Heliobas Disciple
TB Fanatic
Biden's WH calls for a 4th COVID jab; what? a 4th when the 3rd booster FAILS with negative efficacy? where is evidence Mr. POTUS? Has the White House gone nuts? Fire Ashish Jha & Fauci!!! CLUELESS!
Why a 2nd booster shot? Is Fauci insane? I thought he was but now know he is, for there is no evidence for this; the current vaccines do not protect the upper airways and driving variants, severity
Biden's WH calls for a 4th COVID jab; what? a 4th when the 3rd booster FAILS with negative efficacy? where is evidence Mr. POTUS? Has the White House gone nuts? Fire Ashish Jha & Fauci!!! CLUELESS!
Why a 2nd booster shot? Is Fauci insane? I thought he was but now know he is, for there is no evidence for this; the current vaccines do not protect the upper airways and driving variants, severity
Dr. Paul Alexander
17 hr ago
Say NO!!!!!!!!!!!!! No evidence for this, say NO!!!!!!!!!!!!!!!!
Fear porn. That is all it is. Yes, BA.5 is a problem but for the vaccinated. It is the vaccinated that is in trouble due to BA.5 that the vaccine itself due to selection pressure and non-neutralizing antibodies, caused this and more such variants to come. In fact, we predict a severe virulent lethal variant to emerge due to the vaccine.
Where is the data for a 4th shot, a 2nd booster? Where? If something is not working, you do not just do more of it so that it looks like you are doing something. They did same with the failed lockdowns, they did more of it, they hardened it even knowing it was killing people. Same is being done with these injections. At this point, there is no data, no evidence to support these vaccines and the vaccine MUST be stopped.
Moreover, if they went and brought a bi-valent shot as they say in the fall/winter with a Wuhan and omicron spike, this will be even more disastrous for
1) you would be vaccinating into a pandemic a second time with massive infectious pressure of circulating virus
2) you will be again using the failed Wuhan strain that is long gone (a year now it is gone) and not circulating so original antigenic sin will be at play and you will be pressuring the spike antigen driving variants again; the omicron sub-variant BA.5 will likely be gone and displaced and again, you will be vaccinating with a vaccine and content that will mismatch the dominant future variant; antibodies will be to the existing sub-variants when a new variant will likely be dominant; again, with mass vaccination into an ongoing pandemic, you will be driving mounting sub-optimal population immune pressure (with non-neutralizing vaccinal antibodies) as there is concurrent massive infectious pressure. The vaccinal antibodies will be non-neutralizing when they do not match the prevailing variant/clade. Natural selection will play a huge role and the variants that are hardiest and fittest and infectious and which can overcome this sub-optimal non-neutralizing pressure will surmount the vaccinal pressure and become enriched in the environment and become the new dominant, INFECTIOUS variant, and potentially a lethal one.
The FDA’s credibility is now zero! Absolutely zero! Corrupted. Inept. Evidence based medicine (EBM) is also dead. Corrupted. It killed itself over COVID’s grant money. Sold itself out, sadly as I know many of these people and prior to COVID, I thought were principled. Academic research medicine is also dead. I just cannot believe how scientists have stood silent and in many cases joined on in the lies and fraud of COVID, the lockdowns, and this fraud dangerous COVID vaccine. Academic publishing is also dead. Journal editors have zero credibility as corrupted and politicized and biased. They all died over COVID. Over grant money. Yes, they sold us all out.
Our medical doctors are a major part if not the major part with the fraud corrupted disaster of COVID and the response. Of that sordid cabal who sold us out. Doctors should be fired, stripped of licenses, and hang their heads in shame, would be remembered in history for the cowards, the pusillanimous cowards and sell outs they are and were, for going along when they knew and know better. Why? For money, for salary, for grants, for job, when they helped governments enact policies that fired good healthy people and many people and children took their lives in this. They were so destroyed by the losses and the lockdown lunacy and school closures, business closures.
Now, do not forget Gruber and Kraus resigned from the FDA over the political pressure from the White House over boosters.
SOURCE: Two senior FDA officials resign over Biden administration booster shot plan
There is absolutely no basis, no sound justification for a 2nd booster (4th shot). None, and the Biden’s WH knows this but is complicit with the corrupted media in running fear porn stories daily on omicron BA.5 variant. They fail to tell you that it is not the virus but that it is the vaccine that is causing the variants. These COVID injections are non-sterilizing and do not stop transmission and this is critical. They are also harmful. Altarawneh et al.’s study in Qatar below shows us evidence that the boosters have failed e.g. 3rd shot and thus why the need for a 4th when it is likely any antibody protection (if there is any) will wane in a matter of days to a week.
Biden and his White House actually have no data, zero, with which to support a 4th shot. Moreover, these inept NIH and CDC and NIAID and Bourla and Bancel do not seem to understand that the more you vaccinate with a sub-optimal vaccine that they brought, that induces non-neutralizing antibodies, the more you drive selection pressure and infectious variants to emerge. Or do they understand this and are doing this deliberately? I think the latter.
Importantly, the 4th shot will still be based on the initial Wuhan strain that does not hit the omicron sub-variant (antibody dependent enhancement of infection (ADEI), antibody dependent enhancement of disease (ADED) and original antigenic sin (OAS), I call mortal antigenic sin (MAS) all playing a role. This COVID vaccine cannot work and there will be viral immune escape. The vaccinal antibodies from the COVID injections are non-neutralizing and does not sterilize the virus. As said, Original antigenic sin (OAS) will be at play here and the immune response will be to the initial priming, imprinting, prejudicing which is to the Wuhan strain, with no new immune learning to the confronted variant/strain. Thus there will be viral immune escape and there will be as we see now, selection pressure on the spike that drives infectious variant one after the other. As we see, there is antibody dependent enhancement of infection (ADEI). So what is the basis for this 4th shot? Why continue with this vaccine when it is clearly ineffective and not properly safe?
Is this to sell vaccine and get rid of already manufactured vaccine? You do not impose a 4th shot so as to use up the vaccine that is in storage (so it will not expire on your hands), that is stockpiled and no one is taking. You have limited uptake so you are seeking ways to mandate it and force it? This is obscene, for you have no data to support the 4th dose yet you want to approve it to use up your stockpile? You cannot do that without proper trustworthy data and evidence. You have failed to make your case POTUS Biden, and thus this is outrageous. Fauci and Ashish Jha are misleading you and placing you in a terrible situation for a 4th shot will fail and actually cause morbidity and mortality in Americans.
This vaccine does not eliminate the virus and does not stop transmission. It does not work, you will never get to population herd immunity if you cannot cut the chain of transmission. This vaccine does not cut the chain of transmission.
SOURCE:
4th Booster Shot? White House Medical Adviser Dr Fauci Says May Be Needed
Calls for 4th dose of COVID-19 vaccine to protect health-care system
Summer has just begun and already there are signs we may be seeing a new wave of COVID-19 cases. This is prompting calls for fourth doses of the vaccine. Caryn Lieberman reports.
SOURCE:
White House Urges Caution on COVID Variants, Pushes Boosters
Key statements in the Fauci article:
"Immunity wanes, so it is critical to stay up to date with COVID-19 vaccines," he said.
All Americans age 5 and older should get a booster five months after their initial primary series, according to the CDC, and those age 50 and older — or those who are immunocompromised — should get a second booster four months after their first. According to the CDC, tens of millions of eligible Americans haven't received their first booster, and of those older than 50 who got their first booster, only 28% have received their second.
"If you're over 50 and you haven't gotten the shot this year, you should go get a shot," said White House COVID-19 coordinator Dr. Ashish Jha. "It's going to save your life."
So let us look at some evidence by examining the recent Altarawneh et al. Qatar study to help remind POTUS Biden and the two inept technocrats Fauci and Ashish Jha that the COVID injection fails in the 2nd and 3rd (1st booster) shot and as such, why would they think it will be effective for the 2nd booster (4th shot)?
SOURCE:
Altarawneh et al.; Effects of Previous Infection and Vaccination on Symptomatic Omicron Infections
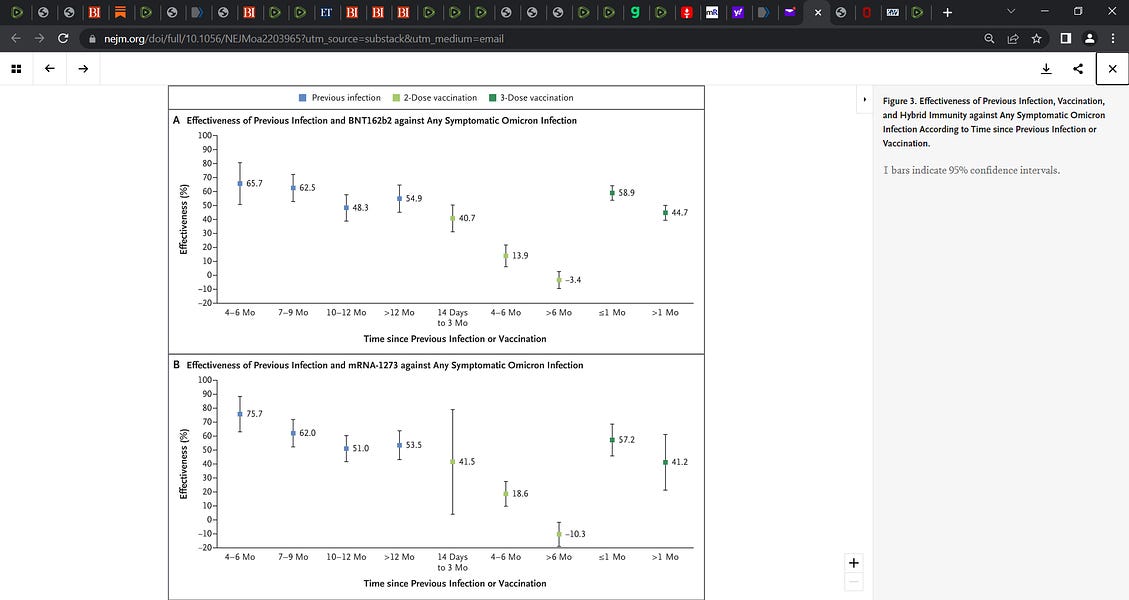
For one, we see the potency of natural immunity from Figure 3 in terms of the protection above vaccinal immunity. We see below in Figure 3 that the mRNA vaccines are (both Pfizer and Moderna) out performed by natural exposure immunity in terms of offering protection. A key to me is that the natural exposure immunity declines much slower than vaccinal immunity and the data shows this clearly.
“Conducted a national, matched, test-negative, case–control study in Qatar from December 23, 2021, through February 21, 2022, to evaluate the effectiveness of vaccination with BNT162b2 (Pfizer–BioNTech) or mRNA-1273 (Moderna), natural immunity due to previous infection with variants other than omicron, and hybrid immunity (previous infection and vaccination) against symptomatic omicron infection and against severe, critical, or fatal coronavirus disease 2019 (Covid-19).”
Key Figure 3 (Pfizer (A) and Moderna (B)):
Figure 3 A Pfizer
Prior infection, protection ranges from 65.7% (4-6 months) to 54.9 >12 months out.
2 dose: protection ranges from 40.7% 14 days to 3 months to -3.4 at > 6 months (falls below 0)
3)3 doses: protection ranges from 58.9 to 44.7
Figure 3 B (Moderna)
Prior infection, protection ranges from 75.7% (4-6 months) to 53.5 >12 months out.
2 dose: protection ranges from 41.5% 14 days to 3 months to -10.3 at > 6 months (falls below 0)
3)3 doses: protection ranges from 57.2 to 41.2
6 months post shot for either mRNA vaccine there is negative effectiveness. We see that the booster for both vaccines, raise the protection above 50% yet at >1 month it falls to 44.7 and 41.2 respectively for Pfizer and Moderna. We see on the other hand, that natural exposure immunity is continuous and stays above 50% even at 12 months onwards.
Authors wrote:
“The analysis of the effectiveness of previous infection, two-dose vaccination, and three-dose vaccination as a function of time since the immunologic event (previous infection or vaccination) showed rapidly waning vaccine protection after the second and third doses but slowly waning protection from previous infection (Figure 3).”
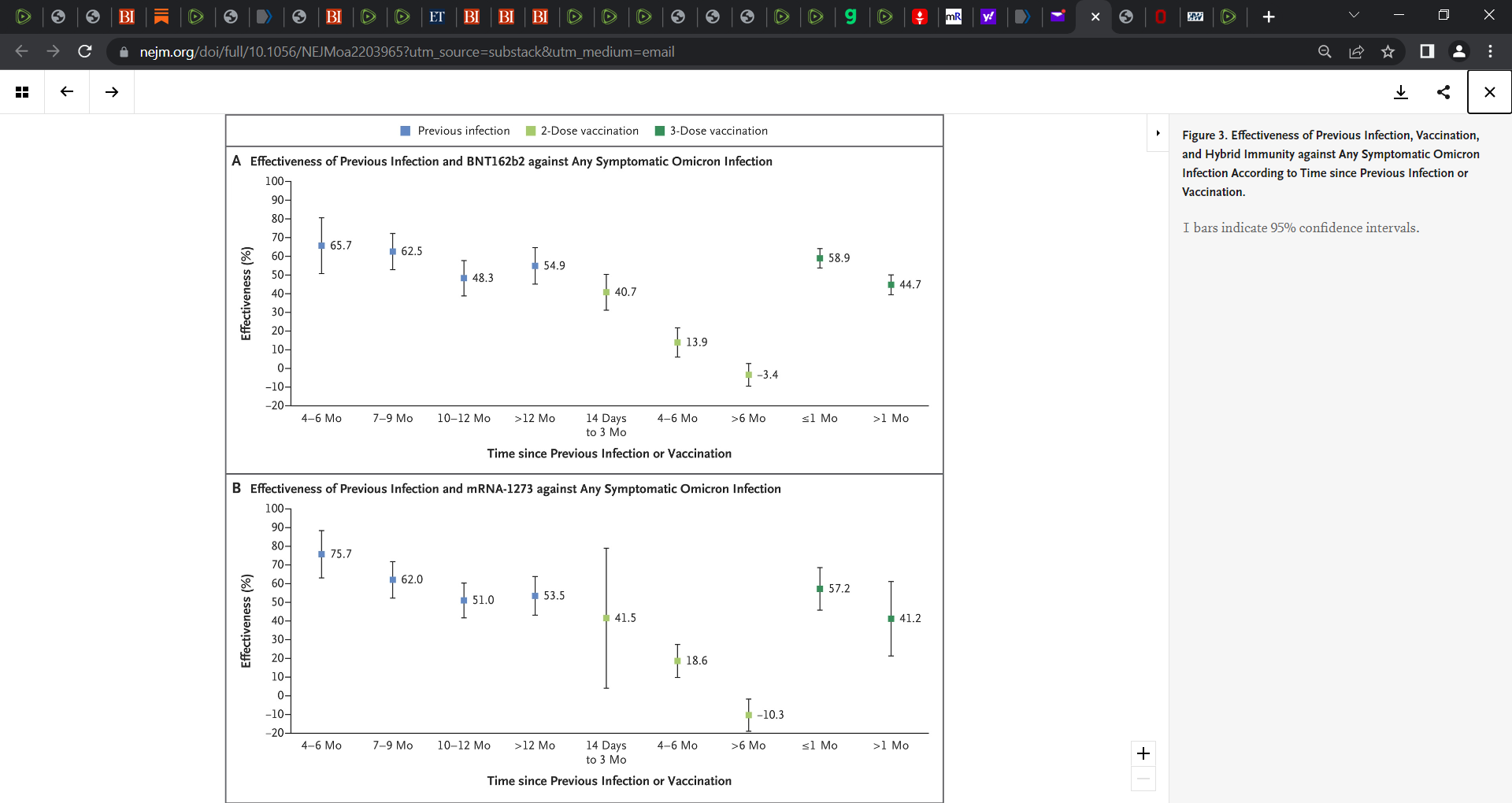
Figure 4 (Moderna):
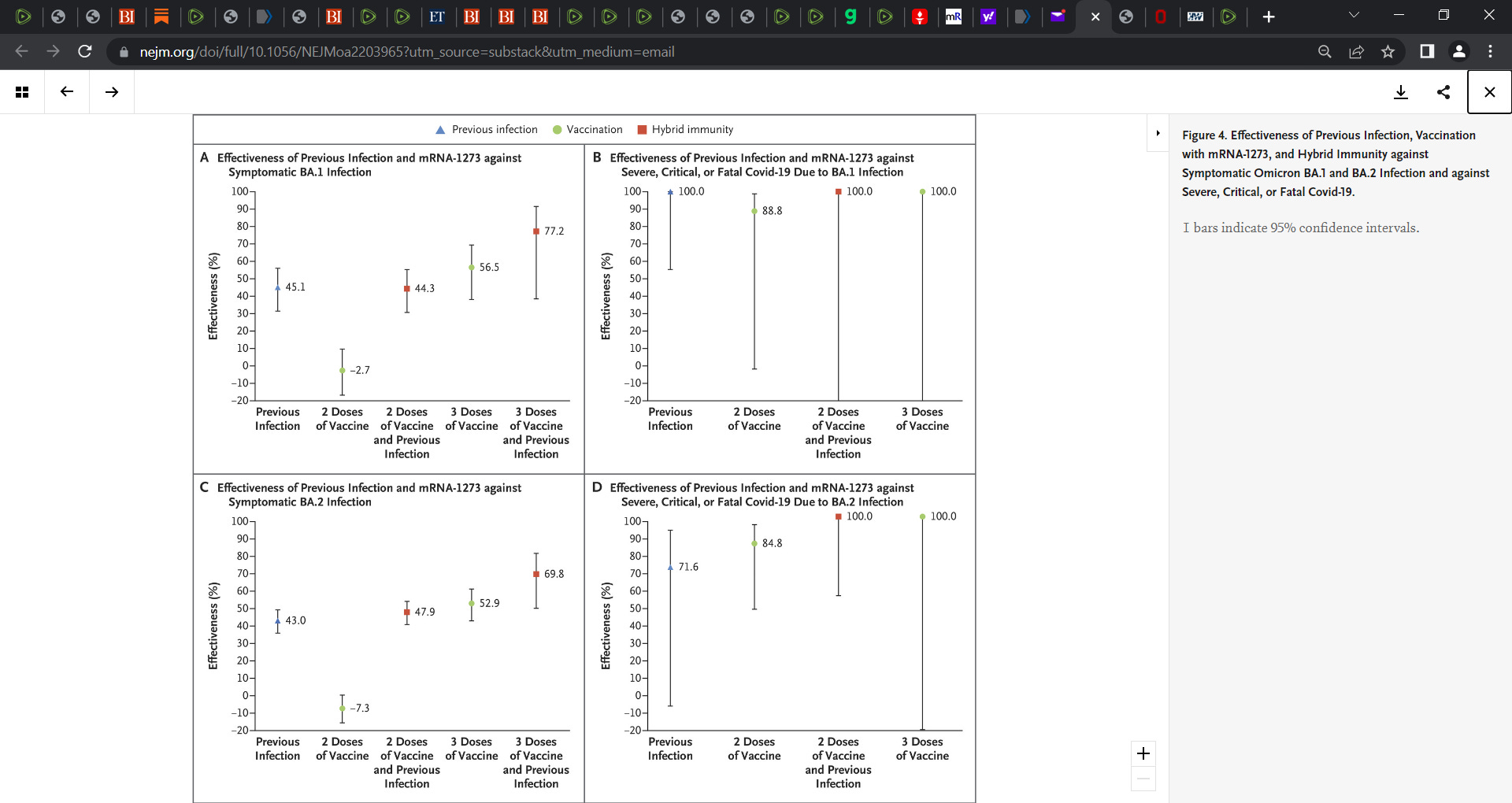
Authors wrote stunningly:
“The protection conferred by hybrid immunity of previous infection and two-dose vaccination was similar to that of previous infection alone, at approximately 50%, which suggests that this protection originated from the previous infection and not from vaccination. This finding is also explained by the short-lived protection of primary-series vaccination against omicron infections.”
Prior pre-print:
Effect of prior infection, vaccination, and hybrid immunity against symptomatic BA.1 and BA.2 Omicron infections and severe COVID-19 in Qatar
BACKGROUND Protection offered by five different forms of immunity, combining natural and vaccine immunity, was investigated against SARS-CoV-2 Omicron symptomatic BA.1 infection, symptomatic BA.2 infection, BA.1 hospitalization and death, and BA.2 hospitalization and death, in Qatar, between...
 www.medrxiv.org
www.medrxiv.org
Makary wrote: “Natural immunity wins again,” Dr. Martin Adel Makary, a public policy researcher at Johns Hopkins University, wrote on Twitter, referring to the Israeli study.
“Among persons who had been previously infected with SARS-CoV-2, protection against reinfection decreased as the time increased,” the authors concluded, “however, this protection was higher” than protection conferred in the same time interval through two doses of the vaccine.”
link: Vaccination Increases Risk of COVID-19 Infection, But Infection Without Vaccination Gives Immunity: Study By Marina Zhang — rupreparing
.









 E-Marie @fiddlestix007
E-Marie @fiddlestix007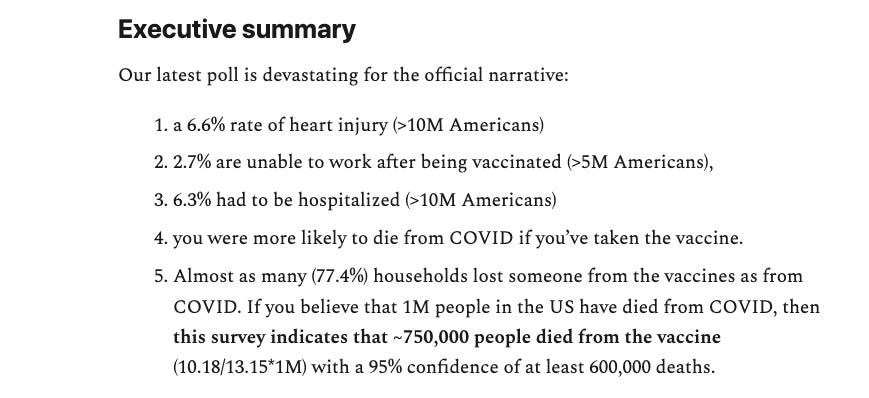
 ⚔Patriot of the North⚔ @patriot_north
⚔Patriot of the North⚔ @patriot_north
 bad cattitude
bad cattitude