
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
CORONA Main Coronavirus thread
- Thread starter Heliobas Disciple
- Start date
-
- Tags
- coronavirus

Zoner
Veteran Member
This U.S. doctor thinks that this pneumonia is something new.
View: https://twitter.com/i/status/1732378727609160116
@mrmickmeThis U.S. doctor thinks that this pneumonia is something new.
View: https://twitter.com/i/status/1732378727609160116
This doctor, just like most of her peers still hasn’t realized that her patients are suffering from a progressively worsening acquired immune deficiency.
jed turtle
a brother in the Lord
Subject: Fwd: Self Assembly Nanotechnology Microplastic Polymers Contributing To Turbo Cancers, Accelerated Aging And All Diseas…
There is much more at the link :(One nice thing we have discovered: fenbendazol
fenbendazole for humans cancer at DuckDuckGo )
From: "Ana Maria Mihalcea, MD, PhD from Humanity United Now - Ana Maria Mihalcea, MD, PhD" <anamihalceamdphd@substack.com>
Much more at link...Subject: Self Assembly Nanotechnology Microplastic Polymers Contributing To Turbo Cancers, Accelerated Aging And All Diseas…
Reply-To: "Ana Maria Mihalcea, MD, PhD from Humanity United Now - Ana Maria Mihalcea, MD, PhD" <reply+2b2bvq&18jevx&&f14859a59b76aef5fab346051b94c80141fb8cd8f1c52ea768a812c89e090d3c@mg1.substack.com>
�:
Microplastic Polymers Contributing To Turbo Cancers, Accelerated Aging And All Diseases

Of course it is amusing hat the “medical freedom movement” is jumping on SV40 contamination as the big story of the day, while ignoring rubbery clots with polyethylene and polyamide signatures, in addition to the revelation about WBAN, brain computer interface, missing mRNA in the shots while toxic heavy metals that are part of semiconducting nanotechnology biosensors are found. They ignore Graphene in Pfizer documents and in scientific investigations of the C19 vials around the world. Additionally, despite extensive talk about Turbo cancers, nobody cares to consider that polymer microplastics are highly inflammatory and carcinogenic.
Legal strategists are claiming that in parliamentary sessions nobody wants to hear about nanotechnology ( well of course not they are part of the deployment of these weapons) and that even judges in courts are not ready to broach the subject. Wait, so the world is not ready to address the number one threat to humanity that is verifiably killing people and modifying the possible survivors into transhuman cyborgs? Who has the authoritiy to make that decision for humanity? When will “they” be ready to discuss it, when the job is done?
Seriously, people would rather have the masses die then address the issues at hand truthfully. That does not project a favorable outcome. People cite the statistics, - NOW we have proof of depopulation! And? Are you just going to watch it happen and keep calculating the numbers while ignoring the real cause?
Microplastics - aka Nanotechnological Self Assembly Polymers - Are Everywhere - Poisoning Our Biosphere, Food Supply And Humans
Here are some review articles about the very polymer plastics I have been writing about and their adverse health effects:
Insights into the potential carcinogenicity of micro- and nano-plastics
The ever-increasing usage of polymer plastics in day-to-day life is a major cause of concern due to their potential implications for human health. The ongoing research efforts suggest that exposure of humans to MNPLs via inhalation and ingestion is inevitable. There is a growing concern in different walks of life regarding the potential of MNPLs as agents increasing the carcinogenic risk in humans. Due to the lack of studies directly evaluating carcinogenic effects, the only way to get some indicative data is the use of surrogate biomarkers. Thus, several in vitro and in vivo studies demonstrated the potential of MNPLs to cause DNA damage, generation of ROS, and inflammatory response suggesting their human health risk.
The epidemiology of increase in early onset colorectal cancer (EOCRC) suggests an environmental driver. This increase in EOCRC matches the time sequence in which we could expect to see an effect of rapid increase of MPs in the environment and, as such, we have explored possible mechanisms for this effect. We suggest that it is possible that the MPs damage the barrier integrity of the colonic mucus layer, thus reducing its protective effect.
The below review article published in 2021 admits that microplastics are in most food, most bottled water and nanoparticles also have been found. This does not take into consideration that these nano and micro plastics also have been utilized in the making of self assembly nanotechnology that continues to indefinitely self replicate for the purpose of total global surveillance. This is called smart dust.
Of course, it is not just the polymers that cause ill health effects like cancer, but also the metal nanoparticles, the smaller the size, the greater the toxicity.

Last edited:
Zoner
Veteran Member

NZ Whistleblower Arrested for Exposing the Truth: Here’s What They Didn’t Want You to See
“There is no chance that this vaccine is not a killer.”
 vigilantnews.com
vigilantnews.com
December 3, 2023
Opinion
NZ Whistleblower Arrested for Exposing the Truth: Here’s What They Didn’t Want You to See
“The data is legit; that's why they are arresting Barry. He's a hero for exposing the truth.”By
The Vigilant Fox
Statistician and whistleblower, Barry Young, also known as “Winston Smith,” 56, has been arrested by New Zealand authorities for exposing a damning database on COVID-19 vaccine deaths. However, the official charge was “dishonestly accessing vaccination data.”

Young, a Ministry of Health employee-turned-whistleblower, was responsible for managing New Zealand’s COVID-19 vaccination database. After discovering some disturbing trends, Young felt compelled to come forward. “I saw too much that I couldn’t do nothing anymore,” he said.
In a long-format interview with Liz Gunn, founder of the New Zealand Loyal Party, on November 30th, Mr. Young presented connections between specific COVID-19 vaccine batches and mortality rates. The data he shared was alarming:
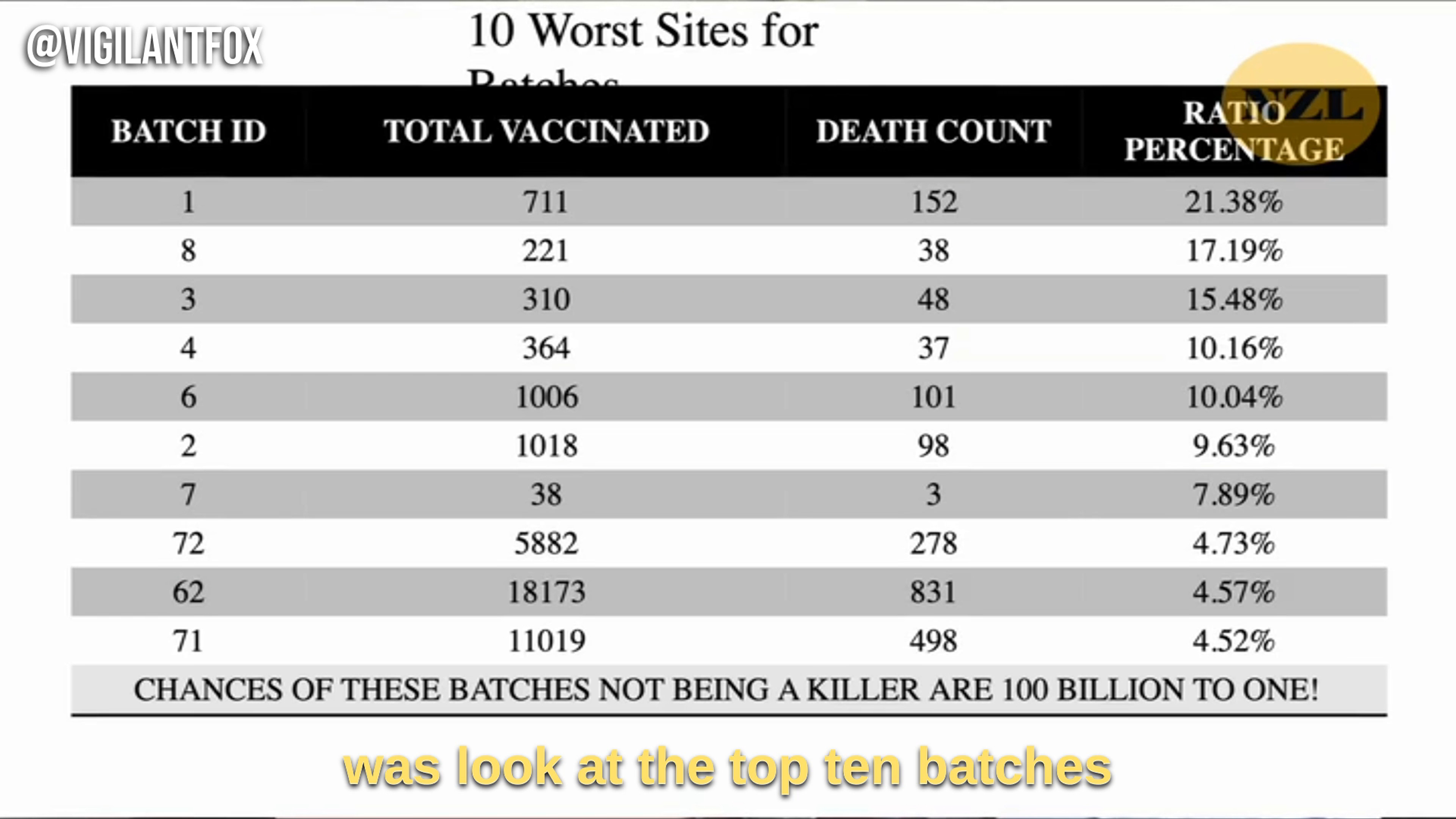
Batch ID 1: Total Vaccinated 711, Death Count 152, 21.38% Dead
Batch ID 8: Total Vaccinated 221, Death Count 38, 17.19% Dead
Batch ID 3: Total Vaccinated 310, Death Count 48, 15.48% Dead
Batch ID 4: Total Vaccinated 364, Death Count 37, 10.16% Dead
Batch ID 6: Total Vaccinated 1006, Death Count 101, 10.04% Dead
Batch ID 2: Total Vaccinated 1018, Death Count 98, 9.63% Dead
Batch ID 7: Total Vaccinated 38, Death Count 3, 7.89% Dead
Batch ID 72: Total Vaccinated 5882, Death Count 278, 4.73% Dead
Batch ID 62: Total Vaccinated 18173, Death Count 831, 4.57% Dead
Batch ID 71: Total Vaccinated 11019, Death Count 498, 4.52% Dead
The underlying mortality rate in New Zealand should be only 0.75%, said Young. He added that these batches were across all age groups, so it should all average out to that 0.75% mortality rate.
At the bottom of the image with the batch data, it says, “Chances of these batches not being a killer are 100 billion to one!” Young clarified what that statement meant, explaining that the odds of death rates this high happening by chance are approximately 100 billion to 1.
“So statistically, what we’re saying is that there is no chance that this vaccine is not a killer,” Young declared.
Heliobas Disciple
TB Fanatic
Thanks Zoner. Here's an interview he just did with Alex Jones. I haven't watched it yet so can't give a summary.
New Zealand COVID Whistleblower Barry Young Interviewed By Alex Jones (and Steve Kirsch)
1 hr 02 min 06 sec
New Zealand COVID Whistleblower Barry Young Interviewed By Alex Jones (and Steve Kirsch)

1 hr 02 min 06 sec
Heliobas Disciple
TB Fanatic

China Approves 5 New COVID-19 Vaccines for ‘Emergency Use’ Amid Worsening Pneumonia Outbreak
While relaunching COVID-19 control measures, Beijing is still reluctant to admit that the country is experiencing a nationwide outbreak.
 www.theepochtimes.com
www.theepochtimes.com
China Approves 5 New COVID-19 Vaccines for ‘Emergency Use’ Amid Worsening Pneumonia Outbreak
While relaunching COVID-19 control measures, Beijing is still reluctant to admit that the country is experiencing a nationwide outbreak.
By Alex Wu
12/6/2023
Five major Chinese pharmaceutical companies recently announced that Beijing approved their newly developed COVID-19 vaccines for “emergency use” amid the fast-worsening pneumonia outbreak in China. Meanwhile, authorities have reinstated COVID-19 control measures, including PCR testing and health codes, in various locations nationwide.
Nevertheless, the ruling Chinese Communist Party’s (CCP) health authorities continue to provide conflicting information regarding the surge in pneumonia infections, particularly among children, since mid-October, refraining from calling it a new COVID-19 outbreak. Experts believe the CCP is once again attempting to conceal information, which is reminiscent of its actions at the onset of the pandemic in late 2019, to safeguard the regime’s political security.
In less than a week, five new coronavirus vaccines have been included for emergency use by governmental departments. The vaccines protect against the subvariants of Omicron XBB—a variant of SARS-CoV-2 (the virus that causes COVID-19)—supposedly causing the epidemic in China, according to various Chinese media reports.
Livzon Pharm and CanSino Biologics announced on Dec. 3 that the new coronavirus vaccines they developed were approved for emergency use.
Watson Biotech and CSPC Pharmaceutical Group issued statements on Dec. 1, confirming that the new coronavirus variant mRNA vaccines they developed had been approved for emergency use by the research and development team of the State Council’s Joint Prevention and Control Mechanism Scientific Research Group.
Shenzhou Cell also announced on the same day that its recombinant new coronavirus Beta/Omicron (BA.1/BQ.1.1/XBB.1) variant S trimer protein vaccine has also been approved by health authorities.
"These newly included COVID-19 vaccines have a common feature: they target XBB mutant strains," Guo Xinfeng, a senior pharmaceutical industry expert, told mainland Chinese media.
He expressed doubt regarding the effectiveness of the new vaccines, saying there is still a risk of a rebound in the COVID-19 epidemic in China this winter.
“According to information disclosed by China’s Center for Disease Control and Prevention, the XBB series of mutant strains are currently prevalent globally and domestically,” Mr. Guo said.
PRC Testing, Health Codes
Patients, predominantly children, infected with the mysterious drug-resistant pneumonia that causes "white lungs," a symptom commonly found in severe COVID-19 cases, continue to overwhelm hospitals across China.
Meanwhile, reports from Chinese media and netizens indicate that in many neighborhoods–including those in Sichuan, Guangzhou, Zhejiang, Hubei, Hebei, Shaanxi, and Tianjin city—authorities have reactivated health codes, which were used to monitor and restrict people’s movements during the regime’s draconian COVID-19 lockdowns.
Furthermore, megacities like Shanghai and Guangzhou have reintroduced PCR testing.
Guangzhou health authorities announced on Dec. 2 that patients must have a green health code to enter all medical facilities in the city. The video of the announcement went viral, sparking public concerns as it harks back to the stringent pandemic controls enforced from late 2019 to December 2022.
Professor Tian Li from Harbin Business School in northern China shared a video on Chinese social media, disclosing that he was required to take a PCR test upon his arrival at the "Understanding China in 2023" international conference in Guangzhou on Dec. 1.
He Xiaopeng, the founder and chairman of Xpeng Motors, shared his experience on Chinese news aggregator Jinri Toutiao or "Today's Headlines" on Dec. 1. He said that when he returned from abroad to attend an international conference in China, he had to undergo a PCR test as soon as he got off the plane in Shanghai. Since the policy for mandatory testing had been lifted, he was puzzled and asked the airport staff why he was tested. He was then told that he was randomly selected. However, he observed that all passengers from the same flight were required to take the PCR test.
An employee at Shanghai Pudong International Airport surnamed Ma told Radio Free Asia on Dec. 4 that many foreign passengers must undergo rapid COVID-19 tests upon arrival.
"At the airport, incoming passengers are said to be randomly checked [for PCR tests]. But I saw that some people and the entire flight were tested for it. Also, a friend of mine flew to Australia yesterday and sprayed that kind of disinfectant [one used during the pandemic] on the plane. It has been a long time since it was sprayed. Health codes in many places have already been relaunched online."
Authorities at Yiwu city—home to Yiwu Market, one of the world's biggest wholesale markets—issued a notice on Dec. 1, advising residents to stock up on food supplies that can last more than 10 days. The notice triggered panic on social media, with residents expressing concern about the prospect of another round of pandemic lockdowns. Although the notice was subsequently removed from the local government's website, it remains accessible through related Chinese media reports and reposts on social media.
Shi Tao, a U.S.-based current affairs commentator, said in his YouTube talk show "Shi Tao Focus" on Dec. 4 that the authorities' recent actions suggest that Beijing is discreetly gearing up for a potential nationwide COVID-19 outbreak and subsequent lockdown.
CCP Downplays Outbreak
As the mysterious pneumonia continues to spread in China, an increasing number of adults have reportedly been infected, including nurses and doctors. Reports indicate that this pneumonia is resistant to drugs, making the antibiotics typically effective against mycoplasma pneumonia ineffective in its treatment.
The CCP's official statements on the outbreak have been contradictory, attributing the disease to influenza, respiratory syncytial virus, rhinovirus, mycoplasma pneumoniae, adenovirus, and cross-infections while downplaying the possibility of a new COVID-19 outbreak.
China’s top diplomat, Wang Yi, said at a United Nations meeting in New York on Nov. 29 that the outbreak in China is a “common phenomenon” and “under effective control.”
Beijing responded to the World Health Organization’s request for data on the outbreak by saying that no “unusual or new pathogens” have been found.
Epoch Times contributor Dr. Dong Yuhong, an infectious disease specialist and scientist, pointed out how the CCP's authoritarian political system influences the management of epidemic information.
“Under the one-party rule of the CCP, the regime controls the flow of information to maintain so-called social stability and its image. Especially under its current leader, Xi Jinping, the response policy to the COVID-19 pandemic initially followed the 'zero-COVID' restrictive control policy for the first three years.
Subsequently, authorities completely reopened the country and halted testing. Over time, the CCP's actions have led to a prolonged cover-up and ongoing outbreaks,” Dr. Dong told the Chinese language edition of The Epoch Times on Dec. 4.
"Disclosing the epidemic data at this point could harm the CCP's international image, triggering demands from the global community and the Chinese population to hold the CCP accountable while causing panic within the leadership," she said.
Dr. Dong emphasized that a continued lack of transparency in information, whether covering up or downplaying the outbreak, may repeat the events seen during the COVID-19 pandemic. This recurrence could result in a new pandemic, she said, which may cause another recession in the slowly recovering global economy.
Fang Xiao and Luo Ya contributed to this report.
Heliobas Disciple
TB Fanatic
(fair use applies)
Latest Actions By China Indicates That A New SARS-CoV-2 Variant Is Possibly Behind The Mysterious White Lung Pneumonia Surge
Nikhil Prasad Fact checked by:Thailand Medical News Team
Dec 07, 2023
China suddenly bringing back mandatory COVID-19 testing and COVID-19 preventive protocols and focusing on COVID-19 is indicting that a new SARS-CoV-2 variant or sub-lineage is behind the surge of “white lung” pneumonia cases
As the world grapples with a new surge of a mysterious white lung pneumonia outbreak that is currently wreaking havoc in China, Netherlands, Denmark and many other geolocations, a perplexing development has emerged in China, raising eyebrows and stirring speculation. In a surprising turn of events, the Chinese government has recently initiated mandatory COVID-19 testing and reinstated a slew of COVID-19 preventive measures in response to the significant surge in cases this mysterious white lung pneumonia. While Chinese health officials initially attributed the surge to known respiratory pathogens such as the RSV virus, influenza virus, and mycoplasma pneumoniae, there is a growing concern and speculation that new variants of the SARS-CoV-2 virus may be contributing to the sudden increase.
Reports from local residents and official government directives suggest a marked resumption of COVID-19 testing across the country, not only in healthcare facilities but also in transportation hubs. The revival of COVID-19 prevention protocols, including the use of tracking apps, further fuels suspicions that the surge in mysterious white lung pneumonia cases may be linked to the emergence of new SARS-CoV-2 variants and sub-lineages.
The State Council, in a directive has ordered local authorities to intensify testing and disease monitoring at key points, including ports, airports, schools, care homes, and other institutions. The directive underscores the need for strengthened prevention and control measures in various settings, urging daily protection and health monitoring to curb the potential spread of respiratory diseases.
Other COVID-19 News coverages have also validated that China is restarting all COVID-19 prevention protocols and testing.
China restarts COVID-19 testing in hospitals, airports
Amidst these developments, unconfirmed reports circulating on social media suggest the resurrection of the notorious "Health Code" COVID-19 tracker app, which was previously employed to enforce stringent quarantine measures. Beijing residents have reported instances of free COVID-19 testing at prominent locations such as railway stations, international airports, and conference venues, signaling a coordinated effort to encourage public cooperation.
Interestingly, at various hospitals across the provinces in China, there is no longer the requirement for laboratory testing for mycoplasma pneumoniae or RSV virus for anyone with pneumonia-like symptoms. Rather COVID-19 testing involving a change to the primers used in the PCR test are being utilized.
Such a move indicates that a new SARS-CoV-2 variant or sub-lineages is likely involved but a gain Chinese authorities are not divulging any reasons behind their recent moves and actions.
While official statements downplay the role of novel pathogens and emphasize a cocktail of known respiratory illnesses as the cause of the surge, some residents express confusion and concern. A Beijing resident, who sought emergency treatment for their child, reported being advised to undergo a nucleic acid test for COVID-19 according to his post on a social media platform. Speculations regarding a mutated strain of the virus are circulating, prompting questions about transparency in the government's reporting.
Adding to the complexity of the situation, the Ministry of Education issued a directive on December 4, calling on schools nationwide to take proactive measures to mitigate the potential impact of a "winter disease," specifically naming COVID-19. The directive acknowledges the ongoing global pandemic and the continuous mutation of the virus, warning of potential superimposed epidemics of multiple respiratory diseases in the coming winter and spring.
Health officials are advising the public to adhere to preventive measures such as wearing masks, practicing hand hygiene, and ensuring proper ventilation to curb the spread of respiratory diseases. Residents report a palpable sense that the government fears a resurgence of the coronavirus, as many cases of pneumonia and respiratory diseases exhibit symptoms strikingly similar to COVID-19.
The situation takes an intriguing turn as social media posts surface regarding the 2023 China Textile Industry Federation Science and Technology Awards Conference, scheduled for December 6 in Beijing. Participants are allegedly required to present a negative COVID-19 test dated the day before the conference, underscoring the seriousness of the situation and the government's proactive approach.
Residents in various regions, including Hunan's provincial capital Changsha, are anticipating a renewed focus on COVID-19 testing. A kindergarten principal in Shaoyang expressed concern over a high number of sick children, revealing that a significant portion of students was absent due to illness.
Reports are also emerging that China is possibly going to reintroduce lockdowns to prevent the spared of the disease and to contain it. Already reports have emerged that the government is asking people to store on food supplies and essential consumer products.

 www.thailandmedical.news
www.thailandmedical.news
This development triggers memories of the initial waves of the Omicron variant, where an estimated 2 million people lost their lives after the lifting of restrictions under China's "zero-COVID" policy. As the Chinese government navigates this challenging situation, concerns are growing among the public about the potential for stricter measures, including the dreaded possibility of another lockdown.
Some researchers are speculating that new SARS-CoV-2 hybrids involving the BA.2.86 variant could be behind the surge in pneumonia cases while others argue that it could involve the emergence of a new SARS-CoV-2 reassortant strain involving another virus. With genomic surveillance extremely low globally, such developments would be of no surprise.
The resumption of COVID-19 testing and the reinforcement of preventive measures in China spotlight the delicate balance that governments worldwide must strike between managing public health and sustaining economic activities. The surge in mysterious white lung pneumonia cases underscores the ever-evolving nature of the COVID-19 pandemic, with new variants and sub-lineages posing continuous challenges to health systems globally.
Despite the uncertainty surrounding the exact cause of the surge, the Chinese government's proactive response indicates a commitment to staying ahead of the curve in terms of virus surveillance and containment. However, as the situation unfolds, transparency and clear communication from authorities will be crucial in maintaining public trust and cooperation.
As the world watches China's response to this latest development, it serves as a stark reminder that the fight against COVID-19 is far from over, requiring continued vigilance, adaptability, and international collaboration to navigate the complexities posed by emerging variants and potential resurgences of the virus.
Latest Actions By China Indicates That A New SARS-CoV-2 Variant Is Possibly Behind The Mysterious White Lung Pneumonia Surge
Nikhil Prasad Fact checked by:Thailand Medical News Team
Dec 07, 2023
China suddenly bringing back mandatory COVID-19 testing and COVID-19 preventive protocols and focusing on COVID-19 is indicting that a new SARS-CoV-2 variant or sub-lineage is behind the surge of “white lung” pneumonia cases
As the world grapples with a new surge of a mysterious white lung pneumonia outbreak that is currently wreaking havoc in China, Netherlands, Denmark and many other geolocations, a perplexing development has emerged in China, raising eyebrows and stirring speculation. In a surprising turn of events, the Chinese government has recently initiated mandatory COVID-19 testing and reinstated a slew of COVID-19 preventive measures in response to the significant surge in cases this mysterious white lung pneumonia. While Chinese health officials initially attributed the surge to known respiratory pathogens such as the RSV virus, influenza virus, and mycoplasma pneumoniae, there is a growing concern and speculation that new variants of the SARS-CoV-2 virus may be contributing to the sudden increase.
Reports from local residents and official government directives suggest a marked resumption of COVID-19 testing across the country, not only in healthcare facilities but also in transportation hubs. The revival of COVID-19 prevention protocols, including the use of tracking apps, further fuels suspicions that the surge in mysterious white lung pneumonia cases may be linked to the emergence of new SARS-CoV-2 variants and sub-lineages.
The State Council, in a directive has ordered local authorities to intensify testing and disease monitoring at key points, including ports, airports, schools, care homes, and other institutions. The directive underscores the need for strengthened prevention and control measures in various settings, urging daily protection and health monitoring to curb the potential spread of respiratory diseases.
Other COVID-19 News coverages have also validated that China is restarting all COVID-19 prevention protocols and testing.
China restarts COVID-19 testing in hospitals, airports
Amidst these developments, unconfirmed reports circulating on social media suggest the resurrection of the notorious "Health Code" COVID-19 tracker app, which was previously employed to enforce stringent quarantine measures. Beijing residents have reported instances of free COVID-19 testing at prominent locations such as railway stations, international airports, and conference venues, signaling a coordinated effort to encourage public cooperation.
Interestingly, at various hospitals across the provinces in China, there is no longer the requirement for laboratory testing for mycoplasma pneumoniae or RSV virus for anyone with pneumonia-like symptoms. Rather COVID-19 testing involving a change to the primers used in the PCR test are being utilized.
Such a move indicates that a new SARS-CoV-2 variant or sub-lineages is likely involved but a gain Chinese authorities are not divulging any reasons behind their recent moves and actions.
While official statements downplay the role of novel pathogens and emphasize a cocktail of known respiratory illnesses as the cause of the surge, some residents express confusion and concern. A Beijing resident, who sought emergency treatment for their child, reported being advised to undergo a nucleic acid test for COVID-19 according to his post on a social media platform. Speculations regarding a mutated strain of the virus are circulating, prompting questions about transparency in the government's reporting.
Adding to the complexity of the situation, the Ministry of Education issued a directive on December 4, calling on schools nationwide to take proactive measures to mitigate the potential impact of a "winter disease," specifically naming COVID-19. The directive acknowledges the ongoing global pandemic and the continuous mutation of the virus, warning of potential superimposed epidemics of multiple respiratory diseases in the coming winter and spring.
Health officials are advising the public to adhere to preventive measures such as wearing masks, practicing hand hygiene, and ensuring proper ventilation to curb the spread of respiratory diseases. Residents report a palpable sense that the government fears a resurgence of the coronavirus, as many cases of pneumonia and respiratory diseases exhibit symptoms strikingly similar to COVID-19.
The situation takes an intriguing turn as social media posts surface regarding the 2023 China Textile Industry Federation Science and Technology Awards Conference, scheduled for December 6 in Beijing. Participants are allegedly required to present a negative COVID-19 test dated the day before the conference, underscoring the seriousness of the situation and the government's proactive approach.
Residents in various regions, including Hunan's provincial capital Changsha, are anticipating a renewed focus on COVID-19 testing. A kindergarten principal in Shaoyang expressed concern over a high number of sick children, revealing that a significant portion of students was absent due to illness.
Reports are also emerging that China is possibly going to reintroduce lockdowns to prevent the spared of the disease and to contain it. Already reports have emerged that the government is asking people to store on food supplies and essential consumer products.
Medical News: Mysterious White Lung Pneumonia Spreads To Indonesia! China Planning Lockdowns! - Thailand Medical News
Medical News: In a concerning turn of events, the Indonesian capital, Jakarta, has reported cases of a mysterious white lung pneumonia, suspected to be linked to Mycoplasma pneumoniae. The outbreak comes just days after the Health Ministry's call for increased surveillance against this...
www.thailandmedical.news
This development triggers memories of the initial waves of the Omicron variant, where an estimated 2 million people lost their lives after the lifting of restrictions under China's "zero-COVID" policy. As the Chinese government navigates this challenging situation, concerns are growing among the public about the potential for stricter measures, including the dreaded possibility of another lockdown.
Some researchers are speculating that new SARS-CoV-2 hybrids involving the BA.2.86 variant could be behind the surge in pneumonia cases while others argue that it could involve the emergence of a new SARS-CoV-2 reassortant strain involving another virus. With genomic surveillance extremely low globally, such developments would be of no surprise.
The resumption of COVID-19 testing and the reinforcement of preventive measures in China spotlight the delicate balance that governments worldwide must strike between managing public health and sustaining economic activities. The surge in mysterious white lung pneumonia cases underscores the ever-evolving nature of the COVID-19 pandemic, with new variants and sub-lineages posing continuous challenges to health systems globally.
Despite the uncertainty surrounding the exact cause of the surge, the Chinese government's proactive response indicates a commitment to staying ahead of the curve in terms of virus surveillance and containment. However, as the situation unfolds, transparency and clear communication from authorities will be crucial in maintaining public trust and cooperation.
As the world watches China's response to this latest development, it serves as a stark reminder that the fight against COVID-19 is far from over, requiring continued vigilance, adaptability, and international collaboration to navigate the complexities posed by emerging variants and potential resurgences of the virus.
Zoner
Veteran Member
@RealCheckMarker
#mycoplasma are also very common bacteria which can lurk in the gut biome until activated by a virus like SARS, capable of bacteriophage.
@mrmickme
Once you can understand this one salient fact, you’ll understand why an enteric variant like JN.1 is leading to a global surge of stuff like m.pneumonia in its wake.
#mycoplasma are also very common bacteria which can lurk in the gut biome until activated by a virus like SARS, capable of bacteriophage.
@mrmickme
Once you can understand this one salient fact, you’ll understand why an enteric variant like JN.1 is leading to a global surge of stuff like m.pneumonia in its wake.
naegling62
Veteran Member

Unanticipated Complications with mRNA Vaccine
The principle of the unknown unknowns comes to bear with this paper. It seems the Pfizer vaccine can cause formation of abnormal proteins, not anticipated by...
 www.youtube.com
www.youtube.com
Very interesting on the mechanics of how the mRNA is supposed to make the protein and the mistakes that the Pfizer vaccine is making. I highly recommend.
RT 18:51
Heliobas Disciple
TB Fanatic

The Updated COVID-19 Shot Works on the Newest Variants
A new study shows that the XBB vaccine can protect against several emerging variants.
The Updated COVID-19 Shot Works on the Newest Variants
Alice Park - TIME
Thu, December 7, 2023, 3:42 PM EST
Every COVID-19 vaccine is a step behind the virus. In the time it takes companies to make the shot, SARS-CoV-2 is already busy mutating into different versions that can evade the immune response produced by it.
But even though the latest vaccine targets XBB.1.5, a variant no longer dominant in the U.S., it seems to be doing a decent job at warding off some of the emerging variants. In a study published on the preprint server bioRxiv, scientists led by Dr. David Ho, director of the Aaron Diamond AIDS Research Center at Columbia University, report that the vaccine can generate strong antibodies that can neutralize not just XBB but variants such as HV.1, which now accounts for 31% of U.S. infections, and HK.3, which contributes to half of new infections in Asia (and about 7% in the U.S.).
The team analyzed blood samples from 60 people with different COVID-19 infection and vaccination histories, representing real-world scenarios. All had four to five doses of mRNA vaccines—most recently, the bivalent BA.4/5 vaccine that was recommended before the new XBB.1.5 shot. One group had never had COVID-19 and received the XBB.1.5 booster. Another group recently recovered from an XBB infection and did not receive the XBB booster. The final group had previously been infected with an Omicron variant and did not receive the XBB.1.5 booster. Blood samples from these volunteers were pitted against lab-based versions of SARS-CoV-2 virus variants: the original, BA.5, XBB.1.5, and EG.5.1 (a variant that spread widely this fall). The samples were also tested against four emerging subvariants: HV.1, HK.3, JD.1.1, and JN.1.
The results suggest that the new XBB.1.5 vaccine helps generate antibodies against variants that the vaccine wasn’t specifically designed to target—namely HV.1, HK.3, JD.1.1, and JN.1. These antibody levels were 13 to 27 times higher in the blood of people who had never had COVID-19 but had an XBB.1.5 vaccine. They increased 10-fold among people with this new shot who had a prior Omicron infection. These responses were slightly lower than antibody levels generated against XBB.1.5, but still suggest that the latest vaccine can provide broader protection against a variety of variants.
That’s encouraging news as the battle between vaccines and the virus continues this season, and new variants that first appeared in other parts of the world make their way to the U.S. These new data support the need for people stay up to date on their vaccines so they can continue to be protected against new versions of the virus.
Heliobas Disciple
TB Fanatic

Getting Sick All the Time? Don't (Necessarily) Blame COVID-19
Are you more likely to get sick after having COVID-19?
Getting Sick All the Time? Don't (Necessarily) Blame COVID-19
Jamie Ducharme - TIME
Thu, December 7, 2023, 2:51 PM EST
Respiratory disease season is in full swing, with influenza, RSV, and COVID-19 case counts rising in various parts of the U.S. Hospitals in some states are also reporting upticks in pediatric pneumonia diagnoses, which experts say seems to be unrelated to the recent spike of pneumonias reported in China.
On the heels of last year’s severe flu and RSV reason, all this contagion has some people wondering if SARS-CoV-2, the virus that causes COVID-19, may be to blame. Some studies suggest the virus leaves its mark on the immune system even after an acute illness passes, raising an important question: does having COVID-19 increase your risk of getting sick from other viruses in the future?
“Any time that we get an infection, it changes us,” says Dr. David Smith, chief of infectious diseases and global public health at UC San Diego Health. “It changes our B cells, which make antibodies, and it changes our T cells, which do cellular functions to clear out infections.”
Sometimes, these changes can be long-lasting. After a case of chickenpox, for example, the body typically builds lifelong immunity that prevents future bouts of the illness. But other viruses have more insidious effects. Measles essentially forces the body to re-learn how to fend off other infections, research shows, while HIV leaves people severely immunocompromised.
SARS-CoV-2 seems to fall somewhere between those two poles, though Smith emphasizes that research is ongoing. Reinfections are not only possible but common, ruling out the idea of widespread lifelong immunity—but there also isn’t currently evidence to suggest COVID-19 is causing population-wide immune deficiency, says Sheena Cruickshank, a professor of immunology at the University of Manchester in the U.K.
Some studies do, however, suggest that SARS-CoV-2 infections—particularly severe ones—can trigger changes to the immune system, including reductions in the number and performance of T cells; disruptions to B cells; deficiencies in dendritic cells, which regulate the immune response; and altered gene expression linked to increased inflammation. Some of these changes seem to last months after a serious case of COVID-19.
Scary as those findings sound, however, “you may see a gazillion changes, but you don’t know which of those changes may be relevant to future function,” says John Tsang, a professor of immunobiology at the Yale School of Medicine. In other words: changes to specific immune cells don’t necessarily mean that the whole system, or even part of it, will stop working.
It’s normal for immune markers to “ebb and flow” after an infection, Cruickshank adds, and even changes that sound bad won’t necessarily have long-lasting implications. “Studies that have looked more long-term have shown that, for most people, the immune response bounces back to normal and restores,” Cruickshank says. In one study co-authored by Tsang, men who recovered from mild COVID-19 actually mounted stronger immune responses to flu vaccines than men who had never had COVID-19, which could be beneficial. (Tsang and his co-authors didn’t observe the same trend in women.)
There are exceptions, though. People who have severe cases of COVID-19 may experience lasting health problems, either from the virus itself or from certain drugs used to treat serious COVID-19, such as steroids and immune-system modulators, Smith says. Many scientists also think that chronic Long COVID symptoms could be a sign of immune dysfunction, and recent research suggests people with Long COVID are more likely to get reinfected by SARS-CoV-2 than people who fully recover.
For people who had mild cases and no long-lasting symptoms, though, Tsang says the scientific literature does not support the idea of widespread immunosuppression after COVID-19. So why does it seem that people are getting sick more often now than before the pandemic?
There’s always the chance that COVID-19 is causing immune changes that haven’t shown up in the research yet, says Katelyn Jetelina, an epidemiologist who devoted a recent edition of her newsletter to COVID-19’s impact on the immune system. But she feels it’s likelier that people are simply more attuned to any respiratory symptoms they experience than they were a few years ago.
It’s also possible, Tsang adds, that the same revved-up immune response that COVID-19 survivors in his study mounted in response to the flu vaccine leads some people to experience more severe symptoms of common illnesses. “We may feel a bit sicker because of the inflammatory response,” Tsang says, “but it’s not because our system now no longer responds to an infection.”
Several years of decreased exposure to pathogens due to masking and social distancing may also have changed disease-transmission patterns, Cruickshank says. Children who were born during the pandemic may not have been exposed to germs they typically would have encountered as babies, leaving them to catch those bugs for the first time as toddlers or young kids. And even adults who'd had multiple prior brushes with common cold or flu viruses may now be faced with new strains of those viruses, to which their bodies are less familiar, Cruickshank says.
None of this is to say that COVID-19 is harmless. It is still a leading cause of death in the U.S.; Long COVID remains a serious risk; and there’s evidence that even seemingly mild infections can affect the heart, brain, and other organs. Avoiding the SARS-CoV-2 virus is still the safest move for your health—regardless of how it affects your risk of getting sick in the future.
Heliobas Disciple
TB Fanatic

Defense bill orders Pentagon to review reinstatement of troops fired for COVID-19 refusal
Congress, in a draft version of the annual defense bill, has directed the Pentagon to review the reinstatement of U.S. troops who were discharged for refusing the COVID-19 vaccine. The provision is included in the compromise version of the National Defense Authorization Act (NDAA), reached by...
Defense bill orders Pentagon to review reinstatement of troops fired for COVID-19 refusal
Brad Dress - The Hill
Thu, December 7, 2023, 1:30 PM EST
Congress, in a draft version of the annual defense bill, has directed the Pentagon to review the reinstatement of U.S. troops who were discharged for refusing the COVID-19 vaccine.
The provision is included in the compromise version of the National Defense Authorization Act (NDAA), reached by negotiators in the Democratic-controlled Senate and Republican-controlled House and released Thursday.
The NDAA orders the Defense Department to consider reinstatement at the request of a service member who was discharged and, if reinstated, should define the period of the individual’s time away from service as a period of inactivation.
The Senate added a secondary provision that requires those seeking reinstatement to have before submitted a request for a religious, administrative or medical exemption.
Lawmakers also included an amendment to create an investigatory board that will review cases of service members who were discharged for refusing the COVID-19 vaccine.
Other amendments require the Pentagon to communicate the path to be reinstated to COVID-related discharged troops and the Defense Department to conduct a study of potential health consequences to service members who got the vaccine.
The COVID-19 provisions were a priority for House Republicans, who had pushed back against American troops being let go for refusing the vaccine.
Last year’s NDAA forced the Pentagon to rescind a COVID-19 vaccine mandate that had been in place but did not touch on reinstatement, setting up this year’s clash.
The mandate had covered the entire armed forces, including the National Guard and Reserve, and troops who did not comply faced a range of punishments, including a loss of days accrued toward retirement, loss of pay and dismissal.
Heliobas Disciple
TB Fanatic

Florida Surgeon General Demands Answers After 'DNA Fragments' Found in COVID Shots
www.theepochtimes.com
Florida Surgeon General Demands Answers After 'DNA Fragments' Found in COVID Shots
By Caden Pearson
12/7/2023
Florida Surgeon General Dr. Joseph Ladapo on Wednesday demanded federal health officials shed light on the discovery of DNA fragments in the Pfizer and Moderna COVID-19 mRNA vaccines "hitchhiking into human cells."
In a letter, Dr. Ladapo asked Dr. Robert M. Califf, commissioner of the U.S. Food and Drug Administration (FDA), to address the findings by researchers. Dr. Mandy Cohen, director of the Centers for Disease Control and Prevention (CDC), was also included in the letter.
"I am writing to you to address the recent discovery of host cell DNA fragments within the Pfizer and Moderna COVID-19 mRNA vaccines," Dr. Ladapo wrote in his letter.
Of particular concern, he noted, was the "presence of nucleic acid contaminants" in the approved monovalent and bivalent mRNA jabs, which were detected "in the presence of lipid nanoparticle complexes, and Simian Virus 40 (SV40) promoter/enhancer DNA."
"Lipid nanoparticles are an efficient vehicle for delivery of the mRNA in the COVID-19 vaccines into human cells, and may therefore be an equally efficient vehicle for delivering contaminant DNA into human cells," he noted. "The presence of SV40 promoter/enhancer DNA may also pose a unique and heightened risk of DNA integration into host cells."
Major Risks
Dr. Ladapo has raised several concerns with the FDA, the federal agency responsible for approving the shots, and the CDC over COVID-19 vaccines and criticized the rollout of shots in September, saying there weren't sufficient clinical trials. Earlier this year, he raised the alarm with the FDA about Florida observing a 4,400 percent increase in reports of life-threatening conditions since the rollout of the mRNA COVID-19 vaccines.
Citing FDA guidance from 2007, Dr. Ladapo noted in his Dec. 6 letter the potential risks associated with DNA integration. He emphasized the need for a comprehensive assessment of the risks of contaminant DNA integration into human DNA, particularly given the wide biodistribution of mRNA COVID-19 vaccines.
Per FDA guidance, there are three significant potential risks associated with DNA integration, including impacts on human oncogenes, chromosomal instability, and certain body parts.
"DNA integration could theoretically impact a human’s oncogenes—the genes which can transform a healthy cell into a cancerous cell," Dr. Ladapo noted.
"DNA integration may result in chromosomal instability," his second point noted. Furthermore, the FDA's guidance discusses the integration of the biodistribution of DNA vaccines, which "could affect unintended parts of the body, including blood, heart, brain, liver, kidney, bone marrow, ovaries/testes, lung, draining lymph nodes, spleen, the site of administration, and subcutis at injection site."
Demanding Answers
Citing the recent detection of DNA fragments in the vaccines, the FDA's 2007 guidance, and the efficacy of the COVID-19 mRNA vaccine’s lipid nanoparticle delivery system, the Florida surgeon general posed three crucial questions to the FDA commissioner:
- Have drug manufacturers evaluated the risk of human genome integration or mutagenesis of residual DNA contaminants from the mRNA COVID-19 vaccines alongside the additional risk of DNA integration from the lipid nanoparticle delivery system and SV40 promoter/enhancer? Has FDA inquired any information from the drug manufacturers to investigate such risk?
- Do current FDA standards for acceptable and safe quantity of residual DNA (present as known contaminants in biological therapies) consider the lipid nanoparticle delivery system for the mRNA COVID-19 vaccines?
- Considering the potentially wide biodistribution of mRNA COVID-19 vaccines and DNA contaminants beyond the local injection site, have you evaluated the risk of DNA integration in reproductive cells with respect to the lipid nanoparticle delivery system?
Dr. Ladapo noted that Dr. Califf and then-CDC Director Dr. Rochelle Walensky had not responded to a previous letter dated Nov. 19, in which he accused the health officials of ignoring several risks surrounding the mRNA COVID-19 vaccines.
"The American people and the scientific community have a right to have all relevant information pertaining to the COVID-19 vaccines to properly inform individual decision-making," Dr. Ladapo wrote.
Noting the "urgency of these questions due to the mass administration" of COVID-19 mRNA shots, he demanded a written response by Dec. 13, addressing the concerns he raised in both his Dec. 6 and Nov. 19 letters.
"If he doesn't have answers, who gave him the right to treat human beings as guinea pigs?" the Florida surgeon general said in a post on X, referring to Dr. Califf.
A spokesperson from the FDA said the agency "has received the letter and will respond directly to the Florida Surgeon General."
This report was updated with the FDA's comment.
LINK TO THE LETTER:
Heliobas Disciple
TB Fanatic
In the kingdom of the blind, the one-eyed is king...
I have no choice, but to react to E. Topol’s latest substack: From a Detour to Global Dominance - by Eric Topol (substack.com) Can you believe this??? These esteemed scientists seem unaware that what they are looking at in their in vitro neutralization assays are ‘pseudo’neutralizing antibodies...
In the kingdom of the blind, the one-eyed is king...
Geert Vanden Bossche
Dec 6, 2023
I have no choice, but to react to E. Topol’s latest substack: From a Detour to Global Dominance - by Eric Topol (substack.com) [*see next post for the substack Geert is referring to]
Can you believe this??? These esteemed scientists seem unaware that what they are looking at in their in vitro neutralization assays are ‘pseudo’neutralizing antibodies (Abs) that merely accelerate viral immune escape. Did you notice how the D614G Abs remained at high levels, while antibodies to Omicron variants plummeted significantly prior to the boost? I bet that that the pseudoneutralizing Abs decreased in just a few weeks after the XBB.1.5 boost, but they are not showing us these data. Nor are they showing us results from Elisa Ab assays! Elisa assays could expose the mismatch and unveil an unprecedented lack of correlation between the results from their alleged 'neutralization' assay and those obtained in an Elisa assay.
‘Pseudo’neutralization occurs when the once-neutralizing Abs are boosted due to vaccine breakthrough infection (VBTI) caused by circulating variants that have largely evaded the protective neutralizing Abs induced by Covid-19 (C-19) vaccines. Boosting results in a significant increase in the titer of these Abs, which therefore acquire the capacity to hinder viral infection by hydrophilizing virus-Ab complexes. However, due to their low binding affinity, especially after maturation into isotype-switched IgG4 Abs, these Abs will rapidly lose their infection-inhibiting (i.e., ‘pseudo’neutralizing) capacity, thereby exerting large-scale suboptimal immune pressure on viral infectiousness in highly C-19 vaccinated populations. This collective immune pressure contributes to the co-emergence and co-circulation of new immune escape variants, which are currently causing large-scale repeated VBTIs in highly C-19 vaccinated populations. The latter are mostly accompanied by (very) mild to moderate symptoms. However, VBTIs, by fostering immune refocusing, fuel the emergence of new, even more infectious immune escape variants. This has now resulted in a scenario where large, poorly solubilized/ hydrophilized virus-Ab aggregates undergo enhanced uptake into antigen-presenting cells (APCs), thereby triggering strong activation of cytotoxic T lymphocytes (CTLs). While strongly activated CTLs substantially reduce viral shedding, viral transmission persists due to a combined enhancement of intrinsic viral infectiousness and a higher incidence of mild/ asymptomatic infection (equally mediated via enhanced CTL activity). Under these circumstances, achieving herd immunity becomes unattainable. On the contrary, as described in my previous substack (Ah, if only they understood the difference between herd immunity and herd immune pressure…..), there is compelling evidence from virological, immunological, and clinical perspectives that this pandemic continues to evolve in a manner beyond control.
Topol openly admits (as also D. Barouch did several months ago) that they don't comprehend how the Abs are still exhibiting neutralizing effects (E. Topol: ‘this is damn lucky’).
How can they accept this lack of understanding? It's like accepting a death sentence.
Death rates in Finland (with a full vaccination rate: 78.5%) appear to be increasing in tandem with the rise in JN.1 throughout Scandinavia. However, regardless of whether the rising hospitalization and mortality rates are still primarily due to non-Covid-19 excess hospitalizations and deaths[1] or to JN.1 already evolving towards a more virulent behavior in C-19 vaccinees, the ignorance and naïve optimism of Topol’s ‘highly regarded labs’ are equally worrisome (as both phenomena underlie the same cause1)! All their hope now solely relies on 'pseudo'neutralization, but that hope will rapidly vanish when clinics eventually reveal the truth….
[1] As previously clarified (What's driving turbo cancers and autoimmune flare-ups? | Voice for Science and Solidarity), these excess hospitalization and death rates are likely caused by immune refocusing. This phenomenon is also responsible for large-scale immune escape, stemming from mRNA vaccination and VBTIs, predominantly caused by Omicron and its descendants.
Heliobas Disciple
TB Fanatic
From a Detour to Global Dominance
The rise of the JN.1 variant
Eric Topol
Dec 5, 2023
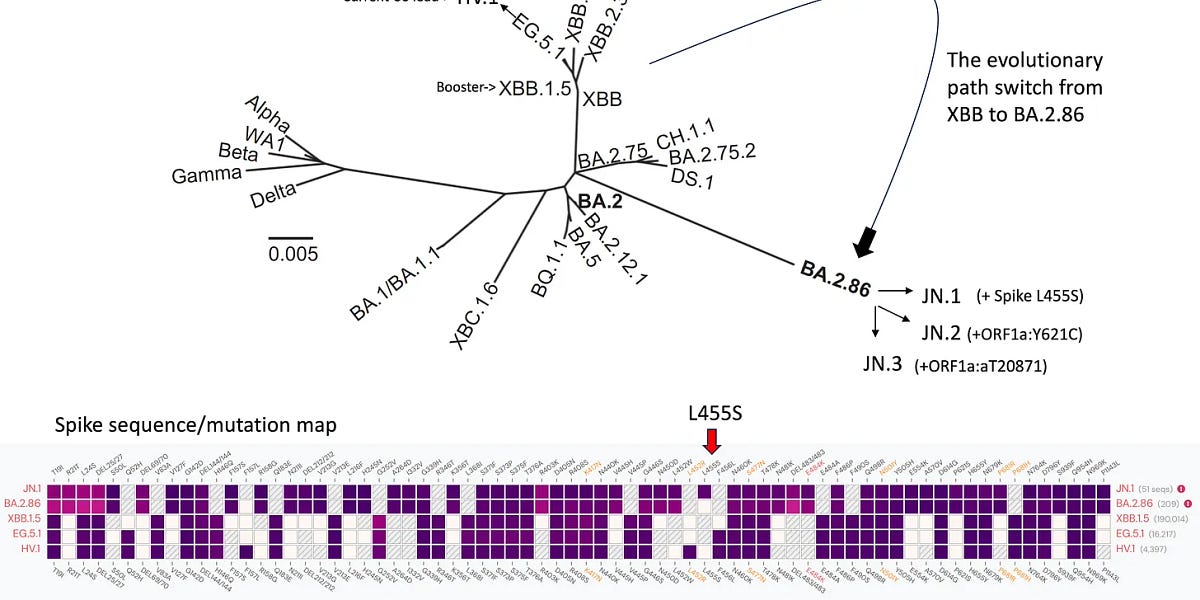
In October, I wrote about a major detour in the evolutionary arc of the SARS-CoV-2 virus, from a series of recombinants known as the XBBs over a year to BA.2.86, a descendant of an early Omicron (BA.2), and its derivative JN.1 which added a pivotal spike mutation (L455S).
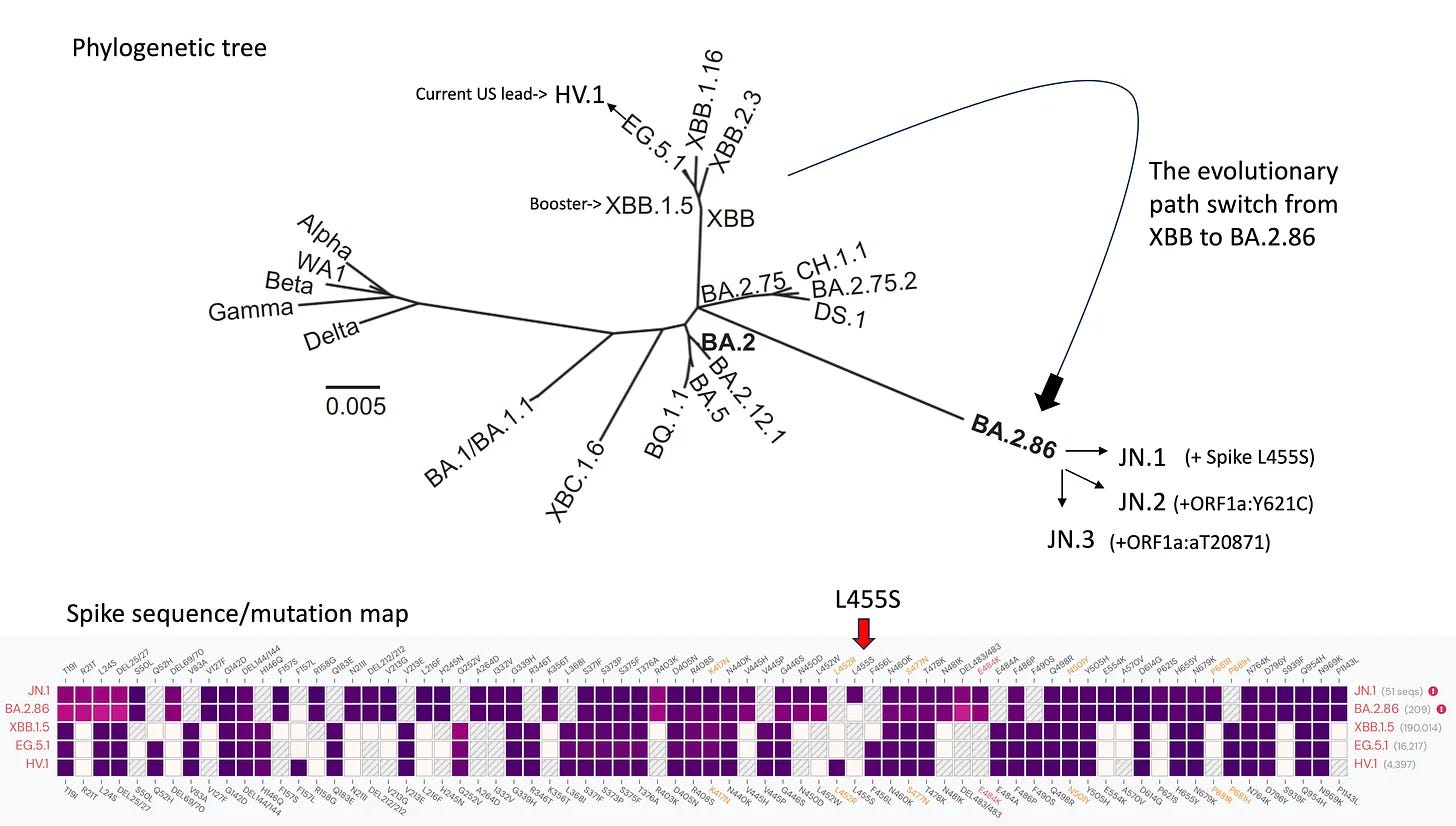
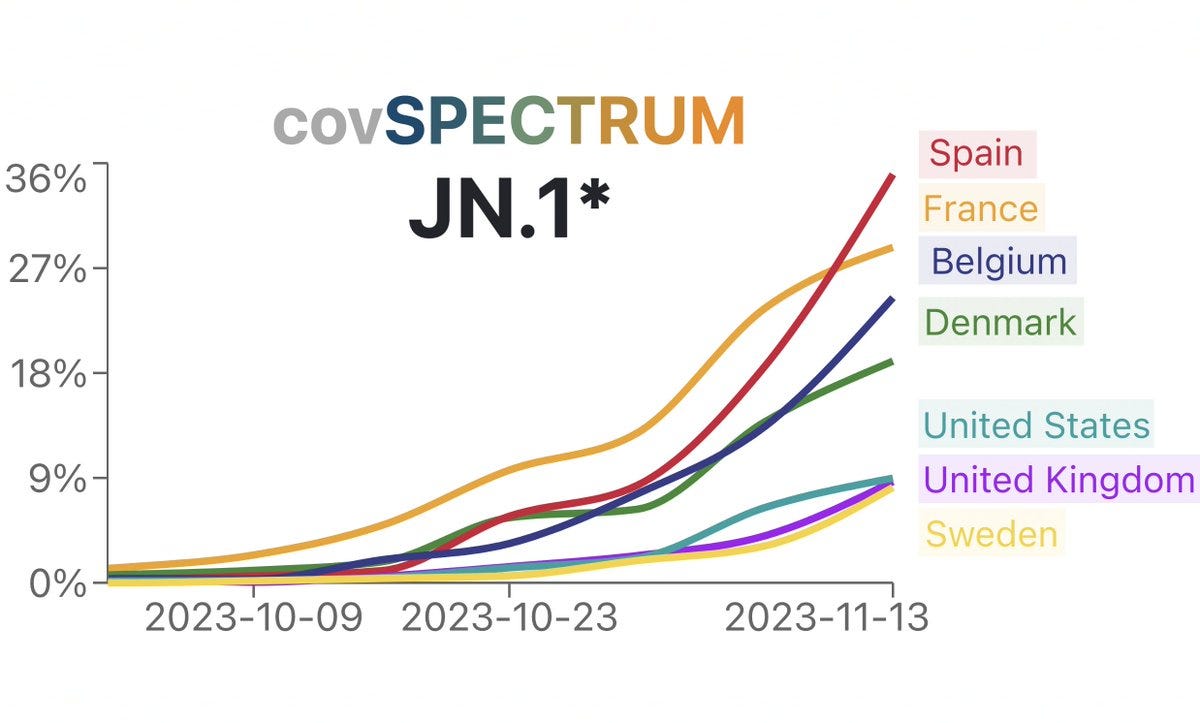
As it turns out, about 6 weeks later, this variant, first spotted up by Dave McNally, a UK data scientist, has proceeded towards global dominance. By mid-November here is the exponential growth seen in several countries in Europe, as posted by Ryan Hisner. Recall that it takes a level of 50% or greater to see the real impact in terms of clinical outcomes such as hospitalizations. By the end of November, this variant, as noted by Mike Honey, had reached >50% in Denmark, where SARS-CoV-2 sequencing is still extensive, and likely the other countries that were already above 20% below. The same pattern is being seen throughout Europe, including The Netherlands, Ireland, and many other countries not included on the graph.
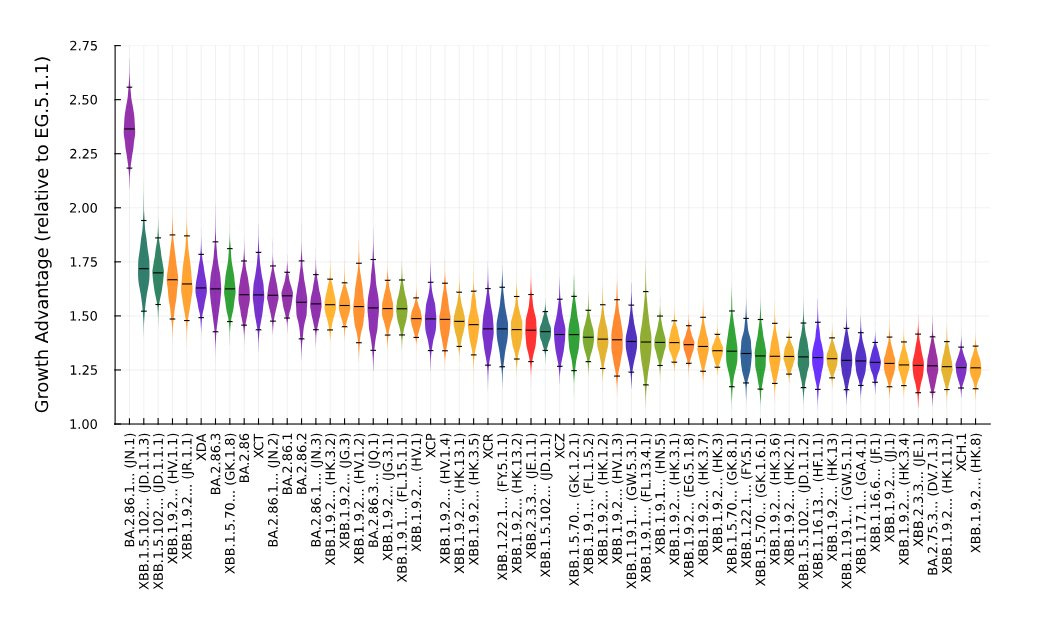
The rapid growth across Europe is no surprise, if you take into account the decided growth advantage that JN.1 has (far left) over all the others currently or previously circulating. Graph via Ben Murrell at the Karolinska Institute in Sweden.
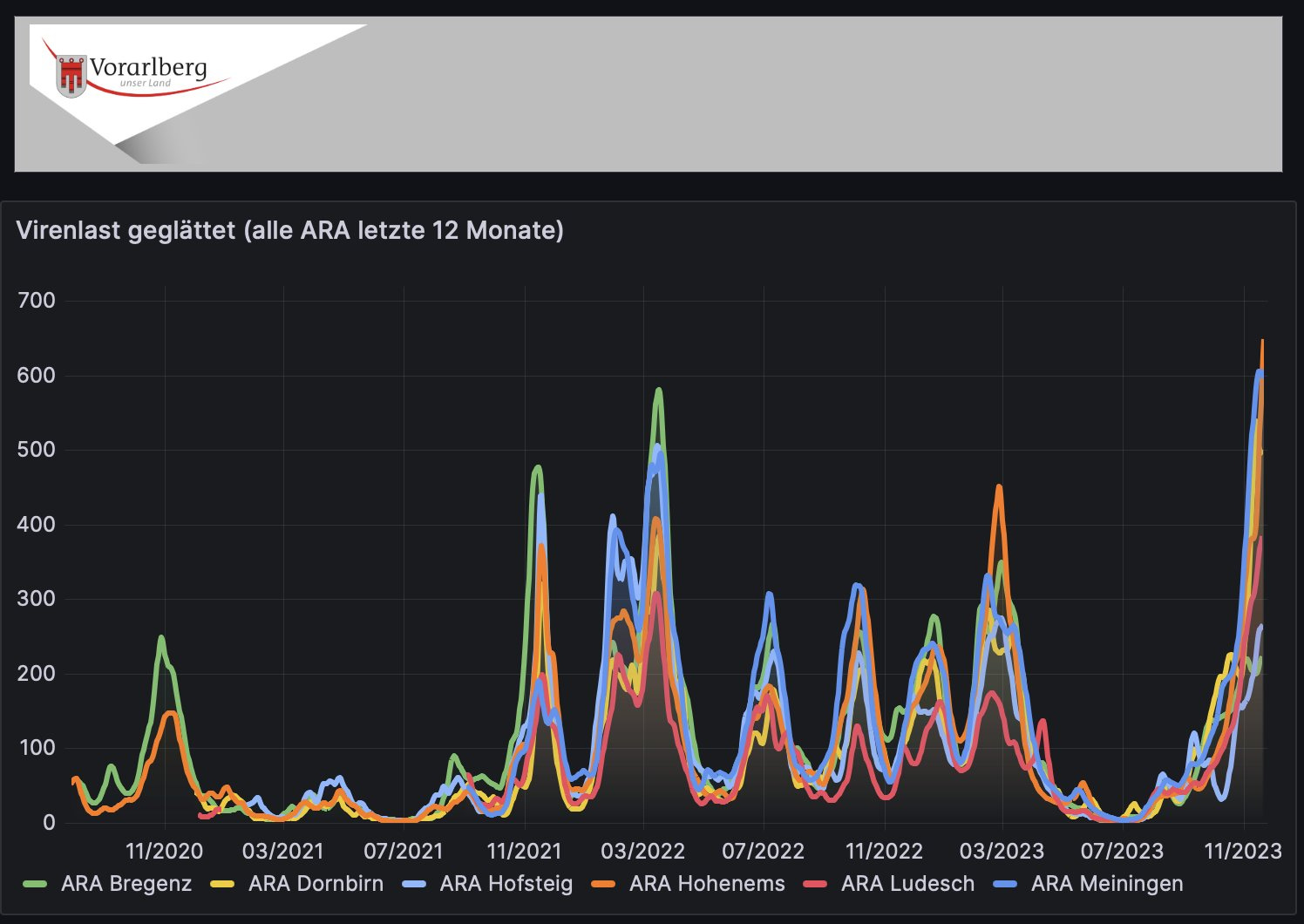
The wastewater SARS-CoV-2 surge in Austria, as noted by Ulrich Elling, surely reflects this, too.
It’s not just, Europe, of course. This variant is taking off in Australia, New Zealand, China, Japan and other places, as seen from 27 November graphic below from our outbreak.info tracking at Scripps Research. By December 5th there were already >4,000 sequences of JN.1 submitted globally, as posted by Andrew Urquhart,

Now let’s turn to the United States, where Jay Weiland, my friend, data scientist and modeler, has been all over this rise of JN.1 for weeks. Remember that we were concerned about the hyper-mutated BA.2.86, its predecessor, but it turned out not to have much growth advantage. That’s remarkably different with the new mutations (especially L455S) seen in JN.1
Take a look at the wastewater levels in the US, as Jay highlighted, with regional surges in the Midwest and Northeast.
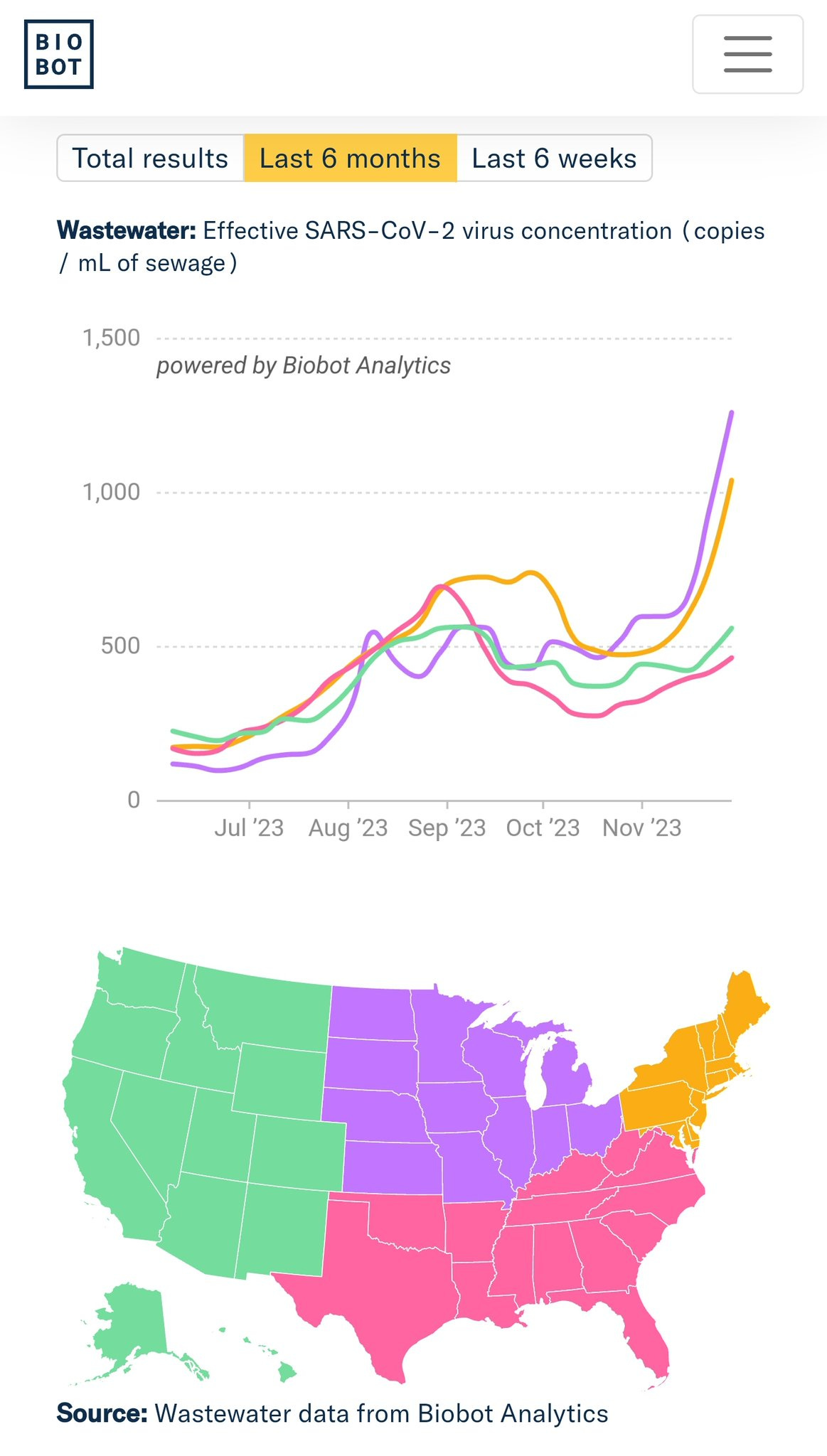
And here’s Jay’s estimate of 4 December for the present case level based on those data. The slope of the rise is especially noteworthy, as is the comparison to some earlier waves.

We’re well below 50% JN.1 throughout the US, so the wave is just getting rooted. Of course, it cannot be solely ascribed to the variant, since colder weather in these northern regions, with more indoor congregation, lack of mitigation, and the Thanksgiving holiday gatherings may well be contributing factors too.
Nonetheless, there is the beginning of a rise in Covid hospitalizations across the country, with the level by late November exceeding 20,000 new admissions per week, which, as a lagging metric, will inevitably rise.

And further evolution of JN.1 is already occurring, with the detection of the SLip variants, as shown by Daniele Focosi’s latest graphic below—that’s the added spike S456L mutation adjacent to L455S (which was the one that BA.2.86→ JN.1). The point here is that JN.1’s path to dominance is by no means signaling any pause in further evolution of SARS-CoV-2.

The Good News
Unexpectedly, given the marked difference in mutations between XBB.1.5, the target of the monovalent “updated” booster compared with JN.1, there is very good cross-recativty as demonstrated in 3 highly regarded labs (Yunlong Cao’s in Peking, David Ho’s at Columbia and David Veesler’s at U Washington). These labs have preprint published data showing solid levels of neutralizing antibodies for the XBB.1.5 booster against JN.1, our best surrogate marker for protection vs severe Covid (hospitalizations and deaths). From the Ho lab report, note the similarity of levels of neutralizing antibodies for XBB.1.5 boosters (Pfizer or Moderna) as seen with JN.1. We’d expect the same for the Novavax booster which was not assessed in that study.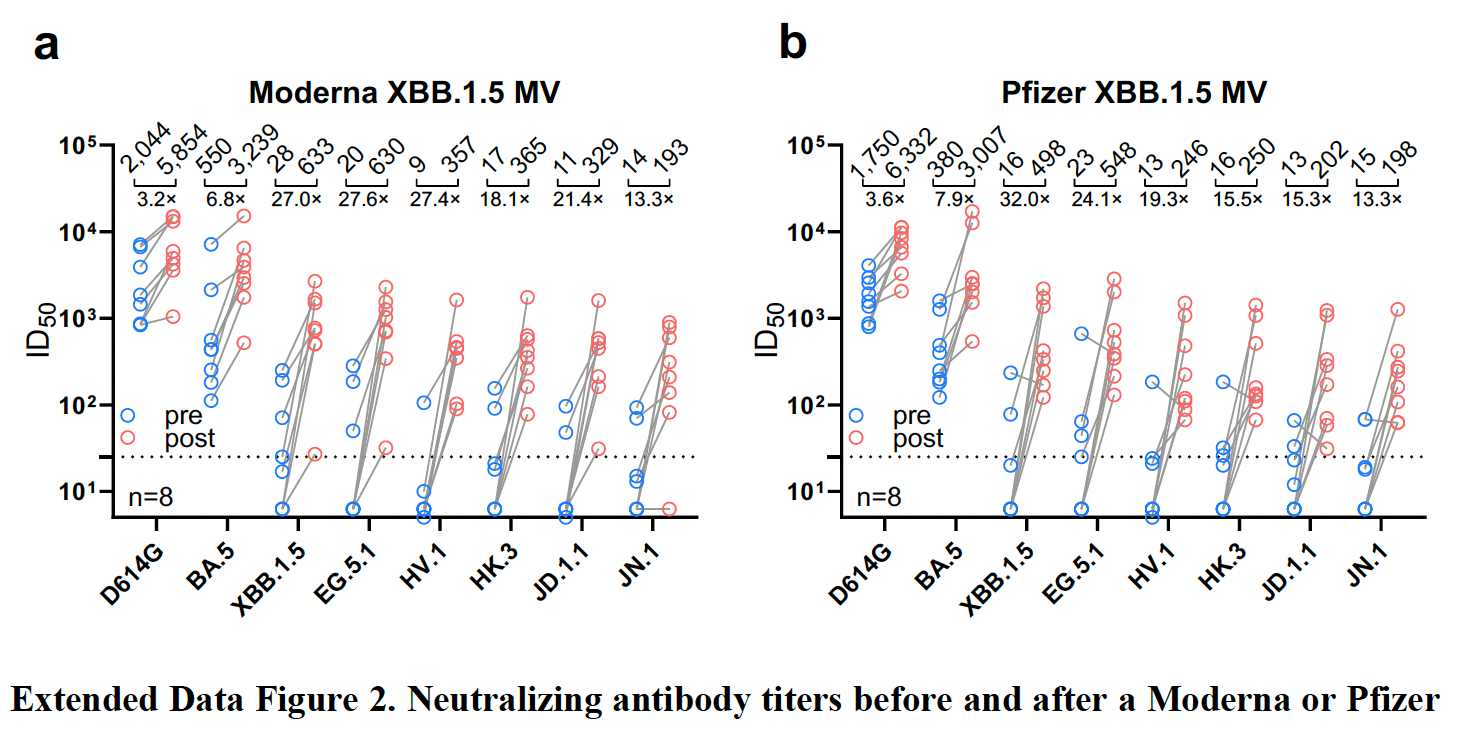
This is lucky. Actually damn lucky if you look at the profound differences in sequence (across the spike below) for the booster’s XBB.1.5 target compared with JN.1. These major differences between XBB.1.5 and JN.1 extend well beyond the spike.

Given this anticipated protection of the booster vs JN.1—which was not anticipated—a strong case is made to get a booster, even though to date only 16% of eligible American adults have done so. If you haven’t, this would be a good time to get ready for the wave ahead, especially if you’re in a high-risk group such as advanced age, immunocompromised, or with co-existing conditions.
Greatly appreciative of the work of Jay Weiland, Ryan Hisner, Dave McNally, Daniele Focosi, Ulrich Elling, Mike Honey, Federico Gueli, Ben Murrell, Andrew Urquhart, and so many others who continue to carefully track the virus.
Thanks for reading Ground Truths. Please share the post to others who might benefit from this information.
Zoner
Veteran Member
Sobering News About the COVID-19 Vaccine
@naomirwolf tells Steve Bannon about a new peer-reviewed article on Nature.com that says COVID-19 vaccine injections cause frame-shifting. That disrupts the reading of the synthetic code in such a way that the body creates nonsense proteins. About 30 percent of people who got the injection have a state of inflammation as a result, Wolf said.
Watch LIVE bit.ly/plutorav
bit.ly/plutorav
@naomirwolf tells Steve Bannon about a new peer-reviewed article on Nature.com that says COVID-19 vaccine injections cause frame-shifting. That disrupts the reading of the synthetic code in such a way that the body creates nonsense proteins. About 30 percent of people who got the injection have a state of inflammation as a result, Wolf said.
Watch LIVE
bit.ly/plutoravZoner
Veteran Member
Watch the whole interview here at this linkSobering News About the COVID-19 Vaccine
@naomirwolf tells Steve Bannon about a new peer-reviewed article on Nature.com that says COVID-19 vaccine injections cause frame-shifting. That disrupts the reading of the synthetic code in such a way that the body creates nonsense proteins. About 30 percent of people who got the injection have a state of inflammation as a result, Wolf said.
Watch LIVE
Heliobas Disciple
TB Fanatic
Dr. McMillan's video is about this study.Unanticipated Complications with mRNA Vaccine
The principle of the unknown unknowns comes to bear with this paper. It seems the Pfizer vaccine can cause formation of abnormal proteins, not anticipated by...
Very interesting on the mechanics of how the mRNA is supposed to make the protein and the mistakes that the Pfizer vaccine is making. I highly recommend.
RT 18:51
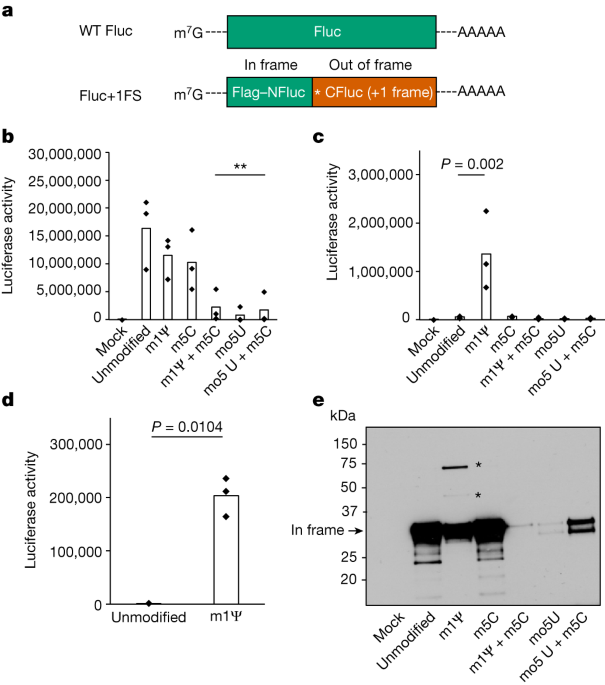
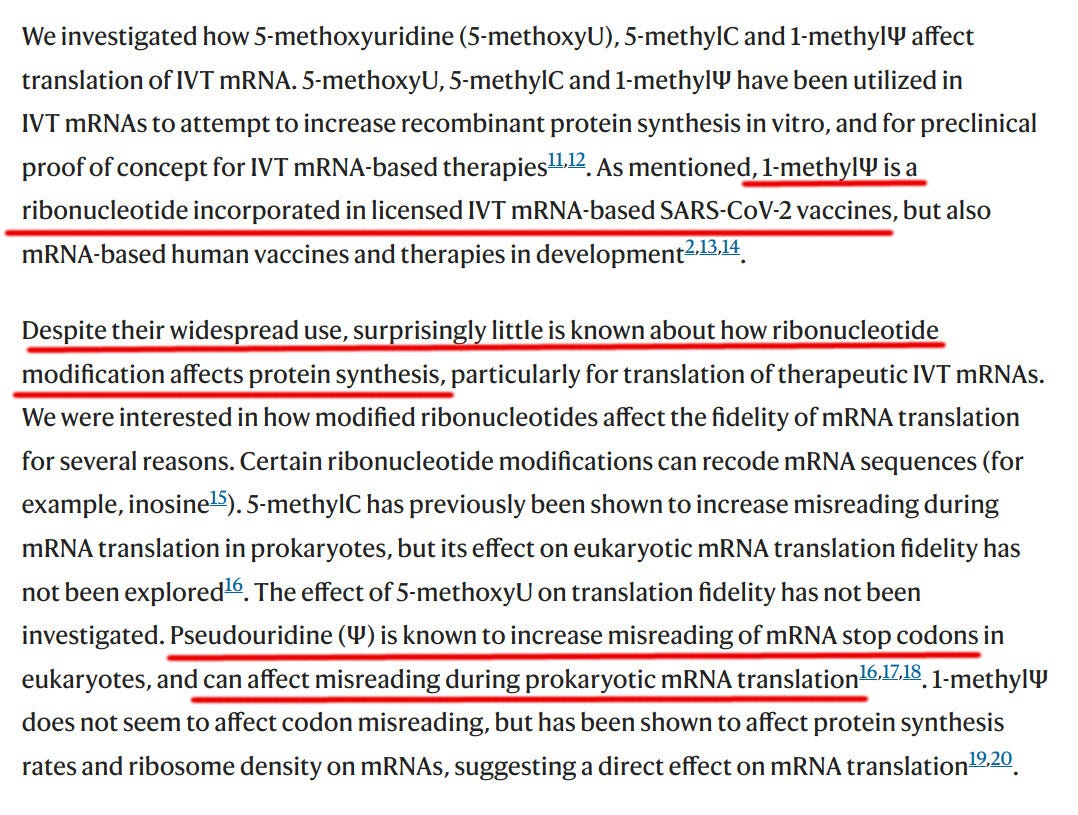
N1-methylpseudouridylation of mRNA causes +1 ribosomal frameshifting - Nature
A study demonstrates that nucleotide modifications in mRNA-based therapeutics can lead to +1 ribosomal frameshifting during translation, yielding products that can trigger immune responses.
 www.nature.com
www.nature.com
Here's an additional video on this study. And Igor Chudov also did a substack article on the same article. (see next post)
mRNA Vaccines - Researchers Propose A Design Fix
Drbeen Medical Lectures
Streamed live December 8, 2023
36 min 36 sec
An article on University of Cambridge contains this statement, "Researchers have discovered that misreading of therapeutic mRNAs by the cell’s decoding machinery can cause an unintended immune response in the body. They have identified the sequence within the mRNA that causes this to occur and found a way to prevent ‘off-target’ immune responses to enable the safer design of future mRNA therapeutics."
URL list from Friday, Dec. 8 2023
Researchers redesign future mRNA therapeutics to prevent potentially harmful immune responses | University of Cambridge
Research news
N1-methylpseudouridylation of mRNA causes +1 ribosomal frameshifting | Nature
The Shape and Structure of Proteins - Molecular Biology of the Cell - NCBI Bookshelf
Ribosomes, Transcription, Translation | Learn Science at Scitable
Genetic code - Wikipedia
DNA and RNA codon tables - Wikipedia
Pseudouridine - Wikipedia
Modifications in an Emergency: The Role of N1-Methylpseudouridine in COVID-19 Vaccines | ACS Central Science
Ribonucleotide - Wikipedia
Translation: DNA to mRNA to Protein | Learn Science at Scitable
Frontiers | On programmed ribosomal frameshifting: the alternative proteomes
Heliobas Disciple
TB Fanatic
Covid Vaccines Produce Random Junk Proteins Thanks to an "Invention" Which Coincidentally Won the Nobel Prize
A Quarter of Vaccinated Subjects Produce Random Junk Proteins due to vaccine "Read Errors" and even get immunity to them, study finds
 www.igor-chudov.com
www.igor-chudov.com
Covid Vaccines Produce Random Junk Proteins Thanks to an "Invention" Which Coincidentally Won the Nobel Prize
A Quarter of Vaccinated Subjects Produce Random Junk Proteins due to vaccine "Read Errors" and even get immunity to them, study finds
Igor Chudov
Dec 7, 2023
Would you like to get a mystery shot, which would make your body produce random, garbage proteins for an indeterminate amount of time? Well, it turned out that mRNA Covid vaccines have precisely that effect!
Scientists discovered that in addition to the toxic “spike protein,” mRNA vaccines have a weakness that introduces “read errors,” making vaccinated individuals produce nearly random proteins with unknown and unpredictable effects.
https://www.nature.com/articles/s41586-023-06800-3
That cannot be good for us!
Explanation of “Frameshifting”
Most readers would know that text characters, such as the letters of the Substack post you are reading right now, are represented as bits in our computers.For instance, computer characters comprising “GOOD MORNING” are encoded by the following bits:
01000111 01001111 01001111 01000100 00100000 01001101
01001111 01010010 01001110 01001001 01001110 01000111
What if a computer error deletes one bit in the second letter of “GOOD MORNING”?

The bits would shift and would encode a garbage sentence “G^ЮИ@ЪЮдЬТЬП”:
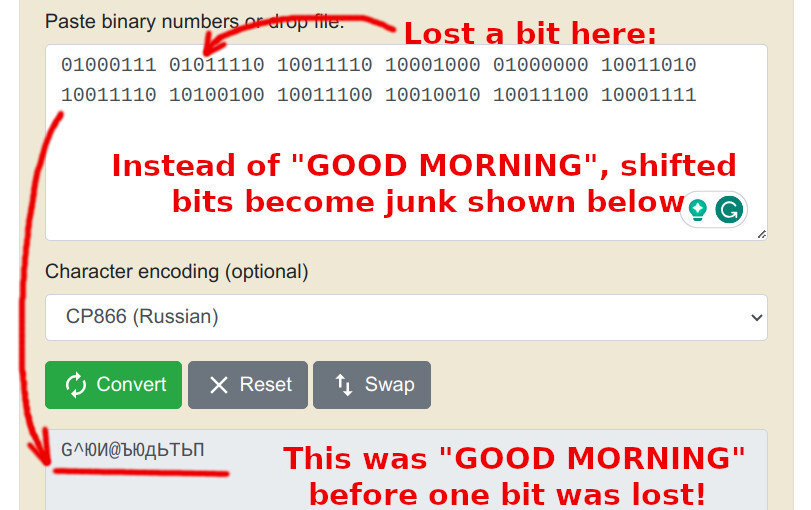
I hope you agree that any technology that causes such random loss of “bits” is not good. Some lost bits can corrupt files and even lead to computer crashes, like the infamous “Blue Screen of Death” in Microsoft Windows:
It turns out that mRNA technologies introduce similar errors, as Mulroney et al. learned using experiments on mice and humans. Just as bits are lost in text, such frameshifting errors can cause garbage outputs to clog human bodies.
mRNA Vaccine Decoding Errors
Our cells have specialized bodies called ribosomes, which help translate genetic instructions in RNA into proteins, the building blocks of our bodies.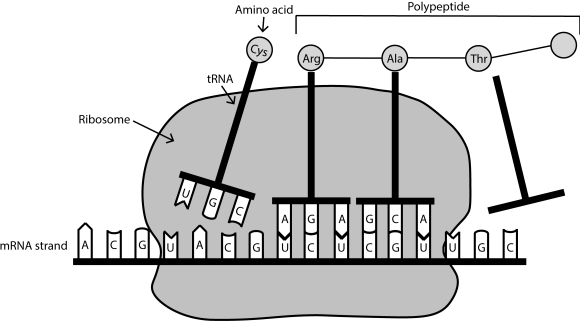
Just as with computer bits, ribosomes read genetic sequences. Based on their content, ribosomes create sequences of amino acids, which chain together and form proteins.
All this works very well. You are still alive and reading this Substack post, as billions of your cells are busy synthesizing protein. Your organism is humming along just fine, digesting food, using oxygen, thinking, etc - using biological pathways perfected by billions of years of evolution.
Until you get injected with mRNA vaccines, that is.
It turns out that mRNA COVID vaccine technology, using pseudouridine instead of uridine, creates potential for “frameshifting,” which is the same thing as bit skipping in computers. Frameshifting means that the cellular machinery erroneously skips one genetic “bit,” causing all subsequently read data to become garbled.
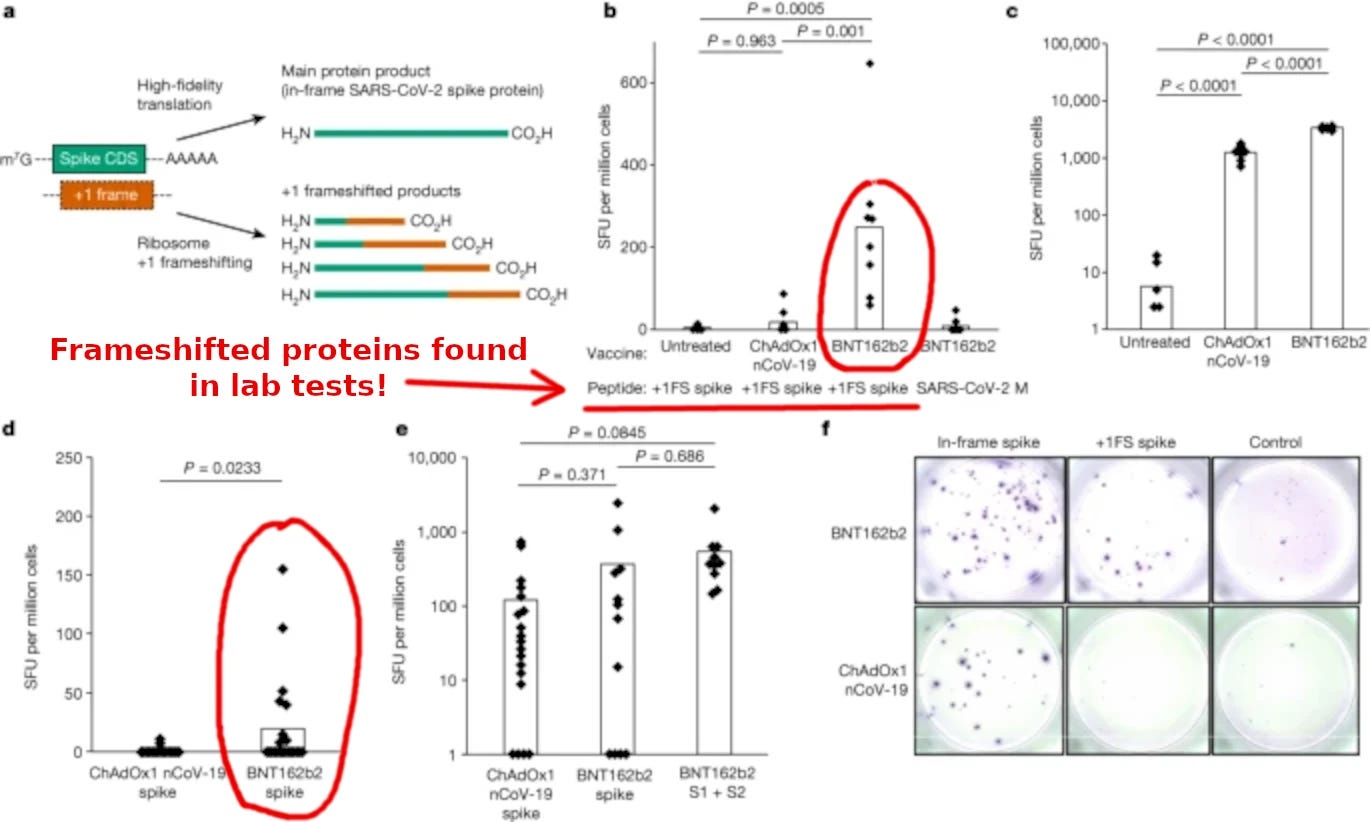
Indeed, scientists found such garbled reads in mice vaccinated with Pfizer COVID vaccine BNT162b2:
We found that responses to +1 frameshifted spike peptides were significantly increased in vaccinated mice compared to untreated mice or those vaccinated with ChAdOx nCoV-19, which does not produce antigen from translation of N1-methylpseudouridylated mRNA22 (Fig. 2b). Both BNT162b2 and ChAdOx1 nCoV-19 vaccination produced ELISpot responses to in-frame SARS-CoV-2 spike (Fig. 2c). These data suggest that +1 frameshifted products encoded in BNT162b2 spike mRNA are T cell antigens for inbred mice, to which off-target immunity can be detected following vaccination.
I feel very sorry for those inbred mice who developed immunity to unnecessary, garbage proteins created due to mRNA vaccine-caused frameshifting. What did these junk proteins do to the innocent rodents? Is the immunity, acquired essentially to random genetic sentences, going to impact the bodily functions of these mice, such as fertility? We have no idea, and neither do Mulroney and his co-authors.
This illustration shows experimental proof that such garbled reads occur routinely upon administration of pseudouridine-modified mRNA. Authors refer to them as “+1FS spike”:
Why Pseudouridine?
mRNA gene transfection technologies are not new. For example, in 1989, in a study by RW Malone et al., scientists “developed an efficient and reproducible method for RNA transfection.” However, mRNA transfections were plagued by our bodies' rejection of such foreign genetic codes for decades.
https://www.statnews.com/2017/01/10/moderna-trouble-mrna/
Safety problems, including dead and infertile animals, plagued mRNA technology trials. As a result, by 2017, as the Statnews article above points out, no successful products had materialized.
Substituting uridine with pseudouridine revolutionized mRNA technology because these artificially modified molecules finally bypassed our immune system checks and allowed for unusual mega-expression of their genetic code. Such prolonged genetic expression can last for half a year!
Igor's Newsletter
However, the new experimental mRNA technology gave us many surprises — after billions of people were force-vaccinated by injections falsely described as well-tested, safe, and effective.We are discussing one such surprise - the lost “bits” of genetic translation leading to garbage proteins produced by vaccinated bodies at random.
Scientists found that 25-30% of vaccinated people experience unintended immune response, as the Telegraph explains:
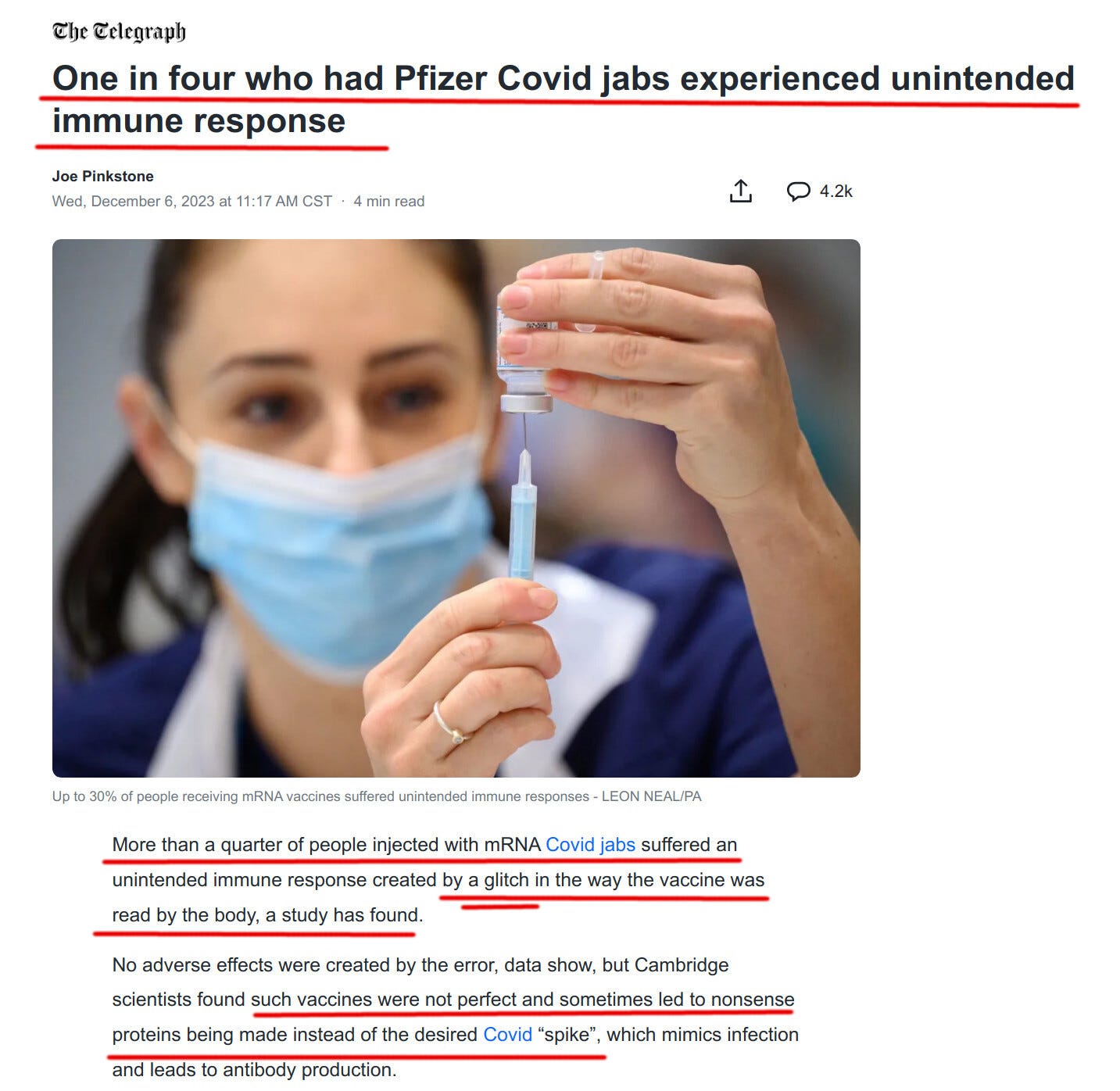
https://news.yahoo.com/more-one-four-had-mrna-171724613.html
One of the coauthors of the study, which suggested a safer alternative to pseudouridine, explains:
“This technology is amazing and it’s going to be revolutionary as a new medicine platform for all sorts of things, but we’ve just made it a whole lot safer going forward,” Professor Anne Willis, co-senior study author and director of the MRC Toxicology Unit told reporters.
If Prof. Willis made mRNA technology “a whole lot safer,” does it mean the current vaccine is unsafe? Professor Anne Willis would not make such a connection, of course. After all, she probably hopes to benefit from her “safer” invention and cannot badmouth the broad technology on which she is staking her future.
What consequences can occur due to garbled reads of COVID-19 genetic codes and the expression of junk frameshifted proteins? Nobody knows!
The Nobel Prize was Given for…Pseudouridine!
The Telegraph helpfully reminds us that the 2023 Nobel Prize was given for the invention to use pseudouridine instead of uridine:But in 2023, the Nobel Prize for Medicine went to the pair of scientists who had spent years working to fix the problem. It was done by taking one of the RNA bases, uridine, and swapping in a very similar synthetic alternative.

May I remind you of another 1949 Nobel Prize given to the inventor of lobotomy Egas Moniz?

https://www.medicina.ulisboa.pt/en/newsfmul-artigo/93/professor-egas-moniz-portuguese-nobel-prize-medicine-and-physiology
The inventors of pseudouridine are definitely in good company!
What do you think?
Heliobas Disciple
TB Fanatic
Japan Approves World’s First ‘Self-Amplifying’ mRNA COVID-19 Vaccine
The latest iteration of the mRNA vaccine is even more potent than the present version, as it generates more spike proteins in the human body.
www.theepochtimes.com
Japan Approves World’s First ‘Self-Amplifying’ mRNA COVID-19 Vaccine Without Published Efficacy or Safety Data
The latest iteration of the mRNA vaccine is even more potent than the present version, as it generates more spike proteins in the human body.
By Naveen Athrappully
12/8/2023
Japan has approved the world’s first self-amplifying mRNA (sa-mRNA) COVID-19 vaccine, although the manufacturer has not published safety or efficacy data for the shot.
Tokyo-based Meiji Seika Pharma received approval for manufacturing and marketing its Kostaive sa-mRNA COVID-19 vaccine, the company announced in a Nov. 28 press release. The mRNA in the vaccine is designed to self-amplify when delivered into cells, which generates a “strong immune response and the potential for extended duration of protection.” The vaccine is intended for primary immunization (2 doses) as well as booster immunization in adults. Kostaive is the "world's first approved product applying self-amplifying mRNA technology," according to the press release.
Both mRNA and sa-mRNA are RNA vaccines that use a virus’ genetic code against it. When an mRNA vaccine is injected into an individual, the mRNA instructs cells to make a specific protein and thus stimulates immune response. An sa-mRNA vaccine takes this concept further by making multiple mRNA copies, which ends up generating more spike protein.
Toby Young, general secretary of the Free Speech Union, a public interest group, pointed out in a Nov. 30 X post that the sa-mRNA vaccine was approved in Japan “despite only testing it on 800 people, no control group and only checking antibody levels not infection rates. Medicine regulation died with Covid.”
A phase 3 study compared the Kostaive ARCT-154 vaccine to Pfizer’s Comirnaty mRNA COVID-19 vaccine. The pre-print study, which has not been peer-reviewed, was posted in July at MedRxiv.
The study, funded by the Japanese Ministry of Health, Labour and Welfare, followed a primary phase study that analyzed the safety and efficacy of the Kostaive vaccine. The results of that study have not been published; the manuscript is “in preparation," according to the phase 3 study report.
The trial was conducted among 828 people between December 2022 and February 2023. This is a far lower number of participants than Pfizer’s phase 3 study, which involved over 40,000 individuals. The small scale of Kostaive trial has raised questions about its validity.
According to the pre-print study, Kostaive recipients reported a slightly lower number of localized reactions—such as localized pain or swelling—compared to Comirnaty. However, Kostaive recipients reported higher numbers in specific adverse events such as chills, diarrhea, dizziness, headache, malaise, nausea, and myalgia, or muscle pain.
According to Meiji Seika Pharma, the phase 3 clinical trials for booster shots showed that Konstaive elicited “higher and longer-lasting neutralizing antibody titers against the original strain” as well as an Omicron subvariant, compared to Comirnaty.
The vaccine was developed by San Diego-based Arcturus Therapeutics. Meiji Seika Pharma licensed the vaccine for sale in Japan via Melbourne-based CSL Seqirus in April this year.
The company is collaborating with Arcalis, an mRNA vaccine manufacturing firm, to establish manufacturing capabilities in Japan. Meiji Seika Pharma is working towards commercializing Kostaive in 2024.
Risks of sa-mRNA
As sa-mRNA vaccines produce copies of mRNA and thus boost the production of proteins, some experts are worried about the consequences they can have on the human body and concerned that any negative effects from mRNA vaccines could be amplified by injecting sa-mRNA shots.
During testimony at the European Parliament last month, cardiologist Peter McCullough said that “there's not a single study showing that the messenger RNA is broken down” in the human body once it is injected. Since the vaccines are “made synthetically, they cannot be broken down.”
The spike protein from the mRNA vaccines has been found circulating in the body as long as six months from vaccination, he pointed out.
Dr. McCullough said that the spike protein is “proven” in 3,400 peer-reviewed manuscripts to cause four major domains of disease—cardiovascular, neurological disease, blood clots, and immunological abnormalities.
In a recent Epoch Times article, molecular biologist Klaus Steger noted that “a small amount of saRNA [sa-mRNA] results in an increased amount of produced antigen.”
“Due to increased antigen levels, one injection of saRNA—whether linear or circular—may cause adverse events comparable with repeated (booster) injections of modRNA.”
Mr. Steger had previously pointed out that BioNTech's "mRNA" vaccines are made not with messenger RNA but with modified RNA (modRNA).
A study published in the journal Trends in Biotechnology in June this year admitted that the “main challenges involved in the global authorization [of sa-mRNA vaccines] are potential safety concerns regarding the replicative character of these vaccines.”
“As for all self-amplifying vaccines, concerns have been raised over adverse events in vulnerable individuals. For example, replicon [sa-mRNA] vaccines could persist in immunocompromised individuals as clearance may be less efficient,” it said.
The use of sa-mRNA vaccines in pregnant women also poses risks, especially if the vectors used in the vaccines come from viruses that cause congenital infections, like the Venezuelan Equine Encephalitis Virus, the study said.
“Additional preclinical and clinical studies are required to safeguard the implementation of replicon vaccines in vulnerable individuals," it cautioned.
Commenting on the Kostaive vaccine, Mike Donio, the founder of science education website Science Defined, said in a Nov. 30 X post, “I’ve been saying for a while that the first generation Covid vaccines were only the start of a coming wave of mRNA therapies.”
“First, they told us that the mRNA wouldn’t persist in cells for a long time. Now they’ve unleashed self-amplifying mRNA, which means it replicates itself. Wonder how long that will last? Maybe forever? Now tell me how they don’t want to at least try to mess with our genetics.”
The Epoch Times reached out to Meiji Holdings for comment.
Heliobas Disciple
TB Fanatic

CCP Orders Expanding Hospital Capacity ‘At All Levels Using All Means Possible’ to Deal With Fast-Worsening Pneumonia Outbreak
Following megacities of Shanghai and Guangzhou, Beijing has restarted COVID-19 PCR testing as the mysterious pneumonia continues to spread.
www.theepochtimes.com
CCP Orders Expanding Hospital Capacity 'At All Levels All Means Possible' to Deal With Fast-Worsening Pneumonia Outbreak
Following megacities of Shanghai and Guangzhou, Beijing has restarted COVID-19 PCR testing as the mysterious pneumonia continues to spread.
By Alex Wu
12/8/2023
The Chinese communist regime’s health authorities issued a notice ordering medical institutions at all levels to expand capacity by all means possible to deal with the worsening pneumonia outbreak that has overwhelmed major hospitals across China.
Experts believe that the new notice reveals that the outbreak has already spread throughout China and the ruling Chinese Communist Party (CCP) wants to shift the responsibility to the local governments at the bottom level.
The CCP’s National Health Commission issued a notice on Dec. 4, requiring all medical institutions to take "every effort to tap resources to carry out pediatric diagnosis and treatment services," and divert sick children to local primary medical and health institutions for first diagnosis and follow-up diagnosis. Primary medical and health institutions in all regions must be fully open to children and must not refuse treatment.
The National Health Commission said that it’s because "the winter respiratory disease epidemic periods overlap in many places across the country, the demand for medical and health services for urban and rural residents, especially children, has increased significantly."
The primary medical and health institutions mentioned in the notice include township health centers, community health service centers, and community hospitals. They are required to be equipped with the necessary facilities and equipment used for COVID-19 infections.
Wang He, a U.S.-based China observer, told The Epoch Times: “The notice issued by the Health Commission is actually acknowledging the full outbreak of the pneumonia throughout China.”
Mr. Wang said that the CCP requires all local-level health institutions to fully open, "which shows that this epidemic is fierce and spreading across the country, and this situation is very dangerous."
This wave of pneumonia has lasted for three months, since it started in September, spiked in mid-October, with many children reported having the "white lung symptom" that is often seen in severe “COVID-19” cases. The outbreak has continued to worsen quickly in China. Children's hospitals in Beijing, Shanghai, Tianjin, Changchun, Dalian, Shenyang, Anhui, Shandong, Sichuan, Guangzhou, Jiangsu, Gansu, and other places across China have recently seen huge crowds of patients overwhelming the hospitals. In late November, the Department of Internal Medicine of Beijing Children's Hospital received an average of more than 7,000 patients every day, far exceeding its capacity.
Sean Lin, an assistant professor in the Biomedical Science Department at Feitian College, former U.S. Army microbiologist, and Epoch Times contributor, told The Epoch Times that large hospitals in China are no longer able to handle the huge number of infected children seeking treatment and must divert them to lower-level local hospitals and clinics.
"Because the [CCP’s] central government has concealed the entire epidemic for at least three months. How much of an obstacle does this bring to local areas in taking active preventive measures?! The officials themselves don't admit it, and the central government doesn't admit it, then they shift blame to the local governments [by issuing the notice], making ordinary people believe that the infected children being turned away is because of the lack of cooperation among local medical services.”
The CCP’s National Health Commission’s notice also said that the outbreak is being caused by epidemic periods of respiratory diseases overlapping in many places in China, including influenza, respiratory syncytial virus, mycoplasma pneumonia bacteria, and COVID-19.
Mr. Lin said that the question that the CCP needs to explain clearly now is: "Why do so many people now need to go to the hospital for treatment, severe cases require IV (intravenous) treatment, and even white lungs [appeared] and require lung washing, etc. How do you explain [the occurrence of these] severe cases?"
"Even if there is cross-infection, there is no specific explanation as to which two viruses are causing cross infections making the symptoms worse."
"Officials are still concealing the number of severe cases and deaths," Mr. Lin said.
There are reports on social media and media of rising death tolls from the epidemic in many places, but authorities have been blocking the information.
A man identified only as Chen who works in the health care industry in Jinzhou city of Liaoning Province, told The Epoch Times sister media NTD that the number of deaths in hospitals has surged, but the news has been blocked by authorities: “Don't look at the official figures. The number of deaths in hospitals has increased a lot now, and waiting lines [for cremation] have begun. They built an additional crematorium here, which has already prepared for it.”
Meanwhile, the regime has reinstated various COVID-19 control measures in the country, including PCR testing. The Shanghai International Airport and customs and the southern mega-city Guangzhou have restarted PCR testing, and Beijing has also restarted PRC testing.
Beijing Restarts PCR Testing
The "China Textile Industry Federation Document" published by the China Textile Economic Information Network shows that on Dec. 6, the 2023 China Textile Industry Federation Science and Technology Awards Conference was held in the small auditorium of People's Great Hall in Beijing.
The first item of specific matters addressed in the document is: "According to the requirements of the Beijing People's Great Hall Administration, a negative COVID-19 PCR test certificate within 24 hours is required to enter the Great Hall, and the conference affairs team will arrange for the testing."
The document also listed that representatives from the China National Textile and Apparel Council to take the PCR test in the east hall on the first floor of the People's Insurance Building, No. 18 Chaoyangmen North Street, Chaoyang District, on the morning of Dec. 5; external representatives would be tested in the lobby of the Capital Hotel on the afternoon of Dec. 5.
A photo circulating on social media shows that a participant of the conference showed a PCR test certificate he/she received, which said to take this certificate to exchange for the invitation to People’s Great Hall in the parking lot at 7:30 a.m. on Dec. 6.
Ms. Yu, a Beijing resident, told Radio Free Asia on Dec. 6 that she took her child to the pediatrician at the General Hospital of the People's Liberation Army of the CCP in Dongsijitiao in Beijing that morning and was required to do a COVID-19 PCR test before seeking treatment.
Heliobas Disciple
TB Fanatic

White Lung Syndrome: Experts Float Theories on What It Is, What Causes It and Does It Even Exist?
Regardless of what’s behind recent outbreaks of white lung disease, some medical experts said they believe public health officials are downplaying environmental stressors and ignoring the immune-degrading effects of vaccination and poor diets that make people — and especially children — more...
 childrenshealthdefense.org
childrenshealthdefense.org
White Lung Syndrome: Experts Float Theories on What It Is, What Causes It and Does It Even Exist?
Regardless of what’s behind recent outbreaks of white lung disease, some medical experts said they believe public health officials are downplaying environmental stressors and ignoring the immune-degrading effects of vaccination and poor diets that make people — and especially children — more vulnerable to infections of all kinds.
By John-Michael Dumais
12/08/23
Media outlets and some mainstream medical experts are sounding the alarm over reports of pediatric white lung disease (or syndrome) outbreaks. But not all medical experts agree on what’s causing the outbreaks or what they mean — or whether the condition even exists.
Many, including experts interviewed by The Defender, do agree on this, however: Regardless of what the disease is and what’s behind the recent outbreaks, public health officials are downplaying environmental stressors and ignoring the immune-degrading effects of vaccination and poor diets that make people — and especially children — more vulnerable to infections of all kinds.
Pediatricians Dr. Paul Thomas and Dr. Larry Palevsky on a recent episode of “Good Morning CHD” on CHD.TV pushed back on media claims of white lung disease, instead pointing to vaccine-induced hyperimmunity and often-dismissed environmental factors.
“There’s no reason to worry,” said Thomas. “We’ve seen this before where you get news that just blows up fear-mongering.” Such news provokes parents to “rush their kids into their pediatrician’s office to get an RSV [respiratory syncytial virus] shot, a COVID shot, a flu shot.”
“There is nothing worse you could do for your immune system than to take those shots,” he said.
Vaccinologist Geert Vanden Bossche, DVM, Ph.D., in a guest post published Wednesday by the Alliance for Natural Health International, theorized surging child pneumonia cases result from hyper-infectious variants caused by mass vaccination that exploit young kids’ temporary gap in immunity.
Dr. Lewis Coleman, a California anesthesiologist and author of “50 Years Lost in Medical Advance,” told The Defender he believes COVID-19 infections and vaccines could be activating the “mammalian stress mechanism,” resulting in a hyperinflammatory response where fibrin from the blood is expelled into the lungs, causing the white appearance on X-rays.
Conventional analyses from Chinese and U.S. health authorities cited the role of prior lockdowns in impaired immunity and common respiratory viruses as the likely cause behind upticks in pediatric hospitalizations, according to internet lecturer John Campbell, Ph.D.
Dr. Marc Siegel told Fox News the Chinese identified Mycoplasma pneumoniae (also called “walking pneumonia”), a common respiratory pathogen, which can become “resistant mycoplasma,” he said, when too many kids receive antibiotic treatments.
Studies from Beijing show the bacterial resistance to myoplasmic pneumonia is between 70-90%, Campbell said.
Mainstream health authorities maintain the increase in childhood respiratory illnesses falls within normal ranges of seasonal sickness.
“There’s no such thing as white lung syndrome,” said Dr. Shira Doron of Tufts Medical Center on a recent NBC Boston segment shown in the CHD.TV episode. “The news story here is that a scary headline will spread even faster than a virus.”
In China, over 3,500 children were admitted for treatment of “white lung” in October and November, said Campbell.
Since August, Ohio’s Warren County Health District has recorded 142 pediatric pneumonia hospitalizations, according to NBC Boston.
The syndrome has also been noted in the Netherlands and Denmark, with the latter reporting 541 cases as of Nov. 26.
Possible role of vaccines, environmental stressors
Thomas told CHD.TV that said routine childhood vaccinations can cause side effects that “are never attributed to the vaccine.”
“My own data, which just compared unvaccinated to variably vaccinated kids showed a really surprising finding: the unvaccinated had much better immune systems, and that translated into way less infections,” Thomas said.
Thomas said it didn’t matter whether he was looking at “ear infections, lung infections, sinus infections, eye infections, [or] all infections combined” — there was a “massive benefit” for those who did not vaccinate.
Thomas shared how his mother, after receiving three COVID-19 shots, developed lung inflammation resembling the reported white lung cases. “Her X-ray looked exactly like those X-rays now,” he said.
Palevsky pointed out that Mycoplasma pneumoniae is listed as a potential side effect of Pfizer’s COVID-19 vaccine.
“We could be colonizing mycoplasma bacteria in our airways and not be sick” until bodily conditions change and symptoms develop, he said, adding that the common medical thinking that “you only got it [a virus] because someone gave it to you” is false.
Palevsky said environmental toxins like air pollution and electromagnetic radiation, inappropriate eating and nutrient deficiencies like low vitamin D levels that alter internal terrain often go overlooked as illness triggers.
These factors are increasing children’s stress levels, he said, resulting in “the body … responding in an appropriate way to get the garbage … the toxins out of their systems.”

Carla Peeters, Ph.D., in a Brownstone Institute article published Wednesday, said white lung syndrome is most likely the result of “a dramatic degradation of the human immune system” creating a susceptibility for “many opportunistic pathogens from bacteria to fungi to viruses.”
She attributed the degradation in part to “chronic fear, anxiety, and pandemic measures,” leading to poverty, homelessness and exposure to frigid air, and noted new studies found masks were linked to “Covid infections, exposure to toxic compounds, and pathogenic bacteria and fungi.”
Peeters called for “affordable nutritious food and warmth” and a better-prepared healthcare system, including natural remedies.
Campbell said it was a pity the World Health Organization, in its Nov. 23 press release about the illness, didn’t talk about strengthening the immune system through nutrition, vitamin D, sleep or exercise, and instead focused on mask-wearing and isolation.
Vanden Bossche: Mass vaccination stresses immature immune systems
According to Vanden Bossche, it is unlikely that the white lung pneumonia reported in children would be connected to COVID-19 vaccination directly (due to low vaccination rates in this age group) or the lifting of confinement policies.
He theorized short-lived pediatric respiratory disease spikes emerge from mass vaccination-caused population-level pressure on viral variants as they seek to evade human immune defenses. The resulting higher transmission rates enable repeat infections in children before they develop mature immunity.
Vanden Bossche explained:
“The reason why WLP [white lung pneumonia] predominantly (but not exclusively) affects children aged 5 to 12 is that, at this stage, they have not yet transitioned from natural/innate antibody(Ab)-mediated protection against glycosylated components (including viruses or small microorganisms containing glycosylated components in their envelope/membrane) to trained, cell-mediated innate immunity …
[‘Glycosylation’ describes how virus particles or other pathogens hijack our cellular machinery to attach sugar molecules to their structural components like surface proteins or envelopes, optimizing their infectivity by evading immune recognition and improving stability.]
“As children grow older, they progressively replace the ‘self’-sensing innate Ab capacity by a pool of pre-primed Natural Killer cells that can recognize pathogen-derived self-mimicking (i.e., ‘altered self’) motifs on virus-infected or otherwise pathologically altered host cells such as to kill those cells.”
In other words, white lung pneumonia largely impacts younger children because their early-stage antibodies have waned before more advanced cellular defenses have fully developed.
This leaves their immune systems vulnerable to being overwhelmed by new viral variants, triggering lung inflammation that allows other pathogens already inhabiting the upper airway tract — such as Mycoplasma pneumoniae, RSV, influenza or Streptococcus pneumoniae — to infect more easily, Vanden Bossche said.
“Massive migration of virus-tethered dendritic cells [immune system ‘first responders’ that detect and attach to pathogens] to the lung likely triggers extensive inflammation,” he said, adding that this theory of pathogenesis “suggests that enhanced microbial infection is not the cause, but rather secondary to pulmonary (lung) inflammation.”
“I therefore prefer to refer to this condition as white lung syndrome (WLS),” he said.
During high population- or family-level infection rates, children are more likely to become reinfected shortly after an asymptomatic infection, “thereby sidelining the innate immune response against airborne glycosylated viruses,” Vanden Bossche said.
Amending his earlier statement about the possible contribution of COVID-19 vaccines to white lung syndrome, Vanden Bossche wrote, “This disease could also affect C[OVID]-19 vaccinees, particularly those who have not yet developed sufficiently strong CTL (cytotoxic T lymphocyte [‘killer T cell’]) activity to eliminate highly infectious progeny virus before it massively adsorbs onto” upper respiratory tract-resident dendritic cells.
Vanden Bossche’s final points highlighted the negative impacts of mass vaccination in general and mRNA vaccines in particular:
“It is crucial to understand that both the enhancement of viral infection and enhanced intrinsic viral infectiousness directly result from collective immune pressure placed on viral infectivity as a consequence of mass vaccination. This population-level immune pressure has driven natural selection and the (co-)circulation of more infectious immune escape variants.
“… Neither MIS-C [multisystemic inflammatory syndrome in children] nor WLS justifies C-19 vaccination for children, as C-19 vaccines, particularly mRNA vaccines, promote the sidelining of the child’s cell-based innate immune system.”
Coleman: The possible role of the ‘mammalian stress mechanism’
Coleman, chair of the science and education board of the American Institute of Stress — founded by the father of stress theory Hans Selye (1907-1982) — offered his theoretical framework for how the spike protein in SARS-CoV-2 and the mRNA vaccines causes hyperactivity of the mammalian stress mechanism that manifests as white lung syndrome.
The summary that follows is a greatly simplified take on a highly complex process, based on Coleman’s discussions with The Defender and his writings.
The mammalian stress mechanism governs physiology, including breathing, blood flow, heart function, digestion, excretion, immune activity, hormone release, tissue maintenance and tissue repair.
The vascular endothelium is the focus of stress mechanism activity. It is a selectively permeable layer of highly specialized cells, one cell thick, which lines the inner walls of all blood vessels and is the sole constituent of capillaries. The blood-brain barrier is an example of this vascular endothelium specialization.
SARS, MERS and other weaponized versions of the coronavirus disrupt the vascular endothelium, increasing the “leakage” of tissue factor from extravascular tissues (connective tissues, fat, muscle, organ tissues, etc.) into flowing blood and through several complex interactions, altering the way thrombin, soluble fibrin and insoluble fibrin (all clotting factors) are generated.
The excessive and/or defective production of these three products, plus depletion of their building blocks, explains the harmful manifestations of disease, including inflammation and blood coagulability, tissue edema, organ dysfunction, pus, fever and so forth.
When the mRNA vaccines are injected into the body, they hijack the cells of the vascular endothelium to replicate themselves, propagate throughout the body, and disrupt organs and tissues.
Coleman theorized that mRNA injections are causing sudden death in young athletes by inducing disseminated intravascular coagulation — abnormal clotting together with bleeding problems due to depletion of clotting reserves — in small peripheral arteries, which disrupts oxygen transport and delivery.
Vaccine-induced thrombocytopenia (low blood platelet levels that can cause excessive bruising and bleeding) and thrombosis (blood clots) — when occurring together sometimes called vaccine-induced immune thrombotic thrombocytopenia (VITT) — have been well documented.
According to Coleman, the white color that appears on the X-rays of children with white lung syndrome is soluble fibrin — a protein that normally facilitates tissue repair — but when produced in excess invades organs and tissues, causing edema (swelling) that disrupts organ function. In the lungs, soluble fibrin protein creates a structure that allows pus and fluids to attach and accumulate, disrupting our ability to breathe.
“Stress mechanism activity is exaggerated by COVID immunizations and exposures to the weaponized coronavirus,” Coleman said, “and when a person subsequently gets exposed to some other type of viruses like a pulmonary virus, then the lungs … become inflamed, their permeability increases and fibrin starts to infiltrate the lungs.”
This process is called extravascular fibrin deposition, a normal part of the tissue repair process but when hyperactivated can lead to an acute inflammatory response. On X-rays, fibrin has a hazy appearance similar to what has been observed in white lung syndrome.
The opportunistic viruses reported with white lung syndrome have an “exaggerated effect they wouldn’t ordinarily have,” Coleman said, because mammalian stress mechanism hyperactivity is determined by the sum total of the various stresses “attacking us from all directions.”
Coleman attributed children’s susceptibility to white lung syndrome to their level of vitality, causing increased reactivity to stressors — not just the spike protein, but other environmental toxins as well.
Coleman and his colleagues at the American Institute of Stress believe the discovery of the mammalian stress mechanism may represent the most important advance in medical theory in a generation, but he admits his work challenges many of the assumptions of current medical-scientific consensus.
Watch experts discuss white lung syndrome on ‘Good Morning CHD’:
31 min 54 sec
[can only be watched at link]
Heliobas Disciple
TB Fanatic

COVID-19 News: Study Shows That SARS-CoV-2 ‘Disarms’ Innate Immunity In ‘Recovered’ Individuals To Pave The Path For Viral Persistence In Lungs! - Thailand Medical News
COVID-19 News: As the world grapples with the ongoing challenges posed by the COVID-19 pandemic, new revelations about the persistence of SARS-CoV-2, the virus responsible for COVID-19, shed light on the intricacies of the human immune response. A recent study conducted by researchers from the...
www.thailandmedical.news
Study Shows That SARS-CoV-2 ‘Disarms’ Innate Immunity In ‘Recovered’ Individuals To Pave The Path For Viral Persistence In Lungs
Nikhil Prasad Fact checked by:Thailand Medical News Team
Dec 09, 2023
As the world grapples with the ongoing challenges posed by the COVID-19 pandemic, new revelations about the persistence of SARS-CoV-2, the virus responsible for COVID-19, shed light on the intricacies of the human immune response. A recent study conducted by researchers from the Institut Pasteur, specializing in HIV, in collaboration with the French public research institute CEA, has unveiled a startling discovery - the SARS-CoV-2 virus persists in the lungs of recovered individuals for up to 18 months after infection, challenging the notion that recovery implies the complete eradication of the virus from the body.
Persistence in the Lungs
Typically, one to two weeks after contracting COVID-19, SARS-CoV-2 becomes undetectable in the upper respiratory tract. However, this does not necessarily indicate its absence from the body. The study covered in this COVID-19 News report, focused on lung cells in a preclinical model of non-human primates to investigate the longevity of SARS-CoV-2 presence. Astonishingly, the results revealed the persistence of the virus in the lungs of certain individuals for an extended period, ranging from 6 to 18 months post-infection.
The Nature of Viral Reservoirs
The concept of viral reservoirs, where viruses linger discreetly after causing an initial infection, is not new. HIV, for instance, can remain latent in specific immune cells, reactivating unpredictably. The researchers hypothesized a similar scenario for SARS-CoV-2, and their findings in the non-human primate model substantiate this hypothesis. Dr Michaela Müller-Trutwin, Head of the Institut Pasteur's HIV, Inflammation, and Persistence Unit, remarked, "We observed that inflammation persisted for long periods in primates that had been infected by SARS-CoV-2. We therefore suspected that it could be due to the presence of the virus in the body."
Surprising Discoveries in the Lungs
The study yielded unexpected findings - even when conventional PCR tests returned negative results and the virus was undetectable in the upper respiratory tract or blood, viruses were discovered in certain immune cells, specifically alveolar macrophages, within the lungs. Dr Nicolas Huot, the first author of the study, emphasized the surprise, stating, "What's more, we cultured these viruses and were able to observe, using the tools we developed to study HIV, that they were still capable of replicating."
Role of Innate Immunity
To unravel the mechanisms behind this prolonged viral presence, the researchers turned their attention to innate immunity, the body's initial defense against pathogens. Natural killer (NK) cells, a crucial component of innate immunity, play a significant role in controlling viral infections. The study found that in some individuals, macrophages infected with SARS-CoV-2 became resistant to destruction by NK cells. In contrast, adaptive NK cells in other individuals successfully adapted to the infection, destroying resistant cells, particularly macrophages.
Understanding the Immune Response
The cellular response of innate immunity, particularly the role of NK cells, had been relatively understudied in the context of SARS-CoV-2 infections. Dr Michaela Müller-Trutwin highlighted the importance of NK cells, stating, "The cellular response of innate immunity, which is the body's first line of defense, has been little studied in SARS-CoV-2 infections until now. Yet it has long been known that NK cells play an important role in controlling viral infections." The study illuminated a potential link between the levels of persistent SARS-CoV-2 and the presence or absence of adaptive NK cells.
Interplay Between NK Cells and Macrophages
The research elucidated a nuanced interplay between NK cells and macrophages that regulated the persistence of SARS-CoV-2 in macrophages. The critical factor was interferon-gamma (IFN-?), a cytokine involved in antiviral responses. The study found that IFN-? inhibited the replication of SARS-CoV-2 in bronchioalveolar lavage (BAL) macrophages. The strongest production of IFN-? occurred in BAL NKG2r+CD8+ T cells and NKG2Alo natural killer cells. However, impaired IFN-? production was observed in NK cells from macaques with persisting virus.
Variability in Immune Response
The study unveiled a variable immune response among individuals, with some exhibiting adaptive NK cell production, associated with lower levels of persistent virus. In contrast, individuals with higher levels of virus not only lacked adaptive NK cells but also demonstrated a reduction in NK cell activity. This variability in innate immunity's effectiveness hinted at potential connections to the phenomenon of long COVID, prompting further investigation into a cohort infected at the start of the pandemic.
Viral Persistence Mechanisms
The researchers discovered that the persistence of SARS-CoV-2 in lung alveolar macrophages was controlled by IFN-? and NK cells. The study delved into the molecular mechanisms involved, shedding light on the role of major histocompatibility complex (MHC)-E on BAL macrophages. IFN-? not only inhibited viral replication but also enhanced the expression of MHC-E, potentially inhibiting NK cell-mediated killing.
Insights from Non-Human Primate Models
Non-human primate models played a crucial role in unraveling the complexities of SARS-CoV-2 persistence and the immune response. Cynomolgus macaques provided a valuable tool for studying immune cell functioning and responses in tissues, offering insights into human infectious diseases. The study used a comprehensive approach, including multiparameter flow cytometry, to analyze BALF cells, revealing alterations in macrophage phenotype and lymphocyte frequencies in infected macaques.
Long-Term Effects on Macrophages
The study explored the long-term effects of SARS-CoV-2 on macrophages (Mac) within the bronchoalveolar lavage fluid (BALF). Mac, comprising a significant portion of the lung's total leukocyte population, responded to microbial threats but exhibited dysregulation during SARS-CoV-2 infection. Long-term alterations in Mac phenotype, marked by increased expression of CD206, CD4, CD11c, MHC-E, and IL-10, were observed. These changes indicated an alternative activation of alveolar Mac, potentially contributing to lung contusion and pneumonia.
Viral Replication in Macrophages
Detection of replication-competent SARS-CoV-2 in BALF Mac was a groundbreaking revelation. The study utilized reverse transcription polymerase chain reaction (RT–PCR) to identify viral RNA in BALF cells, grouping macaques based on viral load levels. The presence of viral antigens in BALF Mac, confirmed through the detection of spike protein, indicated ongoing viral replication. Confocal images revealed the existence of double-stranded RNA and nonstructural protein 3 (NSP3) within BALF Mac, suggesting viral replication through cell-to-cell propagation.
Transcriptomic Analysis of Macrophages
In-depth transcriptomic analysis of cultured BALF Macs exposed the molecular changes induced by SARS-CoV-2 replication. Increased expression of fibronectin (FN1), S100A8/S100A9 (calprotectin), and CD1b, a nonpolymorphic MHC class I-like glycoprotein, hinted at sustained immune activation and chronic inflammation. Notably, the study emphasized the importance of investigating these changes in the context of potential long COVID manifestations, expanding the scope beyond acute infection.
IFN-?'s Dual Role in Viral Persistence
IFN-?, a pivotal immunoregulatory cytokine, demonstrated a dual role in the context of SARS-CoV-2 infection. On one hand, it exhibited antiviral properties by inhibiting viral replication in BALF Mac. On the other hand, IFN-? induced the upregulation of MHC-E on infected cells, potentially shielding them from NK cell-mediated lysis. This dual impact underscored the complexity of the immune response against SARS-CoV-2, where a crucial cytokine simultaneously controlled viral replication and contributed to the persistence of infected cells.
SARS-CoV-2 Spike Protein's Modulation of Immune Response
The study highlighted the role of the SARS-CoV-2 spike protein in modulating NK cell function and immune evasion. Peptides derived from the spike protein, such as V3-11, were identified as binders to MHC-E, inhibiting NK cell degranulation activity. Intriguingly, the extent of inhibition correlated with viral load and the presence of spike protein in infected Mac. This observation suggested a dynamic interaction between the viral protein and immune response, influencing the persistence of SARS-CoV-2.
Conclusion: Unraveling the Tapestry of SARS-CoV-2 Persistence
In conclusion, the study offers a comprehensive exploration of the complex interplay between SARS-CoV-2, innate immunity, and the lungs. The revelation of viral persistence in recovered individuals opens new avenues for understanding the long-term consequences of COVID-19. The dynamic interactions between viral reservoirs, alveolar macrophages, NK cells, and key cytokines like IFN-? provide valuable insights into the mechanisms underlying persistent SARS-CoV-2 infections. As the scientific community delves deeper into the intricacies of viral persistence, these findings pave the way for future research aiming to unravel the mysteries of long COVID and inform the development of targeted therapeutic interventions.
The study findings were published in the peer reviewed journal: Nature Immunology.
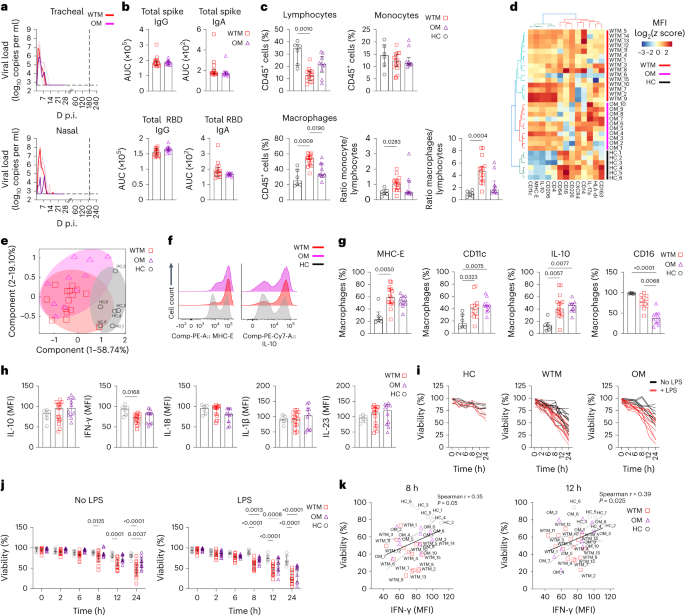
SARS-CoV-2 viral persistence in lung alveolar macrophages is controlled by IFN-γ and NK cells - Nature Immunology
Huot et al. show that interferon-γ (IFN-γ) regulates the persistence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in bronchoalveolar macrophages from cynomolgus macaques up to 18 months postinfection.
www.nature.com
Heliobas Disciple
TB Fanatic

BREAKING COVID-19 News! U.S. CDC Admits That JN.1 Is Possibly More Transmissible As Infections And Hospitalizations Rise In United States! - Thailand Medical News
COVID-19 News: In a startling turn of events, the United States Centers for Disease Control and Prevention (CDC) has issued a new report suggesting that the new SARS-CoV-2 sub-lineages, JN.1, a spawn of the highly mutated BA.2.86 variant that emerged in August 2023 is potentially more...
www.thailandmedical.news
U.S. CDC Admits That JN.1 Is Possibly More Transmissible As Infections And Hospitalizations Rise In United States
Nikhil Prasad Fact checked by:Thailand Medical News Team
Dec 09, 2023
In a startling turn of events, the United States Centers for Disease Control and Prevention (CDC) has issued a new report suggesting that the new SARS-CoV-2 sub-lineages, JN.1, a spawn of the highly mutated BA.2.86 variant that emerged in August 2023 is potentially more transmissible than its predecessors and is also highly immune evasive, causing a significant uptick in COVID-19 infections and hospitalizations across America.
Emergence of JN.1 Subvariant and Rise in Infections
The CDC's latest estimates reveal that JN.1, a sublineage of BA.2.86 or 'pirola,' has been responsible for over 21% of new coronavirus infections in recent weeks.
COVID Data Tracker
CDC’s home for COVID-19 data. Visualizations, graphs, and data in one easy-to-use website.
covid.cdc.gov
The World Health Organization classifies JN.1 as a variant of interest due to its extensive mutation profile. This revelation comes at a critical juncture, with the holiday season facilitating increased travel and indoor gatherings, contributing to the accelerated spread of the virus.
Surge in COVID-19 Hospitalizations
Over the past month, the United States has witnessed a staggering 17% increase in weekly COVID-19 hospitalizations.
COVID Data Tracker
CDC’s home for COVID-19 data. Visualizations, graphs, and data in one easy-to-use website.
covid.cdc.gov
More than 22,500 new hospital admissions were reported, surpassing the peak observed during the late summer wave. This surge was anticipated, given the seasonal trends associated with holiday festivities and increased social interactions.
Surge In COVID-19 Deaths In America.
Latest data also shows that COVID-19 deaths in America has rise by 25% in the last week. Many physicians and experts warn that death rates will rise exponentially in coming weeks as the effects of the cold season and festivities will become more apparent.
COVID Data Tracker
CDC’s home for COVID-19 data. Visualizations, graphs, and data in one easy-to-use website.
covid.cdc.gov
Impact on Specific Age Groups: Seniors and Children Vulnerabilities
The disproportionate impact on specific age groups is a cause for concern. Seniors aged 65 and older continue to bear the brunt of the pandemic, with the highest rate of weekly hospitalizations, standing at 13.5% per 100,000 individuals. The vulnerability of this demographic is attributed to age-related factors and underlying health conditions, further emphasizing the urgent need for booster shots to address waning vaccine protection.
Children under the age of 4 are also facing an elevated risk, constituting the third-highest rate of hospitalizations at 1.6% per 100,000 individuals. While children generally experience milder cases, studies indicate that vaccinations significantly reduce hospitalizations in this age group.
Despite this, vaccine uptake among children for COVID-19 lags behind influenza, with 38.2% receiving flu shots compared to 6.9% for COVID-19 vaccines.
Vaccination Trends—Children
 www.cdc.gov
www.cdc.gov
Vaccination Trends—Adults
JN.1 Subvariant: The New Challenge
The emergence of the JN.1 subvariant adds a new layer of complexity to the situation. JN.1 is rapidly becoming the dominant member of the BA.2.86 family, with its prevalence skyrocketing from 8.1% to 21.4% in the last two weeks alone. It now stands as the second-most detected variant in the U.S., trailing only HV.1.
The U.S. CDC has raised concerns about JN.1's potential for increased transmissibility or immune system evasion. Although there is currently no evidence indicating a higher risk compared to other variants, the continued growth of JN.1 underscores the need for vigilance. Laboratory data suggests that existing COVID-19 vaccines, including booster shots, remain effective against JN.1.
The JN.1 variant is spreading at a phase that has not been seen with previous variants including the Omicron variant and is expected to become the globally predominant variant in the next few weeks.
In highly vaccinated Singapore, latest COVID-19 News updates shows that the JN.1 variant is currently responsible for 60% of all new reported SARS-CoV-2 infections with hospitalizations and ICU admissions also rising there.
BREAKING COVID-19 News! The JN.1 Variant Now Accounts For 60 Percent Of All COVID-19 Cases In Singapore Amidst Rising COVID-19 Hospitalizations! - Thailand Medical News
Severity Indicators In the United States: Hospitalizations and Deaths on the Rise
As the winter holidays approach, the CDC's severity indicators for COVID-19 -hospitalizations and deaths - show notable increases over the past week. Hospitalizations are up by 17.6%, and deaths have risen by 25%, although still at a lower rate than observed in November 2022.
COVID Data Tracker
CDC’s home for COVID-19 data. Visualizations, graphs, and data in one easy-to-use website.
covid.cdc.gov
Moderate levels of hospitalizations are reported, primarily in the Midwest and Mid-Atlantic regions, with high levels in specific states such as Montana, South Dakota, and West Virginia.
States reporting significant increases in deaths last week include Alabama, Maine, Maryland, Minnesota, Missouri, and West Virginia. The U.S. CDC emphasizes that COVID-19 remains the primary driver of viral respiratory deaths.
Seasonal Flu Activity on the Rise
In addition to the COVID-19 surge, the U.S. CDC reports a concurrent rise in seasonal flu activity, particularly in the Southeast and South-Central regions. Influenza A, with the dominant subtype being 2009 H1N1, constitutes 80% of positive samples. While flu hospitalizations are still relatively low, they are increasing, primarily affecting seniors, adults aged 50 to 64, and young children.

Weekly U.S. Influenza Surveillance Report
Learn more about the weekly influenza surveillance report (FluView) prepared by the Influenza Division.
www.cdc.gov
Respiratory Syncytial Virus (RSV) Concerns
Respiratory syncytial virus (RSV) remains a significant concern, with hospitalizations on the rise, particularly in older adults. The U.S. CDC notes that only 15.9% of eligible adults have received the RSV vaccine. Overall, RSV hospitalizations are slightly down, accompanied by a decrease in test positivity for the virus.
Respiratory Virus Data Channel Weekly Snapshot
www.cdc.gov
Early Indicators and Wastewater SARS-CoV-2 Tracking
The U.S. CDC's early indicators show rises in test positivity, up by 0.9%, and emergency department visits, up by 4%. Test positivity is higher in the Midwest, Mountain West, and Northeast regions. Infants and seniors have the highest levels of emergency department visits for COVID, emphasizing the need for targeted preventive measures.
Wastewater SARS-CoV-2 tracking, another early indicator, continues to show high levels, especially in the Midwest, indicating the widespread presence of the virus in communities.

Wastewater COVID-19 National and Regional Trends
CDC’s National Wastewater Surveillance System, U.S. National trends
www.cdc.gov
CDC Director's Urgent Message
In a video message posted on Twitter, CDC Director Mandy Cohen, MD, MPH, emphasizes that it's not too late to be vaccinated against the three respiratory viruses - COVID-19, flu, and RSV. She urges the public to take additional preventive measures, including avoiding sick individuals, practicing regular hand hygiene, improving ventilation in indoor spaces, and wearing masks in crowded settings.
View: https://twitter.com/CDCDirector/status/1732547659292967203
Call to Action: Protecting Public Health During the Holidays
As the holiday season unfolds, health experts stress the importance of staying vigilant and prioritizing public health. Dr John Brownstein, an epidemiologist and chief innovation officer at Boston Children's Hospital, underscores the significance of practicing good hygiene, staying home when unwell, and ensuring proper ventilation in indoor spaces. He emphasizes that getting vaccinated and ensuring family members are vaccinated is the most significant gift individuals can give themselves and their communities during the holiday season.
In conclusion, the United States faces a multifaceted and challenging scenario with the convergence of rising COVID-19 infections, hospitalizations, and the emergence of the JN.1 subvariant. The public is urged to prioritize vaccination, adhere to preventive measures, and stay informed to navigate the evolving landscape of the pandemic. The holiday season, while bringing joy, underscores the need for a collective effort to safeguard public health and mitigate the impact of the ongoing health crisis.
~~~~~~~~~~~~~
View: https://twitter.com/CDCDirector/status/1732547659292967203
video at link 1 min 54 sec

naegling62
Veteran Member
I think we're are definitely in "oh shit" stage of this disease and vaccine.
Zoner
Veteran Member
@theheraldsun
Covid deaths in Victoria have soared to 166 in the most recent reporting period, with nearly 60 per cent of lives lost in a younger age bracket than before. It comes as a potentially dangerous new variant, JN. 1, surfaces in the state > https://bit.ly/46R9WBc
@mrmickme
As I've said before. JN.1 is a highly dangerous variant that can create a deadly systemic infection, once it successfully activates in the gut.
Covid deaths in Victoria have soared to 166 in the most recent reporting period, with nearly 60 per cent of lives lost in a younger age bracket than before. It comes as a potentially dangerous new variant, JN. 1, surfaces in the state > https://bit.ly/46R9WBc
@mrmickme
As I've said before. JN.1 is a highly dangerous variant that can create a deadly systemic infection, once it successfully activates in the gut.
Zoner
Veteran Member
https://twitter.com/BNOFeed
BNO News
@BNOFeed
22,513 Americans were hospitalized with COVID last week, up 18% from the week before.
BNO News
@BNOFeed
22,513 Americans were hospitalized with COVID last week, up 18% from the week before.
psychgirl
Has No Life - Lives on TB
@theheraldsun
Covid deaths in Victoria have soared to 166 in the most recent reporting period, with nearly 60 per cent of lives lost in a younger age bracket than before. It comes as a potentially dangerous new variant, JN. 1, surfaces in the state > https://bit.ly/46R9WBc
@mrmickme
As I've said before. JN.1 is a highly dangerous variant that can create a deadly systemic infection, once it successfully activates in the gut.
View: https://twitter.com/mrmickme/status/1733242038035128674
jed turtle
a brother in the Lord
From the same source Dr. Ana Maria Mihalcea MD….There is much more at the link :
Much more at link...
Methylene Blue Prevents Rubbery Clot Formation, Essential Oils Help Too - Experiment Documentation
….Note, that Polyamides ( Nylon), Polyethylene and Vinyl plastic polymers that Clifford Carnicom and I showed was in the rubbery clots, become hardened when the temperature drops. This could be the cause that the rubber clots develop with time after left to sit for a few hours or overnight and is also consistent with the observation of the embalmer Richard Hirschman that some of the clots appear to develop postmortem, when the body cools down. These most recent follow up tests show that adding Methylene Blue 50mg daily orally helps prevents the rubbery clots in vivo. It appears the essential oils also have some helpful effects. I will have to repeat the testing with essential oils on someone who does not take Methylene Blue…
For now, my frontrunners for the nanotechnology detox are
- EDTA for metal detox that are used for the biosensors and regenerating the red blood cell zeta potential to prevent clotting
- Vitamin C in high doses for clot prevention and regeneration of electical conductivity of the blood,
- Methylene Blue as clean up for the hydrogel and powerful electron donor.
- Essential Oils to disolve polymer plastics like styrene.
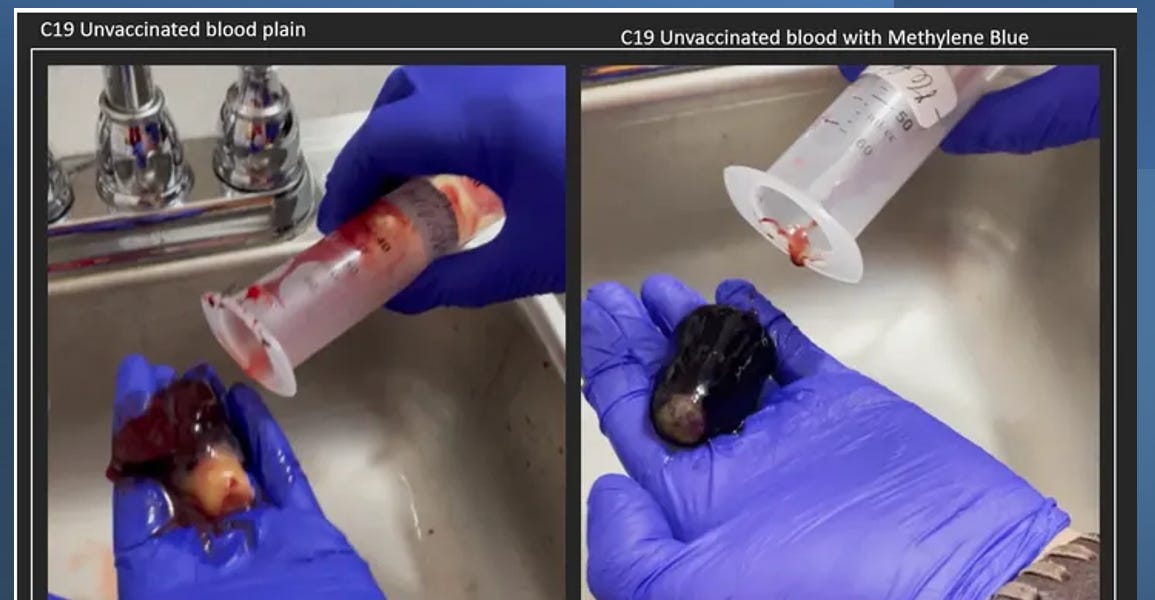
Methylene Blue Prevents Rubbery Clot Formation, Essential Oils Help Too - Experiment Documentation
Image: C19 uninjected blood on the right and same blood mixed with Methylene Blue I have previously posted experiments with C19 unvaccinated blood and Methylene Blue. The control was 30ml of C19 unvaccinated blood. The same individuals blood was mixed with Methylene Blue ( 0.5 cc of a 10mg/ml...
Weft and Warp
Senior Member
I just noticed this-- from the CDC site Risk Assessment Summary for SARS CoV-2 Sublineage BA.2.86 | CDC

Read the second sentence of the bottom paragraph......
Read the second sentence of the bottom paragraph......
Heliobas Disciple
TB Fanatic
Rare clotting effect of early COVID shots finally explained — what could that mean for future vaccines?
Scientists have offered a new explanation for why COVID-19 vaccines that contained adenoviruses carried a rare-but-serious risk of blood clotting.
Rare clotting effect of early COVID shots finally explained — what could that mean for future vaccines?
Scientists have offered a new explanation for why COVID-19 vaccines that contained adenoviruses carried a rare-but-serious risk of blood clotting.
By Stephanie Pappas
published 9 December 2023
Rare blood clots tied to some early COVID-19 vaccines that are no longer in use may have been the result of two out-of-control immune reactions happening at once.
One of these immune reactions was already known, but the second, reported Oct. 26 in the journal Blood, is a new discovery.
The finding could help to explain how other clotting conditions develop and point to better treatments, as well as suggest ways to make vaccines safer for people who are prone to the side effect.
"Understanding how a drug causes an adverse event allows us to design new approaches to make those treatments safer," said Ishac Nazy, an associate professor of medicine at McMaster University in Canada who studies the vaccine-related clotting disorder but was not involved in the current research.
A rare side effect
The vaccine-related clotting disorder, known as vaccine-induced immune thrombotic thrombocytopenia (VITT), was rare and linked to two shots: the Johnson & Johnson (J&J) and AstraZeneca COVID-19 vaccines. Both shots contained common-cold viruses called adenoviruses that were tweaked so that they couldn't infect cells. Instead, the modified viruses carried DNA instructions for part of SARS-CoV-2, the coronavirus that causes COVID-19, into the body.
VITT was a sobering side effect of what many public health experts had hoped would be a promising technology. Unlike the Moderna and Pfizer-BioNTech COVID-19 shots, which contain RNA, the J&J and AstraZeneca vaccines did not need ultracold storage, making them more accessible where cold-chain storage is unreliable. Adenovirus-based vaccines have been investigated for other diseases, but very few have achieved approval. Exceptions are an adenovirus-based Ebola vaccine approved in China and another approved by the European Union, both used only in at-risk individuals.
Soon after rolling out the J&J and AstraZeneca vaccines, doctors began reporting cases of clotting that looked a lot like a previously known disorder called Heparin-induced thrombocytopenia (HIT). About 20 to 30 years ago, HIT affected 3.5% of patients who had knee or hip replacements, said Dr. Andreas Greinacher, a physician who specializes in clotting disorders at the Greifswald University Hospital in Germany and was not involved in the new research. In these patients, heparin, a blood thinner normally given to prevent blood clots, actually triggered runaway clotting instead.
The adenovirus-based COVID vaccines were triggering the same condition as HIT, though scientists gave it a new acronym to reflect the different origin. Researchers reported that about 1 in 50,000 people under 50 who received the vaccine were affected, as well as about 1 in 100,000 of those 50 and older.
Neither vaccine is currently administered in the U.S. (AstraZeneca's shot was never used in the country, and J&J's vaccine was authorized but then retired due to the clotting issue and availability of better vaccines.) However, learning what triggers VITT could still be useful.
Today, HIT is rare because doctors now understand what causes it and can prescribe different, safer versions of heparin, Greinacher told Live Science. Similarly, he said, studying the mechanisms behind HIT and VITT could make adenovirus vaccines safer.
"Our big aim currently is to find which factor in the vaccines is triggering it," Greinacher said. "If you know the factor, I'm certain there are very smart biotechnologists who can modify the adenovirus vector so this factor is no longer present."
Unraveling VITT
When VITT was first observed in patients getting COVID-19 vaccines in February 2021, scientists soon discovered that it had to do with PF4, a chemical signal released by platelets, the blood cells that form clots.
In rare cases after vaccination with an adenovirus-based vaccine, the body would make antibodies to PF4. These antibodies would latch onto PF4 and form clumps that could then bind to receptors called Fc on other platelets. This would activate the platelets and lead to a runaway clotting response.
The new Blood study found that PF4 alone also activates a second set of receptors that cause platelets to accumulate, likely a second reason why clotting goes haywire in this disorder.
There is still a long way to go, Nazy told Live Science, whose team first reported in 2021 how antibodies against PF4 were causing VITT. The new research suggests that there are actually two different ways that PF4 acts in VITT, he said. These two pathways are not exclusive and may work in tandem.
In the new study, researchers tested blood from healthy individuals and people with VITT to trace the cascade of signals that leads to the overactive clotting. They found that the PF4 activates a receptor called c-Mpl on platelets, which causes them to clump together. This is in addition to the mechanism discovered in 2021, in which complexes of PF4 and PF4 antibodies activate platelets' Fc receptors.
"What we have shown is that as well as that antibody trigger, you've also got PF4 itself binding to platelets and activating them, providing a double whammy," Phillip Nicolson, an associate clinical professor of cardiovascular medicine at the University of Birmingham in the U.K. and the leader of the new study, told Live Science. "That may be why [the clotting] happens to a harmful degree."
Scientists have a few clues as to why adenovirus vaccines can trigger this response. PF4 carries a positive electrical charge on its surface, while adenoviruses are highly negatively charged, Nicolson said, so they may bind together easily. But even that is not confirmed, Nazy said, and has mostly been shown with computer modeling rather than with real molecules.
In rare cases, unusual clotting happens without vaccination or treatment with heparin. A recent paper published in the The New England Journal of Medicine, and co-authored by Nazy, found that in at least two of these unexplained clotting cases, the clotting disorder occurred after typical adenovirus infections. In many cases, the connection between unexplained clotting and a viral infection may be missed. And it's still a mystery why very few people are susceptible to these clotting conditions.
"That's the part we need to understand to prevent the disease from even happening," Nazy said.
Last edited:
Heliobas Disciple
TB Fanatic

COVID-19 hospitalizations are increasing in US, rates are highest among oldest and youngest Americans
COVID hospitalizations have been on the rise for nearly a month with rates highest among the oldest and youngest Americans, CDC data shows.
 abcnews.go.com
abcnews.go.com
COVID-19 hospitalizations are increasing in US, rates are highest among oldest and youngest Americans
As of Nov. 25, there were 19,444 weekly COVID hospitalizations, CDC data shows.
By Mary Kekatos and Youri Benadjaoud
December 8, 2023, 8:08 AM
For nearly a month, COVID-19 hospitalizations have been increasing following weeks of decline and relatively low levels throughout the summer, according to data from the Centers for Disease Control and Prevention (CDC).
As of Nov. 25, there were 19,444 weekly hospitalizations due to the virus compared to 15,006 four weeks earlier, data shows.
While this marks an increase of 29.6%, it is lower than the 150,650 weekly hospitalizations at the peak of the omicron wave during the 2021-22 season.
Rates of COVID hospitalizations remain elevated among senior citizens, middle-aged adults and children under age 4, meaning the virus is affecting both the oldest and youngest Americans.
"COVID has not disappeared, although it may have gone from many people's minds and the top of their attention," Dr. William Schaffner, a professor of preventive medicine at Vanderbilt University Medical Center, told ABC News. "I'm afraid the COVID virus is still very much with us."
He added, "These omicron variants and subvariants are highly contagious. They're causing lots of milder illness that does not require hospitalizations. However, there are substantial hospitalizations across the country."
Vaccine protection waning among seniors
Americans aged 65 and older have the highest rate of weekly hospitalizations of any age group in the U.S., as they have throughout the pandemic, at 13.5% per 100,000 for the week ending Dec. 2, CDC data shows.Experts said there are multiple reasons for this age group to have high rates of hospitalizations, including age being a risk factor for severe disease and senior citizens having more chronic underlying medical conditions that raise the risk of severe disease.

Weekly Rates of COVID-19 Hospitalizations
ABC News, CDC COVID-NET Surveillance System
Another reason is vaccine uptake and waning immunity. While 94.4% of adults aged 65 and older completed a primary series of the original vaccine, 33.3% of adults aged 65 and older have received the updated vaccine, according to CDC data.
"Many people, although they have been vaccinated in the past, have not taken advantage of this updated vaccine," Schaffner said. "And the protection afforded by the previous vaccinations is now slowly declining. And so, we have a highly vulnerable population whose protection is slowly waning."
Those aged 50 to 64 have the second-highest rate of weekly hospitalizations by age group at 2.7% per 100,000. Experts said, similarly, this is a group that is starting to see the emergence of chronic underlying conditions that raise the risk of severe illness from COVID.
Dr. Peter Chin-Hong, a professor of medicine and an infectious diseases expert at the University of California, San Francisco, said another reason middle-aged and older Americans have higher rates of hospitalization is that the most vulnerable among this group are not receiving treatments like Paxlovid. Reports have suggested that in some states, it's prescribed in less that 25% of cases.
"It represents a failure of our system to intervene and provide early therapy," Chin-Hong. "You can't really just blame vaccinations because there's a get out of jail card, which is Paxlovid and even remdesivir."
While only those at risk of severe illness are recommended to take Paxlovid, Chin-Hong said it's been a relatively underused treatment because some may feel they don't need the drug or doctors may feel hesitant to prescribe it due to concerns about how the medication interacts with other prescription drugs.
There's also some confusion about who pays for Paxlovid, Chin-Hong said. While it has been and will continue to be free through 2024 for people with Medicare or Medicaid, people with private insurance may have co-pays associated with the drug now that it will no longer be purchased and distributed by the government.
Young kids also at risk of severe illness
Infants and young children under age 4 have the third-highest rate of hospitalizations by age group at 1.6% per 100,000 for the week ending Dec. 2, CDC data shows.Although children are less likely to fall severely ill and die from COVID compared to adults, they can get sick enough to be hospitalized.
Schaffner said it's a fallacy for a parent to think their child does not need to get vaccinated because they are relatively healthy because children can fall severely ill. What's more, studies have shown that COVID vaccines do decrease hospitalizations among kids.
"It has been very difficult for people to keep two apparently conflicting notions in their mind at the same time," Schaffner said. "First, everyone knows that children are less apt to be seriously affected by COVID infections than older adults. The alternate concept that is hard for parents to grasp is that nonetheless, young children account for the third most common age group with hospitalizations."
Chin-Hong said that parents are less hesitant to get their children vaccinated against influenza than against COVID-19. As of Nov. 18, 38.2% of children aged 6 months to 17 years have gotten a flu shot, CDC data shows. Comparatively, 6.9% of children have gotten an updated COVID vaccine as of Nov. 25.
"More than double are getting flu shots," he said. "So, it's not that everybody's saying, 'No' to vaccines. They're being selective."
While COVID has not followed a traditional seasonal trend like flu, experts say that for all age groups, increases in hospitalizations have occurred during the colder months when people begin to stay indoors, heat is turned up, windows are closed, and holiday gatherings people bring people together -- "ideal conditions for respiratory viruses to spread," said Dr. John Brownstein, an epidemiologist and chief innovation officer at Boston Children's Hospital and an ABC News contributor.
"As people gather for the holidays, it's crucial to remain vigilant about COVID-19, especially in protecting vulnerable populations like the elderly and infants," Brownstein continued. "Practicing good hygiene, such as regular hand washing, and staying home if feeling unwell are key. Additionally, ensuring proper ventilation in indoor spaces and considering wearing masks in crowded settings can significantly reduce the risk of transmission."
The experts also advised the importance of staying up to date on COVID-19 vaccinations and said it's not too late to get a shot.
"Seriously, make a plan and do it as quickly as possible," Schaffner said. "Getting yourself vaccinated and making sure your family members are vaccinated, that's without a doubt -- and I mean, this sincerely -- the best present, you can give yourself and give to them this holiday season, and you will help also make your neighborhood and your community safer."
Last edited:
Zoner
Veteran Member
I suspect that JN.1 has found the holy grail of recombination opportunities in our guts, to take its evolutionary capabilities to the next level. I expect it will stay in the gut and continue mixing and matching in there to spawn out ever fitter recombos.
Heliobas Disciple
TB Fanatic
Former Biden COVID official says Wuhan lab leak may have caused pandemic
The official also warned that the chances of another global pandemic are quite high.
Former Biden COVID official says Wuhan lab leak may have caused pandemic
The official also warned that the chances of another global pandemic are quite high.
By Madeline Hubbard
December 10, 2023
Dr. Raj Panjabi, the former top White House national security council pandemic official, said that COVID-19 may have originated in Wuhan, China, as the result of a lab leak.
"It is plausible that Covid originated in a lab accident in Wuhan," Panjabi said last week at the annual Forbes Healthcare Summit, The Daily Mail reported. "We have got to do more to keep labs safe."
He also warned that the world is facing a growing risk of future pandemics.
"There is a 50 percent risk one will happen in the next 25 years. This is because of globalization, or what I call the three Ps," he said.
The "three Ps" he gave are "pathogen spillover," when diseases leap from animals to humans; "planes," since they encourage global travel; and "poor public health systems that are shattered and lack investment."
The Wuhan Institute of Virology was under scrutiny even before the COVID-19 pandemic since it had not provided information about safety and security as required after having received U.S. government funding.
The U.S. government has appeared split on whether COVID originated in a lab or naturally.
Heliobas Disciple
TB Fanatic
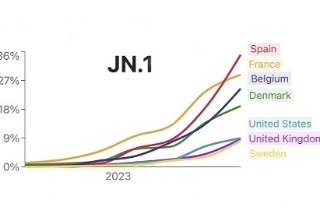
COVID-19 News: BA.2.86 Spawns Such As JN.1, JN.1.1 And Recombinant Like XDD Increasing In Circulation Rapidly! Concerns Raised About Monovalent Jabs! - Thailand Medical News
Expect A Situation Worse Than During The Delta Surge In The Next Few Weeks. Hospitalizations And Deaths Expected To Rise Exponentially Along With Severe Long COVID Issues! Besides JN.1, Expect Sudden Emergence Of Other Fast Spreading Sub-lineages Of BA.2.86 and JN.1 That Are More Pathogenic...
www.thailandmedical.news
BA.2.86 Spawns Such As JN.1, JN.1.1 And Recombinant Like XDD Increasing In Circulation Rapidly. Concerns Raised About Monovalent Jabs
Nikhil Prasad Fact checked by:Thailand Medical News Team
Dec 10, 2023
Expect A Situation Worse Than During The Delta Surge In The Next Few Weeks. Hospitalizations And Deaths Expected To Rise Exponentially Along With Severe Long COVID Issues. Besides JN.1, Expect Sudden Emergence Of Other Fast Spreading Sub-lineages Of BA.2.86 and JN.1 That Are More Pathogenic. Surge Also Expected To Last For A Longer Period This Time Round
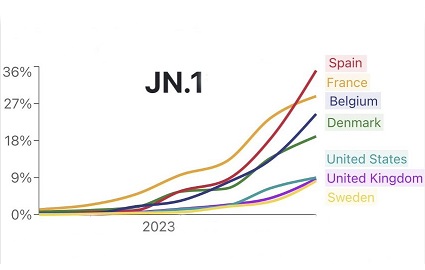
When the hypermutated BA.2.86 variant was identified in mid-August 2023, many so called ‘experts’ said that that the BA.2.86 and its spawns are unlikely to be a threat and that it will unlikely spread.
Should you be concerned about BA.2.86?
Early lab tests suggest new COVID-19 variant BA.2.86 may be less contagious and less immune-evasive than feared
New COVID-19 Variants BA.2.86 and EG.5.1 Not a Threat to Indians
Should you be worried about latest COVID variant? Will the new vaccines fight BA.2.86?
One study published in Nature journal even claimed that BA.2.86 variant had no potential to spread.
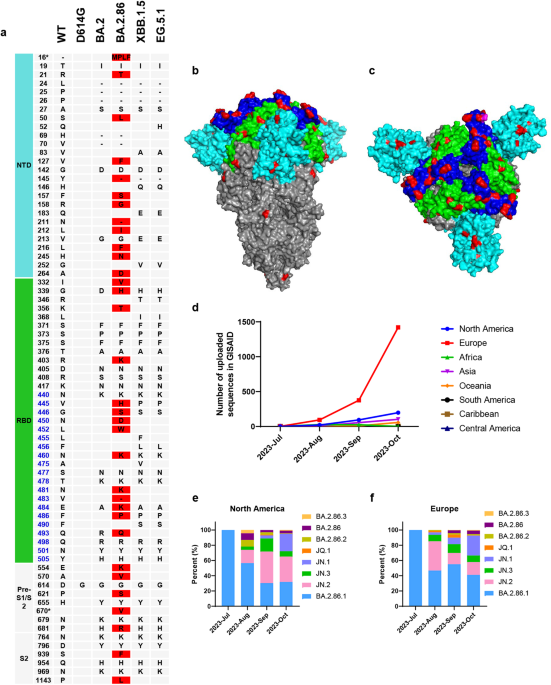
Fast forward to day..unknown to most people the BA.2.86 variant has spawned more than 370 different kinds of sub-lineages of varying viral fitness, transmissibility and immune evasiveness with the most well-known ones being JN.1 JN.1.1, JN.2, JN.3, JN.1.2, etc.
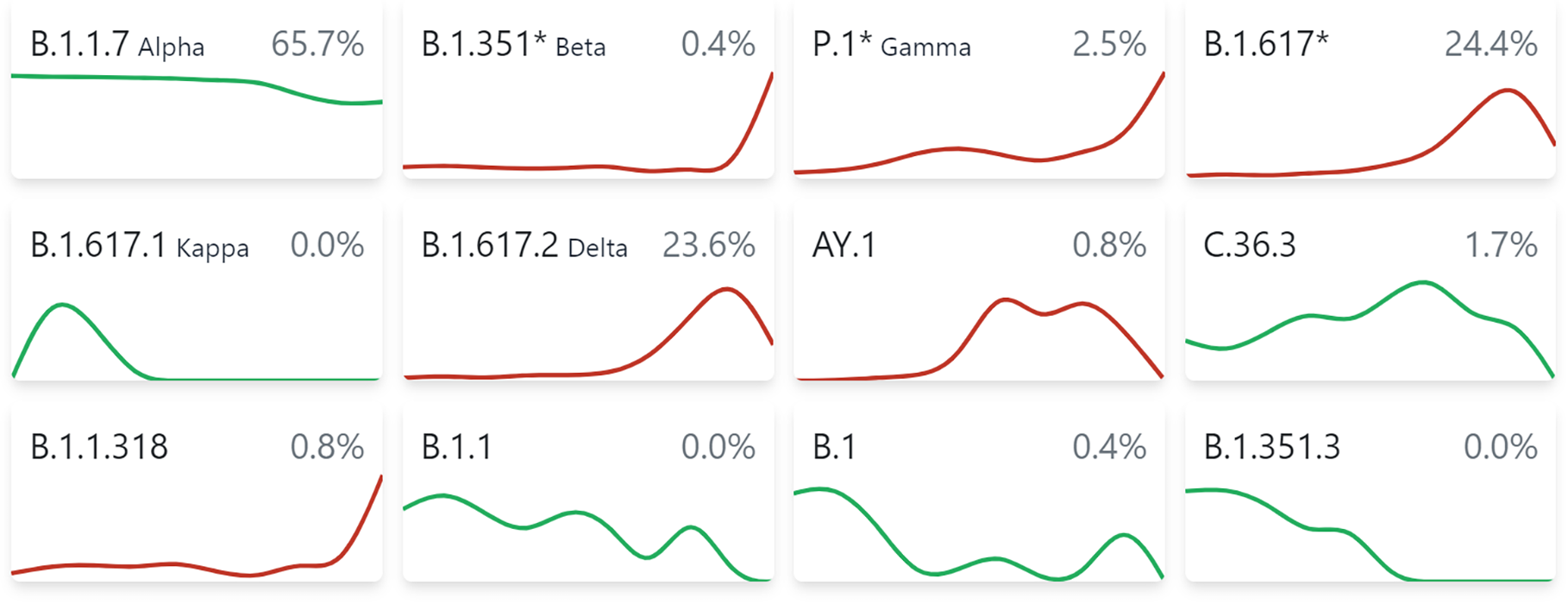
covSPECTRUM
covSPECTRUM is an interactive platform aiming to help scientists investigate and identify variants of SARS-CoV-2.
 cov-spectrum.org
cov-spectrum.org
covSPECTRUM
covSPECTRUM
covSPECTRUM
(Note not all data can be found on CoV-spectrum as it is not updated timely, refer to GISAID to isolate such BA.2.86 sub-lineages)
It has even led to the emergence of a recombinant variant called XDD that involved the BA.2.86 and the EG.5.1.1 (An XBB Sub-lineage ).
XDD: EG.5.1.1*(HK)/JN.1 recombinant, 50 samples, 13 countries · Issue #1024 · sars-cov-2-variants/lineage-proposals
Description: HK.3/JN.1 recombinant, 2 breaking points, Spike from JN.1 Private mutations: none Breakpoint: First between nucleotide 6541 - 7842, second 25416 - 26270 One sequence from: 2023-03-29 f...
 github.com
github.com
The JN.1 variant is not only spreading exponentially across the world and becoming the predominant circulating variant but many of the other BA.2.86 spawns are also slowly gaining a foothold!
In fact, the U.S. CDC has recently even admitted that the JN.1 variant could be the most transmissible variant to date and could also be the most immune evasive variant so far in its latest variant updates issued a few days ago.
Many of the various agencies, ‘experts’ and corrupted mainstream media and news agencies under the direct or indirect payroll of the vaccine manufacturers and the WEF including the WHO, US,.CDC, ECDC had kept on advocating that the latest monovalent vaccine containing the XBB.1.5 spike proteins would be able to provide protection against the BA.2.86 variant and its spawns.
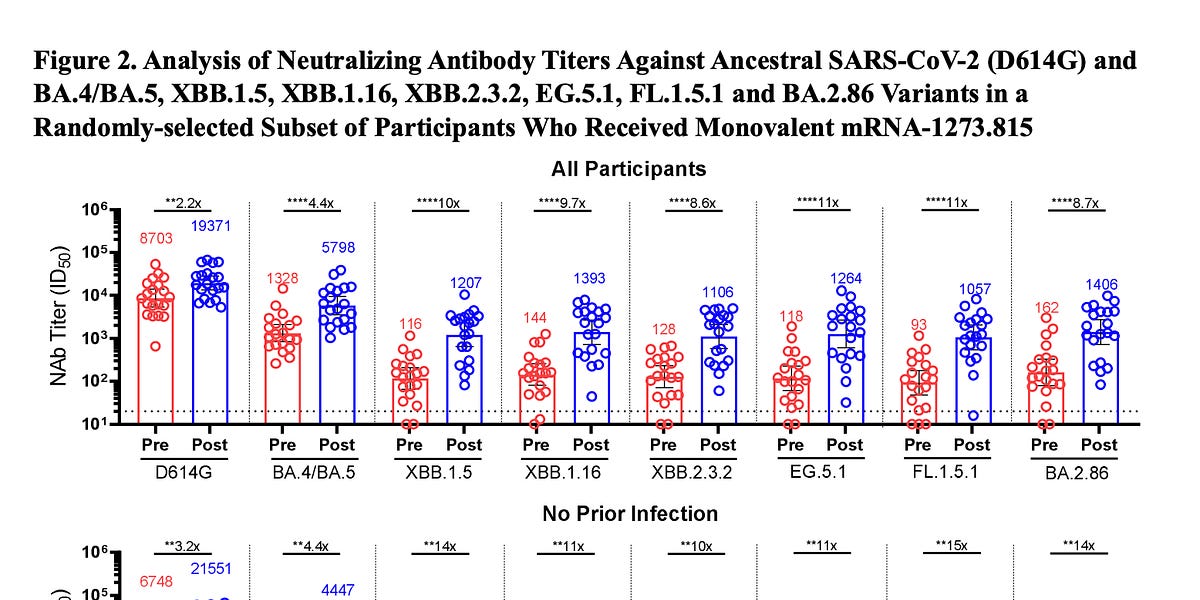
The BA.2.86 variant and the new booster
Facts, data, and analytics about biomedical matters.
 erictopol.substack.com
erictopol.substack.com
Moderna, Pfizer say updated COVID shots generate strong response vs newer variant
BA.2.86 and EG.5: How will the new COVID-19 boosters work with new variants?
View: https://twitter.com/CDCgov/status/1733252642128748768
However, a Japanese study published in early December that was covered in a COVID-19 News report in Thailand Medical News did warn that the XBB1.5 monovalent vaccine might not be effective against the BA.286 variant and its emerging spawns.
BREAKING COVID-19 News! Japanese Study Reveals That New XBB.1.5 Monovalent XBB.1.5 Is Not Effective Against Circulating SARS-CoV-2 Variants! - Thailand Medical News
Many of the agencies like the WHO, U.S. CDC and also various other garbage health authorities and experts also kept on insisting that the BA.2.86 and its spawns are not driving disease severity despite data showing that where JN.1 is increasing in dominance of circulation, hospitalizations are also rising.

What you need to know about BA.2.86, the new ‘highly mutated’ COVID variant
The highly mutated BA.2.86 "Pirola" variant is spreading quickly in the US. Here's what we know about its transmissibility, ability to escapte immunity, and boosters this fall.
 www.today.com
www.today.com
Update on SARS-CoV-2 Variant JN.1 | CDC
https://www.thailandmedical.news/ne...ns-and-hospitalizations-rise-in-united-states
A latest study update by the same Japanese research lab that issued the warnings about the possibly ineffectiveness of the monovalent XBB.1.5 vaccine against the BA.2.86 variant but this time focusing on the JN.1 variant has indeed shown that the current XBB1.5 monovalent vaccine is unlikely to protect against the JN.1 variant and its emerging sub-lineages.
Virological characteristics of the SARS-CoV-2 JN.1 variant
The SARS-CoV-2 BA.2.86 lineage, first identified in August 2023, is phylogenetically distinct from the currently circulating SARS-CoV-2 Omicron XBB lineages, including EG.5.1 and HK.3. Comparing to XBB and BA.2, BA.2.86 carries more than 30 mutations in the spike (S) protein, indicating a high...
 www.biorxiv.org
www.biorxiv.org
View: https://twitter.com/SystemsVirology/status/1733661271445385626
Meanwhile preliminary data from studies underway that have yet to be published are showing that the JN.1 variant and its sub-lineages are better enhanced at utilizing the TMPRSS2 and ACE-2 receptors.
View: https://twitter.com/dronico/status/1731621226735415742
View: https://twitter.com/dronico/status/1732141782039966213
Case reports and studies underway are also showing that JN.1 and its newer sub-lineages are causing more serious lower respiratory infections and also affecting the gastrointestinal tract more.
Other studies underway show that it is also better adapt at using the NRP1 receptor hence possibly leading to better infections involving the brain and the CNS system. Yet another study underway shows that JN.1 and its newer sub-lineages can even use the bind to the nectin-1 & -2 & 3-O sulfated heparan sulfate (3-OS HS) receptors that are found in various ocular cell types.
Interestingly, we are seeing people infected with the JN.1 variant or its newer sub-lineages manifesting persistent coughs, chest pains, breathing issues, chronic fatigue and weakness headaches and body pains and vision issues along with abdominal issues, diarrhea and loss of appetite.
Some individuals do not express disease severity during initial stages of infections but develop other serious health issues later that required hospitalization. (This could be due to the fact that JN.1 and its newer sub-lineages are excellent at immune evasiveness and disarming the initial immune responses but still causing damage to various cells and cellular pathways.)
The JN.1 variant is now becoming predominant in various parts of the world including Singapore, France, Belgium, Denmark, Canada, Australia, the United States, Brazil etc.
View: https://twitter.com/theheraldsun/status/1732965732991042025
View: https://twitter.com/njasbech/status/1732691393498218594
View: https://twitter.com/juanitron777/status/1732553063775281428
View: https://twitter.com/AussieSteve6/status/1733726385561280572
View: https://twitter.com/RajlabN/status/1733734948404600940/photo/1
View: https://twitter.com/RajlabN/status/1730849022884147591
View: https://twitter.com/BarryHunt008/status/1733674290552172966
View: https://twitter.com/MarioNawfal/status/1733002625790923013
There are also speculation that the Mysterious White Lung Pneumonia seen in China and elsewhere and where Mycoplasma Pneumoniae has been blamed for it..... is actually caused by newer sub-lineages of JN.1, where they are not only causing lung damage but also causing rapid depletion of the immune system, paying the way for secondary opportunistic infections for the lungs including Mycoplasma Penumoniae, other fungus infections and even other viral and bacterial pathogens.
We can expect to see more fun in coming weeks but again note that we are expecting a very interesting announcement a few days before Christmas.
Zoner
Veteran Member
(fair use applies)COVID-19 News: BA.2.86 Spawns Such As JN.1, JN.1.1 And Recombinant Like XDD Increasing In Circulation Rapidly! Concerns Raised About Monovalent Jabs! - Thailand Medical News
Expect A Situation Worse Than During The Delta Surge In The Next Few Weeks. Hospitalizations And Deaths Expected To Rise Exponentially Along With Severe Long COVID Issues! Besides JN.1, Expect Sudden Emergence Of Other Fast Spreading Sub-lineages Of BA.2.86 and JN.1 That Are More Pathogenic...
BA.2.86 Spawns Such As JN.1, JN.1.1 And Recombinant Like XDD Increasing In Circulation Rapidly. Concerns Raised About Monovalent Jabs
Nikhil Prasad Fact checked by:Thailand Medical News Team
Dec 10, 2023
Expect A Situation Worse Than During The Delta Surge In The Next Few Weeks. Hospitalizations And Deaths Expected To Rise Exponentially Along With Severe Long COVID Issues. Besides JN.1, Expect Sudden Emergence Of Other Fast Spreading Sub-lineages Of BA.2.86 and JN.1 That Are More Pathogenic. Surge Also Expected To Last For A Longer Period This Time Round
When the hypermutated BA.2.86 variant was identified in mid-August 2023, many so called ‘experts’ said that that the BA.2.86 and its spawns are unlikely to be a threat and that it will unlikely spread.
Should you be concerned about BA.2.86?
Early lab tests suggest new COVID-19 variant BA.2.86 may be less contagious and less immune-evasive than feared
New COVID-19 Variants BA.2.86 and EG.5.1 Not a Threat to Indians
Should you be worried about latest COVID variant? Will the new vaccines fight BA.2.86?
One study published in Nature journal even claimed that BA.2.86 variant had no potential to spread.
Fast forward to day..unknown to most people the BA.2.86 variant has spawned more than 370 different kinds of sub-lineages of varying viral fitness, transmissibility and immune evasiveness with the most well-known ones being JN.1 JN.1.1, JN.2, JN.3, JN.1.2, etc.
covSPECTRUM
covSPECTRUM is an interactive platform aiming to help scientists investigate and identify variants of SARS-CoV-2.
covSPECTRUM
covSPECTRUM
covSPECTRUM
(Note not all data can be found on CoV-spectrum as it is not updated timely, refer to GISAID to isolate such BA.2.86 sub-lineages)
It has even led to the emergence of a recombinant variant called XDD that involved the BA.2.86 and the EG.5.1.1 (An XBB Sub-lineage ).

XDD: EG.5.1.1*(HK)/JN.1 recombinant, 50 samples, 13 countries · Issue #1024 · sars-cov-2-variants/lineage-proposals
Description: HK.3/JN.1 recombinant, 2 breaking points, Spike from JN.1 Private mutations: none Breakpoint: First between nucleotide 6541 - 7842, second 25416 - 26270 One sequence from: 2023-03-29 f...
The JN.1 variant is not only spreading exponentially across the world and becoming the predominant circulating variant but many of the other BA.2.86 spawns are also slowly gaining a foothold!
In fact, the U.S. CDC has recently even admitted that the JN.1 variant could be the most transmissible variant to date and could also be the most immune evasive variant so far in its latest variant updates issued a few days ago.
Many of the various agencies, ‘experts’ and corrupted mainstream media and news agencies under the direct or indirect payroll of the vaccine manufacturers and the WEF including the WHO, US,.CDC, ECDC had kept on advocating that the latest monovalent vaccine containing the XBB.1.5 spike proteins would be able to provide protection against the BA.2.86 variant and its spawns.
The BA.2.86 variant and the new booster
Facts, data, and analytics about biomedical matters.
Moderna, Pfizer say updated COVID shots generate strong response vs newer variant
BA.2.86 and EG.5: How will the new COVID-19 boosters work with new variants?
View: https://twitter.com/CDCgov/status/1733252642128748768
However, a Japanese study published in early December that was covered in a COVID-19 News report in Thailand Medical News did warn that the XBB1.5 monovalent vaccine might not be effective against the BA.286 variant and its emerging spawns.
BREAKING COVID-19 News! Japanese Study Reveals That New XBB.1.5 Monovalent XBB.1.5 Is Not Effective Against Circulating SARS-CoV-2 Variants! - Thailand Medical News
Many of the agencies like the WHO, U.S. CDC and also various other garbage health authorities and experts also kept on insisting that the BA.2.86 and its spawns are not driving disease severity despite data showing that where JN.1 is increasing in dominance of circulation, hospitalizations are also rising.
What you need to know about BA.2.86, the new ‘highly mutated’ COVID variant
The highly mutated BA.2.86 "Pirola" variant is spreading quickly in the US. Here's what we know about its transmissibility, ability to escapte immunity, and boosters this fall.
Update on SARS-CoV-2 Variant JN.1 | CDC
BREAKING COVID-19 News! U.S. CDC Admits That JN.1 Is Possibly More Transmissible As Infections And Hospitalizations Rise In United States! - Thailand Medical News
A latest study update by the same Japanese research lab that issued the warnings about the possibly ineffectiveness of the monovalent XBB.1.5 vaccine against the BA.2.86 variant but this time focusing on the JN.1 variant has indeed shown that the current XBB1.5 monovalent vaccine is unlikely to protect against the JN.1 variant and its emerging sub-lineages.

Virological characteristics of the SARS-CoV-2 JN.1 variant
The SARS-CoV-2 BA.2.86 lineage, first identified in August 2023, is phylogenetically distinct from the currently circulating SARS-CoV-2 Omicron XBB lineages, including EG.5.1 and HK.3. Comparing to XBB and BA.2, BA.2.86 carries more than 30 mutations in the spike (S) protein, indicating a high...
View: https://twitter.com/SystemsVirology/status/1733661271445385626
Meanwhile preliminary data from studies underway that have yet to be published are showing that the JN.1 variant and its sub-lineages are better enhanced at utilizing the TMPRSS2 and ACE-2 receptors.
View: https://twitter.com/dronico/status/1731621226735415742
View: https://twitter.com/dronico/status/1732141782039966213
Case reports and studies underway are also showing that JN.1 and its newer sub-lineages are causing more serious lower respiratory infections and also affecting the gastrointestinal tract more.
Other studies underway show that it is also better adapt at using the NRP1 receptor hence possibly leading to better infections involving the brain and the CNS system. Yet another study underway shows that JN.1 and its newer sub-lineages can even use the bind to the nectin-1 & -2 & 3-O sulfated heparan sulfate (3-OS HS) receptors that are found in various ocular cell types.
Interestingly, we are seeing people infected with the JN.1 variant or its newer sub-lineages manifesting persistent coughs, chest pains, breathing issues, chronic fatigue and weakness headaches and body pains and vision issues along with abdominal issues, diarrhea and loss of appetite.
Some individuals do not express disease severity during initial stages of infections but develop other serious health issues later that required hospitalization. (This could be due to the fact that JN.1 and its newer sub-lineages are excellent at immune evasiveness and disarming the initial immune responses but still causing damage to various cells and cellular pathways.)
The JN.1 variant is now becoming predominant in various parts of the world including Singapore, France, Belgium, Denmark, Canada, Australia, the United States, Brazil etc.
View: https://twitter.com/theheraldsun/status/1732965732991042025
View: https://twitter.com/njasbech/status/1732691393498218594
View: https://twitter.com/juanitron777/status/1732553063775281428
View: https://twitter.com/AussieSteve6/status/1733726385561280572
View: https://twitter.com/RajlabN/status/1733734948404600940/photo/1
View: https://twitter.com/RajlabN/status/1730849022884147591
View: https://twitter.com/BarryHunt008/status/1733674290552172966
View: https://twitter.com/MarioNawfal/status/1733002625790923013
There are also speculation that the Mysterious White Lung Pneumonia seen in China and elsewhere and where Mycoplasma Pneumoniae has been blamed for it..... is actually caused by newer sub-lineages of JN.1, where they are not only causing lung damage but also causing rapid depletion of the immune system, paying the way for secondary opportunistic infections for the lungs including Mycoplasma Penumoniae, other fungus infections and even other viral and bacterial pathogens.
We can expect to see more fun in coming weeks but again note that we are expecting a very interesting announcement a few days before Christmas.
This is an excellent post HD!! So much is in here ... I really think you should post this in a new thread. The members of TB2K need to see this before it gets buried. Thank you!
Zoner
Veteran Member
(fair use applies)COVID-19 News: BA.2.86 Spawns Such As JN.1, JN.1.1 And Recombinant Like XDD Increasing In Circulation Rapidly! Concerns Raised About Monovalent Jabs! - Thailand Medical News
Expect A Situation Worse Than During The Delta Surge In The Next Few Weeks. Hospitalizations And Deaths Expected To Rise Exponentially Along With Severe Long COVID Issues! Besides JN.1, Expect Sudden Emergence Of Other Fast Spreading Sub-lineages Of BA.2.86 and JN.1 That Are More Pathogenic...
BA.2.86 Spawns Such As JN.1, JN.1.1 And Recombinant Like XDD Increasing In Circulation Rapidly. Concerns Raised About Monovalent Jabs
Nikhil Prasad Fact checked by:Thailand Medical News Team
Dec 10, 2023
Expect A Situation Worse Than During The Delta Surge In The Next Few Weeks. Hospitalizations And Deaths Expected To Rise Exponentially Along With Severe Long COVID Issues. Besides JN.1, Expect Sudden Emergence Of Other Fast Spreading Sub-lineages Of BA.2.86 and JN.1 That Are More Pathogenic. Surge Also Expected To Last For A Longer Period This Time Round
When the hypermutated BA.2.86 variant was identified in mid-August 2023, many so called ‘experts’ said that that the BA.2.86 and its spawns are unlikely to be a threat and that it will unlikely spread.
Should you be concerned about BA.2.86?
Early lab tests suggest new COVID-19 variant BA.2.86 may be less contagious and less immune-evasive than feared
New COVID-19 Variants BA.2.86 and EG.5.1 Not a Threat to Indians
Should you be worried about latest COVID variant? Will the new vaccines fight BA.2.86?
One study published in Nature journal even claimed that BA.2.86 variant had no potential to spread.
Fast forward to day..unknown to most people the BA.2.86 variant has spawned more than 370 different kinds of sub-lineages of varying viral fitness, transmissibility and immune evasiveness with the most well-known ones being JN.1 JN.1.1, JN.2, JN.3, JN.1.2, etc.
covSPECTRUM
covSPECTRUM is an interactive platform aiming to help scientists investigate and identify variants of SARS-CoV-2.
covSPECTRUM
covSPECTRUM
covSPECTRUM
(Note not all data can be found on CoV-spectrum as it is not updated timely, refer to GISAID to isolate such BA.2.86 sub-lineages)
It has even led to the emergence of a recombinant variant called XDD that involved the BA.2.86 and the EG.5.1.1 (An XBB Sub-lineage ).
XDD: EG.5.1.1*(HK)/JN.1 recombinant, 50 samples, 13 countries · Issue #1024 · sars-cov-2-variants/lineage-proposals
Description: HK.3/JN.1 recombinant, 2 breaking points, Spike from JN.1 Private mutations: none Breakpoint: First between nucleotide 6541 - 7842, second 25416 - 26270 One sequence from: 2023-03-29 f...
The JN.1 variant is not only spreading exponentially across the world and becoming the predominant circulating variant but many of the other BA.2.86 spawns are also slowly gaining a foothold!
In fact, the U.S. CDC has recently even admitted that the JN.1 variant could be the most transmissible variant to date and could also be the most immune evasive variant so far in its latest variant updates issued a few days ago.
Many of the various agencies, ‘experts’ and corrupted mainstream media and news agencies under the direct or indirect payroll of the vaccine manufacturers and the WEF including the WHO, US,.CDC, ECDC had kept on advocating that the latest monovalent vaccine containing the XBB.1.5 spike proteins would be able to provide protection against the BA.2.86 variant and its spawns.
The BA.2.86 variant and the new booster
Facts, data, and analytics about biomedical matters.
Moderna, Pfizer say updated COVID shots generate strong response vs newer variant
BA.2.86 and EG.5: How will the new COVID-19 boosters work with new variants?
View: https://twitter.com/CDCgov/status/1733252642128748768
However, a Japanese study published in early December that was covered in a COVID-19 News report in Thailand Medical News did warn that the XBB1.5 monovalent vaccine might not be effective against the BA.286 variant and its emerging spawns.
BREAKING COVID-19 News! Japanese Study Reveals That New XBB.1.5 Monovalent XBB.1.5 Is Not Effective Against Circulating SARS-CoV-2 Variants! - Thailand Medical News
Many of the agencies like the WHO, U.S. CDC and also various other garbage health authorities and experts also kept on insisting that the BA.2.86 and its spawns are not driving disease severity despite data showing that where JN.1 is increasing in dominance of circulation, hospitalizations are also rising.
What you need to know about BA.2.86, the new ‘highly mutated’ COVID variant
The highly mutated BA.2.86 "Pirola" variant is spreading quickly in the US. Here's what we know about its transmissibility, ability to escapte immunity, and boosters this fall.
Update on SARS-CoV-2 Variant JN.1 | CDC
BREAKING COVID-19 News! U.S. CDC Admits That JN.1 Is Possibly More Transmissible As Infections And Hospitalizations Rise In United States! - Thailand Medical News
A latest study update by the same Japanese research lab that issued the warnings about the possibly ineffectiveness of the monovalent XBB.1.5 vaccine against the BA.2.86 variant but this time focusing on the JN.1 variant has indeed shown that the current XBB1.5 monovalent vaccine is unlikely to protect against the JN.1 variant and its emerging sub-lineages.
Virological characteristics of the SARS-CoV-2 JN.1 variant
The SARS-CoV-2 BA.2.86 lineage, first identified in August 2023, is phylogenetically distinct from the currently circulating SARS-CoV-2 Omicron XBB lineages, including EG.5.1 and HK.3. Comparing to XBB and BA.2, BA.2.86 carries more than 30 mutations in the spike (S) protein, indicating a high...
View: https://twitter.com/SystemsVirology/status/1733661271445385626
Meanwhile preliminary data from studies underway that have yet to be published are showing that the JN.1 variant and its sub-lineages are better enhanced at utilizing the TMPRSS2 and ACE-2 receptors.
View: https://twitter.com/dronico/status/1731621226735415742
View: https://twitter.com/dronico/status/1732141782039966213
Case reports and studies underway are also showing that JN.1 and its newer sub-lineages are causing more serious lower respiratory infections and also affecting the gastrointestinal tract more.
Other studies underway show that it is also better adapt at using the NRP1 receptor hence possibly leading to better infections involving the brain and the CNS system. Yet another study underway shows that JN.1 and its newer sub-lineages can even use the bind to the nectin-1 & -2 & 3-O sulfated heparan sulfate (3-OS HS) receptors that are found in various ocular cell types.
Interestingly, we are seeing people infected with the JN.1 variant or its newer sub-lineages manifesting persistent coughs, chest pains, breathing issues, chronic fatigue and weakness headaches and body pains and vision issues along with abdominal issues, diarrhea and loss of appetite.
Some individuals do not express disease severity during initial stages of infections but develop other serious health issues later that required hospitalization. (This could be due to the fact that JN.1 and its newer sub-lineages are excellent at immune evasiveness and disarming the initial immune responses but still causing damage to various cells and cellular pathways.)
The JN.1 variant is now becoming predominant in various parts of the world including Singapore, France, Belgium, Denmark, Canada, Australia, the United States, Brazil etc.
View: https://twitter.com/theheraldsun/status/1732965732991042025
View: https://twitter.com/njasbech/status/1732691393498218594
View: https://twitter.com/juanitron777/status/1732553063775281428
View: https://twitter.com/AussieSteve6/status/1733726385561280572
View: https://twitter.com/RajlabN/status/1733734948404600940/photo/1
View: https://twitter.com/RajlabN/status/1730849022884147591
View: https://twitter.com/BarryHunt008/status/1733674290552172966
View: https://twitter.com/MarioNawfal/status/1733002625790923013
There are also speculation that the Mysterious White Lung Pneumonia seen in China and elsewhere and where Mycoplasma Pneumoniae has been blamed for it..... is actually caused by newer sub-lineages of JN.1, where they are not only causing lung damage but also causing rapid depletion of the immune system, paying the way for secondary opportunistic infections for the lungs including Mycoplasma Penumoniae, other fungus infections and even other viral and bacterial pathogens.
We can expect to see more fun in coming weeks but again note that we are expecting a very interesting announcement a few days before Christmas.
This seems to me, to be what Geert was talking about. It's here... He said we'll know because the hospitalizations will go thru the roof. I just ordered more Vitamin C powder which is about the best thing you can do ...after mainlining it. But I hope everyone has their Ivermectin, Zinc/Quercitin ready. You don't want this Variant. And Pray Psalm 91
Last edited:
psychgirl
Has No Life - Lives on TB
I just read it too, and agree.This is an excellent post HD!! So much is in here ... I really think you should post this in a new thread. The members of TB2K need to see this before it gets buried. Thank you!
Get ready for the “naysayers and laugh emojis” though.
The reason this article sticks out to me is that I’ve known of people who had those exact severe Covid symptoms including the severe GI aspects but they’ve all tested negative for Covid.
I don’t think the current tests are picking it up; I think in general the tests are almost worthless but this particular variant is severe.
If people are negative they are more apt to ignore the initial symptons and not treat it fast enough!