It is possible to get COVID-19 twice and even more than that. Experts explain why coronavirus reinfections happen and how long immune protection via infection really lasts.

www.yahoo.com
(fair use applies)
How Many Times Can You Get COVID-19? Experts Discuss Coronavirus Reinfections
Sarah Jacoby - TODAY
Fri, July 15, 2022, 3:52 PM
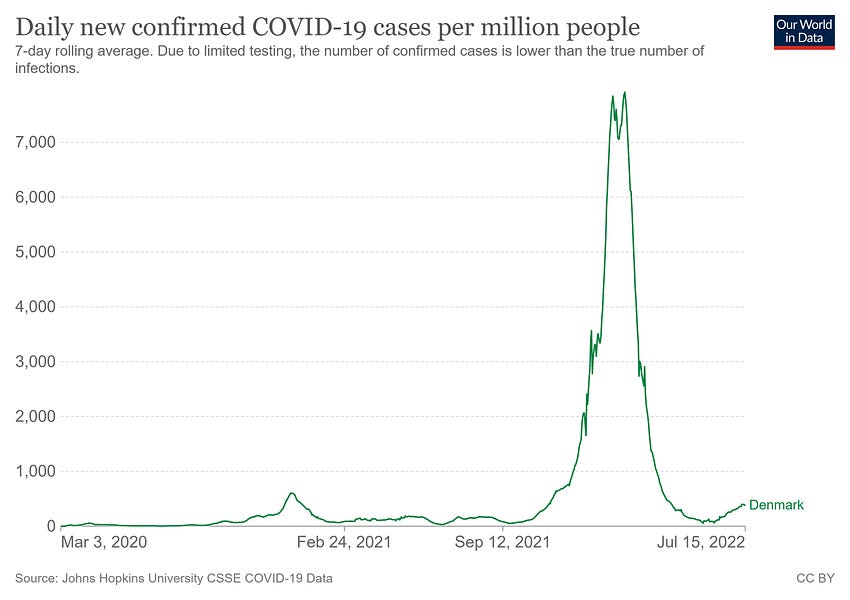
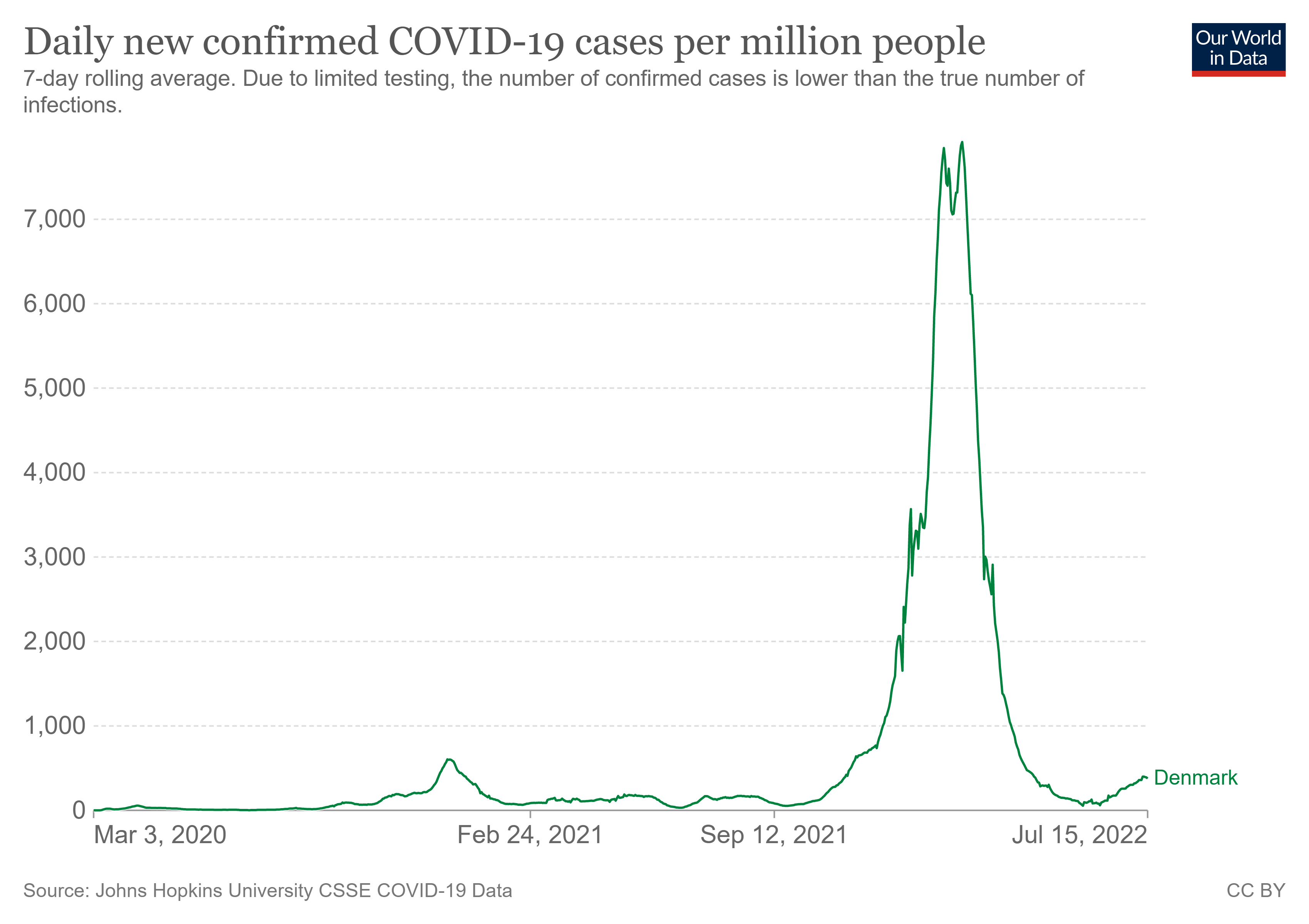
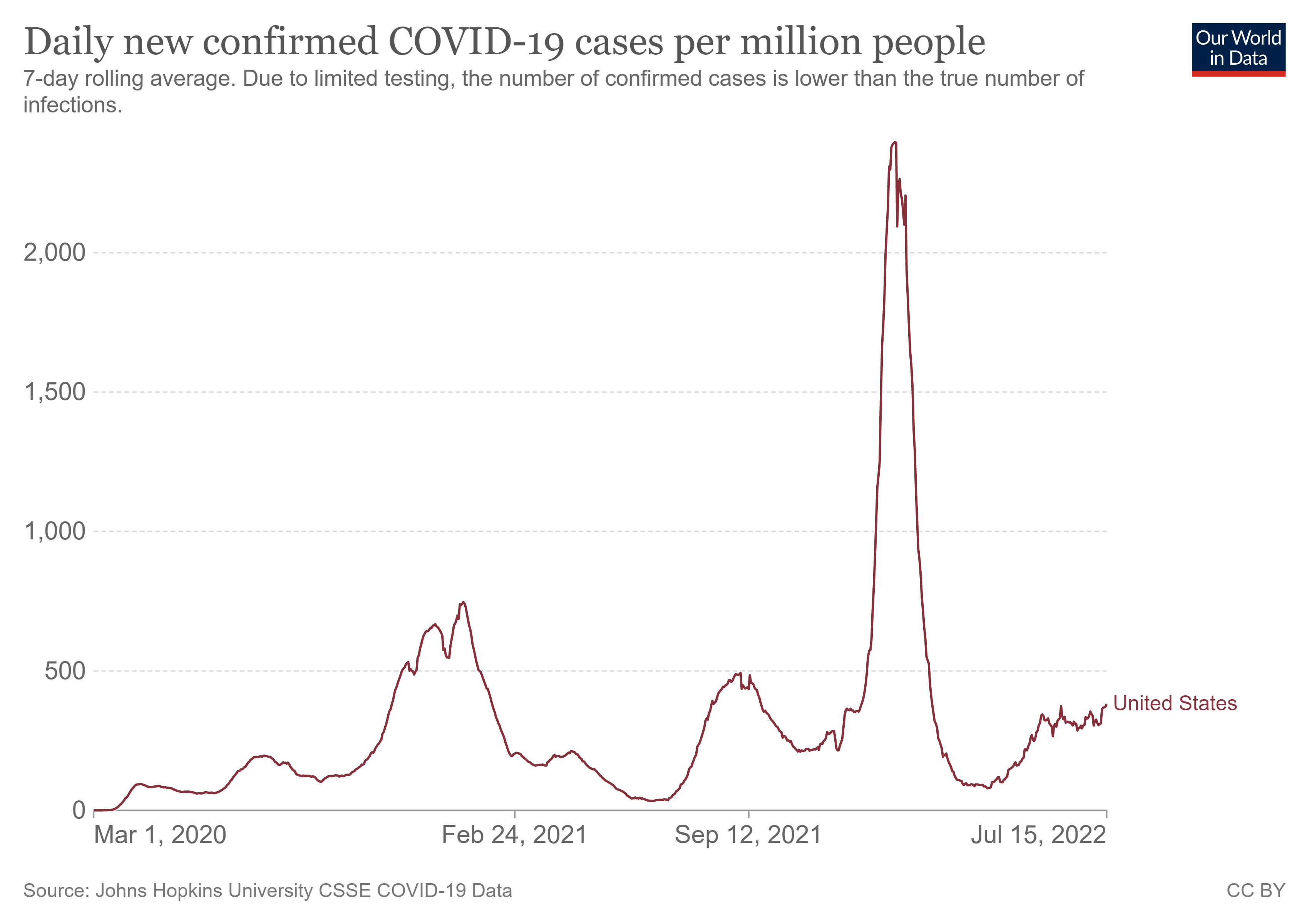
Now in the midst of yet another COVID-19 surge in the U.S., some people may find themselves recovering from a coronavirus infection or even reinfection.
As the virus mutates and your protection from a previous infection wanes, you can be reinfected by the coronavirus. So even if you got sick during the previous delta, omicron or
BA.2 waves, that doesn’t mean you’re immune from the other coronavirus
variants and subvariants that are taking over now.
Right now, the
BA.5 variant is fueling the majority of cases in the U.S., according to data from the
Center for Disease Control and Prevention. But other related variants — including BA.4 and BA.2.12.1 — are still out there.
While getting COVID-19 can provide some protection against a future coronavirus infection for a short time, experts say it's much safer to rely on vaccines and boosters for that protection instead. And if you got COVID-19 previously, you should still get vaccinated to protect yourself and those around you in the future.
Can you get reinfected with the coronavirus?
Yes, it's definitely possible to get COVID-19 more than once.
"Even before the virus started to turn into different variants, even with the original strain that was circulating, there were already
many documented cases of people getting reinfected," Dr. Otto Yang, professor of medicine in the division of infectious diseases and of microbiology, immunology and molecular genetics at the David Geffen School of Medicine at UCLA, told TODAY.
That's not particularly surprising considering that you can be infected and reinfected within a year by pre-COVID coronaviruses that cause the common cold, he said.
As
more variants emerge, including the BA.5 strain, reinfections only become more likely because those variants can potentially evade the immune protection you already have.
"If you had delta, you can get omicron — definitely," Dr. Bernard Camins, medical director for infection prevention at the Mount Sinai Health System, told TODAY. And the reverse is true as well; if you had an infection with the omicron variant, you can still get delta. That's because "the spike protein of the delta variant is very different from the spike protein of omicron," Camins said.
The coronavirus
spike protein is what the virus uses to infect human cells.
Antibodies that you might develop after a previous COVID-19 infection "have to bind to a really specific area of the spike protein to block the virus," Yang explained.
If the spike protein keeps changing in significant ways, antibodies aren't as able to do their jobs to protect you from infection. So, if more coronavirus variants emerge, that makes reinfections more likely.
How many times can you get infected with the coronavirus?
Whether or not you'll be reinfected — and how many times you'll be reinfected — depends on a few factors, Michael Gale, Ph.D., an immunologist at the University of Washington, told TODAY.
The first key is variants. As mutations arise, especially in the coronavirus's spike protein, they can
help the virus evade the natural defenses that the body builds up after an infection. Next is the community level of protection and spread. If the virus is
able to spread widely within a community, there's a better chance you'll be exposed.
But whether the exposure will lead to another infection can come down to individual differences in biology and behavior. Some people naturally develop a more robust response after vaccination or an infection, which will provide more protection down the line, Gale explained.
If it feels like reinfections are becoming more common, there is some data to back that up:
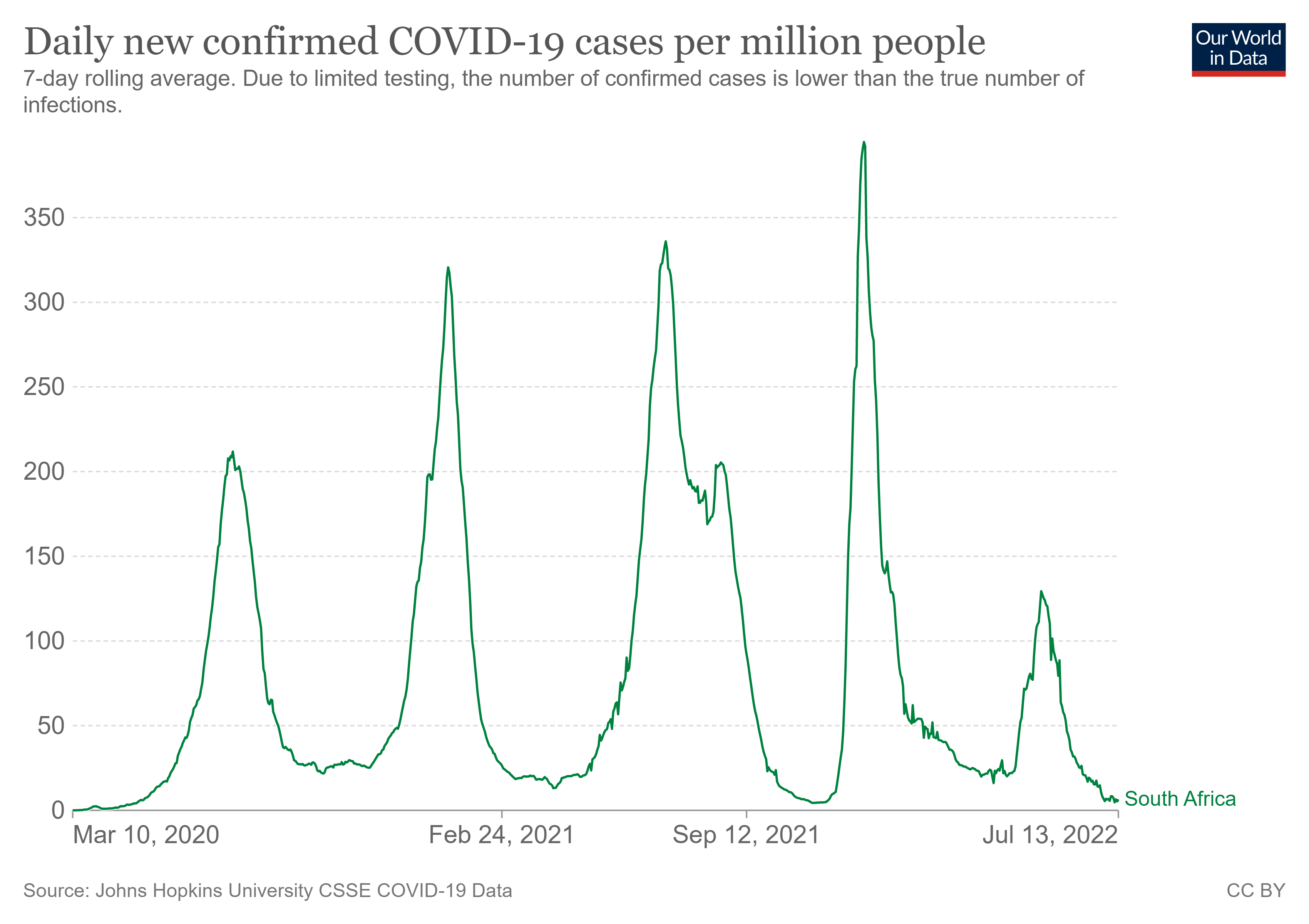
Researchers in South Africa recently found that the omicron wave made reinfections significantly more likely than they were during the previous delta and beta waves. And with new omicron subvariants taking over, reinfections could become even more frequent.
The original omicron variant is similar enough to its subvariants that “immunity to BA.1 might offer you some protection against the others,” Gale said. “But they’re different enough that, depending on the individual, you could also you could get reinfected with a different omicron variant.”
In fact, other recent
research, published to a preprint server, found that it was possible for people get BA.2 infections after an omicron infection — and that the two infections could occur less than 60 days apart. Other research, published in
Nature, found that an omicron infection doesn’t necessarily protect against infections with emerging variants BA.2.12.1, BA.4 or BA.5.
So, will COVID-19 eventually be like the common cold, infecting us multiple times in a year? "It could be, as long as it keeps changing," Gale said.
And we may reach a point where people can get infected within a few weeks rather than months, he said. "It just depends on the individual." Those individual biological and behavioral differences, combined with the dynamics of a virus that's still changing rapidly, may make it possible for some people to become infected more frequently than we're used to.
In fact,
experts told TODAY that the BA.5 variant is better than previous strains at getting around the protection we have from vaccines and past infections. But the norm will likely still be for people to have at least a few months in between infections, they said.
"Typically, it would be a few months as your antibodies from the previous infection start to wane and you get exposed to a new variant," Gale explained. "(At that point), you have lesser antibody protection, and the virus is different enough that it could confer a new infection."
One thing that would help prevent that is for the entire population to develop immunity to omicron, Gale said, ideally through a variant-specific booster or second-generation COVID-19 vaccine. Just last month, the Food and Drug Administration directed manufacturers to include protection against
subvariants BA.4 and BA.5 (along with the original strain) in new COVID-19 vaccines. And the FDA anticipates those new vaccines becoming available in the fall.
We can also continue to use those familiar public health tools (such as vaccines, boosters,
tests and masks) which will prevent infections and
reduce the chances for more variants to develop.
How severe are coronavirus reinfections?
Generally, reinfections are milder than the initial infection regardless of which variants you're infected with, the experts said.
That's partly because, even if your antibodies aren't able to muster enough protection against getting infected, the protection from your T-cells — another
major player in the immune system — will still help protect you from the most severe consequences of the disease even if you get infected, Yang said.
"T-cells are not restricted by recognizing any one area of the spike," he said. "They're not really affected as much or at all by different
variants. They should act just as well
against omicron as against delta as against the prior variants."
But Camins noted that what experts may define as a "mild" infection can still feel subjectively awful — and, of course, cause disruptions in your daily life. "In most cases, the symptoms are less severe, meaning your likelihood of death or severe disease is lower," he said. But if your symptoms cause you to miss work for a prolonged period of time or it takes you a few weeks to recover, "that's still pretty significant" even if it doesn't send you to the hospital.
And there is still the small chance that you may experience severe symptoms or complications — or that you'll spread the virus to someone with a weakened immune system or other underlying condition that puts them at a higher risk.
How long does immunity from a previous COVID-19 infection last?
Having had COVID-19 in the past will protect you to some degree from reinfection in the future. But you may have less protection against other strains of the virus, especially if emerging variants have mutations that make them significantly different from the version you were originally infected with, Gale said.
In general, the experts said that you'll have some protection for about three to six months after a COVID-19 infection. But the protection you’ll get from this type of “natural immunity” can be unpredictable, Yang said, meaning there's no guarantee you won’t be reinfected in this time frame.
People who have more severe bouts of COVID-19, meaning people who were hospitalized, typically end up with more robust protection from the virus, he explained. But on the other hand, that also probably means they have a risk factor that made it more likely for them to get COVID-19 once — and people in that situation really don't want to get it again.
A
CDC study published in November underscores just how much better it is to get protection through vaccination than infection: Among 7,300 patients hospitalized with COVID-like symptoms, those who were unvaccinated but had previously had the illness were five times more likely to
test positive for the infection than those who were vaccinated (and didn't have any record of a previous COVID-19 infection).
Of course, getting that protection via infection also comes with the risks of
long COVID, as well as hospitalization and even death. So, if you had COVID-19 and aren't vaccinated, it's still worth getting the shots to protect you in the future.
What can you do to protect yourself from COVID-19 reinfections?
To prevent COVID-19 reinfections, you can
use the same public health strategies that we know can help prevent an initial coronavirus infection. That includes getting vaccinated and
boosted, wearing a mask in public (especially an
N95 or KN95 respirator, Camins said), getting tested when appropriate and focusing on ventilation.
But some people are more likely to get COVID-19 and therefore to get it more than once. That includes those with certain underlying conditions or who are taking medications that suppress the immune system, such as those with uncontrolled diabetes or autoimmune diseases, as well as those undergoing chemotherapy.
Reducing the amount of the virus that's circulating in your community will keep you and those around you safer, including those who might have risk factors that could make COVID-19 more severe for them.
"It's not necessarily just about you," Yang said. "It may be that you had mild COVID and that if you get infected again, it will be mild COVID. But we should be thinking as a society about everybody."


 www.theepochtimes.com
www.theepochtimes.com


") !
!