at the Vaccine and Infectious Disease Organization at the University of Saskatchewan, in Saskatoon, Canada.
Many of the 87 new sequences that were uploaded to the database of the National Center for Biotechnology Information — run by the National Institutes of Health’s National Library of Medicine — are from samples retrieved from poultry and wild birds, and may not pertain to the dairy cow outbreak. But 10 of the new viral sequences are from cattle, two more are from cats, and another is from a pigeon. These sequences are all believed to be part of the outbreak.
The fact that basic information — called metadata — isn’t being shared about the samples “hinders our efforts a lot,” said Gytis Dudas, a senior researcher in genomic epidemiology and metagenomics at the Vilnius University Life Sciences Center in Lithuania. Dudas is working with a group of U.S. and international researchers to try to make sense of what the genetic sequences say about the H5N1 outbreak in cows.
A number of scientists have openly questioned whether the USDA is deliberately withholding these data, or even removing more specific information.
“I can’t imagine that they’d be getting these samples, running the sequences, and not somehow recording that data for themselves, for what state it came from and what date it was sampled. That’s really extremely basic data,” said Rasmussen.
A USDA spokesman denied that the department is taking metadata off the sequence files before uploading them. In an email exchange with STAT, he said samples it receives contain only laboratory information numbers when they are sequenced. “Metadata is added by [Animal and Plant Health Inspection Service] staff after the sequencing occurs,” he said. “APHIS adds ‘USA’ and ‘2024’ as metadata tags and posts the sequences as they become available, in order to expedite public access to sequence data.”
The department has committed to sharing raw sequence data as quickly as it is available and has said it will upload what are called “consensus sequences” in an internationally used database, GISAID — the Global Initiative on Sharing All Influenza Data — when they are ready. Consensus sequences are more thoroughly edited and contain the metadata scientists are seeking.
It’s not just academic scientists who are seeking it, Peacock said, noting international public health agencies that are trying to assess the risk the U.S. outbreak poses are keen to get more data too. “They’re just being much more quiet about it. But you know they’re all requesting this and not getting it as well, as far as I’m aware.”
The USDA has only posted consensus sequences to GISAID from this outbreak once, in late March. It’s clear, though, that they have many more than they have shared to date. At an online symposium last week, Rosemary Sifford, the USDA’s chief veterinary officer, showed a phylogenetic tree featuring dozens of sequences, using the figure to explain that the department believes the outbreaks across the country are all linked and began from one spillover of the virus from wild birds to cows, likely in Texas.
A phylogenetic tree is like a family tree of a virus, showing how it is changing over time, but also providing a sense of when the virus spilled over from wild birds into cattle. The genetic sequence data available so far suggest that it occurred in late 2023 or early 2024.
The sequences featured in the phylogenetic tree in Sifford’s presentation would have been consensus sequences, Peacock said. “It does suggest they have them and they’re just not uploading them.”
The group of scientists Peacock, Dudas, and Rasmussen are part of quickly went through the sequences on the slide Sifford showed, harvesting from it the metadata the USDA has to date failed to provide. “That was less than ideal,” Dudas said.
Heliobas Disciple
TB Fanatic
Well take it fwiw. But I'll post it FYI. Shots began in 2021.
View: https://twitter.com/toobaffled/status/1785815719848116277
Dolores Cahill was one of the doctors whose warnings influenced my decision on the vaccine. God bless her for speaking out when she did. She got into a lot of trouble in Ireland for doing so IIRC.
Here are links to the original articles/videos of her speaking about this in 2021. This isn't something new, it's a playback of past video. I haven't heard anything from her in a few years. I think she was succesfully silenced

Horrific Latent Deaths Predicted Among the Elderly by Genetics Professor After Immunization With RNA Vaccines - LewRockwell
PROFESSOR DOLORES CAHILL, PROFESSOR of TRANSLATIONAL RESEARCH (FORSCHUNG) AND MOLECULAR GENETICS, School of Medicine, University College Dublin, chairperson Irish Freedom Party, speaking at RENSE.com, predicts impending mass death from RNA vaccines (paraphrased): Professor Dolores Cahill...
 www.lewrockwell.com
www.lewrockwell.com
Horrific Latent Deaths Predicted Among The Elderly By Genetics Professor After Immunization With RNA Vaccines
By Bill Sardi
January 27, 2021
PROFESSOR DOLORES CAHILL, PROFESSOR of TRANSLATIONAL RESEARCH (FORSCHUNG) AND MOLECULAR GENETICS, School of Medicine, University College Dublin, chairperson Irish Freedom Party, speaking at RENSE.com, predicts impending mass death from RNA vaccines (paraphrased):
Professor Dolores Cahill, speaking about RNA vaccines
4 min 39 sec
“I suppose there are potentially three adverse reactions (from messenger RNA vaccines—MODERNA, PFIZER).
Beginning with anaphylaxis (severe, potentially life-threatening allergic reaction) in the first week. Therefore, these vaccines shouldn’t be given in the 2nd dose. Buy New $9.97 ($0.04 / Count) (as of 06:22 UTC - Details)
Then the real adverse events will happen, against whatever is the real mRNA in the vaccines, and when the person vaccinated comes across (this coronavirus) sometime later …. what happened in the animal studies, 20% or 50% or 100% of the animals died!
Among people over 80, maybe about 2.5% will experience severe side effects, adverse events where people cannot work or live life normally.
Then with the 2nd vaccination it could be 1 in 10 or ten percent. For the over 80-year-olds, I would think that 80% of them would have life-limiting reactions or die when they come across the messenger RNA again.
For others (not elderly) it could be half of the people who could be severely harmed.
What it does is… this gene therapy or medical device is setting up an autoimmune disease chronically. It’s like injecting people who have nut allergies with peanuts.
It’s anaphylaxis in the first wave. It’s anaphylaxis +allergic reaction the 2nd wave. But the 3rd reaction occurs when you come across whatever the messenger RNA is against (virus, bacterium, etc.), and now you have stimulated your immune system to have a low-grade autoimmune disease, not immunity to yourself per se because the mRNA is expressing a viral protein.
Now you made yourself a genetically modified organism, and so the immune system that is meant to push the viruses or bacteria out… now the autoimmune reaction is attacking your body low grade.
Now (months later) when you come across the virus that stimulates the immune system to get rid of the virus and when it (the immune system) sees that you have viral proteins in your own cells and organs, then about a week later (the adaptive immune system kicks in, the mechanism that makes specific long-term memory antibodies against a pathogen) and you go into organ failure. Because your immune system is killing your own organs. Those patients will present as sepsis initially. Then (later) you die of organ failure.
If you have one or two co-morbidities, the energy the immune system requires to boost your immune system will make the older person very tired and exhausted and they don’t have the capacity to survive if you have underlying conditions.
Normally, because the mRNA is in every cell of their body, it’s almost unstoppable. It destroys the heart, or the spleen, or the lungs, or the liver because the mRNA is expressing the protein in every cell.
Just as a solution, what we urgently need, just as a repository, 1 in 100, or 1 in 200 vaccine vials injected, to be set aside, especially into the elderly in the care homes. They need to be stored in a biorepository of the vaccine vials randomly, so when the people start to die, we can actually see what is in this vaccine. We should be doing this now.
I am concerned that there are maybe multiple mRNAs in this vaccine, not just something for coronavirus. If it is influenza or other viruses, we would be priming these people to other natural (cold and flu) viruses that are circulating.
We urgently need quality control to randomly require doctors to give 1 in 100 vaccine vials to a repository and someone like me could forensically analyze what’s in these vaccines. So, when the elderly start dying, we will know. We should be knowing now what’s in them.
It’s absolutely a dangerous gene therapy. Should not be given to the elderly,” emphasized professor Cahill.
The allergic reactions and deaths begin
Moderna, maker of the RNA COVID-19 vaccine, reports only 10 of 4 million vaccinees had an early (within 10 minutes of inoculation) allergic reaction. However, there is no data for 80+ year-olds with this vaccine, the group Dr. Cahill warns about, that typically have weak immune systems.
Now suddenly there are reports of a number of individuals at one vaccination center in California experiencing allergic reactions from an RNA-vaccine. While health authorities claim allergic reactions are rare, 10 patients are reported to have required medical attention for severe allergic reactions within 24-hours after vaccination at one site in California and six health care workers had allergic reactions at another vaccination center in San Diego in one day.
Hot lot withdrawn
Health officials withdrew one lot (41L20A) of the RNA vaccine. Inexplicably, health officials continue to offer false assurance it is “safe to use” the Moderna RNA vaccine when no conclusive safety data among large populations have been completed yet. No one knows if the Moderna RNA vaccine is safe. It is an unlicensed experimental vaccine. Remember, according to Professor Cahill, the really severe reactions will be latent – occur months later.
Then again, news agencies report of 33 deaths among 48,000+ people age 75 and over following immunization with the Pfizer COVID-19 RNA vaccine. Health officials continue to blame these deaths on the frailty of older subjects. But that is precisely the point – they may be too old and frail to benefit from vaccination.
RNA to DNA
The COVID-19 coronavirus is an RNA virus. The MODERNA COVID-19 vaccine is an RNA vaccine. Gene activation involves transcription of DNA into messenger RNA and then to gene-derived proteins.
Merle Nass MD, calls attention to the fact messenger RNA (or any RNA) can potentially be converted to DNA in the presence of the enzyme reverse transcriptase. That DNA could then become linked to your native DNA. There is the possibility of vaccine-RNA being converted to DNA and then permanently inserted into our DNA. (Resveratrol, a red wine molecule, by virtue of its ability to inhibit reverse transcriptase, could put a halt to this potential biogenetic hazard.)
It would be wise for people undergoing any vaccination to supplement their diet with vitamins A and D, zinc and resveratrol which normalize the immune response, especially individuals that have experienced allergic reactions or are allergy prone.
AND

Professor Dolores Cahill: People Will Start Dying After COVID Vaccine | Principia Scientific Intl.
Dolores Cahill Dolores Cahill, a professor at University College Dublin and recognised international expert in this field, predicts deaths will occur around the world as a direct consequence of taking the COVID-19 vaccines. In her latest video interview the influential professor, Dolores Cahill...
 principia-scientific.com
principia-scientific.com
Professor Dolores Cahill: People Will Start Dying After COVID Vaccine
by John O'Sullivan
January 5, 2021
Dolores Cahill Dolores Cahill, a professor at University College Dublin and recognised international expert in this field, predicts deaths will occur around the world as a direct consequence of taking the COVID-19 vaccines.
In her latest video interview the influential professor, Dolores Cahill, makes this grim prediction based on what is known already about the vaccines, their rushed development and the entirely novel approach using mRNA instead of conventional antibodies.
As with almost every leading expert who speaks out against the official pandemic narrative Professor Cahill has suffered professional and personal retaliation. In her case Professor Cahill was forced to resign her position as vice chair of the Scientific Committee of the Innovative Medicines Initiative (IMI), a partnership between the European Commission and the drugs industry to promote new drugs.

Professor Dolores Cahill: Why People Will Start DYING A Few Months After The First mRNA Vaccination
⚠️MORE UP TO DATE CONTENT HERE⚠️: https://odysee.com/$/invite/@SixthSense-Truth-Search-Labs:0 ⚠️What is in the so-calledCOVID-19 “Vaccines”? Part 1: Evidence of a Global Crime Against Humanity:⚠️ https://ijvtpr.com/index.php/IJVTPR/article/view/52…
Embarrassed by Cahill’s outspoken whistleblowing the European Commission denounced her claims declaring she, could cause “significant harm”, if taken seriously.
Zoner
Veteran Member
A voice in the wilderness. Thx HDDolores Cahill was one of the doctors whose warnings influenced my decision on the vaccine. God bless her for speaking out when she did. She got into a lot of trouble in Ireland for doing so IIRC.
Here are links to the original articles/videos of her speaking about this in 2021. This isn't something new, it's a playback of past video. I haven't heard anything from her in a few years. I think she was succesfully silenced
(fair use applies)Horrific Latent Deaths Predicted Among the Elderly by Genetics Professor After Immunization With RNA Vaccines - LewRockwell
PROFESSOR DOLORES CAHILL, PROFESSOR of TRANSLATIONAL RESEARCH (FORSCHUNG) AND MOLECULAR GENETICS, School of Medicine, University College Dublin, chairperson Irish Freedom Party, speaking at RENSE.com, predicts impending mass death from RNA vaccines (paraphrased): Professor Dolores Cahill...
Horrific Latent Deaths Predicted Among The Elderly By Genetics Professor After Immunization With RNA Vaccines
By Bill Sardi
January 27, 2021
PROFESSOR DOLORES CAHILL, PROFESSOR of TRANSLATIONAL RESEARCH (FORSCHUNG) AND MOLECULAR GENETICS, School of Medicine, University College Dublin, chairperson Irish Freedom Party, speaking at RENSE.com, predicts impending mass death from RNA vaccines (paraphrased):
Professor Dolores Cahill, speaking about RNA vaccines
4 min 39 sec
“I suppose there are potentially three adverse reactions (from messenger RNA vaccines—MODERNA, PFIZER).
Beginning with anaphylaxis (severe, potentially life-threatening allergic reaction) in the first week. Therefore, these vaccines shouldn’t be given in the 2nd dose. Buy New $9.97 ($0.04 / Count) (as of 06:22 UTC - Details)
Then the real adverse events will happen, against whatever is the real mRNA in the vaccines, and when the person vaccinated comes across (this coronavirus) sometime later …. what happened in the animal studies, 20% or 50% or 100% of the animals died!
Among people over 80, maybe about 2.5% will experience severe side effects, adverse events where people cannot work or live life normally.
Then with the 2nd vaccination it could be 1 in 10 or ten percent. For the over 80-year-olds, I would think that 80% of them would have life-limiting reactions or die when they come across the messenger RNA again.
For others (not elderly) it could be half of the people who could be severely harmed.
What it does is… this gene therapy or medical device is setting up an autoimmune disease chronically. It’s like injecting people who have nut allergies with peanuts.
It’s anaphylaxis in the first wave. It’s anaphylaxis +allergic reaction the 2nd wave. But the 3rd reaction occurs when you come across whatever the messenger RNA is against (virus, bacterium, etc.), and now you have stimulated your immune system to have a low-grade autoimmune disease, not immunity to yourself per se because the mRNA is expressing a viral protein.
Now you made yourself a genetically modified organism, and so the immune system that is meant to push the viruses or bacteria out… now the autoimmune reaction is attacking your body low grade.
Now (months later) when you come across the virus that stimulates the immune system to get rid of the virus and when it (the immune system) sees that you have viral proteins in your own cells and organs, then about a week later (the adaptive immune system kicks in, the mechanism that makes specific long-term memory antibodies against a pathogen) and you go into organ failure. Because your immune system is killing your own organs. Those patients will present as sepsis initially. Then (later) you die of organ failure.
If you have one or two co-morbidities, the energy the immune system requires to boost your immune system will make the older person very tired and exhausted and they don’t have the capacity to survive if you have underlying conditions.
Normally, because the mRNA is in every cell of their body, it’s almost unstoppable. It destroys the heart, or the spleen, or the lungs, or the liver because the mRNA is expressing the protein in every cell.
Just as a solution, what we urgently need, just as a repository, 1 in 100, or 1 in 200 vaccine vials injected, to be set aside, especially into the elderly in the care homes. They need to be stored in a biorepository of the vaccine vials randomly, so when the people start to die, we can actually see what is in this vaccine. We should be doing this now.
I am concerned that there are maybe multiple mRNAs in this vaccine, not just something for coronavirus. If it is influenza or other viruses, we would be priming these people to other natural (cold and flu) viruses that are circulating.
We urgently need quality control to randomly require doctors to give 1 in 100 vaccine vials to a repository and someone like me could forensically analyze what’s in these vaccines. So, when the elderly start dying, we will know. We should be knowing now what’s in them.
It’s absolutely a dangerous gene therapy. Should not be given to the elderly,” emphasized professor Cahill.
The allergic reactions and deaths begin
Moderna, maker of the RNA COVID-19 vaccine, reports only 10 of 4 million vaccinees had an early (within 10 minutes of inoculation) allergic reaction. However, there is no data for 80+ year-olds with this vaccine, the group Dr. Cahill warns about, that typically have weak immune systems.
Now suddenly there are reports of a number of individuals at one vaccination center in California experiencing allergic reactions from an RNA-vaccine. While health authorities claim allergic reactions are rare, 10 patients are reported to have required medical attention for severe allergic reactions within 24-hours after vaccination at one site in California and six health care workers had allergic reactions at another vaccination center in San Diego in one day.
Hot lot withdrawn
Health officials withdrew one lot (41L20A) of the RNA vaccine. Inexplicably, health officials continue to offer false assurance it is “safe to use” the Moderna RNA vaccine when no conclusive safety data among large populations have been completed yet. No one knows if the Moderna RNA vaccine is safe. It is an unlicensed experimental vaccine. Remember, according to Professor Cahill, the really severe reactions will be latent – occur months later.
Then again, news agencies report of 33 deaths among 48,000+ people age 75 and over following immunization with the Pfizer COVID-19 RNA vaccine. Health officials continue to blame these deaths on the frailty of older subjects. But that is precisely the point – they may be too old and frail to benefit from vaccination.
RNA to DNA
The COVID-19 coronavirus is an RNA virus. The MODERNA COVID-19 vaccine is an RNA vaccine. Gene activation involves transcription of DNA into messenger RNA and then to gene-derived proteins.
Merle Nass MD, calls attention to the fact messenger RNA (or any RNA) can potentially be converted to DNA in the presence of the enzyme reverse transcriptase. That DNA could then become linked to your native DNA. There is the possibility of vaccine-RNA being converted to DNA and then permanently inserted into our DNA. (Resveratrol, a red wine molecule, by virtue of its ability to inhibit reverse transcriptase, could put a halt to this potential biogenetic hazard.)
It would be wise for people undergoing any vaccination to supplement their diet with vitamins A and D, zinc and resveratrol which normalize the immune response, especially individuals that have experienced allergic reactions or are allergy prone.
AND
(fair use applies)Professor Dolores Cahill: People Will Start Dying After COVID Vaccine | Principia Scientific Intl.
Dolores Cahill Dolores Cahill, a professor at University College Dublin and recognised international expert in this field, predicts deaths will occur around the world as a direct consequence of taking the COVID-19 vaccines. In her latest video interview the influential professor, Dolores Cahill...
Professor Dolores Cahill: People Will Start Dying After COVID Vaccine
by John O'Sullivan
January 5, 2021
Dolores Cahill Dolores Cahill, a professor at University College Dublin and recognised international expert in this field, predicts deaths will occur around the world as a direct consequence of taking the COVID-19 vaccines.
In her latest video interview the influential professor, Dolores Cahill, makes this grim prediction based on what is known already about the vaccines, their rushed development and the entirely novel approach using mRNA instead of conventional antibodies.
As with almost every leading expert who speaks out against the official pandemic narrative Professor Cahill has suffered professional and personal retaliation. In her case Professor Cahill was forced to resign her position as vice chair of the Scientific Committee of the Innovative Medicines Initiative (IMI), a partnership between the European Commission and the drugs industry to promote new drugs.
12 min 37 secProfessor Dolores Cahill: Why People Will Start DYING A Few Months After The First mRNA Vaccination
⚠️MORE UP TO DATE CONTENT HERE⚠️: https://odysee.com/$/invite/@SixthSense-Truth-Search-Labs:0 ⚠️What is in the so-calledCOVID-19 “Vaccines”? Part 1: Evidence of a Global Crime Against Humanity:⚠️ https://ijvtpr.com/index.php/IJVTPR/article/view/52…www.bitchute.com
Embarrassed by Cahill’s outspoken whistleblowing the European Commission denounced her claims declaring she, could cause “significant harm”, if taken seriously.
Zoner
Veteran Member
When "pandemics are declared" - what does this mean in practice?
Beware of any "freedom fighter" who supports the government's power to declare pandemics. They are they are fighting freedom and defending the tyranny.

Sasha Latypova
May 03, 2024
Historically, epidemics could only be recognized AFTER the fact: after a substantial number of people became ill, died and after a significant economic impact. Examples of real epidemics include mostly water-born, crowding/poor sanitation and vermin-related diseases such as cholera, plague, typhus and smallpox. All of these diseases are eliminated by proper sanitation of water, hygiene and improvement in living conditions.
It is not possible to predict an epidemic, unless one purposefully takes measures to poison water or cause significant deterioration of people’s living standards.
In the clown-infested reality that we currently inhabit, the international government-military blob is claiming that they can predict pandemics and declare emergencies based on one fake PCR case of a made-up virus somewhere in the world.
In 2022 Attorneys General of 15 states sued HHS trying to repeal the HHS’ definitions of “public health emergency”. They raised the following concerns:
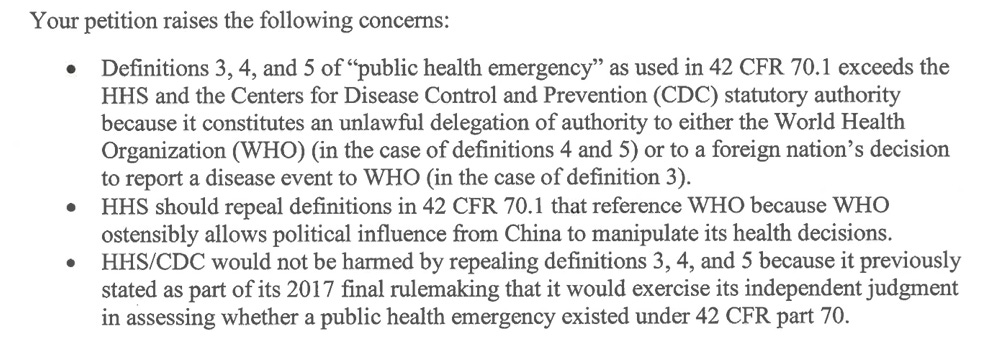
HHS refused to amend its definitions of a pandemic and insisted that they can claim absolutely anything is a pandemic.
HHS ultimately prevailed, the case was re-filed by OK and TX, the judge dismissed it and it was not appealed.
In the refusal to amend its definition of a pandemic, HHS stated that “any communicable disease event” - this means a single case of anything they claim “communicable” anywhere in the world (for example, a single cow that “tested positive” for “avian flu”), once announced by the WHO, can qualify for forced testing, tracing, detention and injections of humans or animals in any town or village in any state of the US!

Respiratory seasonal illness is endemic of course, so using these definitions the world can be permanently in a health emergency.
Salivating over the final solution, ahem, potential of permanent tyranny, the regime has created a permanent office within the Executive Branch - Office of Pandemic Preparedness and Response (OPPR).
Here is the Executive Order from April 12, 2024:
Initial and current OPPR Director is Retired Maj. Gen. Paul Friedrichs.OPPR created in March 2023, in response to section 2104 of Dec. 2022 Congressional act, PL 117-328 (Consolidated Appropriations Act), as permanent office in the Executive Office of the President (EOP) charged with leading, coordinating, and implementing actions related to preparedness for, and response to, known and unknown biological threats or pathogens that could lead to a pandemic or to significant public health-related disruptions in the United States.
While OPPR is “leading, implementing and coordinating” the HHS Secretary bestows himself with the power to decide which groups of people he can imprison without any real cause in what location. To do this, he only needs to “reasonably” identify these people as being in “pre-communicable stage of a communicable disease”!
I am not making this up. I wish I were. This simply says you can be thrown into the quarantine camp by HHS on their belief that you may have common cold. Potentially. Some day.

The HHS is also saying that they are not delegating authority to the WHO… that’s good, right? Freedom! Sovereignty! Yippeee! Oh wait…

…but rather, the WHO’s definitions and pronouncements are only “one way” to initiate the medical fascism. Not to worry. The HHS has several other ways in its arsenal!
I think this is highly relevant to the impending WHO/IHR global takeover, because these measures will be enforced by the federal/state/local governments, and of course will be used to imprison people without due process. Because they already exercised this power in 2020.
I found this statement from HHS in their argument against the 2022 petition for rule-making from 15 AGs. They described how they detained over 3000 people and held them at several DOD facilities (translation: arrested them on false pretenses without due process). Approximately 1100 were those repatriated from Wuhan as well as passengers from Diamond Princess, arriving internationally. However, an additional 2000 people from Grand Princess were already in the US (off CA coast).

History for both cruise ships from CDC can be found here.
There were 800 fake-PCRed “covid cases” and 10 quite real deaths among the combined 3100 detainees. Did the deaths occur in the military detention facilities? Were these people pumped full of remdesivir and fentanyl, designated as “covid deaths”, bodies promptly disposed off while the family paid and threatened to keep silent? You bet.
Does ANY of this require WHO pandemic treaty and IHR sign-off and ratification?
NO, silly!!!
All of this is already firmly enshrined in the US federal and practically all states’ public health laws. In early 2020, the regime (figure-headed by Trump at the time) ran several tests: Diamond Princess for international arrivals and Grand Princess for domestic to make sure they test the procedure and create the legal precedent.
Do you think a vague designation as a “pre-communicable stage” of “potentially pandemic illness” is NOT going to be abused to throw anyone inconvenient to the regime into a DOD prison? Then murder them and call it “Disease X”? Same methods are typically used by communists to round up the masses targeted for extermination.
Here is a sample of quarantine order by HHS (this is for foreign arrivals).
I am writing this for our collective preparedness to future tyranny under pretenses of public health.
Many of my subscribers are attorneys. If you have any advice on how to resist this lawfully, please post in comments.
My own advice is the following:
- Do not take cruise ship vacations. Even in the best of times they are floating prisons with great food (the captain is your warden);
- Do not test with PCR tests for anything. They are all fake methods to target you as “pre-communicable”;
- Find out if your community sewage system is under CDC’s surveillance for “viruses” (about 40% of US is);
- Talk to your neighbors, county commissioner, sheriff to find out where they stand on this. Mass awareness is a deterrent;
- If any quarantine orders are issued to you or your community, take photos, videos, post on social media, be vocal;
- Take names of any CDC or other agents trying to test, trace or otherwise designate you as a disease vector. Do not let them touch you or examine you as this may be a method to introduce toxic substances to make you sick.
- Just as with any attempt at detaining you, ask them if you are under arrest, and what are you charged with, do not volunteer any information, insist on having your attorney present;
- Do not travel to the secondary crime scene (quarantine detention center) that’s never a good idea, as you maybe murdered there and labeled a “Disease X death”;
- Realize that they cannot prove you have any illness, unless you cooperate, and historically CDC was only able to order quarantine if someone came from a location designated as epidemic outbreak. Use your brain and good judgement
"Pandemics are declared" - what does this mean in practice?
Beware of any "freedom fighter" who supports the government's power to declare pandemics. They are they are in fact fighting freedom and defending the tyranny.
Last edited:
jward
passin' thru
Common diabetes drug lowers SARS-CoV-2 levels, clinical trial finds
Stephanie Soucheray, MA
Today, researchers from the University of Minnesota published evidence that the common diabetes drug metformin decreases the amount of SARS-CoV-2 in the body and helps reduce the risk of rebound symptoms if given early in the course of non-severe illness.
The study, published in Clinical Infectious Diseases, suggests metformin may also help prevent long COVID.
The researchers tested metformin against a placebo in 999 adults infected with COVID-19. More than 50% of the study enrollees were vaccinated, and treatment took place when the Omicron variant was the most dominant strain in the United States.
Study included those at standard-risk
Moreover, according to Carolyn Bramante, MD, principal investigator of the study and an assistant professor at the University of Minnesota, the study participants represented a standard- risk population, a group that currently lacks effective treatment options for the novel coronavirus.
"This is not a high-risk population," Bramante told CIDRAP News. Instead, participants were 30 years or older, had a body mass index of 25 or higher (overweight), and did not require hospitalization for their COVID-19 infection.
In several trials, Paxlovid has been shown to prevent deaths and hospitalization in high-risk, unvaccinated people, but standard-risk populations have not shown improvement in either time to resolution of symptoms or the incidence of hospitalization or death.
Bramante said that these patient population demographics suggest metformin may be a clinical tool in outpatient medication that could be widely used.
"The data would be justified in prescribing it outpatient medication that works," she said.
Four-fold reduction in viral load by day 10
Participants were given a 14-day course of metformin, and participants collected nasal swabs on days 1, 5, and 10. Bramante said early treatment was key: Participants were enrolled within 3 days of a positive test, and if symptomatic, reported having symptoms for 7 or fewer days.
The mean SARS-CoV-2 viral load was reduced 3.6-fold with metformin relative to placebo by day 10, the authors found, and those who received metformin were less likely to have a detectable viral load than placebo at days 5 or 10 (odds ratio [OR], 0.72; 95% confidence interval [CI], 0.55 to 0.94).
Metformin reduced the odds of hospitalization or death through 28 days by 58%; emergency department visits, hospitalizations, and death through 14 days by 42%; and long COVID through 10 months by 42%.
Viral rebound, defined as a higher viral load at day 10 than day 5, was less frequent with metformin (3.28%) than placebo (5.95%; OR, 0.68; 95% CI, 0.36 to 1.29).
While the mechanism of action is not known, Bramante said metformin likely lowers inflammation and inhibits translation of the virus.
This study makes a strong case for a potential effect of metformin on COVID-19 virologic decay.
In a commentary on the study, the authors write, "This study makes a strong case for a potential effect of metformin on COVID-19 virologic decay and prompts reevaluation of existing data in support of its use."

 www.cidrap.umn.edu
www.cidrap.umn.edu
Stephanie Soucheray, MA
Today, researchers from the University of Minnesota published evidence that the common diabetes drug metformin decreases the amount of SARS-CoV-2 in the body and helps reduce the risk of rebound symptoms if given early in the course of non-severe illness.
The study, published in Clinical Infectious Diseases, suggests metformin may also help prevent long COVID.
The researchers tested metformin against a placebo in 999 adults infected with COVID-19. More than 50% of the study enrollees were vaccinated, and treatment took place when the Omicron variant was the most dominant strain in the United States.
Study included those at standard-risk
Moreover, according to Carolyn Bramante, MD, principal investigator of the study and an assistant professor at the University of Minnesota, the study participants represented a standard- risk population, a group that currently lacks effective treatment options for the novel coronavirus.
"This is not a high-risk population," Bramante told CIDRAP News. Instead, participants were 30 years or older, had a body mass index of 25 or higher (overweight), and did not require hospitalization for their COVID-19 infection.
In several trials, Paxlovid has been shown to prevent deaths and hospitalization in high-risk, unvaccinated people, but standard-risk populations have not shown improvement in either time to resolution of symptoms or the incidence of hospitalization or death.
Bramante said that these patient population demographics suggest metformin may be a clinical tool in outpatient medication that could be widely used.
"The data would be justified in prescribing it outpatient medication that works," she said.
Four-fold reduction in viral load by day 10
Participants were given a 14-day course of metformin, and participants collected nasal swabs on days 1, 5, and 10. Bramante said early treatment was key: Participants were enrolled within 3 days of a positive test, and if symptomatic, reported having symptoms for 7 or fewer days.
The mean SARS-CoV-2 viral load was reduced 3.6-fold with metformin relative to placebo by day 10, the authors found, and those who received metformin were less likely to have a detectable viral load than placebo at days 5 or 10 (odds ratio [OR], 0.72; 95% confidence interval [CI], 0.55 to 0.94).
Metformin reduced the odds of hospitalization or death through 28 days by 58%; emergency department visits, hospitalizations, and death through 14 days by 42%; and long COVID through 10 months by 42%.
Viral rebound, defined as a higher viral load at day 10 than day 5, was less frequent with metformin (3.28%) than placebo (5.95%; OR, 0.68; 95% CI, 0.36 to 1.29).
While the mechanism of action is not known, Bramante said metformin likely lowers inflammation and inhibits translation of the virus.
This study makes a strong case for a potential effect of metformin on COVID-19 virologic decay.
In a commentary on the study, the authors write, "This study makes a strong case for a potential effect of metformin on COVID-19 virologic decay and prompts reevaluation of existing data in support of its use."
Common diabetes drug lowers SARS-CoV-2 levels, clinical trial finds
jward
passin' thru
LEGAL - All Republican senators (49), have formally urged President Joe Biden to withdraw support in expanding the WHO pandemic authority.
The Vigilant Fox @VigilantFox US Senators Drop a Bombshell on the World Health Organization The tide is turning. In a shocking turn of events, all Republican senators (49), led by Senator Ron Johnson, have formally urged President Joe Biden to withdraw his support in expanding the World...
psychgirl
Has No Life - Lives on TB
I’m tired from working 11 hrs and not making the connection, most likely; but….diabetes IS a comorbidity for serious Covid infections.Common diabetes drug lowers SARS-CoV-2 levels, clinical trial finds
Stephanie Soucheray, MA
Today, researchers from the University of Minnesota published evidence that the common diabetes drug metformin decreases the amount of SARS-CoV-2 in the body and helps reduce the risk of rebound symptoms if given early in the course of non-severe illness.
The study, published in Clinical Infectious Diseases, suggests metformin may also help prevent long COVID.
The researchers tested metformin against a placebo in 999 adults infected with COVID-19. More than 50% of the study enrollees were vaccinated, and treatment took place when the Omicron variant was the most dominant strain in the United States.
Study included those at standard-risk
Moreover, according to Carolyn Bramante, MD, principal investigator of the study and an assistant professor at the University of Minnesota, the study participants represented a standard- risk population, a group that currently lacks effective treatment options for the novel coronavirus.
"This is not a high-risk population," Bramante told CIDRAP News. Instead, participants were 30 years or older, had a body mass index of 25 or higher (overweight), and did not require hospitalization for their COVID-19 infection.
In several trials, Paxlovid has been shown to prevent deaths and hospitalization in high-risk, unvaccinated people, but standard-risk populations have not shown improvement in either time to resolution of symptoms or the incidence of hospitalization or death.
Bramante said that these patient population demographics suggest metformin may be a clinical tool in outpatient medication that could be widely used.
"The data would be justified in prescribing it outpatient medication that works," she said.
Four-fold reduction in viral load by day 10
Participants were given a 14-day course of metformin, and participants collected nasal swabs on days 1, 5, and 10. Bramante said early treatment was key: Participants were enrolled within 3 days of a positive test, and if symptomatic, reported having symptoms for 7 or fewer days.
The mean SARS-CoV-2 viral load was reduced 3.6-fold with metformin relative to placebo by day 10, the authors found, and those who received metformin were less likely to have a detectable viral load than placebo at days 5 or 10 (odds ratio [OR], 0.72; 95% confidence interval [CI], 0.55 to 0.94).
Metformin reduced the odds of hospitalization or death through 28 days by 58%; emergency department visits, hospitalizations, and death through 14 days by 42%; and long COVID through 10 months by 42%.
Viral rebound, defined as a higher viral load at day 10 than day 5, was less frequent with metformin (3.28%) than placebo (5.95%; OR, 0.68; 95% CI, 0.36 to 1.29).
While the mechanism of action is not known, Bramante said metformin likely lowers inflammation and inhibits translation of the virus.
This study makes a strong case for a potential effect of metformin on COVID-19 virologic decay.
In a commentary on the study, the authors write, "This study makes a strong case for a potential effect of metformin on COVID-19 virologic decay and prompts reevaluation of existing data in support of its use."
Common diabetes drug lowers SARS-CoV-2 levels, clinical trial finds
So…,doesn’t it make sense then that many diabetics already ARE on metformin, therefore they should not be at risk?
Help me with this one here
Heliobas Disciple
TB Fanatic
This article is an analysis by the reporter about the next article, which they also wrote. I posted them in the wrong order. So read the next post first, then come back to read this. The 3rd post after this is a video on the subject.

 news.yahoo.com
(fair use applies)
news.yahoo.com
(fair use applies)
COVID Vaccine Side Effects: 4 Takeaways From Our Investigation
Apoorva Mandavilli - New York Times
Fri, May 3, 2024, 1:53 PM EDT
Soon after their arrival in late December 2020, the COVID-19 vaccines turned the pandemic around and opened a path back to normalcy. They prevented about 14.4 million deaths worldwide, according to one estimate.
In a small percentage of people, they also produced side effects.
Over the course of more than a year, The New York Times talked to 30 people who said they had been harmed by COVID vaccines. Their symptoms may turn out to be unrelated to the shots. But they — along with more than a dozen experts — felt federal officials are not doing enough to investigate their complaints.
All vaccines carry some risk of side effects. More than 270 million Americans received about 677 million doses of the COVID vaccines, and even rare side effects — occurring, say, in just 0.001% of patients — might mean thousands of recipients were affected.
Indeed, more than 13,000 have submitted claims to a government fund that compensates people for COVID vaccine injuries. So far, however, only a dozen people have been compensated, nearly all of them for a heart problem caused by the vaccines.
Here are four takeaways from our investigation.
For most people, the benefits of COVID vaccines outweigh any risks.
Even the best vaccines and drugs have some side effects. That does not negate their benefits, nor does it suggest that people should stop taking them.
The rotavirus vaccine, for example, is an unmitigated success, but it can lead to intussusception — a life-threatening condition in which the intestine folds in on itself — in about 0.02% of children who are vaccinated.
Some side effects caused by the COVID vaccines may be equally rare. Researchers in Hong Kong analyzed that area’s health records and found that about 7 of every 1 million doses of Pfizer-BioNTech vaccine triggered a bout of shingles serious enough to require hospitalization.
Other side effects are slightly more common. The COVID vaccines may lead to myocarditis, or inflammation of the heart, in 1 of every 10,000 adolescent males. (Myocarditis is one of the four serious side effects acknowledged by federal health officials.)
Deaths from the vaccines are vanishingly rare, despite claims from some conspiracy theorists that vaccines have led to a spike in mortality rates.
More intensive analysis may indicate that in some groups, like young men, the benefit of COVID shots may no longer outweigh the risks. But for the majority of Americans, the vaccines continue to be far safer than contracting COVID itself.
Federal surveillance has found some side effects but may miss others.
To detect problems with vaccines, federal agencies rely on multiple databases. The largest, the Vaccine Adverse Event Reporting System, is useful for generating hypotheses but contains unverified accounts of harms. Other databases combine electronic health records and insurance claims.
These systems spotted blood-clotting problems associated with the Johnson & Johnson vaccine and a potential risk of stroke after mRNA immunizations, which is still under investigation. But federal researchers trailed Israeli scientists in picking up myocarditis as a problem among young men.
The U.S. health care system is fragmented, with medical records stored by multiple companies that do not collaborate. Electronic health records do not all describe symptoms the same way, making comparisons difficult. Insurance claims databases may have no record of shots administered at mass vaccination sites.
Federal systems may also miss symptoms that defy easy description or diagnosis.
Proving vaccination led to an illness is complicated.
Among the hundreds of millions of Americans who were immunized against COVID, there were deaths, heart attacks, strokes, miscarriages and autoimmune illnesses. How to distinguish illnesses caused by the vaccine from those that would have happened anyway?
The rarer the condition, the harder it is to answer this question.
Merely judging by the timing — the appearance of a particular problem after vaccination — can be misleading. Most famously, childhood vaccines were mistakenly linked to autism because the first noticeable features often coincided with the immunization schedule.
Serious side effects may first turn up in animal studies of vaccines. But few such studies were possible, given the nation’s desperate timeline in 2020. Clinical trials of the vaccines were intended to test their effectiveness, but they were far from big enough to detect side effects that may occur only in a few people per million doses.
Most independent studies of side effects have not been large enough to detect rare events, nor to exclude their possibility; others have looked only for a preset list of symptoms and might have missed the rare outliers.
An expert panel convened by the National Academies concluded in April that for most side effects, there was not enough data to accept or reject a link to COVID vaccination.
Understanding the full range of side effects may take years.
Federal health officials acknowledge four major side effects of COVID vaccines — not including the temporary injection site pain, fever and malaise that may accompany the shots.
But in federal databases, thousands of Americans have reported that COVID vaccines caused ringing in the ears, dizziness, brain fog, sharp fluctuations in blood pressure and heart rate, new or relapsed autoimmune conditions, hives, vision problems, kidney disorders, tingling, numbness and a loss of motor skills.
Some studies have examined reports of side effects and largely concluded that there was no link. Closer scrutiny may reveal that many, perhaps most, of the other reported side effects are unrelated to immunization. Most of them are also associated with COVID and may be the result of undiagnosed infections. But without in-depth studies, it is impossible to be sure, experts said.
COVID Vaccine Side Effects: 4 Takeaways From Our Investigation
Soon after their arrival in late December 2020, the COVID-19 vaccines turned the pandemic around and opened a path back to normalcy. They prevented about 14.4 million deaths worldwide, according to one estimate. In a small percentage of people, they also produced side effects. Over the course of...
COVID Vaccine Side Effects: 4 Takeaways From Our Investigation
Apoorva Mandavilli - New York Times
Fri, May 3, 2024, 1:53 PM EDT
Soon after their arrival in late December 2020, the COVID-19 vaccines turned the pandemic around and opened a path back to normalcy. They prevented about 14.4 million deaths worldwide, according to one estimate.
In a small percentage of people, they also produced side effects.
Over the course of more than a year, The New York Times talked to 30 people who said they had been harmed by COVID vaccines. Their symptoms may turn out to be unrelated to the shots. But they — along with more than a dozen experts — felt federal officials are not doing enough to investigate their complaints.
All vaccines carry some risk of side effects. More than 270 million Americans received about 677 million doses of the COVID vaccines, and even rare side effects — occurring, say, in just 0.001% of patients — might mean thousands of recipients were affected.
Indeed, more than 13,000 have submitted claims to a government fund that compensates people for COVID vaccine injuries. So far, however, only a dozen people have been compensated, nearly all of them for a heart problem caused by the vaccines.
Here are four takeaways from our investigation.
For most people, the benefits of COVID vaccines outweigh any risks.
Even the best vaccines and drugs have some side effects. That does not negate their benefits, nor does it suggest that people should stop taking them.
The rotavirus vaccine, for example, is an unmitigated success, but it can lead to intussusception — a life-threatening condition in which the intestine folds in on itself — in about 0.02% of children who are vaccinated.
Some side effects caused by the COVID vaccines may be equally rare. Researchers in Hong Kong analyzed that area’s health records and found that about 7 of every 1 million doses of Pfizer-BioNTech vaccine triggered a bout of shingles serious enough to require hospitalization.
Other side effects are slightly more common. The COVID vaccines may lead to myocarditis, or inflammation of the heart, in 1 of every 10,000 adolescent males. (Myocarditis is one of the four serious side effects acknowledged by federal health officials.)
Deaths from the vaccines are vanishingly rare, despite claims from some conspiracy theorists that vaccines have led to a spike in mortality rates.
More intensive analysis may indicate that in some groups, like young men, the benefit of COVID shots may no longer outweigh the risks. But for the majority of Americans, the vaccines continue to be far safer than contracting COVID itself.
Federal surveillance has found some side effects but may miss others.
To detect problems with vaccines, federal agencies rely on multiple databases. The largest, the Vaccine Adverse Event Reporting System, is useful for generating hypotheses but contains unverified accounts of harms. Other databases combine electronic health records and insurance claims.
These systems spotted blood-clotting problems associated with the Johnson & Johnson vaccine and a potential risk of stroke after mRNA immunizations, which is still under investigation. But federal researchers trailed Israeli scientists in picking up myocarditis as a problem among young men.
The U.S. health care system is fragmented, with medical records stored by multiple companies that do not collaborate. Electronic health records do not all describe symptoms the same way, making comparisons difficult. Insurance claims databases may have no record of shots administered at mass vaccination sites.
Federal systems may also miss symptoms that defy easy description or diagnosis.
Proving vaccination led to an illness is complicated.
Among the hundreds of millions of Americans who were immunized against COVID, there were deaths, heart attacks, strokes, miscarriages and autoimmune illnesses. How to distinguish illnesses caused by the vaccine from those that would have happened anyway?
The rarer the condition, the harder it is to answer this question.
Merely judging by the timing — the appearance of a particular problem after vaccination — can be misleading. Most famously, childhood vaccines were mistakenly linked to autism because the first noticeable features often coincided with the immunization schedule.
Serious side effects may first turn up in animal studies of vaccines. But few such studies were possible, given the nation’s desperate timeline in 2020. Clinical trials of the vaccines were intended to test their effectiveness, but they were far from big enough to detect side effects that may occur only in a few people per million doses.
Most independent studies of side effects have not been large enough to detect rare events, nor to exclude their possibility; others have looked only for a preset list of symptoms and might have missed the rare outliers.
An expert panel convened by the National Academies concluded in April that for most side effects, there was not enough data to accept or reject a link to COVID vaccination.
Understanding the full range of side effects may take years.
Federal health officials acknowledge four major side effects of COVID vaccines — not including the temporary injection site pain, fever and malaise that may accompany the shots.
But in federal databases, thousands of Americans have reported that COVID vaccines caused ringing in the ears, dizziness, brain fog, sharp fluctuations in blood pressure and heart rate, new or relapsed autoimmune conditions, hives, vision problems, kidney disorders, tingling, numbness and a loss of motor skills.
Some studies have examined reports of side effects and largely concluded that there was no link. Closer scrutiny may reveal that many, perhaps most, of the other reported side effects are unrelated to immunization. Most of them are also associated with COVID and may be the result of undiagnosed infections. But without in-depth studies, it is impossible to be sure, experts said.
Last edited:
Heliobas Disciple
TB Fanatic
(fair use applies)
Thousands Believe Covid Vaccines Harmed Them. Is Anyone Listening?
All vaccines have at least occasional side effects. But people who say they were injured by Covid vaccines believe their cases have been ignored.
By Apoorva Mandavilli - New York Times
Within minutes of getting the Johnson & Johnson Covid-19 vaccine, Michelle Zimmerman felt pain racing from her left arm up to her ear and down to her fingertips. Within days, she was unbearably sensitive to light and struggled to remember simple facts.
She was 37, with a Ph.D. in neuroscience, and until then could ride her bicycle 20 miles, teach a dance class and give a lecture on artificial intelligence, all in the same day. Now, more than three years later, she lives with her parents.
Eventually diagnosed with brain damage, she cannot work, drive or even stand for long periods of time.
“When I let myself think about the devastation of what this has done to my life, and how much I’ve lost, sometimes it feels even too hard to comprehend,” said Dr. Zimmerman, who believes her injury is due to a contaminated vaccine batch.
The Covid vaccines, a triumph of science and public health, are estimated to have prevented millions of hospitalizations and deaths. Yet even the best vaccines produce rare but serious side effects. And the Covid vaccines have been given to more than 270 million people in the United States, in nearly 677 million doses.
Dr. Zimmerman’s account is among the more harrowing, but thousands of Americans believe they suffered serious side effects following Covid vaccination. As of April, just over 13,000 vaccine-injury compensation claims have been filed with the federal government — but to little avail. Only 19 percent have been reviewed. Only 47 of those were deemed eligible for compensation, and only 12 have been paid out, at an average of about $3,600.
Some scientists fear that patients with real injuries are being denied help and believe that more needs to be done to clarify the possible risks.
“At least long Covid has been somewhat recognized,” said Akiko Iwasaki, an immunologist and vaccine expert at Yale University. But people who say they have post-vaccination injuries are “just completely ignored and dismissed and gaslighted,” she added.
In interviews and email exchanges conducted over several months, federal health officials insisted that serious side effects were extremely rare and that their surveillance efforts were more than sufficient to detect patterns of adverse events.
“Hundreds of millions of people in the United States have safely received Covid vaccines under the most intense safety monitoring in U.S. history,” Jeff Nesbit, a spokesman for the Department of Health and Human Services, said in an emailed statement.
But in a recent interview, Dr. Janet Woodcock, a longtime leader of the Food and Drug Administration, who retired in February, said she believed that some recipients had experienced uncommon but “serious” and “life-changing” reactions beyond those described by federal agencies.
“I feel bad for those people,” said Dr. Woodcock, who became the F.D.A.’s acting commissioner in January 2021 as the vaccines were rolling out. “I believe their suffering should be acknowledged, that they have real problems, and they should be taken seriously.”
“I’m disappointed in myself,” she added. “I did a lot of things I feel very good about, but this is one of the few things I feel I just didn’t bring it home.”
Federal officials and independent scientists face a number of challenges in identifying potential vaccine side effects.
The nation’s fragmented health care system complicates detection of very rare side effects, a process that depends on an analysis of huge amounts of data. That’s a difficult task when a patient may be tested for Covid at Walgreens, get vaccinated at CVS, go to a local clinic for minor ailments and seek care at a hospital for serious conditions. Each place may rely on different health record systems.
There is no central repository of vaccine recipients, nor of medical records, and no easy to way to pool these data. Reports to the largest federal database of so-called adverse events can be made by anyone, about anything. It’s not even clear what officials should be looking for.
“I mean, you’re not going to find ‘brain fog’ in the medical record or claims data, and so then you’re not going to find” a signal that it may be linked to vaccination, Dr. Woodcock said. If such a side effect is not acknowledged by federal officials, “it’s because it doesn’t have a good research definition,” she added. “It isn’t, like, malevolence on their part.”
The government’s understaffed compensation fund has paid so little because it officially recognizes few side effects for Covid vaccines. And vaccine supporters, including federal officials, worry that even a whisper of possible side effects feeds into misinformation spread by a vitriolic anti-vaccine movement.
‘I’m Not Real’
Patients who believe they experienced serious side effects say they have received little support or acknowledgment.
Shaun Barcavage, 54, a nurse practitioner in New York City who has worked on clinical trials for H.I.V. and Covid, said that ever since his first Covid shot, merely standing up sent his heart racing — a symptom suggestive of postural orthostatic tachycardia syndrome, a neurological disorder that some studies have linked to both Covid and, much less often, vaccination.
He also experienced stinging pain in his eyes, mouth and genitals, which has abated, and tinnitus, which has not.
“I can’t get the government to help me,” Mr. Barcavage said of his fruitless pleas to federal agencies and elected representatives. “I am told I’m not real. I’m told I’m rare. I’m told I’m coincidence.”
Renee France, 49, a physical therapist in Seattle, developed Bell’s palsy — a form of facial paralysis, usually temporary — and a dramatic rash that neatly bisected her face. Bell’s palsy is a known side effect of other vaccines, and it has been linked to Covid vaccination in some studies.
But Ms. France said doctors were dismissive of any connection to the Covid vaccines. The rash, a bout of shingles, debilitated her for three weeks, so Ms. France reported it to federal databases twice.
“I thought for sure someone would reach out, but no one ever did,” she said.
Similar sentiments were echoed in interviews, conducted over more than a year, with 30 people who said they had been harmed by Covid shots. They described a variety of symptoms following vaccination, some neurological, some autoimmune, some cardiovascular.
All said they had been turned away by physicians, told their symptoms were psychosomatic, or labeled anti-vaccine by family and friends — despite the fact that they supported vaccines.
Even leading experts in vaccine science have run up against disbelief and ambivalence.
Dr. Gregory Poland, 68, editor in chief of the journal Vaccine, said that a loud whooshing sound in his ears had accompanied every moment since his first shot, but that his entreaties to colleagues at the Centers for Disease Control and Prevention to explore the phenomenon, tinnitus, had led nowhere.
He received polite responses to his many emails, but “I just don’t get any sense of movement,” he said.
“If they have done studies, those studies should be published,” Dr. Poland added. In despair that he might “never hear silence again,” he has sought solace in meditation and his religious faith.
Dr. Buddy Creech, 50, who led several Covid vaccine trials at Vanderbilt University, said his tinnitus and racing heart lasted about a week after each shot. “It’s very similar to what I experienced during acute Covid, back in March of 2020,” Dr. Creech said.
Research may ultimately find that most reported side effects are unrelated to the vaccine, he acknowledged. Many can be caused by Covid itself.
“Regardless, when our patients experience a side effect that may or may not be related to the vaccine, we owe it to them to investigate that as completely as we can,” Dr. Creech said.
Federal health officials say they do not believe that the Covid vaccines caused the illnesses described by patients like Mr. Barcavage, Dr. Zimmerman and Ms. France. The vaccines may cause transient reactions, such as swelling, fatigue and fever, according to the C.D.C., but the agency has documented only four serious but rare side effects.
Two are associated with the Johnson & Johnson vaccine, which is no longer available in the United States: Guillain-Barré syndrome, a known side effect of other vaccines, including the flu shot; and a blood-clotting disorder.
The C.D.C. also links mRNA vaccines made by Pfizer-BioNTech and Moderna to heart inflammation, or myocarditis, especially in boys and young men. And the agency warns of anaphylaxis, or severe allergic reaction, which can occur after any vaccination.
Listening for Signals
Agency scientists are monitoring large databases containing medical information on millions of Americans for patterns that might suggest a hitherto unknown side effect of vaccination, said Dr. Demetre Daskalakis, director of the C.D.C.’s National Center for Immunization and Respiratory Diseases.
“We toe the line by reporting the signals that we think are real signals and reporting them as soon as we identify them as signals,” he said. The agency’s systems for monitoring vaccine safety are “pretty close” to ideal, he said.
Those national surveillance efforts include the Vaccine Adverse Event Reporting System (VAERS). It is the largest database, but also the least reliable: Reports of side effects can be submitted by anyone and are not vetted, so they may be subject to bias or manipulation.
The system contains roughly one million reports regarding Covid vaccination, the vast majority for mild events, according to the C.D.C.
Federal researchers also comb through databases that combine electronic health records and insurance claims on tens of millions of Americans. The scientists monitor the data for 23 conditions that may occur following Covid vaccination. Officials remain alert to others that may pop up, Dr. Daskalakis said.
But there are gaps, some experts noted. The Covid shots administered at mass vaccination sites were not recorded in insurance claims databases, for example, and medical records in the United States are not centralized.
“It’s harder to see signals when you have so many people, and things are happening in different parts of the country, and they’re not all collected in the same system,” said Rebecca Chandler, a vaccine safety expert at the Coalition for Epidemic Preparedness Innovations.
An expert panel convened by the National Academies concluded in April that for the vast majority of side effects, there was not enough data to accept or reject a link.
Asked at a recent congressional hearing whether the nation’s vaccine-safety surveillance was sufficient, Dr. Peter Marks, director of the F.D.A.’s Center for Biologics Evaluation and Research, said, “I do believe we could do better.”
A Red Flag
In some countries with centralized health care systems, officials have actively sought out reports of serious side effects of Covid vaccines and reached conclusions that U.S. health authorities have not.
In Hong Kong, the government analyzed centralized medical records of patients after vaccination and paid people to come forward with problems. The strategy identified “a lot of mild cases that other countries would not otherwise pick up,” said Ian Wong, a researcher at the University of Hong Kong who led the nation’s vaccine safety efforts.
That included the finding that in rare instances — about seven per million doses — the Pfizer-BioNTech vaccine triggered a bout of shingles serious enough to require hospitalization.
The European Medicines Agency has linked the Pfizer and Moderna vaccines to facial paralysis, tingling sensations and numbness. The E.M.A. also counts tinnitus as a side effect of the Johnson & Johnson vaccine, although the American health agencies do not. There are more than 17,000 reports of tinnitus following Covid vaccination in VAERS.
Are the two linked? It’s not clear. As many as one in four adults has some form of tinnitus. Stress, anxiety, grief and aging can lead to the condition, as can infections like Covid itself and the flu.
There is no test or scan for tinnitus, and scientists cannot easily study it because the inner ear is tiny, delicate and encased in bone, said Dr. Konstantina Stankovic, an otolaryngologist at Stanford University.
Still, an analysis of health records from nearly 2.6 million people in the United States found that about 0.04 percent, or about 1,000, were diagnosed with tinnitus within three weeks of their first mRNA shot. In March, researchers in Australia published a study linking tinnitus and vertigo to the vaccines.
The F.D.A. is monitoring reports of tinnitus, but “at this time, the available evidence does not suggest a causal association with the Covid-19 vaccines,” the agency said in a statement.
Despite surveillance efforts, U.S. officials were not the first to identify a significant Covid vaccine side effect: myocarditis in young people receiving mRNA vaccines. It was Israeli authorities who first raised the alarm in April 2021. Officials in the United States said at the time that they had not seen a link.
On May 22, 2021, news broke that the C.D.C. was investigating a “relatively few” cases of myocarditis. By June 23, the number of myocarditis reports in VAERS had risen to more than 1,200 — a hint that it is important to tell doctors and patients what to look for.
Later analyses showed that the risk for myocarditis and pericarditis, a related condition, is highest after a second dose of an mRNA Covid vaccine in adolescent males aged 12 to 17 years.
In many people, vaccine-related myocarditis is transient. But some patients continue to experience pain, breathlessness and depression, and some show persistent changes on heart scans. The C.D.C. has said there were no confirmed deaths related to myocarditis, but in fact there have been several accounts of deaths reported post-vaccination.
Pervasive Misinformation
The rise of the anti-vaccine movement has made it difficult for scientists, in and out of government, to candidly address potential side effects, some experts said. Much of the narrative on the purported dangers of Covid vaccines is patently false, or at least exaggerated, cooked up by savvy anti-vaccine campaigns.
Questions about Covid vaccine safety are core to Robert F. Kennedy Jr.’s presidential campaign. Citing debunked theories about altered DNA, Florida’s surgeon general has called for a halt to Covid vaccination in the state.
“The sheer nature of misinformation, the scale of misinformation, is staggering, and anything will be twisted to make it seem like it’s not just a devastating side effect but proof of a massive cover-up,” said Dr. Joshua Sharfstein, a vice dean at Johns Hopkins University.
Among the hundreds of millions of Americans who were immunized for Covid, some number would have had heart attacks or strokes anyway. Some women would have miscarried. How to distinguish those caused by the vaccine from those that are coincidences? The only way to resolve the question is intense research.
But the National Institutes of Health is conducting virtually no studies on Covid vaccine safety, several experts noted. William Murphy, a cancer researcher who worked at the N.I.H. for 12 years, has been prodding federal health officials to initiate these studies since 2021.
The officials each responded with “that very tired mantra: ‘But the virus is worse,’” Dr. Murphy recalled. “Yes, the virus is worse, but that doesn’t obviate doing research to make sure that there may be other options.”
A deeper understanding of possible side effects, and who is at risk for them, could have implications for the design of future vaccines, or may indicate that for some young and healthy people, the benefit of Covid shots may no longer outweigh the risks — as some European countries have determined.
Thorough research might also speed assistance to thousands of Americans who say they were injured.
The federal government has long run the National Vaccine Injury Compensation Program, designed to compensate people who suffer injuries after vaccination. Established more than three decades ago, the program sets no limit on the amounts awarded to people found to have been harmed.
But Covid vaccines are not covered by that fund because Congress has not made them subject to the excise tax that pays for it. Some lawmakers have introduced bills to make the change.
Instead, claims regarding Covid vaccines go to the Countermeasures Injury Compensation Program. Intended for public health emergencies, this program has narrow criteria to pay out and sets a limit of $50,000, with stringent standards of proof.
It requires applicants to prove within a year of the injury that it was “the direct result” of getting the Covid vaccine, based on “compelling, reliable, valid, medical, and scientific evidence.”
The program had only four staff members at the beginning of the pandemic, and now has 35 people evaluating claims. Still, it has reviewed only a fraction of the 13,000 claims filed, and has paid out only a dozen.
Ilka Warshawsky, a 58-year-old pathologist, said she lost all hearing in her right ear after a Covid booster shot. But hearing loss is not a recognized side effect of Covid vaccination.
The compensation program for Covid vaccines sets a high bar for proof, she said, yet offers little information on how to meet it: “These adverse events can be debilitating and life-altering, and so it’s very upsetting that they’re not acknowledged or addressed.”
Dr. Zimmerman, the neuroscientist, submitted her application in October 2021 and provided dozens of supporting medical documents. She received a claim number only in January 2023.
In adjudicating her claim for workers’ compensation, Washington State officials accepted that Covid vaccination caused her injury, but she has yet to get a decision from the federal program.
One of her therapists recently told her she might never be able to live independently again.
“That felt like a devastating blow,” Dr. Zimmerman said. “But I’m trying not to lose hope there will someday be a treatment and a way to cover it.”
Thousands Believe Covid Vaccines Harmed Them. Is Anyone Listening?
All vaccines have at least occasional side effects. But people who say they were injured by Covid vaccines believe their cases have been ignored.
By Apoorva Mandavilli - New York Times
Within minutes of getting the Johnson & Johnson Covid-19 vaccine, Michelle Zimmerman felt pain racing from her left arm up to her ear and down to her fingertips. Within days, she was unbearably sensitive to light and struggled to remember simple facts.
She was 37, with a Ph.D. in neuroscience, and until then could ride her bicycle 20 miles, teach a dance class and give a lecture on artificial intelligence, all in the same day. Now, more than three years later, she lives with her parents.
Eventually diagnosed with brain damage, she cannot work, drive or even stand for long periods of time.
“When I let myself think about the devastation of what this has done to my life, and how much I’ve lost, sometimes it feels even too hard to comprehend,” said Dr. Zimmerman, who believes her injury is due to a contaminated vaccine batch.
The Covid vaccines, a triumph of science and public health, are estimated to have prevented millions of hospitalizations and deaths. Yet even the best vaccines produce rare but serious side effects. And the Covid vaccines have been given to more than 270 million people in the United States, in nearly 677 million doses.
Dr. Zimmerman’s account is among the more harrowing, but thousands of Americans believe they suffered serious side effects following Covid vaccination. As of April, just over 13,000 vaccine-injury compensation claims have been filed with the federal government — but to little avail. Only 19 percent have been reviewed. Only 47 of those were deemed eligible for compensation, and only 12 have been paid out, at an average of about $3,600.
Some scientists fear that patients with real injuries are being denied help and believe that more needs to be done to clarify the possible risks.
“At least long Covid has been somewhat recognized,” said Akiko Iwasaki, an immunologist and vaccine expert at Yale University. But people who say they have post-vaccination injuries are “just completely ignored and dismissed and gaslighted,” she added.
In interviews and email exchanges conducted over several months, federal health officials insisted that serious side effects were extremely rare and that their surveillance efforts were more than sufficient to detect patterns of adverse events.
“Hundreds of millions of people in the United States have safely received Covid vaccines under the most intense safety monitoring in U.S. history,” Jeff Nesbit, a spokesman for the Department of Health and Human Services, said in an emailed statement.
But in a recent interview, Dr. Janet Woodcock, a longtime leader of the Food and Drug Administration, who retired in February, said she believed that some recipients had experienced uncommon but “serious” and “life-changing” reactions beyond those described by federal agencies.
“I feel bad for those people,” said Dr. Woodcock, who became the F.D.A.’s acting commissioner in January 2021 as the vaccines were rolling out. “I believe their suffering should be acknowledged, that they have real problems, and they should be taken seriously.”
“I’m disappointed in myself,” she added. “I did a lot of things I feel very good about, but this is one of the few things I feel I just didn’t bring it home.”
Federal officials and independent scientists face a number of challenges in identifying potential vaccine side effects.
The nation’s fragmented health care system complicates detection of very rare side effects, a process that depends on an analysis of huge amounts of data. That’s a difficult task when a patient may be tested for Covid at Walgreens, get vaccinated at CVS, go to a local clinic for minor ailments and seek care at a hospital for serious conditions. Each place may rely on different health record systems.
There is no central repository of vaccine recipients, nor of medical records, and no easy to way to pool these data. Reports to the largest federal database of so-called adverse events can be made by anyone, about anything. It’s not even clear what officials should be looking for.
“I mean, you’re not going to find ‘brain fog’ in the medical record or claims data, and so then you’re not going to find” a signal that it may be linked to vaccination, Dr. Woodcock said. If such a side effect is not acknowledged by federal officials, “it’s because it doesn’t have a good research definition,” she added. “It isn’t, like, malevolence on their part.”
The government’s understaffed compensation fund has paid so little because it officially recognizes few side effects for Covid vaccines. And vaccine supporters, including federal officials, worry that even a whisper of possible side effects feeds into misinformation spread by a vitriolic anti-vaccine movement.
‘I’m Not Real’
Patients who believe they experienced serious side effects say they have received little support or acknowledgment.
Shaun Barcavage, 54, a nurse practitioner in New York City who has worked on clinical trials for H.I.V. and Covid, said that ever since his first Covid shot, merely standing up sent his heart racing — a symptom suggestive of postural orthostatic tachycardia syndrome, a neurological disorder that some studies have linked to both Covid and, much less often, vaccination.
He also experienced stinging pain in his eyes, mouth and genitals, which has abated, and tinnitus, which has not.
“I can’t get the government to help me,” Mr. Barcavage said of his fruitless pleas to federal agencies and elected representatives. “I am told I’m not real. I’m told I’m rare. I’m told I’m coincidence.”
Renee France, 49, a physical therapist in Seattle, developed Bell’s palsy — a form of facial paralysis, usually temporary — and a dramatic rash that neatly bisected her face. Bell’s palsy is a known side effect of other vaccines, and it has been linked to Covid vaccination in some studies.
But Ms. France said doctors were dismissive of any connection to the Covid vaccines. The rash, a bout of shingles, debilitated her for three weeks, so Ms. France reported it to federal databases twice.
“I thought for sure someone would reach out, but no one ever did,” she said.
Similar sentiments were echoed in interviews, conducted over more than a year, with 30 people who said they had been harmed by Covid shots. They described a variety of symptoms following vaccination, some neurological, some autoimmune, some cardiovascular.
All said they had been turned away by physicians, told their symptoms were psychosomatic, or labeled anti-vaccine by family and friends — despite the fact that they supported vaccines.
Even leading experts in vaccine science have run up against disbelief and ambivalence.
Dr. Gregory Poland, 68, editor in chief of the journal Vaccine, said that a loud whooshing sound in his ears had accompanied every moment since his first shot, but that his entreaties to colleagues at the Centers for Disease Control and Prevention to explore the phenomenon, tinnitus, had led nowhere.
He received polite responses to his many emails, but “I just don’t get any sense of movement,” he said.
“If they have done studies, those studies should be published,” Dr. Poland added. In despair that he might “never hear silence again,” he has sought solace in meditation and his religious faith.
Dr. Buddy Creech, 50, who led several Covid vaccine trials at Vanderbilt University, said his tinnitus and racing heart lasted about a week after each shot. “It’s very similar to what I experienced during acute Covid, back in March of 2020,” Dr. Creech said.
Research may ultimately find that most reported side effects are unrelated to the vaccine, he acknowledged. Many can be caused by Covid itself.
“Regardless, when our patients experience a side effect that may or may not be related to the vaccine, we owe it to them to investigate that as completely as we can,” Dr. Creech said.
Federal health officials say they do not believe that the Covid vaccines caused the illnesses described by patients like Mr. Barcavage, Dr. Zimmerman and Ms. France. The vaccines may cause transient reactions, such as swelling, fatigue and fever, according to the C.D.C., but the agency has documented only four serious but rare side effects.
Two are associated with the Johnson & Johnson vaccine, which is no longer available in the United States: Guillain-Barré syndrome, a known side effect of other vaccines, including the flu shot; and a blood-clotting disorder.
The C.D.C. also links mRNA vaccines made by Pfizer-BioNTech and Moderna to heart inflammation, or myocarditis, especially in boys and young men. And the agency warns of anaphylaxis, or severe allergic reaction, which can occur after any vaccination.
Listening for Signals
Agency scientists are monitoring large databases containing medical information on millions of Americans for patterns that might suggest a hitherto unknown side effect of vaccination, said Dr. Demetre Daskalakis, director of the C.D.C.’s National Center for Immunization and Respiratory Diseases.
“We toe the line by reporting the signals that we think are real signals and reporting them as soon as we identify them as signals,” he said. The agency’s systems for monitoring vaccine safety are “pretty close” to ideal, he said.
Those national surveillance efforts include the Vaccine Adverse Event Reporting System (VAERS). It is the largest database, but also the least reliable: Reports of side effects can be submitted by anyone and are not vetted, so they may be subject to bias or manipulation.
The system contains roughly one million reports regarding Covid vaccination, the vast majority for mild events, according to the C.D.C.
Federal researchers also comb through databases that combine electronic health records and insurance claims on tens of millions of Americans. The scientists monitor the data for 23 conditions that may occur following Covid vaccination. Officials remain alert to others that may pop up, Dr. Daskalakis said.
But there are gaps, some experts noted. The Covid shots administered at mass vaccination sites were not recorded in insurance claims databases, for example, and medical records in the United States are not centralized.
“It’s harder to see signals when you have so many people, and things are happening in different parts of the country, and they’re not all collected in the same system,” said Rebecca Chandler, a vaccine safety expert at the Coalition for Epidemic Preparedness Innovations.
An expert panel convened by the National Academies concluded in April that for the vast majority of side effects, there was not enough data to accept or reject a link.
Asked at a recent congressional hearing whether the nation’s vaccine-safety surveillance was sufficient, Dr. Peter Marks, director of the F.D.A.’s Center for Biologics Evaluation and Research, said, “I do believe we could do better.”
A Red Flag
In some countries with centralized health care systems, officials have actively sought out reports of serious side effects of Covid vaccines and reached conclusions that U.S. health authorities have not.
In Hong Kong, the government analyzed centralized medical records of patients after vaccination and paid people to come forward with problems. The strategy identified “a lot of mild cases that other countries would not otherwise pick up,” said Ian Wong, a researcher at the University of Hong Kong who led the nation’s vaccine safety efforts.
That included the finding that in rare instances — about seven per million doses — the Pfizer-BioNTech vaccine triggered a bout of shingles serious enough to require hospitalization.
The European Medicines Agency has linked the Pfizer and Moderna vaccines to facial paralysis, tingling sensations and numbness. The E.M.A. also counts tinnitus as a side effect of the Johnson & Johnson vaccine, although the American health agencies do not. There are more than 17,000 reports of tinnitus following Covid vaccination in VAERS.
Are the two linked? It’s not clear. As many as one in four adults has some form of tinnitus. Stress, anxiety, grief and aging can lead to the condition, as can infections like Covid itself and the flu.
There is no test or scan for tinnitus, and scientists cannot easily study it because the inner ear is tiny, delicate and encased in bone, said Dr. Konstantina Stankovic, an otolaryngologist at Stanford University.
Still, an analysis of health records from nearly 2.6 million people in the United States found that about 0.04 percent, or about 1,000, were diagnosed with tinnitus within three weeks of their first mRNA shot. In March, researchers in Australia published a study linking tinnitus and vertigo to the vaccines.
The F.D.A. is monitoring reports of tinnitus, but “at this time, the available evidence does not suggest a causal association with the Covid-19 vaccines,” the agency said in a statement.
Despite surveillance efforts, U.S. officials were not the first to identify a significant Covid vaccine side effect: myocarditis in young people receiving mRNA vaccines. It was Israeli authorities who first raised the alarm in April 2021. Officials in the United States said at the time that they had not seen a link.
On May 22, 2021, news broke that the C.D.C. was investigating a “relatively few” cases of myocarditis. By June 23, the number of myocarditis reports in VAERS had risen to more than 1,200 — a hint that it is important to tell doctors and patients what to look for.
Later analyses showed that the risk for myocarditis and pericarditis, a related condition, is highest after a second dose of an mRNA Covid vaccine in adolescent males aged 12 to 17 years.
In many people, vaccine-related myocarditis is transient. But some patients continue to experience pain, breathlessness and depression, and some show persistent changes on heart scans. The C.D.C. has said there were no confirmed deaths related to myocarditis, but in fact there have been several accounts of deaths reported post-vaccination.
Pervasive Misinformation
The rise of the anti-vaccine movement has made it difficult for scientists, in and out of government, to candidly address potential side effects, some experts said. Much of the narrative on the purported dangers of Covid vaccines is patently false, or at least exaggerated, cooked up by savvy anti-vaccine campaigns.
Questions about Covid vaccine safety are core to Robert F. Kennedy Jr.’s presidential campaign. Citing debunked theories about altered DNA, Florida’s surgeon general has called for a halt to Covid vaccination in the state.
“The sheer nature of misinformation, the scale of misinformation, is staggering, and anything will be twisted to make it seem like it’s not just a devastating side effect but proof of a massive cover-up,” said Dr. Joshua Sharfstein, a vice dean at Johns Hopkins University.
Among the hundreds of millions of Americans who were immunized for Covid, some number would have had heart attacks or strokes anyway. Some women would have miscarried. How to distinguish those caused by the vaccine from those that are coincidences? The only way to resolve the question is intense research.
But the National Institutes of Health is conducting virtually no studies on Covid vaccine safety, several experts noted. William Murphy, a cancer researcher who worked at the N.I.H. for 12 years, has been prodding federal health officials to initiate these studies since 2021.
The officials each responded with “that very tired mantra: ‘But the virus is worse,’” Dr. Murphy recalled. “Yes, the virus is worse, but that doesn’t obviate doing research to make sure that there may be other options.”
A deeper understanding of possible side effects, and who is at risk for them, could have implications for the design of future vaccines, or may indicate that for some young and healthy people, the benefit of Covid shots may no longer outweigh the risks — as some European countries have determined.
Thorough research might also speed assistance to thousands of Americans who say they were injured.
The federal government has long run the National Vaccine Injury Compensation Program, designed to compensate people who suffer injuries after vaccination. Established more than three decades ago, the program sets no limit on the amounts awarded to people found to have been harmed.
But Covid vaccines are not covered by that fund because Congress has not made them subject to the excise tax that pays for it. Some lawmakers have introduced bills to make the change.
Instead, claims regarding Covid vaccines go to the Countermeasures Injury Compensation Program. Intended for public health emergencies, this program has narrow criteria to pay out and sets a limit of $50,000, with stringent standards of proof.
It requires applicants to prove within a year of the injury that it was “the direct result” of getting the Covid vaccine, based on “compelling, reliable, valid, medical, and scientific evidence.”
The program had only four staff members at the beginning of the pandemic, and now has 35 people evaluating claims. Still, it has reviewed only a fraction of the 13,000 claims filed, and has paid out only a dozen.
Ilka Warshawsky, a 58-year-old pathologist, said she lost all hearing in her right ear after a Covid booster shot. But hearing loss is not a recognized side effect of Covid vaccination.
The compensation program for Covid vaccines sets a high bar for proof, she said, yet offers little information on how to meet it: “These adverse events can be debilitating and life-altering, and so it’s very upsetting that they’re not acknowledged or addressed.”
Dr. Zimmerman, the neuroscientist, submitted her application in October 2021 and provided dozens of supporting medical documents. She received a claim number only in January 2023.
In adjudicating her claim for workers’ compensation, Washington State officials accepted that Covid vaccination caused her injury, but she has yet to get a decision from the federal program.
One of her therapists recently told her she might never be able to live independently again.
“That felt like a devastating blow,” Dr. Zimmerman said. “But I’m trying not to lose hope there will someday be a treatment and a way to cover it.”
Last edited:
Heliobas Disciple
TB Fanatic
Dr. Syed did a video about the above anger and the heart and the 2nd part is about the NYT article in the above post. He starts the discussion on the NYT article at 12 min 6 sec, the link is prompted to start at that point. You can always start at the beginning if you want to watch the entire video.

 www.youtube.com
Don't Be Angry | NY Times and Vaccine Harm
www.youtube.com
Don't Be Angry | NY Times and Vaccine Harm
Drbeen Medical Lectures
Streamed live May 3, 2024
33 min 49 sec
Today I will like to share these two important articles. A study demonstrating that anger for 8 minutes can cause vascular health issues that may lead to cardiovascular disease events in the long run. And, the second is an article in NY Times about the vaccine harm.
URL list from Friday, May. 3 2024 16:09 PM
Translational Research of the Acute Effects of Negative Emotions on Vascular Endothelial Health: Findings From a Randomized Controlled Study | Journal of the American Heart Association
PowerPoint Presentation
Endothelin 1 - Wikipedia
Thousands Believe Covid Vaccines Harmed Them. Is Anyone Listening? - The New York Times
Don't Be Angry | NY Times and Vaccine Harm
Don't Be Angry | NY Times and Vaccine HarmToday I will like to share these two important articles. A study demonstrating that anger for 8 minutes can cause v...
www.youtube.com
Drbeen Medical Lectures
Streamed live May 3, 2024
33 min 49 sec
Today I will like to share these two important articles. A study demonstrating that anger for 8 minutes can cause vascular health issues that may lead to cardiovascular disease events in the long run. And, the second is an article in NY Times about the vaccine harm.
URL list from Friday, May. 3 2024 16:09 PM
Translational Research of the Acute Effects of Negative Emotions on Vascular Endothelial Health: Findings From a Randomized Controlled Study | Journal of the American Heart Association
PowerPoint Presentation
Endothelin 1 - Wikipedia
Thousands Believe Covid Vaccines Harmed Them. Is Anyone Listening? - The New York Times
Heliobas Disciple
TB Fanatic
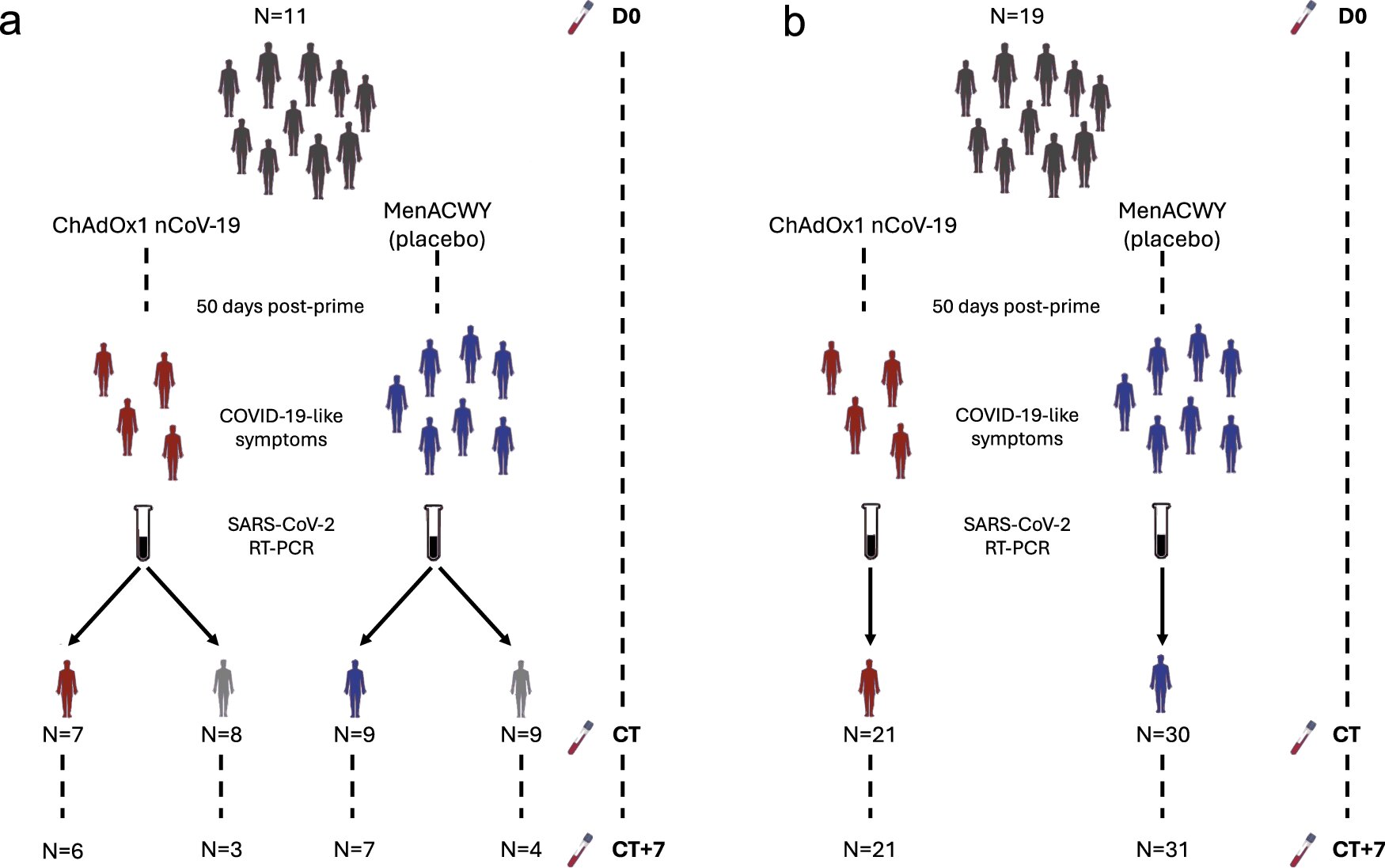
Study reveals how COVID-19 vaccines prevent severe disease
A study by scientists at the University of Oxford, has unveiled crucial insights into the way that COVID-19 vaccines mitigate severe illness in those who have been vaccinated.
Study reveals how COVID-19 vaccines prevent severe disease
by University of Oxford
May 3, 2024
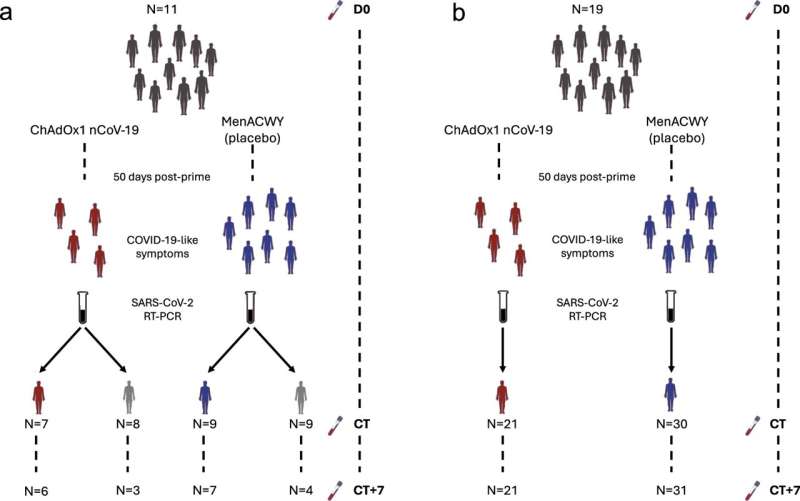
Study overview and cohort description. a Stage 1, symptomatic cohort: ChAdOx1 nCoV-19 vaccinees are shown in red. MenACWY vaccinees are placebo vaccinees (blue). NAAT+ve are participants with COVID-19, NAAT-ve are people who had COVID-19-like symptoms and thus had a CT visit but were subsequently shown not to have COVID-19 (gray); (b) Stage 2: all participants had COVID-19 (i.e. were NAAT+ve). D0: Baseline visit, before vaccination. CT: COVID-19 test visit. CT?+?7: 7 days after CT visit. Credit: Nature Communications (2024). DOI: 10.1038/s41467-024-47463-6
A study by scientists at the University of Oxford, has unveiled crucial insights into the way that COVID-19 vaccines mitigate severe illness in those who have been vaccinated.
Despite the global success of COVID-19 vaccination campaigns, concerns remain around the continued spread of this disease including in vaccinated individuals. For this reason, researchers at the Oxford Vaccine Group conducted an extensive investigation into the human immune response to COVID-19, in both vaccinated and unvaccinated individuals.
Employing contemporary "big-data" analyses, scientists can find novel associations between fundamental biological entities and indicators of the severity of a disease—to build patterns of health and disease.
Results of this study, published in the journal Nature Communications, categorically show a reduction in indicators of disease severity in those who had received the vaccine, demonstrating that the harmful inflammatory reaction to COVID-19 is less severe in those who have been vaccinated, when compared with those who haven't.
Professor Daniel O'Connor, Head of Bioinformatics at the Oxford Vaccine Group (OVG), led the study. He said, "These results confirm the efficacy of vaccination and its pivotal role in reducing the harmful consequences associated with COVID-19. The results of our research highlight the ChAdOx1 nCoV-19 vaccine's ability to modulate harmful responses to the SARS-CoV-2 virus, and therefore to reduce the severity of illness.
"The implications of these findings are far-reaching, offering evidence that is fundamental to future vaccine development and pandemic mitigation strategies. It also provides valuable guidance for policymakers and public health experts."
Professor Sir Andrew Pollard, Ashall Professor of Infection and Immunity and Director of the Oxford Vaccine Group, said, "Better understanding of how vaccines can reduce the severity of infections caused by viruses like COVID-19 is a key part of our preparedness to make effective vaccines against the next pandemic threat. Ongoing research is critical as we know the next one is coming but we don't know which virus or when it will be."
The study employed state-of-the-art technologies, including RNA-sequencing (to capture the level of genes produced by blood cells), to achieve these results. While the findings are promising, the study acknowledges limitations such as a focus on mild cases and sample size constraints, highlighting the need for further research utilizing advanced techniques to enhance resolution.
Key findings from the study include:
- Identification of unique responses to COVID-19 among vaccinated individuals, highlighting the vaccine's influence on responses to this disease.
- Demonstrated reduction in harmful responses associated with COVID-19 severity in recipients of the ChAdOx1 nCoV-19 vaccine compared with unvaccinated counterparts.
- COVID-19 in vaccinated individuals resulted in less COVID-19-induced blood cell count changes.
- Correlation between decreased levels of a particular class of molecules in blood (microRNAs) and elevated levels of inflammation, suggesting a regulatory role for these molecules in inflammatory responses to viral infection.
More information: Ruth E. Drury et al, Multi-omics analysis reveals COVID-19 vaccine induced attenuation of inflammatory responses during breakthrough disease, Nature Communications (2024). DOI: 10.1038/s41467-024-47463-6
Journal information: Nature Communications
Provided by University of Oxford
Heliobas Disciple
TB Fanatic

Doctors describe Texas dairy farm worker's case of bird flu
Doctors in Texas are describing the only known human case of H5N1 avian flu connected to the ongoing outbreak of the disease in dairy cows.
Doctors describe Texas dairy farm worker's case of bird flu
by Ernie Mundell
May 3, 2024
Doctors in Texas are describing the only known human case of H5N1 avian flu connected to the ongoing outbreak of the disease in dairy cows.
Bird flu in humans remains extremely rare, but in the hundreds of cases documented worldwide over the past few years, about half proved fatal—upping scientists' concerns about the possibility that an easily transmitted human bird flu might one day emerge.
The unidentified Texas man, a dairy farm worker, appears to have been lucky: His case of H5N1 amounted to little more than a case of conjunctivitis, an inflammatory "pinkeye" that resolved after antibiotic treatment.
A team led by Dr. Timothy Uyeki of the U.S. Centers for Disease Control and Atlanta and Dr. Scott Milton of the Texas Department of State Health Services described the case in a report published May 3 in the New England Journal of Medicine.
"In late March 2024, an adult dairy farm worker had onset of redness and discomfort in the right eye," they wrote.
Upon examination, they diagnosed what looked like a normal case of conjunctivitis—bloodshot and painful eyes but with no effect on the man's vision.
Other than that, his "vital signs were unremarkable," the team said, with no respiratory symptoms, clear lungs and a normal blood-oxygen level.
However, "the worker reported no contact with sick or dead wild birds, poultry, or other animals but reported direct and close exposure to dairy cows that appeared to be well and with sick cows that showed the same signs of illness as cows at other dairy farms in the same area of northern Texas with confirmed HPAI A(H5N1) virus infection," the researchers said.
"The worker reported wearing gloves when working with cows but did not use any respiratory or eye protection."
Swabs were taken of his eyes and nasal passages, and they tested positive for flu. Further testing narrowed that diagnosis down to H5N1.
The man's condition didn't worsen, but he was given a standard antiviral medication, oseltamivir, twice daily for five days, and was told to isolate at home. People living in his home were also given the antiviral to protect them from H5N1.
"Over the subsequent days, the worker reported resolution of conjunctivitis without respiratory symptoms, and household contacts remained well," the team wrote.
Close laboratory inspection of the strain implicated in the man's infection reveal a key viral mutation, called PB2 E627K. This mutation "has been associated with viral adaptation to mammalian hosts and detected previously in humans and other mammals infected with HPAI A(H5N1) viruses," the researchers noted.
They added that the man's H5N1 strain showed no evidence of mutations that might make it any less responsive to treatment with standard antivirals recommended against influenza.
And there was good news for scientists developing avian influenza vaccines, should they become necessary: Specific vaccine-sensitive components of the strain of H5N1 that infected the dairy worker are "closely related" to viruses already being studied by bird flu vaccine researchers.
"Because influenza A(H5N1) viruses have pandemic potential, these candidate vaccine viruses are available to manufacturers and could be used to produce vaccine if needed," the researchers noted.
The latest data on the outbreak of bird flu among U.S. dairy cows has detected infection in 36 herds across nine states. Tests conducted by federal health officials have found evidence of inactive DNA "fragments" of H5N1 in about 1 in 20 samples of milk, but no live virus—it is thought that pasteurization kills the virus. Tests of ground beef have also turned up negative for the virus.
More information: Timothy M. Uyeki et al, Highly Pathogenic Avian Influenza A(H5N1) Virus Infection in a Dairy Farm Worker, New England Journal of Medicine (2024). DOI: 10.1056/NEJMc2405371
Heliobas Disciple
TB Fanatic
(fair use applies)
USDA Study Shows Various New Mutations In H5N1 Virus Found In Dairy Cows
Nikhil Prasad Fact checked by:Thailand Medical News Team
May 04, 2024
In recent months, a concerning development has emerged within the dairy farming industry in the United States. A strain of the H5N1 virus, commonly known as bird flu, has been detected in dairy cows across several states, prompting significant attention from health authorities and researchers alike. A comprehensive genetic analysis conducted by the United States Department of Agriculture (USDA) that is covered in this H5N1 News report, has revealed a series of new mutations within the virus, raising questions about its potential impact on public health and agricultural practices.
The Discovery of New Mutations
The USDA study uncovered a total of 491 amino acid sites with nonsynonymous changes in the H5N1 virus strains infecting the dairy cows in the United States. Among these changes, 309 mutations were identified at sites associated with functional alterations, indicating a substantial level of genetic variation within the virus population.
Notably, several of these mutations were linked to changes in pathogenicity, virulence, host range specificity, and mammalian adaptation, suggesting an evolving landscape of viral characteristics.
Notably, variants affecting pathogenicity in key virus components like HA, MP, NP, and PB2 were detected, such as an increase in Q154R and S207G, a decrease in V105M, and an increase in D701N. Furthermore, mutations linked to increased virulence (Q134K/R, V67I, E627K) and host-range specificity (A55T, E57G, N71S, E229K) were also identified.
Of particular concern were variants in PB2 associated with mammalian adaptation, with E627K, M631L, and D701N showing high frequencies, especially M631L detected in 99% of 214 cattle. However, the critical mammal adaptation mutation PB2 271A was notably absent, except for one sample. Additionally, mutations affecting receptor binding affinity were observed in HA, adding another layer of complexity to the virus's behavior.
These findings underscore the dynamic nature of the H5N1 virus and its potential to evolve rapidly, posing challenges for containment and control efforts.
Implications for Transmission and Spread
Another key findings of the study was the ability of the H5N1 virus to cross species barriers, with evidence of transmission from wild birds to cattle in the Texas Panhandle. This spillover event was followed by rapid dissemination of the virus within dairy farms across multiple states, including Texas, Kansas, Michigan, and New Mexico. The movement of asymptomatic cattle played a crucial role in facilitating the spread of the virus, highlighting the challenges in containing and controlling such outbreaks within livestock populations.
Risk Factors and Concerns
While none of the identified mutations individually posed an immediate cause for alarm, the cumulative effect of these genetic changes raised concerns among experts. Of particular worry is the potential for the virus to evolve in ways that enhance its ability to spread between species, including humans. The study emphasized the need for ongoing surveillance and monitoring to track the prevalence of these mutations and assess their impact on public health.
Timeline and Epidemiological Insights
The timeline of the outbreak, as revealed by genetic analyses, indicated that the virus had been circulating in cattle for several months before formal confirmation by regulatory authorities. This period of undetected transmission underscored the challenges in early detection and containment of emerging infectious diseases within livestock populations. The study also highlighted instances of interspecies transmission, with the virus spreading from cattle back to wild birds, poultry, domestic cats, and even a raccoon.
Surveillance and Preventive Measures
In response to the findings, researchers and health officials stressed the importance of enhanced surveillance measures, not only on affected farms but also across the broader agricultural landscape. Large-scale monitoring efforts were recommended to track the movement of the virus, identify potential hotspots of infection, and implement targeted control strategies. Additionally, the study advocated for continuous assessment of antiviral drug efficacy against the evolving viral strains.
Public Health Implications
The emergence of new mutations in the H5N1 virus within dairy cows raised significant public health concerns. While the virus had primarily affected livestock, there were fears of potential spillover into human populations, especially given the observed mutations associated with increased mammalian adaptation. The study highlighted the need for vigilance and preparedness in dealing with zoonotic threats, emphasizing the importance of early detection, rapid response protocols, and effective communication channels between veterinary and public health agencies.
Future Research Directions
Looking ahead, the study called for further research into the pathobiology and evolution of the virus within dairy cattle. Understanding the mechanisms driving viral transmission, host adaptation, and genetic variability would be crucial in devising targeted interventions and preventive measures. Moreover, ongoing surveillance efforts would be essential in assessing the evolving risk landscape and informing evidence-based strategies for mitigating the spread of zoonotic diseases.
Conclusion
The USDA study shed light on the complex dynamics of the H5N1 virus outbreak in dairy cows, unveiling a landscape of genetic mutations that could impact its transmission, virulence, and potential for interspecies spread. While the immediate risk to human health remained relatively low, the findings underscored the need for proactive monitoring, robust surveillance systems, and collaborative efforts across sectors to address emerging infectious threats in both animal and human populations.
The study findings were published on a preprint server and are currently being peer reviewed.
USDA Study Shows Various New Mutations In H5N1 Virus Found In Dairy Cows
Nikhil Prasad Fact checked by:Thailand Medical News Team
May 04, 2024
In recent months, a concerning development has emerged within the dairy farming industry in the United States. A strain of the H5N1 virus, commonly known as bird flu, has been detected in dairy cows across several states, prompting significant attention from health authorities and researchers alike. A comprehensive genetic analysis conducted by the United States Department of Agriculture (USDA) that is covered in this H5N1 News report, has revealed a series of new mutations within the virus, raising questions about its potential impact on public health and agricultural practices.
The Discovery of New Mutations
The USDA study uncovered a total of 491 amino acid sites with nonsynonymous changes in the H5N1 virus strains infecting the dairy cows in the United States. Among these changes, 309 mutations were identified at sites associated with functional alterations, indicating a substantial level of genetic variation within the virus population.
Notably, several of these mutations were linked to changes in pathogenicity, virulence, host range specificity, and mammalian adaptation, suggesting an evolving landscape of viral characteristics.
Notably, variants affecting pathogenicity in key virus components like HA, MP, NP, and PB2 were detected, such as an increase in Q154R and S207G, a decrease in V105M, and an increase in D701N. Furthermore, mutations linked to increased virulence (Q134K/R, V67I, E627K) and host-range specificity (A55T, E57G, N71S, E229K) were also identified.
Of particular concern were variants in PB2 associated with mammalian adaptation, with E627K, M631L, and D701N showing high frequencies, especially M631L detected in 99% of 214 cattle. However, the critical mammal adaptation mutation PB2 271A was notably absent, except for one sample. Additionally, mutations affecting receptor binding affinity were observed in HA, adding another layer of complexity to the virus's behavior.
These findings underscore the dynamic nature of the H5N1 virus and its potential to evolve rapidly, posing challenges for containment and control efforts.
Implications for Transmission and Spread
Another key findings of the study was the ability of the H5N1 virus to cross species barriers, with evidence of transmission from wild birds to cattle in the Texas Panhandle. This spillover event was followed by rapid dissemination of the virus within dairy farms across multiple states, including Texas, Kansas, Michigan, and New Mexico. The movement of asymptomatic cattle played a crucial role in facilitating the spread of the virus, highlighting the challenges in containing and controlling such outbreaks within livestock populations.
Risk Factors and Concerns
While none of the identified mutations individually posed an immediate cause for alarm, the cumulative effect of these genetic changes raised concerns among experts. Of particular worry is the potential for the virus to evolve in ways that enhance its ability to spread between species, including humans. The study emphasized the need for ongoing surveillance and monitoring to track the prevalence of these mutations and assess their impact on public health.
Timeline and Epidemiological Insights
The timeline of the outbreak, as revealed by genetic analyses, indicated that the virus had been circulating in cattle for several months before formal confirmation by regulatory authorities. This period of undetected transmission underscored the challenges in early detection and containment of emerging infectious diseases within livestock populations. The study also highlighted instances of interspecies transmission, with the virus spreading from cattle back to wild birds, poultry, domestic cats, and even a raccoon.
Surveillance and Preventive Measures
In response to the findings, researchers and health officials stressed the importance of enhanced surveillance measures, not only on affected farms but also across the broader agricultural landscape. Large-scale monitoring efforts were recommended to track the movement of the virus, identify potential hotspots of infection, and implement targeted control strategies. Additionally, the study advocated for continuous assessment of antiviral drug efficacy against the evolving viral strains.
Public Health Implications
The emergence of new mutations in the H5N1 virus within dairy cows raised significant public health concerns. While the virus had primarily affected livestock, there were fears of potential spillover into human populations, especially given the observed mutations associated with increased mammalian adaptation. The study highlighted the need for vigilance and preparedness in dealing with zoonotic threats, emphasizing the importance of early detection, rapid response protocols, and effective communication channels between veterinary and public health agencies.
Future Research Directions
Looking ahead, the study called for further research into the pathobiology and evolution of the virus within dairy cattle. Understanding the mechanisms driving viral transmission, host adaptation, and genetic variability would be crucial in devising targeted interventions and preventive measures. Moreover, ongoing surveillance efforts would be essential in assessing the evolving risk landscape and informing evidence-based strategies for mitigating the spread of zoonotic diseases.
Conclusion
The USDA study shed light on the complex dynamics of the H5N1 virus outbreak in dairy cows, unveiling a landscape of genetic mutations that could impact its transmission, virulence, and potential for interspecies spread. While the immediate risk to human health remained relatively low, the findings underscored the need for proactive monitoring, robust surveillance systems, and collaborative efforts across sectors to address emerging infectious threats in both animal and human populations.
The study findings were published on a preprint server and are currently being peer reviewed.
jward
passin' thru
IIRC from the study abstract, the group tested were those who did not comprise high risk groups- I recall they were overweight, but assume that not falling into high risk groups meant there was no diabetes present; without doing a long slog through the parameters and supporting docs, I'd guess that either those diabetics are seen to accrue some benefit from metformin that lessons their experience, or conversely the physical conditions due to their more advanced disease states dampens the benefits.I’m tired from working 11 hrs and not making the connection, most likely; but….diabetes IS a comorbidity for serious Covid infections.
So…,doesn’t it make sense then that many diabetics already ARE on metformin, therefore they should not be at risk?
Help me with this one here
This particular study seemed to be aimed at bolstering the use of metformin in those subsets of groups not rigourously studied yet- those not sick enough for hospitalization and not traditionally on metformin- with the conclusion being hey yeah, it shaves some time/symptom/intensity off the illness and is not contraindicated. Prescription is indicated.
:: shrug :: Gimme at least a first cup o' coffee and I'll give ya another, probably better answer though

northern watch
TB Fanatic

psychgirl
Has No Life - Lives on TB
Thank you!IIRC from the study abstract, the group tested were those who did not comprise high risk groups- I recall they were overweight, but assume that not falling into high risk groups meant there was no diabetes present; without doing a long slog through the parameters and supporting docs, I'd guess that either those diabetics are seen to accrue some benefit from metformin that lessons their experience, or conversely the physical conditions due to their more advanced disease states dampens the benefits.
This particular study seemed to be aimed at bolstering the use of metformin in those subsets of groups not rigourously studied yet- those not sick enough for hospitalization and not traditionally on metformin- with the conclusion being hey yeah, it shaves some time/symptom/intensity off the illness and is not contraindicated. Prescription is indicated.
:: shrug :: Gimme at least a first cup o' coffee and I'll give ya another, probably better answer though
Lol, yep, grab that coffee!!
")
Lee2
Senior Member
Do we still believe that everyone who had a Covid vaxx is likely to die within 5 years (would be 2026)? I've known many who have had the vaxx and though some have had some serious health issues, they are doing pretty well now and seem to be on the road to good health. A few had clots and blockage but after heart stents are doing very well. One had cancer but seems to have beaten that. Others have not had health issues at all!
Have opinions in the know changed on this at all?
Edit to add - don't get me wrong. I've known some people who were vaxxed and died from fast acting cancers (a few weeks) and some who passed away within 7 months of getting their vaxx - no idea of cause. So I am not blind but I just wonder if we can breathe about our loved ones yet.
Have opinions in the know changed on this at all?
Edit to add - don't get me wrong. I've known some people who were vaxxed and died from fast acting cancers (a few weeks) and some who passed away within 7 months of getting their vaxx - no idea of cause. So I am not blind but I just wonder if we can breathe about our loved ones yet.
Last edited:
Profit of Doom
Dismember
Don’t forget this.
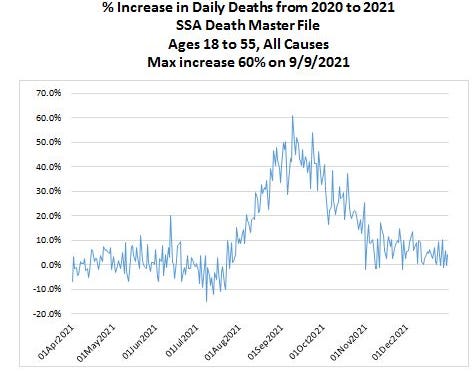
 kirschsubstack.com
kirschsubstack.com
Vaccines are taking an average of 5 months to kill people
The CDC has been hiding the Social Security Administration death master file. I got it from a whistleblower. This shows deaths are taking 5 months from the jab to happen. This is why it's hard to see.
kirschsubstack.com
naegling62
Veteran Member
Do we still believe that everyone who had a Covid vaxx is likely to die within 5 years (would be 2026)? I've known many who have had the vaxx and though some have had some serious health issues, they are doing pretty well now and seem to be on the road to good health. A few had clots and blockage but after heart stents are doing very well. One had cancer but seems to have beaten that. Others have not had health issues at all!
Have opinions in the know changed on this at all?
Edit to add - don't get me wrong. I've known some people who were vaxxed and died from fast acting cancers (a few weeks) and some who passed away within 7 months of getting their vaxx - no idea of cause. So I am not blind but I just wonder if we can breathe about our loved ones yet.

jward
passin' thru
Leading Report
@LeadingReport
BREAKING: Former CNN anchor and vaccine pusher Chris Cuomo disclosed for the first time that he has been suffering from side effects he attributes to the COVID-19 vaccine.
Cuomo admitted his side effects during an in-depth interview with nurse practitioner Sean Barcavage.
“We know that vaccines can have unintended consequences, a.k.a. side effects… But nobody’s really talking about it because they’re too afraid of blame, and they just want it to go away.”
“Sean, I can’t help you because I’m no clinician. I’m sick myself. But I’m working with people who are working on this, so I’ll make sure that we’re in touch right after the show, and I’ll help any way I can. You may be ahead of me. I’ll connect you with my clinicians, and maybe you can share different protocols and things that may help. But I will never stop reporting on this. All I’m doing is just beating the drum for a 9/11-style commission to figure out what worked and what didn’t and what questions need to be answered because it’s not over,” Cuomo said.
@LeadingReport
BREAKING: Former CNN anchor and vaccine pusher Chris Cuomo disclosed for the first time that he has been suffering from side effects he attributes to the COVID-19 vaccine.
Cuomo admitted his side effects during an in-depth interview with nurse practitioner Sean Barcavage.
“We know that vaccines can have unintended consequences, a.k.a. side effects… But nobody’s really talking about it because they’re too afraid of blame, and they just want it to go away.”
“Sean, I can’t help you because I’m no clinician. I’m sick myself. But I’m working with people who are working on this, so I’ll make sure that we’re in touch right after the show, and I’ll help any way I can. You may be ahead of me. I’ll connect you with my clinicians, and maybe you can share different protocols and things that may help. But I will never stop reporting on this. All I’m doing is just beating the drum for a 9/11-style commission to figure out what worked and what didn’t and what questions need to be answered because it’s not over,” Cuomo said.
Heliobas Disciple
TB Fanatic
Common diabetes drug lowers SARS-CoV-2 levels, clinical trial finds
Stephanie Soucheray, MA
Today, researchers from the University of Minnesota published evidence that the common diabetes drug metformin decreases the amount of SARS-CoV-2 in the body and helps reduce the risk of rebound symptoms if given early in the course of non-severe illness.
The study, published in Clinical Infectious Diseases, suggests metformin may also help prevent long COVID.
The researchers tested metformin against a placebo in 999 adults infected with COVID-19. More than 50% of the study enrollees were vaccinated, and treatment took place when the Omicron variant was the most dominant strain in the United States.
Study included those at standard-risk
Moreover, according to Carolyn Bramante, MD, principal investigator of the study and an assistant professor at the University of Minnesota, the study participants represented a standard- risk population, a group that currently lacks effective treatment options for the novel coronavirus.
"This is not a high-risk population," Bramante told CIDRAP News. Instead, participants were 30 years or older, had a body mass index of 25 or higher (overweight), and did not require hospitalization for their COVID-19 infection.
In several trials, Paxlovid has been shown to prevent deaths and hospitalization in high-risk, unvaccinated people, but standard-risk populations have not shown improvement in either time to resolution of symptoms or the incidence of hospitalization or death.
Bramante said that these patient population demographics suggest metformin may be a clinical tool in outpatient medication that could be widely used.
"The data would be justified in prescribing it outpatient medication that works," she said.
Four-fold reduction in viral load by day 10
Participants were given a 14-day course of metformin, and participants collected nasal swabs on days 1, 5, and 10. Bramante said early treatment was key: Participants were enrolled within 3 days of a positive test, and if symptomatic, reported having symptoms for 7 or fewer days.
The mean SARS-CoV-2 viral load was reduced 3.6-fold with metformin relative to placebo by day 10, the authors found, and those who received metformin were less likely to have a detectable viral load than placebo at days 5 or 10 (odds ratio [OR], 0.72; 95% confidence interval [CI], 0.55 to 0.94).
Metformin reduced the odds of hospitalization or death through 28 days by 58%; emergency department visits, hospitalizations, and death through 14 days by 42%; and long COVID through 10 months by 42%.
Viral rebound, defined as a higher viral load at day 10 than day 5, was less frequent with metformin (3.28%) than placebo (5.95%; OR, 0.68; 95% CI, 0.36 to 1.29).
While the mechanism of action is not known, Bramante said metformin likely lowers inflammation and inhibits translation of the virus.
This study makes a strong case for a potential effect of metformin on COVID-19 virologic decay.
In a commentary on the study, the authors write, "This study makes a strong case for a potential effect of metformin on COVID-19 virologic decay and prompts reevaluation of existing data in support of its use."
Common diabetes drug lowers SARS-CoV-2 levels, clinical trial finds
The first time we discussed Metformin for Covid on this thread was posted by marsh on Sept 29, 2021. (We've posted about it since then too.) Once again, we were ahead of the curve
Also posted on this thread by Krayola was an article with a study that determined NOT TO USE metformin with hydroxychloroquine or chloroquine. So if you are going that route, keep that in mind. link description is wrong, it should take you to the correct post.see:
CORONA - Main Coronavirus thread
https://www.wfla.com/community/health/coronavirus/coronavirus-has-stabilized-in-florida-gov-ron-desantis-says/ (fair use applies) Coronavirus has ‘stabilized’ in Florida, Gov. Ron DeSantis says by: Mahsa Saeidi Posted: Jul 6, 2020 / 07:21 PM EDT / Updated: Jul 6, 2020 / 07:33 PM EDT...
Here's another angle on the recent study:

Research strengthens case to treat COVID-19 with metformin, not ivermectin
Patients with COVID-19 had lower viral loads if treated with metformin, according to new University of Minnesota research that argues for broader use of the cheap anti-diabetes drug and against the controversial use of ivermectin.
Research strengthens case to treat COVID-19 with metformin, not ivermectin
by Jeremy Olson, Star Tribune
May 4, 2024
Patients with COVID-19 had lower viral loads if treated with metformin, according to new University of Minnesota research that argues for broader use of the cheap anti-diabetes drug and against the controversial use of ivermectin.
The findings helped connect the dots and explain why metformin in a U-led clinical trial reduced the likelihood of COVID-related hospitalizations or the development of long COVID illness. The amount of virus in patients is often associated with the severity of illnesses and complications, and it was found to be almost fourfold lower in patients in the trial who took metformin vs. non-medicating placebo pills.
The results "could be a tipping point" that convinces doctors to prescribe metformin to treat COVID, said Dr. Carolyn Bramante, the lead U researcher of the drug trial. "But people don't want to be wrong" so she predicted many will wait for results of a larger drug trial called ACTIV-6.
The U study results also showed that metformin users were less likely to see a rebound in 10 days of their viral loads, which also can be a proxy for the development of post-COVID complications, or long COVID.
Researchers of the U-led trial, named COVID-OUT, found no statistically significant evidence of lower viral loads in participants who took ivermectin, an anti-parasitic drug that has been championed by some doctors, politicians and vaccine skeptics. A third drug, fluvoxamine, also showed no benefit.
All three drugs had been identified early in the pandemic as promising targets, but a U computer simulation singled out metformin for its potential to disrupt the life cycle of the coronavirus that causes COVID-19.
Metformin's benefits appeared statistically stronger in unvaccinated participants, but the drug also appeared to work for vaccinated participants. It also reduced viral loads in those infected by the alpha, delta or omicron coronavirus variants that caused distinct COVID-19 waves over the three years of the pandemic.
COVID has become something of an afterthought in 2024. Hospitalizations related to the infectious disease have plummeted since December, according to Thursday's state update. Signs of the coronavirus in Minnesota wastewater samples were at their lowest since August.
COVID-19 related deaths have declined from 113 in February in Minnesota to 62 in March to 40 so far in April—almost all among senior citizens. Health officials warned that this is still an elevated mortality rate that has just been normalized by the earlier severity of the pandemic.
Long COVID also remains a concern: federal survey data showed that more than 7% of Minnesota adults were dealing with the lingering condition last month.
Federal health officials earlier this year urged people 65 and older at greatest risk of severe COVID to seek additional vaccine boosters. Uptake has been slow; the most recent state data showed only 3% of seniors were up to date on COVID vaccinations since the latest recommendations.
2024 StarTribune. Distributed by Tribune Content Agency, LLC.
Heliobas Disciple
TB Fanatic

People With More COVID-19 Vaccine Doses More Likely to Contract COVID-19: Study
Vaccinated people were at higher risk of contracting COVID-19, researchers find.
www.theepochtimes.com
People With More COVID-19 Vaccine Doses More Likely to Contract COVID-19: Study
Vaccinated people were at higher risk of contracting COVID-19, researchers find.
By Zachary Stieber, Senior Reporter
5/3/2024
People who received more than one dose of a COVID-19 vaccine were more likely to contract COVID-19, according to a new study.
An analysis of data from Cleveland Clinic employees found that people who received two or more doses were at higher risk of COVID-19, Dr. Nabin Shrestha and his co-authors reported.
The risk of contracting COVID-19 was 1.5 times higher for those who received two doses, 1.95 times higher for those who received three doses, and 2.5 times higher for those who received more than three doses, the researchers found.
The higher risk was compared to people who received zero or one dose of a vaccine.
Even after adjusting for variables, the elevated risk remained.
“The exact reason for this finding is not clear. It is possible that this may be related to the fact that vaccine-induced immunity is weaker and less durable than natural immunity. So, although somewhat protective in the short term, vaccination may increase risk of future infection,” the researchers said in the paper, which was released as a preprint.
Dr. Robert Malone, a vaccine researcher who was not involved in the paper, told The Epoch Times that the paper served as “another acknowledgment that the products are not effective or are at very low effectiveness and are contributing to negative effectiveness [down the line].”
He noted that the researchers did not study vaccine safety among the employee population. The COVID-19 vaccines can cause a number of side effects, including fatal heart inflammation, according to the literature and death records.
Earlier studies and data have also suggested that people with more vaccine doses are more susceptible to COVID-19 infection, including previous papers from the Cleveland Clinic scientists and a study from Iceland.
The U.S. Centers for Disease Control and Prevention (CDC), which has repeatedly declined requests to comment on outside research, recommends virtually all people aged 6 months and older receive one of the currently available COVID-19 vaccines, regardless of how many shots they’ve received, although a meeting later in May is set to discuss whether to update the vaccine formulations to improve protection.
CDC scientists said in a paper published in February in the agency’s weekly report that the latest version of the vaccines, a monovalent targeting the XBB.1.5 subvariant, provided 49 percent effectiveness between 60 and 119 days later when the JN.1 virus strain was dominant. Supplementary data, however, showed that people aged 50 and older who received the previous bivalent version were more susceptible to symptomatic infection.
Authors disclosed no conflicts of interest and acknowledged at least five limitations, including how they used a proxy for infection with JN.1.
Another study, released ahead of peer review in April, estimated the effectiveness of Pfizer’s updated vaccine as 32 percent against hospitalization from late 2023 through early 2024. The research was conducted by scientists from multiple institutions, including the U.S. Department of Veterans Affairs and Pfizer, many authors reported conflicts of interest, and some of the funding came from Pfizer.
People’s immune systems being trained to react to older virus strains at the expense of protection against newer variants is one theory for why the vaccinated might be more prone to infection.
“Multiple vaccine doses may have the effect of antibody-dependent enhancement or ‘original antigenic sin,’ which increase the infection response disproportionally to antibodies generated from the first vaccine dose, rather than from the current vaccine or the current infection, making the antibody response less effective,” Dr. Harvey Risch, professor emeritus of epidemiology at the Yale School of Public Health, told The Epoch Times in an email after reviewing the paper.
Dr. Shrestha, who did not respond to a request for comment, and the Cleveland Clinic researchers aimed to analyze the effectiveness of the XBB.1.5 shots against JN.1, which displaced XBB.1.5 before the end of 2023.
To do so, they analyzed the incidence of COVID-19 among Cleveland Clinic employees from Dec. 31, 2023, to April 22, 2024.
Among approximately 47,500 employees included in the study, 838 tested positive for COVID-19 during that period.
Unadjusted data showed no difference between people who received one of the updated shots and people who didn’t, but after adjusting for age and other factors, the researchers estimated the shots provided 23 percent effectiveness against infection.
Federal and global guidelines consider vaccines ineffective if they provide under 50 percent shielding.
The number of severe illnesses among the study population was too small to estimate effectiveness against severe illness, the researchers said.
Listed limitations included the inability to separate symptomatic and asymptomatic infections. No conflicts of interest were reported and authors said they received no funding.
Heliobas Disciple
TB Fanatic
VIRAL SEPSIS: A New Presentation of the Covid Virus?
Vejon Health
Streamed live May 4, 2024
32 min 38 sec
Is viral sepsis a new presentation of the Covid virus? Dr. Philip McMillan discusses this novel variant and its implications in this informative video. How would we know before it is too late? Is Geert Vanden Bossche correct again?
Timecodes
0:00 - 0:10 - Intro
0:11 - 5:39 - Exploring potential shift in Covid-19 presentation towards viral sepsis and implications for intensive care.
5:40 - 9:31 - Emergence of the KP2 variant with increased transmissibility and presence in multiple countries.
9:32 - 13:54 - Immune cells are significantly impacted by the virus, even in cases of mild symptoms.
13:55 - 18:46 - Immune response analogy to combat Covid virus variants.
18:47 - 23:35 - Implications of viral sepsis caused by Covid virus on immune response and endothelial cells.
23:36 - 28:13 - Neurological implications of Covid virus crossing brain barrier triggering significant immune response.
28:14 - 32:39 - Potential link between low lymphocytes and viral infection causing excess deaths.
Recap by Tammy AI
Heliobas Disciple
TB Fanatic
Thousands Believe Covid Vaccines Harmed Them. Is Anyone Listening?
All vaccines have at least occasional side effects. But people who say they were injured by Covid vaccines believe their cases have been ignored.
By Apoorva Mandavilli - New York Times
Within minutes of getting the Johnson & Johnson Covid-19 vaccine, Michelle Zimmerman felt pain racing from her left arm up to her ear and down to her fingertips. Within days, she was unbearably sensitive to light and struggled to remember simple facts.
She was 37, with a Ph.D. in neuroscience, and until then could ride her bicycle 20 miles, teach a dance class and give a lecture on artificial intelligence, all in the same day. Now, more than three years later, she lives with her parents.
Eventually diagnosed with brain damage, she cannot work, drive or even stand for long periods of time.
[snip]
Pandemic Officials are "Disappointed in Themselves", per the New York Times
Should we forgive them?
 www.igor-chudov.com
www.igor-chudov.com
EMPHASIS AT ORIGINAL SOURCE (not added by me)
Pandemic Officials are "Disappointed in Themselves", per the New York Times
Should we forgive them?
Igor Chudov
May 03, 2024
An article in the New York Times is titled “Thousands Believe Covid Vaccines Harmed Them. Is Anyone Listening?” (no paywall)
The author, Apoorva Mandavilli, was correctly described by Vinay Prasad as the worst science reporter. She states her surprise about “thousands” who believe that Covid vaccines harmed them. While we know that number to be an understatement, it is interesting how the New York Times recognizes them after years of stonewalling.
But in a recent interview, Dr. Janet Woodcock, a longtime leader of the Food and Drug Administration, who retired in February, said she believed that some recipients had experienced uncommon but “serious” and “life-changing” reactions beyond those described by federal agencies.
“I feel bad for those people,” said Dr. Woodcock, who became the F.D.A.’s acting commissioner in January 2021 as the vaccines were rolling out. “I believe their suffering should be acknowledged, that they have real problems, and they should be taken seriously.”
FDA’s Dr. Woodcock is disappointed in herself:
“I’m disappointed in myself,” she added. “I did a lot of things I feel very good about, but this is one of the few things I feel I just didn’t bring it home.”
The article discusses thousands of people gaslit by vaccine promoters and their doctors, who were intimidated not to report vaccine injuries:
Similar sentiments were echoed in interviews, conducted over more than a year, with 30 people who said they had been harmed by Covid shots. They described a variety of symptoms following vaccination, some neurological, some autoimmune, some cardiovascular.
All said they had been turned away by physicians, told their symptoms were psychosomatic, or labeled anti-vaccine by family and friends — despite the fact that they supported vaccines.
Even some key vaccine promoters report vaccine injuries, which they could not report anywhere:Dr. Gregory Poland, 68, editor in chief of the journal Vaccine, said that a loud whooshing sound in his ears had accompanied every moment since his first shot, but that his entreaties to colleagues at the Centers for Disease Control and Prevention to explore the phenomenon, tinnitus, had led nowhere.
He received polite responses to his many emails, but “I just don’t get any sense of movement,” he said.
The federal officials in charge of setting the policy still refuse to believe these reports:Federal health officials say they do not believe that the Covid vaccines caused the illnesses described by patients like Mr. Barcavage, Dr. Zimmerman and Ms. France. The vaccines may cause transient reactions, such as swelling, fatigue and fever, according to the C.D.C., but the agency has documented only four serious but rare side effects.
The excuse that these officials give for ignoring vaccine harms is that they were fighting misinformation:The rise of the anti-vaccine movement has made it difficult for scientists, in and out of government, to candidly address potential side effects, some experts said. Much of the narrative on the purported dangers of Covid vaccines is patently false, or at least exaggerated, cooked up by savvy anti-vaccine campaigns.
Questions about Covid vaccine safety are core to Robert F. Kennedy Jr.’s presidential campaign. Citing debunked theories about altered DNA, Florida’s surgeon general has called for a halt to Covid vaccination in the state.
“The sheer nature of misinformation, the scale of misinformation, is staggering, and anything will be twisted to make it seem like it’s not just a devastating side effect but proof of a massive cover-up,” said Dr. Joshua Sharfstein, a vice dean at Johns Hopkins University.
So, get this please, the massive coverup was necessary to debunk '“misinformation” about the existence of a massive coverup. I hope it makes sense to you, my dear reader!They finally note miscarriages caused by COVID vaccines:
Among the hundreds of millions of Americans who were immunized for Covid, some number would have had heart attacks or strokes anyway. Some women would have miscarried. How to distinguish those caused by the vaccine from those that are coincidences? The only way to resolve the question is intense research.
Another way to get the alarm signal of miscarriages is to ask, why does the Moderna vaccine cause 42% more miscarriages, compared to the Pfizer vaccine:
Why Now?
Are we observing a paradoxical awakening of honesty among federal officials and vaccine researchers? Have Apoorva Mandavilli and her employer finally decided to come clean about Covid vaccines?Did these dishonest people suddenly straighten their ways, after being paid millions in research grants, CDC vaccine promotion fees paid to the media, etc? As much as I hope people can improve, I doubt that explanation.
The most likely explanation is that:
- Most vaccine-injured people are Democrats
- Facing a tough election in 2024, the Democratic party is afraid that the victims of vaccines that their party promoted and that disproportionally affected their core voters, might divert their votes and vote for an anti-vax Democrat, Robert Kennedy.
Igor’s NewsletterRasmussen Survey on Covid Vaccine Deaths Proves Antivaxxers Right!Dear paid subscribers: I want to THANK YOU for your paid subscriptions. Thanks to your generous payments, I am not only reporting on the public part of the Rasmussen vaccine report that was just published, but I also could report on the PAID-ONLY Platinum part…Read morea year ago · 680 likes · 621 comments · Igor Chudov
That might explain a puzzling turnaround in reporting vaccine injury in major newspapers such as the New York Times.
Do you have any other explanation? Please share your opinion in the comments.
Why I Have Not Posted Much Recently
I apologize to my readers for a lower post volume last month. There are several reasons, and I must explain them.I am experiencing discomfort and cognitive dissonance about where I am finding myself.
The Covid pandemic is experiencing a lull. Vaccinations are no longer mandatory. The people who continue to harm themselves with Covid vaccines, for the most part, are not the people I deeply care about. Let them take as many shots as they want!
The lab origin of Sars-Cov-2 has become common knowledge, to the point that discussing it is almost redundant. The general public is aware that the people who made the virus and the vaccine are mostly the same people.
The World Economic Forum, always a source of amazing conspiracies it was promulgating, has wisened up and publishes mostly utterly boring, trivial articles on its public website, which I still peruse daily in hopes of finding something newsworthy, with less success than before.
So, naturally, I and many other commentators have fewer topics coming up that are worth discussing.
As a result, the anti-COVID-19 vaccine community, fighting for the declining attention of still-interested readers, has deteriorated. I am deeply embarrassed by some people (I will not name them) posting outright garbage just to stay relevant.
Even though I always try to make posts based on solidly confirmed public information or good research studies, I occasionally ask myself if I am one of them. What topics should I discuss on my blog? What would be good subjects about which I know enough, that are compatible with my values and would be interesting to my readers?
This is further exacerbated by some doubts about my foundational beliefs. I followed a variety of “conservative commentators” and Twitter accounts, many pseudonymous. I slowly recognized that their posts consistently upset me more than they enlightened me.
For example, while I have serious phobias regarding some sexual minorities, I realized that one thing I dislike even more than certain sexual behaviors is people posting about those minorities and their behaviors incessantly. Are the various gross and disgusting videos purposely selected to anger readers published for my benefit? Or are they simply monetizing emotions? Who pays them, and are their sponsors wishing their readers well? Who benefits from whipping up anger and division?
I have to ask, do people who engage in private sexual behaviors that make me deeply insecure, deserve equality and respect despite my discomfort? (yes they do)
I love money and my Substack revenue, but I do not love it so much that I start telling falsehoods to “gain market share.” I have a nice net worth and sources of income outside of Substack that make it unnecessary.
I want to continue posting, and I have many ideas. I have to work out my concerns, possibly by removing the paid option entirely so that the money does not unduly influence me. Worrying about revenue stands in the way of free thinking. I am very thankful to my paid readers, whom I love, and yet, I want to be sure that I am free of unavoidable, perverse financial incentives.
I hope you understand, and again, I am sorry about my two-week silence.
What do you think?
Last edited:
Heliobas Disciple
TB Fanatic
Do we still believe that everyone who had a Covid vaxx is likely to die within 5 years (would be 2026)? I've known many who have had the vaxx and though some have had some serious health issues, they are doing pretty well now and seem to be on the road to good health. A few had clots and blockage but after heart stents are doing very well. One had cancer but seems to have beaten that. Others have not had health issues at all!
Have opinions in the know changed on this at all?
Edit to add - don't get me wrong. I've known some people who were vaxxed and died from fast acting cancers (a few weeks) and some who passed away within 7 months of getting their vaxx - no idea of cause. So I am not blind but I just wonder if we can breathe about our loved ones yet.
Good question.
I certainly hope not. And in my personal opinion, no they won't. I think while Dolores Cahill and others were rightfully concerned at the time their worst fears will not be realized. I think those who were going to die from the vaccine already did. But I will readily admit my thinking is influenced by my hope (like you, most of my loved ones are vaxxed) and that I do not have the scientific background or expertise someone like Dr. Cahill has. I would love to see a follow up interview with her done in 2024 to see if HER predictions have changed.
Now, whether or not the vaxxed will more vulnerable to a covid mutation not as yet seen, as predicted by Geert Vanden Bossche, or to some other Disease X that may come down the pike, that is still open but I pray that's not the case either. Or the case for the unvaxxed. Let's hope we all have stronger immune systems for anything that may be thrown at us.
HD