Public health and national defense experts worry the next pandemic will come at an even higher price than this one. And the nation needs to be ready.

news.yahoo.com
(fair use applies)
As COVID turns 3, experts worry where the next pandemic will come from – and if we'll be ready
Karen Weintraub, USA TODAY
Wed, January 4, 2023, 12:28 PM EST
For years, public health experts warned of the possibility of an illness spreading across the globe and killing millions. After all, it had happened before.
Measures were in place around the world to spot early signs of a never-before-seen bug with dangerous potential.
That's why on Dec. 31, 2019, China notified the World Health Organization that a novel pathogen was circulating in Wuhan, the most populous city in central China. A day later, in that city of 12 million, a wet market selling live animals was shuttered because of fears it was the source of the virus that would later be named SARS-CoV-2.
Three years later, the risk of a deadly pathogen spreading around the world remains.
Now, in addition to worrying about a virus that might jump from animals to humans, experts are concerned about research accidents and – what should be unthinkable – the possibility of someone intentionally unleashing a highly contagious and lethal pathogen.
A pandemic has long been known to be far riskier for global security than conventional, nuclear or chemical warfare, said Lawrence Gostin, a professor of public health law at Georgetown University and a leading expert in global health.
"We've seen that play out with COVID, and COVID is far from the worst pandemic threat that we face," he said.
Although COVID-19 has killed more than 6.6 million people worldwide, other pandemics have been more lethal. The 1918 flu is estimated to have cost 50 million lives across the globe, and in the 14th century, the Black Death killed 30% to 60% of all Europeans in just four years.
Public health and national defense experts worry the next pandemic will come at an even higher price than this one. And they say the nation needs to be ready.
"It's incumbent on the United States and other countries to be prepared for whatever comes from biology, whether it's from nature or from engineering or a laboratory accident," said Dr. Tom Inglesby, director of the Johns Hopkins Center for Health Security at the Bloomberg School of Public Health.
The next pandemic could be worse
Gostin sees nature as the most likely source of the next pandemic. A highly lethal strain of bird or swine flu could mutate naturally to become contagious to humans. That scenario kept health experts like Gostin awake at night long before COVID-19.
But other causes are possible.
"We have a whole host of threats from lab leaks to bioterror to bioweapons to naturally occurring zoonotic spillovers," said Gostin, author of the 2021 book "Global Health Security: A Blueprint for the Future."
"All of that leads to quite a high probability that we're going to have more frequent pandemic-like threats and we need to take them seriously as a national security threat."
The SARS-CoV-2 virus is the third coronavirus to pose a major health threat, following the first SARS and Middle East respiratory syndrome – both of which are far more lethal. Another coronavirus with the contagious potential of SARS-CoV-2 and the 30% death rate of MERS would threaten the economy, supply chains and the health care system, not to mention human life.
And those are just the direct consequences.
With COVID-19, we're likely to see indirect effects for years as people who skipped routine medical care are diagnosed with more advanced and deadlier cancers and children who missed routine vaccines fall ill with preventable diseases, among other consequences, Gostin said.
"If you think of a far worse pandemic, you can multiply that by ten- or even fiftyfold in terms of the economic and social harms the United States would suffer," he said.
That means the world needs to have a better capacity to fight such threats, not spending money only after the crisis arrives, he and others said.
Right now, only about 5% of the country's health care dollars are spent on public health and preventing the next crisis. "That's a rounding error in the U.S. budget," Gostin said.
The idea of engineering a deadly pathogen that sickens the world sounds like the stuff of science fiction or superhero movies. But it's no longer a fantasy.
Kevin Esvelt, an MIT biologist, said people in his own lab could theoretically assemble a dangerous virus from DNA ordered on the internet for under $1,000.
Once pandemic-capable viruses are identified, thousands of people worldwide have the scientific training to make them from mail-ordered synthetic DNA.
"Imagine a world where you can order weapons-grade plutonium in the mail," he said, "and there are thousands of engineers who have the skills to put together something that might be a bomb."
In less than 100 days last fall and winter, the omicron coronavirus variant spread from southern Africa to the rest of the world, infecting 26% of Americans, Esvelt said, illustrating how fast a pandemic response needs to be.
Esvelt warned Congress earlier this year that pandemic virus identification would make pandemics widely accessible and recently released a 30-page plan preparing for a world in which it's feasible to unleash one.
The risk is real and growing over time as engineering biology becomes easier, said Jaime Yassif, vice president of the Nuclear Threat Initiative's Global Biological Policy and Programs. Still, it's not "trivial to create a biological weapon that would cause significant harm," she said.
COVID-19 made the threat more real, she and others said, by showing how much chaos a global pandemic can sow.
"Some people may have taken note of the impact and paid more attention than before," Yassif said. "It's reasonable to assume that the intentions are already there and they may be growing, and that capabilities are increasingly within reach. That's my rational calculus about why I take it seriously."
The potential for bioterrorism
The global Biological Weapons Convention was enacted in March 1975 to prevent countries from ever developing or producing biological weapons. It has largely held ever since, though a few countries that signed on to the treaty are believed to have or have had secret programs.
The Soviets once tried to engineer Ebola into a more contagious pathogen, for instance, but it didn't work well, said Christine Parthemore, CEO of the Council on Strategic Risks, a nonprofit, nonpartisan security policy institute.
China and Iran may have come right up to the line, if not crossed it, making offensive weapons, she said. Based on U.S. government public assessments, for example, Iran may be using "botulinum toxin that we don't think is for Botox, at least not solely."
"The history is there," Parthemore said. "Countries have engineered pathogens."
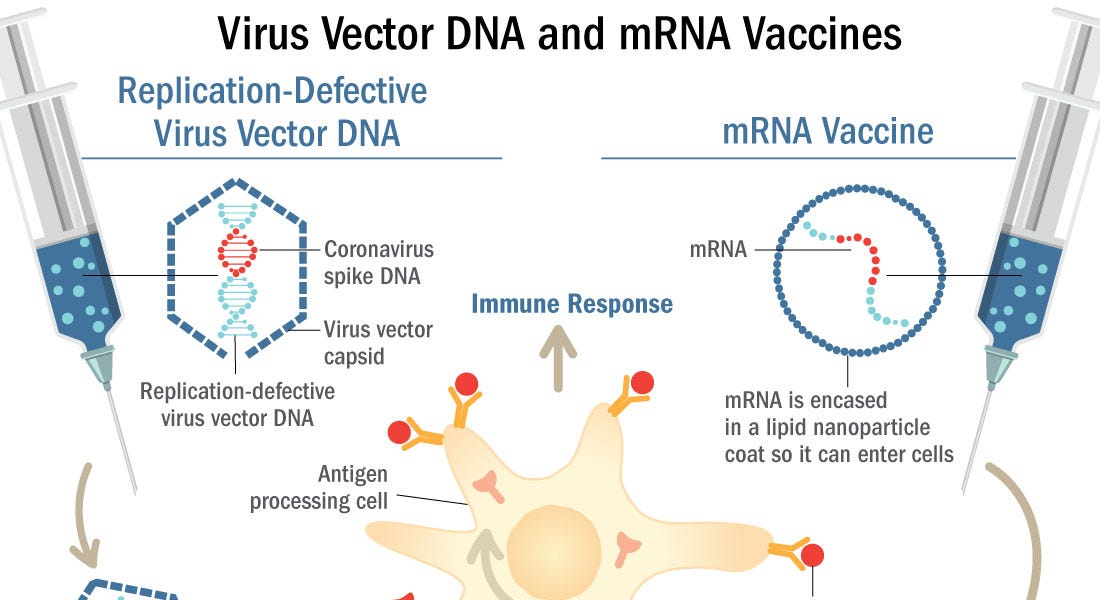
The Defense Department initially became interested in mRNA vaccines, which were used to fight COVID-19, as a rapid way to counter state-based biological threats and engineered pathogens, she said.
And the vaccine that proved effective this summer against mpox (formerly known as monkeypox) was developed to counter the possibility that someone might try to unleash its deadlier cousin smallpox on the world.
But the vast majority of countries are unlikely to try to unleash a deadly pathogen, she said, because it would be hard to protect their own people during a massive outbreak.
Still, Parthemore worries nations are losing faith in international institutions and treaties. Russia's war against Ukraine and the United Nations' inability to stop it have weakened international agreements in the eyes of many nations, including those focused on biosecurity.
"The loss of faith in cooperation and the U.N. and collective action and Russia and others acting as they have further degrading the norms we've held onto so dearly for decades – it's pretty scary," she said.
Should research be regulated?
One question is how much regulation should be imposed on scientific work and researchers involved in synthesizing potential pathogens.
Yassif supports "more rules of the road" to safeguard the scientific advances that might be misused by bad actors.
In 2012, the scientific community and others debated research in the U.S. and the Netherlands that explored five mutations making avian influenza more contagious to humans. Some in the virology community defended that research as essential for understanding naturally emerging risks. Yassif and others worry it made creating a global hazard one step easier.
"The systems we have in place are not as broad in scope or as robust as they need to be," Yassif said.
The construction of new biosafety labs also has raised concerns among experts.
Since the start of the COVID-19 pandemic, more than a dozen countries have announced plans to build Level 4 labs, the highest level of security, designed to investigate the most dangerous pathogens.
These labs lack strong international oversight, Parthemore said. "Obviously, if you had an offensive program and you were trying to engineer pathogens in certain ways, a BSL-4 laboratory is where you would do the work," she said. "The lack of transparency in these labs and their proliferation is a huge problem."
It's also too easy to order the building blocks of a pathogen on the internet, Yassif said. Some companies screen orders to make sure they're not selling dangerous DNA sequences to bad actors, but they're not required to do so. "There's probably a sizeable market share that's not being screened, and we're trying to close that gap," she said.
How to prepare for the next one
No single action can reduce the pandemic risk to zero, the experts said.
But there are plenty of options for actions and a "layered defense." Intervening at multiple points in the process a bad actor would use to create a biological weapon will make the world much safer.
Technology can solve the problem created by biology, Esvelt said. He envisions better protective gear, especially for health care and other essential workers, as well as germicidal lights that kill pathogens without harming the people who use the same indoor space. He wants wastewater and air surveillance at airports to detect new pathogens that might have a long incubation period before showing symptoms, as HIV does.
Preparedness isn't just about scientific breakthroughs. It also involves investing in people, said Dr. Raj Panjabi, senior director for global health security and biodefense for the U.S. National Security Council.
For decades, the U.S. has underinvested in those who deliver public and animal health, he said, including epidemiologists, veterinarians, public health nurses and community health workers.
In October, the Biden administration launched what it called a National Biodefense Strategy and Implementation Plan for Countering Biological Threats, Enhancing Pandemic Preparedness, and Achieving Global Health Security.
Panjabi described some of the strategy's goals and timelines in a webinar this fall:
- Testing: Enable testing for a new pathogen within 12 hours, surge testing within a week and pathogen-specific testing within 30 days
- Vaccination: A new vaccine should be developed within 100 days, enough manufactured for the entire U.S. population within 130 days, and for high-risk populations around the world within 200 days.
- Treatment: Drugs should be repurposed within 90 days and new therapeutics developed within 180 days.
"Time is lives in an emergency," he said. "How well we respond depends on how well we prepare."
The administration has asked for $88 billion over the next five years to implement the plan. "Billions to be invested now to save trillions in the future and an incalculable amount of human lives both American and around the world," Panjabi said.
Congress has not yet followed up with enough funding to pursue this agenda.
"It makes no sense that Congress has not taken up the administration’s proposed pandemic preparedness agenda," said Inglesby, who recently co-wrote a proposal for the development of diagnostics in a health emergency. He hopes the money will be allocated soon.
Another disastrous pandemic is not inevitable, he and others said, but prevention requires preparation and forethought.
"Pathogens of various forms are very good at adapting and changing form. But modern science is very good at countering that," Gostin said. "If we're smart and well prepared and invest strongly and robustly in it, we can substantially lower the risk."

 voiceforscienceandsolidarity.substack.com
(fair use applies)
voiceforscienceandsolidarity.substack.com
(fair use applies)