www.theepochtimes.com
(fair use applies)
Conflicting Evidence of mRNA Technology Raises Serious Concerns About Rush for Use in New Vaccine Development
Megan Redshaw, J.D.
Aug 31 2023
The U.S. government and pharmaceutical companies are investing a substantial amount to develop new mRNA vaccines for infectious diseases and cancer, fueling a lucrative mRNA platform valued at $136.2 billion.
A newly established White House program announced on Aug. 23 that it is granting a total of $25 million over three years to Emory University, Yale School of Medicine, and the University of Georgia to develop personalized therapeutic vaccines against cancers and emerging infections, similar to how COVID-19 mRNA vaccines target SARS-CoV-2. They aim to use mRNA—an essential element in COVID-19 vaccines developed to prevent SARS-CoV-2 infections—to program a unique class of immune cells called dendritic cells to initiate a desired immunological response.
Pharmaceutical companies such as Moderna, BioNTech, and CureVac are conducting clinical trials using mRNA-based vaccines with advanced melanoma, ovarian, colorectal, and pancreatic cancers. The National Institutes of Health is partnering with BioNTech to develop a personalized vaccine for pancreatic cancers. In addition to COVID-19 and cancer, other mRNA-based vaccines in development target influenza, genital herpes, respiratory viruses, and shingles.
Although mRNA platforms are appealing because they reduce costs and shorten the vaccine development timeline, evidence and experience suggest the mRNA technology used for novel COVID-19 vaccines is associated with various harms and neither prevents COVID-19 nor its transmission.
Evidence Challenging Vaccine ‘Safe and Effective’ Narrative
The unprecedented rates of adverse events following COVID-19 vaccination overshadow the benefits, according to researchers from Australia who say the SARS-CoV-2 spike protein, whether from the virus or created from genetic code in mRNA and adenovectorDNA vaccines, is toxic and causes a wide array of diseases.
In their recently published paper published in Biomedicines titled, “‘Spikeopathy’: COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA,” the researchers explored peer-reviewed data countering the “safe and effective” narrative attached to new technologies used to develop mRNA and adenovectorDNA vaccines at “warp speed” to end the pandemic.
Spike protein pathogenicity, termed “spikeopathy,” describes the ability of the spike protein to cause disease, and the researchers say it can affect many organ systems.
Researchers noted the following key problem areas:
- Spike protein toxicity (spikeopathy) from both the virus and when produced by gene codes in people vaccinated with COVID-19 vaccines.
- Inflammatory properties in specific lipid nanoparticles (LNPs) used to transport mRNA.
- Long-lasting action caused by N1-methyl pseudouridine in the synthetic mRNA—also referred to as modRNA.
- Widespread distribution of mRNA and DNA codes via the LNP and viral vector carrier matrices, respectively.
- Human cells produce a foreign protein that can cause autoimmunity.
Now that vaccines utilizing mRNA technology have been available and widely distributed for several years, data show these vaccines produce foreign antigens in human tissues and increase the risk of autoimmune, neurological, cardiovascular, inflammatory disorders, and cancers, especially when the vaccine ingredients do not remain localized at the injection site. An antigen is any substance that stimulates an immune response. If the immune system encounters an antigen that is not found on the body’s own cells, it will launch an attack against that antigen.
Pharmacokinetic and pharmacodynamic data show the design of the mRNA and adenovectorDNA COVID-19 vaccines allow uncontrolled biodistribution, durability, and persistent bioavailability of the spike protein inside the body after vaccination. Pharmacokinetics is the study of how the body interacts with administered substances for the entire duration of exposure. Pharmacodynamics assesses the drug’s effect on the body more closely.
This may explain the unprecedented number of adverse events that appear to be associated with the spike protein produced by the gene-based technologies employed by Pfizer, Moderna, AstraZeneca, and Johnson & Johnson, as well as the viral vector DNA technology used by other countries, researchers said.
mRNA Vaccines Are Gene Therapy and May Cause Harm
Gene-based COVID-19 vaccines are therapeutic products that actually fit within the FDA’s definition of gene therapy because they cause the cells of the vaccinated person to produce antigens for transmembrane expression that invokes an immune response. By design, these novel vaccine platforms risk tissue damage secondary to autoimmune responses raised against cells expressing foreign spike antigens, researchers said.
The FDA was aware of the pathogenicity of spike proteins before releasing COVID-19 vaccines to the public. In an October 2022 meeting with its vaccine advisors, the FDA presented a highly accurate list of potential adverse events associated with COVID-19 vaccines, including neurological, cardiovascular, and autoimmune “possible adverse events.”
React19, an organization that provides financial, emotional, and physical support to those experiencing long-term injuries from COVID-19 vaccines, provided a list of over 3,400 published papers and case reports of injuries affecting more than 20 organ systems. More than 432 peer-reviewed papers relate to papers and case reports of myocarditis, cardiomyopathy, myocardial infarction, hypertension, aortic dissection, postural orthostatic tachycardia syndrome (POTS), tachycardia, and conduction disturbance—a problem with the electrical system that controls the heart’s rate and rhythm.
The most common group of adverse events reported following COVID-19 vaccination to both pharmacovigilance databases and Pfizer involve neurological disorders. According to the paper, neurological symptoms and cognitive decline with accelerated neurodegenerative disease are features of acute COVID-19 vaccine injuries and, to some extent, long COVID syndrome. Research suggests (pdf) LNPs transporting the mRNA to make spike proteins can cross the blood-brain barrier and cause neurotoxic effects.
Lipid Nanoparticles Are Toxic and Pro-Inflammatory
It’s not just the spike protein that can cause disease. LNPs that serve as the delivery method are also toxic and pro-inflammatory.
Research from 2018 showed even small amounts of nanoparticles taken up by the lungs can lead to cytotoxic effects. Ingested nanoparticles have been shown to affect lymph nodes, the liver, and the spleen, while when injected as a drug carrier, they can pass any barrier and translocate to the brain, ovaries, and testes, mainly after phagocytosis by macrophages, which help distribute them across the body. The effects on the reproductive system suggest lipid nanoparticles can be cytotoxic and damage DNA.
According to the authors, two components in the mRNA lipid nanoparticle complexes, ALC-0315 and ALC-0159, are concerning, as they have never been used in a medicinal product and are not registered in either the European Pharmacopoeia or in the European C&L Inventory database. A question posed to the European Parliament in December 2021 pointed out that the manufacturer of the nanoparticles specifies the nanoparticles are for research only and not for human use. The European Commission responded that the excipient in Pfizer’s Comirnaty vaccine “has been demonstrated to be appropriate … in compliance with the relevant EMA scientific guidelines and standards.”
Still, this could explain the root cause of numerous post-vaccination adverse events, researchers said.
“Even if it were non-toxic in its own right, by virtue of its foreignness, spike protein could still produce pathophysiological damage through autoimmune responses. A straightforward consequence of a foreign protein,” the researchers stated. “The lipid-nanoparticle matrix permits widespread biodistribution of mRNA gene codes to cells in most or all organs. The subsequent expression of the spike protein on cell surfaces, and as a soluble protein within the organs and bloodstream, induces T-cell destruction of cells and tissues and B-cell antibodies. The latter may also cause immune complex deposition, further damaging tissues … ”
In a 2021 preprint, researchers noted the pharmacokinetics of mRNA COVID-19 vaccines generated far greater numbers of spike proteins than the SARS-CoV-2 virus and “more systemically in most people not prone to overwhelming COVID-19 viral infection.”
In addition to their potential toxicity, LNPs in COVID-19 vaccines have been found to “induce significant inflammatory cytokine secretion and macrophage inflammatory proteins with cell death.” Research has shown this pro-inflammatory effect can increase vaccine adjuvant immunogenicity of COVID-19 mRNA vaccines and contribute to adverse events. Researchers also stated that widespread biodistribution of the LNPs was not considered, nor was the potential for wide-ranging serious adverse events across multiple organs and systems.
In the presence of polyethylene glycol, a common vaccine ingredient, mRNA in lipid nanoparticles becomes more resistant to degradation and evades the immune system with the nanoparticles helping with biodistribution and bioaccumulation. According to the paper, bioaccumulation can “lead to blockage of small blood and lymphatic vessels,” and biodistribution can cause cell death and inflammation in all organs.
Lipid Nanoparticles Widely Distribute mRNA Throughout the Body
According to the paper, LNPs in COVID-19 vaccines containing potentially inflammatory synthetic mRNA do not remain at the injection site after vaccination but are widely distributed throughout the body and can cross protective membranes.
A European Medicines Agency report found, “mRNA could be detected in the brain following intramuscular administration at about 2 percent of the level found in plasma.” Another paper described how lipid nanoparticles can easily cross the blood-brain barrier.
Byram Bridle, Canadian virologist and vaccinologist, obtained a Pfizer biodistribution study in rodents from Japan that showed lipid nanoparticles could pass easily through biological tissues and membranes and travel to all organs. By 48 hours after vaccination, 75 percent of lipid nanoparticles had left the injection site with the highest concentrations in the spleen and liver. Levels were also detected in the ovaries, adrenal glands, brain, eyes, heart, testes, uterus, pituitary gland, spinal cord, thymus, and bone marrow. Further studies have since confirmed the results of Pfizer’s rat distribution study, researchers said.
Although health regulatory authorities assured the public that persistent mRNA spike protein production would be brief and localized at the injection site, this is not the case. Because natural messenger RNA is highly unstable, synthetic mRNA that codes for the spike protein in Moderna and Pfizer’s COVID-19 vaccines was stabilized by replacing uridine with N1-methylpseudourine. This essentially “modified” the RNA to stabilize synthetic mRNA over a period of time. This may be why some experts say mRNA stands for “modified RNA” instead of “messenger RNA.”
Numerous studies have found lipid nanoparticles containing mRNA still circulating in the blood after vaccination, with one study (pdf) showing the presence of mRNA and free spike proteins—for the entire 60-day duration of the study—in the cytoplasm and nuclei of germinal cells in armpit lymph nodes on the same side of the body as the injection site. Other research detected spike proteins in circulating exosomes that carry nucleic acids, proteins, lipids, and metabolites throughout the body for at least four months after vaccination with Pfizer’s COVID-19 vaccine.
Although some research suggests detection of the spike protein is restricted after the second dose due to anti-spike antibodies, since modified RNA molecules are highly stable, researchers say the spike protein production will persist until the immune system attacks or kills the cell.
“No studies have determined the stability of the vaccine-induced spike protein, but free spike protein has been found circulating up to 19 days post-vaccination in the plasma of young individuals with post-vaccine myocarditis,” the authors said.
Booster Shots Increase Potential for Adverse Events From Spike Protein
Both mRNA and adenovector DNA vaccines cause human cells to create a slightly modified version of the original Wuhan strain spike protein. In contrast, the bivalent booster doses add genetic code for the omicron variant spike protein.
According to the researchers, if an individual experiences wide biodistribution of this genetic code, the body could produce many more spike proteins than what would occur with the natural virus. This is more likely the case with young and healthy people who typically rid themselves of the virus through the upper respiratory mucosa.
“Therefore, in the young and healthy, the encoding-based COVID-19 vaccines will transfect a far more diverse set of tissues than infection by the virus itself,” they concluded.
Further research has noted that “potential toxicological issues were not taken into consideration in the studies that led to the marketing authorization, precisely because … these products were treated as conventional vaccines when, in fact, they are gene insertions acting as prodrugs.”
Data Suggest Risks of COVID-19 Vaccines Far Outweigh Low Efficacy
Although it’s claimed COVID-19 vaccines have saved millions of lives, this belief is founded upon an early 2020 infection fatality rate in China, modeling estimates produced by vaccine manufacturers, and a false assumption vaccines would protect against infection and transmission. Even Pfizer admitted its phase 3 clinical trial didn’t assess viral transmission. Yet health authorities, regulatory agencies, medical publications, and the media continue to claim vaccines are effective.
To accurately assess the efficacy of gene-based COVID-19 vaccines, the researchers said there would need to be long-term studies between the vaccinated and unvaccinated individuals, which cannot occur because Pfizer, Moderna, AstraZeneca, and Janssen vaccinated their control group who were initially administered placebos.
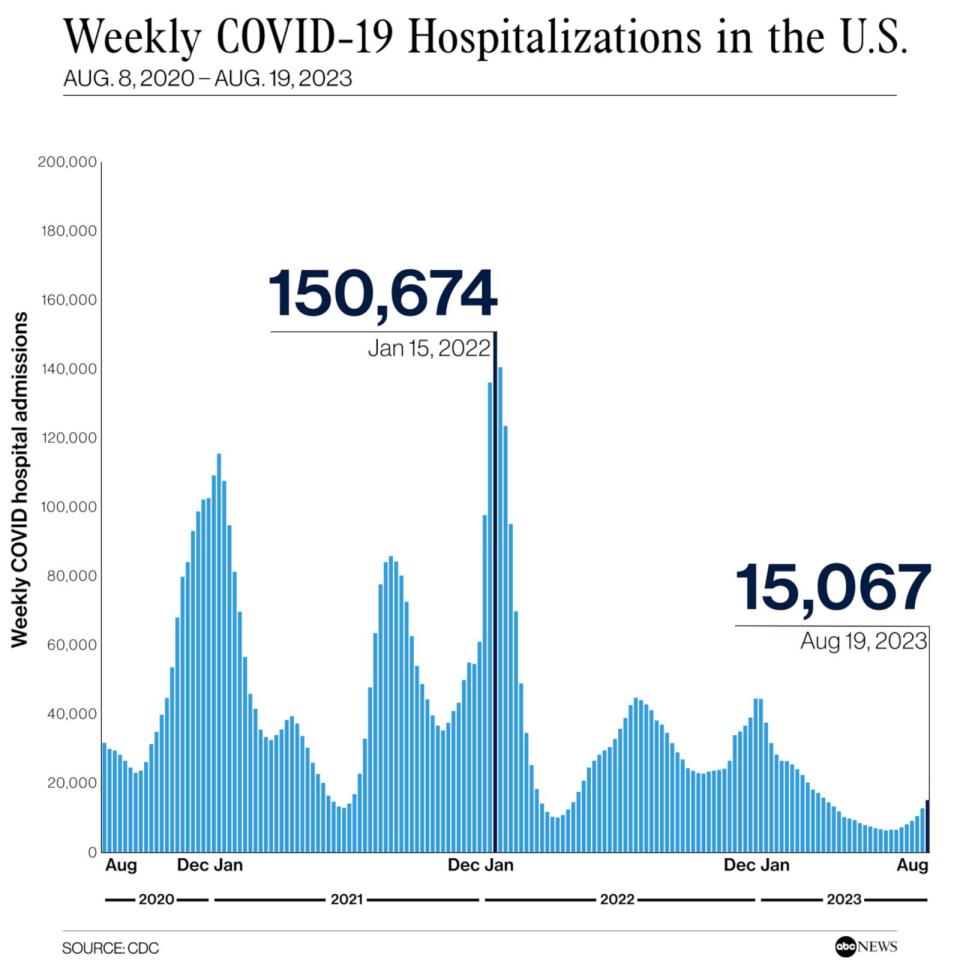
There is currently only one worldwide control group, and data show that the unvaccinated cohort faired better than expected. Australian data from December 2022 show the unvaccinated barely exist in hospitalization data, whereas the most vaccinated are overrepresented. The data “do not suggest significant efficacy against hospitalization, ICU admission and death, at least after the emergence of the Omicron strain,” researchers concluded. Instead, the data indicate a relationship between more vaccine doses with severe COVID-19, and increased all-cause mortality that coincides with the rollout of vaccines, they said.













 Again, talking about the GV only. That hasn't manifested yet. There will be no doubt it's here when/if it arrives.
Again, talking about the GV only. That hasn't manifested yet. There will be no doubt it's here when/if it arrives.