
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
CORONA Main Coronavirus thread
- Thread starter Heliobas Disciple
- Start date
-
- Tags
- coronavirus

Heliobas Disciple
TB Fanatic

State Moves to Revoke Dr. Ryan Cole's License for Prescribing Ivermectin, COVID-19 Vaccine Comments
Washington state's medical commission has brought charges against Dr. Ryan Cole, a pathologist, over alleged false and misleading ...
 www.theepochtimes.com
www.theepochtimes.com
State Moves to Revoke Dr. Ryan Cole’s License for Prescribing Ivermectin, COVID-19 Vaccine Comments
By Zachary Stieber
January 21, 2023
Washington state’s medical commission has brought charges against Dr. Ryan Cole, a pathologist, over alleged false and misleading statements about COVID-19 vaccines and his prescribing of ivermectin to treat COVID-19.
The Washington Medical Commission announced the allegations on Jan. 18 against Cole after receiving complaints about Cole’s conduct.
Cole lives in Idaho but is licensed in Washington state.
The state alleges that Cole made “numerous false and misleading statements” during the COVID-19 pandemic about the pandemic, vaccines, ivermectin, and the effectiveness of protective masks.
The statements “were harmful and dangerous to individual patients, generated mistrust in the medical profession and in public health, and had a wide-spread negative impact on the health and well-being of our communities,” the commission said.
Cole also provided “negligent care” to four patients by prescribing ivermectin, which is “not indicated for a COVID-19 infection,” according to a statement of charges.
Cole did not respond to requests for comment.
Cole has until Jan. 30 to file a response to the charges, according to the commission. Cole will have a chance to defend himself against the allegations at a hearing.
The commission is a licensing authority. The charges can lead to the suspension of Cole’s license.
Statements on Vaccines, COVID-19
Washington state authorities say that Cole’s alleged false and misleading statements include claims that the COVID-19 vaccines have caused more deaths than COVID-19 and that the vaccines can lead to cancer and infertility.
Cole, the founder of Cole Diagnostics, has said in interviews with The Epoch Times and other outlets, as well as during public presentations, that he observed a spike in unusual cancers and other problems after the messenger RNA COVID-19 vaccines were introduced in late 2020. He asserted that heart inflammation is known to be caused by the shots, as well as other issues not proven to be linked, that stem from introducing the spike protein into the human body.
“The naysayers [say], Oh, the spike isn’t … [a] toxin,” Cole said during one interview with The Epoch Times “American Thought Leaders.”
“I’m like, ‘The cells don’t lie.’ And that’s my defense. The cells don’t lie. These people aren’t looking at the cells under the microscope. They’re not seeing the damage I am. Many of my colleagues are. The cells don’t lie. If it’s inconvenient to what you want to tell yourself, that’s fine. But the cells don’t lie. The clots don’t lie. The damaged organs don’t lie,” he added.
Cole has also said COVID-19 vaccines are “fake” and referred to vaccination with them as “needle rape,” the commission noted.
Some of the statements the commission referenced as “false and misleading: were actually accurate. Among them: Cole’s noting that natural immunity, or post-infection immunity, against COVID-19 is superior to the protection bestowed by vaccines. That’s been shown or indicated in many studies, including a study from the U.S. Centers for Disease Control and Prevention and a paper from Israel.
According to the commission, Cole said it in a written statement in 2022 that he has not advised people not to get a COVID-19 vaccine.
Treatment
Cole was part of MyFreeDoctor.com, according to archived versions of the website. The website is a telehealth service that enables doctors to correspond with and see patients remotely using the internet. The charges say Cole treated patients for COVID-19 over a “virtual telemedicine platform.”
Cole prescribed medicine to four patients after reviewing their records and speaking with them over an instant chat function on the platform, according to authorities. He prescribed ivermectin multiple times. Ivermectin is approved by the U.S. Food and Drug Administration to treat conditions caused by parasitic worms but the administration says it should not be used against COVID-19, though some of the studies it cites actually support its use.
Cole’s treatment of the patients, including not documenting “appropriate medical decision-making” for them, constituted unprofessional conduct, according to the commission.
State law defines unprofessional conduct as “the commission of any act involving moral turpitude, dishonesty, or corruption relating to the practice of the person’s profession, whether the act constitutes a crime or not.”
A practitioner can also violate the law if they commit “Incompetence, negligence, or malpractice which results in injury to a patient or which creates an unreasonable risk that a patient may be harmed,” though the code stipulates that “the use of a nontraditional treatment by itself shall not constitute unprofessional conduct, provided that it does not result in injury to a patient or create an unreasonable risk that a patient may be harmed.”
Cole has told The Epoch Times in previous interviews that he has seen 500,000 patients in his 26-year career and has never had a patient complain about him or file a lawsuit.
“Now all of a sudden I find myself in the crosshairs for sharing science. Because of that, I lost one of my major insurance contracts for my ‘unprofessional behavior’ of talking about ivermectin and helping save a handful of lives with that for free. I never charged a patient,” he said.
“Then they say, ‘Well gosh, you’re a pathologist.’ I did years of emergency medicine, years of family medicine, years of dermatology,” Cole said. “I never quit being a doctor. I’m the doctor to the doctor, as a laboratory physician now.”
Heliobas Disciple
TB Fanatic

Chinese People Say the CCP Forces Doctors and Community Staff to Not List COVID as Cause of Death
Western media have recently reported that doctors in China are discouraged from citing COVID-19 as the cause of ...
www.theepochtimes.com
Chinese People Say the CCP Forces Doctors and Community Staff to Not List COVID as Cause of Death
By Ellen Wan and Kane Zhang
January 21, 2023
Western media have recently reported that doctors in China are discouraged from citing COVID-19 as the cause of death in an attempt to downplay the severity and extent of the ongoing explosive COVID infection wave.
A number of Chinese citizens spoke to the Chinese language edition of The Epoch Times and shared their personal stories, saying that the regime orders doctors and community workers to falsify the cause of death on death certificates.
On Jan. 17, Zhang Miao (pseudonym), a community worker in Changchun City, Jilin Province, told the Chinese language edition of The Epoch Times that she had just prepared a death certificate for a senior resident who passed away from COVID-19.
“The local police chief came to our community office on Jan. 14 and asked me to issue a death certificate for his father-in-law,” Zhang said. “I asked him if the death was caused by COVID-19, and he said yes.”
“Then I explained to him that we received an instruction from above, saying the cause of death can’t be listed as COVID-19,” Zhang said.
She further explained that if the patient died at home, his family first needed to go to the community office to get a death certificate, then present it to a public hospital in exchange for a hospital-issued death certificate. The local police will only acknowledge a hospital-issued death certificate before they will remove the residential registration of the deceased. These steps are necessary before the body of the deceased can be sent to a crematorium.
“However, the thing is, the community cannot state that COVID-19 is the cause of death on the certificate; otherwise the hospital will not issue the formal death certificate. Even if you go back to the community asking for a re-issuance, the hospital won’t give you this chance. You only have one chance to get it ‘right.’ The death certificate I gave to his father-in-law said the elder died of a cerebral infarction,” Zhang said.
Hospitals Ordered to Lie on Death Certificate
Liu Chen (pseudonym), a doctor at a hospital in Dalian, Liaoning Province, told the Chinese language edition of The Epoch Times on Jan. 17 that the government has set a rule that “patients who die due to COVID-19 aggravation of underlying disease(s) cannot be counted as COVID-19 deaths.”
“That is the standard we all have to follow. So from the top to the bottom, no one knows the exact mortality rate of COVID-19. Even for the top authorities, there is no way they can have the exact figures,” he said.
Cheng Ying (pseudonym), a doctor at the Yantai Mountain Hospital, made a similar statement when he spoke to the Chinese language Epoch Times on Jan. 17. “Even our hospital does not have the exact number of people who died from COVID-19 in our facility, as the government does not allow us to register them as COVID-19 deaths.”
Wang Ling (pseudonym), a doctor at another hospital in Yantai, Shandong Province, revealed on Jan. 15 that the number of deaths due to COVID-19 was so large that the Shandong medical system issued an emergency notice forbidding doctors to cite COVID-19 as cause of death.
“As long as there are other underlying diseases, those diseases can be listed as the cause of death. Basically, whatever cause can be cited, other than COVID-19. Moreover, the doctors must get approval from the hospital authorities on the specific details before filling out a death certificate; they are not allowed to do it on their own.”
Gu Cheng (pseudonym), a resident of Yantai, Shandong Province, told The Epoch Times on Jan. 17 that a friend just lost his father last month.
“His father was hospitalized in Yantai Hospital for the treatment of heart disease in early December last year and was originally scheduled to be discharged in a week. But after the sudden removal of lockdown and restrictions, his father tested COVID positive while still in the hospital, and passed away a few days later. Doctors refused to list COVID-19 as the cause of death, and cited heart disease instead. It’s the same in other hospitals. The doctors are forbidden to list COVID-19 as the cause of death,” Gu said.
Chinese Question the Official Death Toll
China’s National Health and Wellness Commission reported on Jan. 14 that 60,000 COVID deaths occurred between Dec. 8, 2022 and Jan. 12, 2023.
However, the visible explosive wave of infections and the overcrowded funeral homes are telling a different story.
Qu Li (pseudonym), a Beijing resident, told The Epoch Times on Jan. 18 that she saw a very long line of vehicles outside a crematorium.
“My mother passed away after COVID-19 infection. Our wait time for her cremation was a whole week at the Pingfang Crematorium in Chaoyang District, and this was the result of our cutting in line using a personal connection. On the day of the cremation, there were huge crowds of people outside queuing up to get their numbers, and you can’t see the end [of the queue] at a glance. When we left the crematorium, the car drove for a long way and you could still see the people in line,” Qu said.
Qu heard that the same is true at other crematoria in Beijing.
“My brother said that 21 people he knew of recently passed away, including three relatives of my family. None of the death certificates said that these were COVID-19 deaths. The number of recent COVID deaths can be said to be ‘shocking.’ The authorities said 60,000 people died, but I don’t believe it,” she added.
Yang Hai (pseudonym), a resident of Hailun City, Heilongjiang Province, told The Epoch Times on Jan. 17 that his uncle just passed away due to COVID-19 infection.
“Inside the funeral home, there were layers of coffins on the shelves. The employees were transporting some corpses to another crematorium more than 50 kilometers (31 miles) away to be cremated. There are two crematoriums in Hailun City. Both are too busy to handle all the cremation requests because there are so many corpses. The deceased are mostly elderly people, there are also some in their 50s.”
Zhang, the community worker, said she issued five death certificates that day, including the one for the police chief’s father-in-law. On most certificates, she cited heart failure as the cause of death.
“There are three police stations in our area. The police chief told me that he removed 23 deceased from the registration system in one day when he was on duty. If that’s the average number for one police station, wouldn’t there be an average of 70 deaths a day in three police stations?” Zhang said.
China’s State Council held a press conference on Jan. 17 on the topic of the country’s economy in 2022. When asked about death toll and population data in December, Kang Yi, director of the National Bureau of Statistics, said that in non-census years, the time point of population sampling survey is Nov. 1 every year, so there is no data on the number of deaths in December 2022 yet.
He also claimed that the data about the pandemic, including the number of infections and other aspects, is released to the world and shared with the relevant organizations as soon as it is available.
Chinese netizens expressed anger at his remarks. They left comments such as, “With such a strict household registration system that requires timely submission of a death certificate, how come you don’t know the number of deaths?” and “Now that household information is all online, you should be able to find out the total number of death certificates within your system. How come you claim you don’t have December’s data?”
“The authorities’ claim that they put people first, putting life first is a sheer lie. They falsified COVID-related data when people were under lockdown, and they continued to falsify data when restrictions were removed. They have been lying all along,” Zhang said.
Heliobas Disciple
TB Fanatic

China says COVID outbreak has infected 80% of population
The possibility of a big COVID-19 rebound in China over the next two or three months is remote as 80% of people have been infected, a prominent government scientist said on Saturday. The mass movement of people during the ongoing Lunar New Year holiday period may spread the pandemic, boosting...
China says COVID outbreak has infected 80% of population
by Beijing newsroom
Sat, January 21, 2023, 4:59 AM EST·1 min read
BEIJING (Reuters) - The possibility of a big COVID-19 rebound in China over the next two or three months is remote as 80% of people have been infected, a prominent government scientist said on Saturday.
The mass movement of people during the ongoing Lunar New Year holiday period may spread the pandemic, boosting infections in some areas, but a second COVID wave is unlikely in the near term, Wu Zunyou, chief epidemiologist at the China Center for Disease Control and Prevention, said on the Weibo social media platform.
Hundreds of millions of Chinese are travelling across the country for holiday reunions that had been suspended under recently eased COVID curbs, raising fears of fresh outbreaks in rural areas less equipped to manage large outbreaks.
China has passed the peak of COVID patients in fever clinics, emergency rooms and with critical conditions, a National Health Commission official said on Thursday.
Nearly 60,000 people with COVID had died in hospital as of Jan. 12, roughly a month after China abruptly dismantled its zero-COVID policy, according to government data.
But some experts said that figure probably vastly undercounts the full impact, as it excludes those who die at home, and because many doctors have said they are discouraged from citing COVID as a cause of death.
Heliobas Disciple
TB Fanatic

China rings in Lunar New Year with most COVID rules lifted
BEIJING (AP) — People across China rang in the Lunar New Year on Sunday with large family gatherings and crowds visiting temples after the government lifted its strict “zero-COVID” policy, marking the biggest festive celebration since the pandemic began three years ago.
 apnews.com
apnews.com
China rings in Lunar New Year with most COVID rules lifted
January 22, 2023
BEIJING (AP) — People across China rang in the Lunar New Year on Sunday with large family gatherings and crowds visiting temples after the government lifted its strict “zero-COVID” policy, marking the biggest festive celebration since the pandemic began three years ago.
The Lunar New Year is the most important annual holiday in China. Each year is named after one of the 12 signs of the Chinese zodiac in a repeating cycle, with this year being the Year of the Rabbit. For the past three years, celebrations were muted in the shadow of the pandemic.
With the easing of most COVID-19 restrictions, many people could finally make their first trip back to their hometowns to reunite with their families without worrying about the hassles of quarantine, potential lockdowns and suspension of travel. Larger public celebrations also returned for what is known as the Spring Festival in China, with the capital hosting thousands of cultural events — on a larger scale than a year ago.
In Beijing, many worshippers offered morning prayers at the Lama Temple but the crowds appeared to be smaller compared to pre-pandemic days. The Tibetan Buddhist site allows up to 60,000 visitors a day, citing safety reasons, and requires an advance reservation.
Throngs of residents and tourists swarmed pedestrian streets in the Qianmen area near Tiananmen Square. Many of them enjoyed snacks from barbecue and New Year rice cake stands, and some children wore traditional Chinese rabbit hats. Others held blown sugar or marshmallows shaped like rabbits.
Beijing resident Si Jia said she felt that life in Beijing was back to normal in general, pointing to the return of tourists. She said she brought her 7-year-old son to Qianmen to experience the festive vibe in Beijing and learn about traditional Chinese culture.
“He has never experienced what a traditional new year is like because he was too young three years ago and he had no memory of that,” she said. “But this year I can show him around here.”
At Taoranting Park, there was no sign of the usual bustling New Year food stalls despite its walkways being decorated with traditional Chinese lanterns. A popular temple fair at Badachu Park that was suspended for three years will be back this week, but similar events at Ditan Park and Longtan Lake Park have yet to return.
The mass movement of people may cause the virus to spread in certain areas, said Wu Zunyou, the chief epidemiologist at China’s Center for Disease Control. But a large-scale COVID-19 surge will be unlikely in the next two or three months because about 80% of the country’s 1.4 billion people have been infected during the recent wave, he wrote on the social media platform Weibo on Saturday.
In Hong Kong, revelers flocked to the city’s largest Taoist temple, Wong Tai Sin Temple, to burn the first incense sticks of the year. The site’s popular ritual was suspended the last two years due to the pandemic.
Traditionally, big crowds gather before 11 p.m. on Lunar New Year’s Eve, with everyone trying to be the first, or among the first, to put their incense sticks into the stands in front of the temple’s main hall. Worshippers believe those who are among the first to place their incense sticks will stand the best chance of having their prayers answered.
Local resident Freddie Ho, who visited the temple on Saturday night, was happy that he could join the event in person.
“I hope to place the first incense stick and pray that the New Year brings world peace, that Hong Kong’s economy will prosper, and that the pandemic will go away from us and we can all live a normal life,” Ho said. “I believe this is what everyone wishes.”
Meanwhile, the crowds praying for good fortune at the historic Longshan Temple in Taipei, the capital of Taiwan, were smaller than a year ago even as the pandemic has eased. That is partly because many people there had ventured to other parts of Taiwan or overseas on long-awaited trips.
As communities across Asia welcomed the Year of the Rabbit, the Vietnamese were celebrating the Year of the Cat instead. There’s no official answer to explain the difference. But one theory suggests cats are popular because they often help Vietnamese rice farmers to chase away rats.
___
Associated Press researcher Henry Hou, video journalist Emily Wang and video producer Olivia Zhang in Beijing and video journalists Alice Fung in Hong Kong and Taijing Wu in Taipei, Taiwan contributed to this report.
Tristan
Has No Life - Lives on TB
(fair use applies)State Moves to Revoke Dr. Ryan Cole's License for Prescribing Ivermectin, COVID-19 Vaccine Comments
Washington state's medical commission has brought charges against Dr. Ryan Cole, a pathologist, over alleged false and misleading ...
State Moves to Revoke Dr. Ryan Cole’s License for Prescribing Ivermectin, COVID-19 Vaccine Comments
By Zachary Stieber
January 21, 2023
Washington state’s medical commission has brought charges against Dr. Ryan Cole, a pathologist, over alleged false and misleading statements about COVID-19 vaccines and his prescribing of ivermectin to treat COVID-19.
The Washington Medical Commission announced the allegations on Jan. 18 against Cole after receiving complaints about Cole’s conduct.
Cole lives in Idaho but is licensed in Washington state.
The state alleges that Cole made “numerous false and misleading statements” during the COVID-19 pandemic about the pandemic, vaccines, ivermectin, and the effectiveness of protective masks.
The statements “were harmful and dangerous to individual patients, generated mistrust in the medical profession and in public health, and had a wide-spread negative impact on the health and well-being of our communities,” the commission said.
Cole also provided “negligent care” to four patients by prescribing ivermectin, which is “not indicated for a COVID-19 infection,” according to a statement of charges.
Cole did not respond to requests for comment.
Cole has until Jan. 30 to file a response to the charges, according to the commission. Cole will have a chance to defend himself against the allegations at a hearing.
The commission is a licensing authority. The charges can lead to the suspension of Cole’s license.
Statements on Vaccines, COVID-19
Washington state authorities say that Cole’s alleged false and misleading statements include claims that the COVID-19 vaccines have caused more deaths than COVID-19 and that the vaccines can lead to cancer and infertility.
Cole, the founder of Cole Diagnostics, has said in interviews with The Epoch Times and other outlets, as well as during public presentations, that he observed a spike in unusual cancers and other problems after the messenger RNA COVID-19 vaccines were introduced in late 2020. He asserted that heart inflammation is known to be caused by the shots, as well as other issues not proven to be linked, that stem from introducing the spike protein into the human body.
“The naysayers [say], Oh, the spike isn’t … [a] toxin,” Cole said during one interview with The Epoch Times “American Thought Leaders.”
“I’m like, ‘The cells don’t lie.’ And that’s my defense. The cells don’t lie. These people aren’t looking at the cells under the microscope. They’re not seeing the damage I am. Many of my colleagues are. The cells don’t lie. If it’s inconvenient to what you want to tell yourself, that’s fine. But the cells don’t lie. The clots don’t lie. The damaged organs don’t lie,” he added.
Cole has also said COVID-19 vaccines are “fake” and referred to vaccination with them as “needle rape,” the commission noted.
Some of the statements the commission referenced as “false and misleading: were actually accurate. Among them: Cole’s noting that natural immunity, or post-infection immunity, against COVID-19 is superior to the protection bestowed by vaccines. That’s been shown or indicated in many studies, including a study from the U.S. Centers for Disease Control and Prevention and a paper from Israel.
According to the commission, Cole said it in a written statement in 2022 that he has not advised people not to get a COVID-19 vaccine.
Treatment
Cole was part of MyFreeDoctor.com, according to archived versions of the website. The website is a telehealth service that enables doctors to correspond with and see patients remotely using the internet. The charges say Cole treated patients for COVID-19 over a “virtual telemedicine platform.”
Cole prescribed medicine to four patients after reviewing their records and speaking with them over an instant chat function on the platform, according to authorities. He prescribed ivermectin multiple times. Ivermectin is approved by the U.S. Food and Drug Administration to treat conditions caused by parasitic worms but the administration says it should not be used against COVID-19, though some of the studies it cites actually support its use.
Cole’s treatment of the patients, including not documenting “appropriate medical decision-making” for them, constituted unprofessional conduct, according to the commission.
State law defines unprofessional conduct as “the commission of any act involving moral turpitude, dishonesty, or corruption relating to the practice of the person’s profession, whether the act constitutes a crime or not.”
A practitioner can also violate the law if they commit “Incompetence, negligence, or malpractice which results in injury to a patient or which creates an unreasonable risk that a patient may be harmed,” though the code stipulates that “the use of a nontraditional treatment by itself shall not constitute unprofessional conduct, provided that it does not result in injury to a patient or create an unreasonable risk that a patient may be harmed.”
Cole has told The Epoch Times in previous interviews that he has seen 500,000 patients in his 26-year career and has never had a patient complain about him or file a lawsuit.
“Now all of a sudden I find myself in the crosshairs for sharing science. Because of that, I lost one of my major insurance contracts for my ‘unprofessional behavior’ of talking about ivermectin and helping save a handful of lives with that for free. I never charged a patient,” he said.
“Then they say, ‘Well gosh, you’re a pathologist.’ I did years of emergency medicine, years of family medicine, years of dermatology,” Cole said. “I never quit being a doctor. I’m the doctor to the doctor, as a laboratory physician now.”
This is what tyranny looks like.
Tristan
Has No Life - Lives on TB
(fair use applies)Chinese People Say the CCP Forces Doctors and Community Staff to Not List COVID as Cause of Death
Western media have recently reported that doctors in China are discouraged from citing COVID-19 as the cause of ...
Chinese People Say the CCP Forces Doctors and Community Staff to Not List COVID as Cause of Death
By Ellen Wan and Kane Zhang
January 21, 2023
Western media have recently reported that doctors in China are discouraged from citing COVID-19 as the cause of death in an attempt to downplay the severity and extent of the ongoing explosive COVID infection wave.
A number of Chinese citizens spoke to the Chinese language edition of The Epoch Times and shared their personal stories, saying that the regime orders doctors and community workers to falsify the cause of death on death certificates.
On Jan. 17, Zhang Miao (pseudonym), a community worker in Changchun City, Jilin Province, told the Chinese language edition of The Epoch Times that she had just prepared a death certificate for a senior resident who passed away from COVID-19.
“The local police chief came to our community office on Jan. 14 and asked me to issue a death certificate for his father-in-law,” Zhang said. “I asked him if the death was caused by COVID-19, and he said yes.”
“Then I explained to him that we received an instruction from above, saying the cause of death can’t be listed as COVID-19,” Zhang said.
She further explained that if the patient died at home, his family first needed to go to the community office to get a death certificate, then present it to a public hospital in exchange for a hospital-issued death certificate. The local police will only acknowledge a hospital-issued death certificate before they will remove the residential registration of the deceased. These steps are necessary before the body of the deceased can be sent to a crematorium.
“However, the thing is, the community cannot state that COVID-19 is the cause of death on the certificate; otherwise the hospital will not issue the formal death certificate. Even if you go back to the community asking for a re-issuance, the hospital won’t give you this chance. You only have one chance to get it ‘right.’ The death certificate I gave to his father-in-law said the elder died of a cerebral infarction,” Zhang said.
Hospitals Ordered to Lie on Death Certificate
Liu Chen (pseudonym), a doctor at a hospital in Dalian, Liaoning Province, told the Chinese language edition of The Epoch Times on Jan. 17 that the government has set a rule that “patients who die due to COVID-19 aggravation of underlying disease(s) cannot be counted as COVID-19 deaths.”
“That is the standard we all have to follow. So from the top to the bottom, no one knows the exact mortality rate of COVID-19. Even for the top authorities, there is no way they can have the exact figures,” he said.
Cheng Ying (pseudonym), a doctor at the Yantai Mountain Hospital, made a similar statement when he spoke to the Chinese language Epoch Times on Jan. 17. “Even our hospital does not have the exact number of people who died from COVID-19 in our facility, as the government does not allow us to register them as COVID-19 deaths.”
Wang Ling (pseudonym), a doctor at another hospital in Yantai, Shandong Province, revealed on Jan. 15 that the number of deaths due to COVID-19 was so large that the Shandong medical system issued an emergency notice forbidding doctors to cite COVID-19 as cause of death.
“As long as there are other underlying diseases, those diseases can be listed as the cause of death. Basically, whatever cause can be cited, other than COVID-19. Moreover, the doctors must get approval from the hospital authorities on the specific details before filling out a death certificate; they are not allowed to do it on their own.”
Gu Cheng (pseudonym), a resident of Yantai, Shandong Province, told The Epoch Times on Jan. 17 that a friend just lost his father last month.
“His father was hospitalized in Yantai Hospital for the treatment of heart disease in early December last year and was originally scheduled to be discharged in a week. But after the sudden removal of lockdown and restrictions, his father tested COVID positive while still in the hospital, and passed away a few days later. Doctors refused to list COVID-19 as the cause of death, and cited heart disease instead. It’s the same in other hospitals. The doctors are forbidden to list COVID-19 as the cause of death,” Gu said.
Chinese Question the Official Death Toll
China’s National Health and Wellness Commission reported on Jan. 14 that 60,000 COVID deaths occurred between Dec. 8, 2022 and Jan. 12, 2023.
However, the visible explosive wave of infections and the overcrowded funeral homes are telling a different story.
Qu Li (pseudonym), a Beijing resident, told The Epoch Times on Jan. 18 that she saw a very long line of vehicles outside a crematorium.
“My mother passed away after COVID-19 infection. Our wait time for her cremation was a whole week at the Pingfang Crematorium in Chaoyang District, and this was the result of our cutting in line using a personal connection. On the day of the cremation, there were huge crowds of people outside queuing up to get their numbers, and you can’t see the end [of the queue] at a glance. When we left the crematorium, the car drove for a long way and you could still see the people in line,” Qu said.
Qu heard that the same is true at other crematoria in Beijing.
“My brother said that 21 people he knew of recently passed away, including three relatives of my family. None of the death certificates said that these were COVID-19 deaths. The number of recent COVID deaths can be said to be ‘shocking.’ The authorities said 60,000 people died, but I don’t believe it,” she added.
Yang Hai (pseudonym), a resident of Hailun City, Heilongjiang Province, told The Epoch Times on Jan. 17 that his uncle just passed away due to COVID-19 infection.
“Inside the funeral home, there were layers of coffins on the shelves. The employees were transporting some corpses to another crematorium more than 50 kilometers (31 miles) away to be cremated. There are two crematoriums in Hailun City. Both are too busy to handle all the cremation requests because there are so many corpses. The deceased are mostly elderly people, there are also some in their 50s.”
Zhang, the community worker, said she issued five death certificates that day, including the one for the police chief’s father-in-law. On most certificates, she cited heart failure as the cause of death.
“There are three police stations in our area. The police chief told me that he removed 23 deceased from the registration system in one day when he was on duty. If that’s the average number for one police station, wouldn’t there be an average of 70 deaths a day in three police stations?” Zhang said.
China’s State Council held a press conference on Jan. 17 on the topic of the country’s economy in 2022. When asked about death toll and population data in December, Kang Yi, director of the National Bureau of Statistics, said that in non-census years, the time point of population sampling survey is Nov. 1 every year, so there is no data on the number of deaths in December 2022 yet.
He also claimed that the data about the pandemic, including the number of infections and other aspects, is released to the world and shared with the relevant organizations as soon as it is available.
Chinese netizens expressed anger at his remarks. They left comments such as, “With such a strict household registration system that requires timely submission of a death certificate, how come you don’t know the number of deaths?” and “Now that household information is all online, you should be able to find out the total number of death certificates within your system. How come you claim you don’t have December’s data?”
“The authorities’ claim that they put people first, putting life first is a sheer lie. They falsified COVID-related data when people were under lockdown, and they continued to falsify data when restrictions were removed. They have been lying all along,” Zhang said.
This, as well...
Heliobas Disciple
TB Fanatic
I just saw this article and a (admittedly very woo) lightbulb went off. Can't get everyone on board to take a new mrna vaxx without having the covid crisis to push them towards it, can you? Let's see how long they take to actually roll this out. If it is in trials for a few years, no conspiracy. If this is out on shelves ready for injection in a few months, tighten the tin foil.

 www.chinadaily.com.cn
(fair use applies)
www.chinadaily.com.cn
(fair use applies)
Sinopharm's mRNA Omicron vaccine gets green light for trials
By Cui Jia | China Daily
Updated: 2023-01-21 07:29
China National Biotec Group, a subsidiary of China National Pharmaceutical Group Co Ltd (Sinopharm), announced on Friday that its biotech unit in Shanghai has received regulatory approval for clinical trials of China's first mRNA COVID-19 vaccine targeting the Omicron strains.
The approval for Omicron-specific mRNA vaccine clinical trials, granted by the State Drug Administration on Thursday, is a "milestone" in the company's COVID-19 vaccine development after producing inactivated and genetic recombinant vaccines, Zhang Yuntao, vice-president and chief scientist of the group, said in a statement.
"From the early stage of research and development, CNBG has been working toward developing a world-class Omicron-specific mRNA vaccine in all aspects. Also, we have been making efforts to speed up the process for clinical trials," Zhang said.
CNBG began research on and development of Omicron-specific vaccines near the end of 2021, Zhang had previously said.
Jia Weiguo, chief scientist at CNBG's Virogin Biotech Company, said the new mRNA vaccine, which can encode the full length of the Omicron variant's S protein, could help the body to create antibodies more efficiently. It has proved effective in preventing infection in animal trials.
"The company's advanced mRNA-LNP encapsulation technology can further guarantee the production capacity of the vaccine," Jia said.
Virogin, which is based in Shanghai, has built a research and development platform, as well as production lines with an annual capacity of 2 billion doses of mRNA vaccine. They can quickly produce mRNA vaccines to deal with pandemics, CNBG said.
The company added that it will further assess the safety, immunogenicity and effectiveness of production during clinical trials.
According to the Ministry of Industry and Information Technology, China's annual COVID-19 vaccine production capacity has reached 7 billion doses, and the annual output exceeded 5.5 billion doses in 2022, which is a big improvement compared with the capacity of 5 billion doses in 2021.
Gao Fu, an academician with the Chinese Academy of Sciences, said in an interview with China Newsweek that vaccines against the mutant strains of COVID-19 should be approved for use as soon as possible.
Gao, also former head of the Chinese Center for Disease Control and Prevention, suggested that approval procedures for COVID-19 vaccines should be similar to those for influenza vaccines. If the vaccines come from the same company and use the same technology, there's no need for them to go through the whole clinical trial process, as long as they are only different in strain or gene sequence,according to the China Newsweek report published on Thursday.
Gao added that although breakthrough infections are common,vaccination can still provide protection, and that the elderly may need to get vaccinated every six months because of the possibility that COVID-19 could become an endemic disease over the long term.
Sinopharm's mRNA Omicron vaccine gets green light for trials
China National Biotec Group, a subsidiary of China National Pharmaceutical Group Co Ltd (Sinopharm), announced on Friday that its biotech unit in Shanghai has received regulatory approval for clinical trials of China's first mRNA COVID-19 vaccine targeting the Omicron strains.
www.chinadaily.com.cn
Sinopharm's mRNA Omicron vaccine gets green light for trials
By Cui Jia | China Daily
Updated: 2023-01-21 07:29
China National Biotec Group, a subsidiary of China National Pharmaceutical Group Co Ltd (Sinopharm), announced on Friday that its biotech unit in Shanghai has received regulatory approval for clinical trials of China's first mRNA COVID-19 vaccine targeting the Omicron strains.
The approval for Omicron-specific mRNA vaccine clinical trials, granted by the State Drug Administration on Thursday, is a "milestone" in the company's COVID-19 vaccine development after producing inactivated and genetic recombinant vaccines, Zhang Yuntao, vice-president and chief scientist of the group, said in a statement.
"From the early stage of research and development, CNBG has been working toward developing a world-class Omicron-specific mRNA vaccine in all aspects. Also, we have been making efforts to speed up the process for clinical trials," Zhang said.
CNBG began research on and development of Omicron-specific vaccines near the end of 2021, Zhang had previously said.
Jia Weiguo, chief scientist at CNBG's Virogin Biotech Company, said the new mRNA vaccine, which can encode the full length of the Omicron variant's S protein, could help the body to create antibodies more efficiently. It has proved effective in preventing infection in animal trials.
"The company's advanced mRNA-LNP encapsulation technology can further guarantee the production capacity of the vaccine," Jia said.
Virogin, which is based in Shanghai, has built a research and development platform, as well as production lines with an annual capacity of 2 billion doses of mRNA vaccine. They can quickly produce mRNA vaccines to deal with pandemics, CNBG said.
The company added that it will further assess the safety, immunogenicity and effectiveness of production during clinical trials.
According to the Ministry of Industry and Information Technology, China's annual COVID-19 vaccine production capacity has reached 7 billion doses, and the annual output exceeded 5.5 billion doses in 2022, which is a big improvement compared with the capacity of 5 billion doses in 2021.
Gao Fu, an academician with the Chinese Academy of Sciences, said in an interview with China Newsweek that vaccines against the mutant strains of COVID-19 should be approved for use as soon as possible.
Gao, also former head of the Chinese Center for Disease Control and Prevention, suggested that approval procedures for COVID-19 vaccines should be similar to those for influenza vaccines. If the vaccines come from the same company and use the same technology, there's no need for them to go through the whole clinical trial process, as long as they are only different in strain or gene sequence,according to the China Newsweek report published on Thursday.
Gao added that although breakthrough infections are common,vaccination can still provide protection, and that the elderly may need to get vaccinated every six months because of the possibility that COVID-19 could become an endemic disease over the long term.
Heliobas Disciple
TB Fanatic
Exactly. This is what Geert was saying early on, the more cases there are, the more opportunity for variants to emerge from the 'soup'. This has been my worry with what's going on in China, not that they may have started out with the Geert variant, but that they will spawn it.... See next post about all the variants now being found in China and Japan.
HD
Heliobas Disciple
TB Fanatic

COVID-19 News: East Asian Variants BF.7.14, BF.7.15, BF.5.2, BA.5.2.48, BA.5.2.49. BA.5.2.50 Continue To Wreak Havoc In China And Japan! Deaths Rising! - Thailand Medical News
COVID-19 News: The SARS-CoV-2 East Asian variants BF.7.14, BF.7.15, BF.5.1, BF.5.2, BA.5.2.48, BA.5.2.49 and the latest BA.5.2.50 are continuing to wreak havoc not in China and Japan but have also started new rise of infections in Taiwan, South Korea and Hong Kong and it its expected that many...
 www.thailandmedical.news
www.thailandmedical.news
COVID-19 News: East Asian Variants BF.7.14, BF.7.15, BF.5.2, BA.5.2.48, BA.5.2.49. BA.5.2.50 Continue To Wreak Havoc In China And Japan! Deaths Rising
Thailand Medical News
Jan 22, 2023
The SARS-CoV-2 East Asian variants BF.7.14, BF.7.15, BF.5.1, BF.5.2, BA.5.2.48, BA.5.2.49 and the latest BA.5.2.50 are continuing to wreak havoc not in China and Japan but have also started new rise of infections in Taiwan, South Korea and Hong Kong and it its expected that many South East Asia countries especially those promoting their countries as tourist destinations to the Chinese vectors are expected to be hit hard next.
China reported that there were at least another 12,600 COVID-19 deaths in the week just before Chinese New Year which falls on the 22nd of January 2023. However once again, international experts and local Chinese health care workers are disputing the figures, claiming that there is huge underreporting and that at least the actual number of deaths for the week preceding Chinese New Year could be as high as ten to twelve-fold.
The same goes for figures for COVID-19 hospitalizations that were reported by official Chinese COVID-19 News coverages claiming that there were only 471,739 COVID-19-related patients in hospitals nationwide on Jan. 19, including 51,683 in critical condition.
Chinese healthcare workers are claiming that the actual figures could be an astronomical figure of about 4.2 million people with more than half a million in critical condition! Already almost all hospitals nationwide are reporting lack of hospital beds and also staff shortages, drug and medical equipment shortages.
In Japan, the situation is just as bad with 398 COVId-19 deaths reported in the last 24 hours and more than 628,000 people hospitalized due to COVID-19
Coronavirus (COVID-19) infections in Japan - The Mainichi
Visualizing the data: information on COVID-19 infections
Strangely, not many mainstream media in Japan or even in the West are reporting about the catastrophic situation unfolding in Japan since the last 8 weeks that has one of the highest rates of vaccinated and boostered individuals in the world.
It is estimated that more than 17,000 Japanese have died from COVID-19 since the 1st Of December 2022 till now! But at the same time, excess deaths rates are also shooting up at an exponential phase according to local Japanese health experts as mortality rates within 30 days of acute COVID-19 infections are also rising with many dying due to strokes heart failures, sepsis and organ failures.
Meanwhile it was reported that Japan will downgrade the legal classification of COVID-19 this spring, bringing an end to quarantine guidelines for COVID-19 patients and review border controls and mask recommendations, Prime Minister Fumio Kishida announced Friday, marking a major policy change nearly three years since the start of the pandemic.
Although, the exact timing has yet to be decided, the government will downgrade COVID-19 from the current Class II to Class V under the Infectious Diseases Control Law, putting it on par with the seasonal flu.
The Japanese government will decide how to lift a range of pandemic measures after consulting a panel of medical experts under the health ministry, the prime minister told a news conference after meeting with ministers involved in the nation’s COVID-19 response.
Japanese chief cabinet secretary Hirokazu Matsuno said, without going into details, that border controls will also be reviewed with the impending classification change. This may mean that travelers from mainland China and Macao would no longer be required to show a negative PCR test or be asked to quarantine if they test positive on arrival.
Interestingly how Japan transitions to a post-pandemic normalcy remains uncertain, as it continues to see hundreds of daily deaths from COVID-19 and hospitals are packed with patients amid an eighth wave of infections.
At present, Japan recommends the use of masks indoors, except when people are able to keep a distance of at least 2 meters from one another or there’s no conversation. Outdoors, people are only encouraged to wear masks in crowds, according to the health ministry.
This new review comes long after many Western countries removed mask mandates and recommendations over the past year, though some have periodically recommended masking indoors when cases spike. Japanese officials have so far refrained from announcing an end to indoor masking entirely, given the unpredictability of the virus and the constantly mutating and highly contagious subvariants of the omicron strain.
There seems to a concerted effort by Western virologists, variant trackers, researchers and medical experts (many of who are either linked to institutions that frequently received funding from the vaccine manufacturers or are themselves receiving financial support from these vaccine manufacturers) to downplay the seriousness of the new East Asian variants and very little research have even been initiated on these new East Asian variants.
The coming weeks should prove to be interesting with millions of Chinese vectors already travelling to various parts of the globe to help spread these new SARS-CoV-2 subvariants and sub-lineages.
Heliobas Disciple
TB Fanatic
Jeff Zients, Who Predicted a "Winter of Illness and Death for the Unvaccinated" in 2021, set to become White House Chief of Staff
This winter's excess mortality is 35%, and our authorities do not care
 igorchudov.substack.com
igorchudov.substack.com
Jeff Zients, Who Predicted a "Winter of Illness and Death for the Unvaccinated" in 2021, set to become White House Chief of Staff
This winter's excess mortality is 35%, and our authorities do not care
Igor Chudov
12 hr ago
Remember Jeff Zients? Jeff is the former White House Covid Response Coordinator who famously hoped for a “winter of illness and death for the unvaccinated.” Here’s a video of him making that prediction:
Jeff resigned when the winter of illness and death did not materialize. The latest news is that Jeff is being brought back as the White House Chief of Staff.

I do not care about Jeff, besides remembering how he wished us to die a year ago. Bringing him back to the White House is a nice touch for the Biden administration.
The Winter of 2022-2023 Is a Winter of Illness and Death
Luckily, Jeff Zients was wrong about the previous winter of 2021-2022. The deaths were somewhat elevated but not catastrophic.This winter, however, is starting very disturbingly.
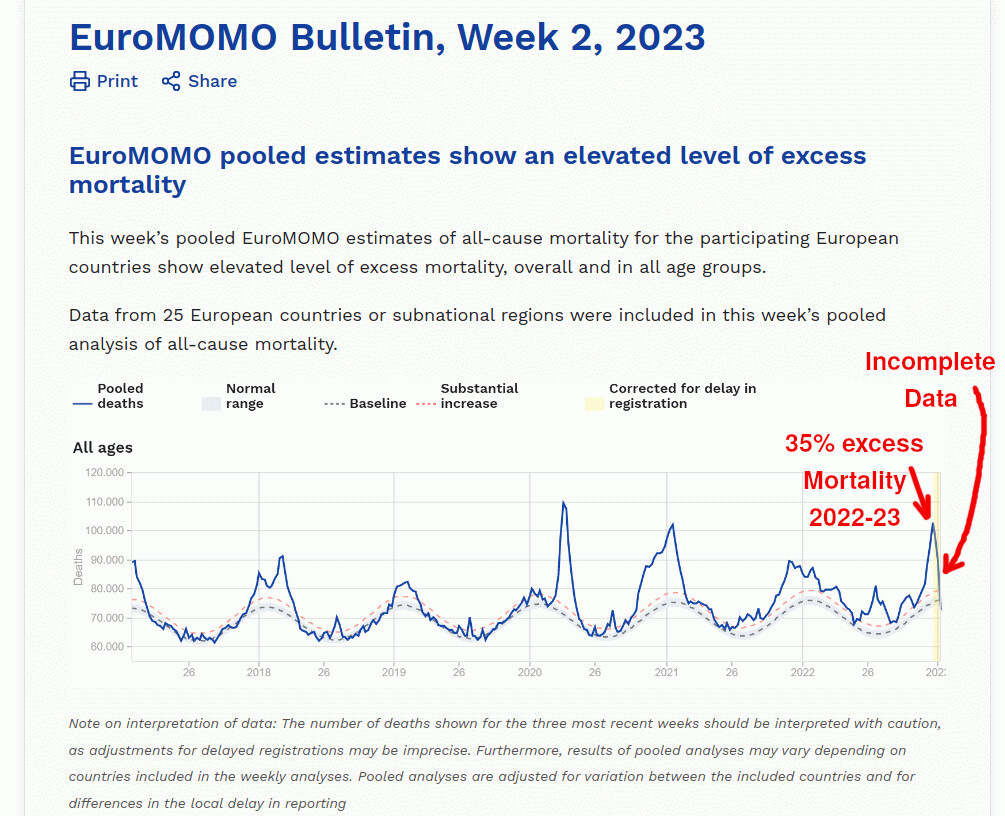
- Aggregated across Europe (see above), deaths for week 52, the last week when complete data is available, are at 35% above normal.
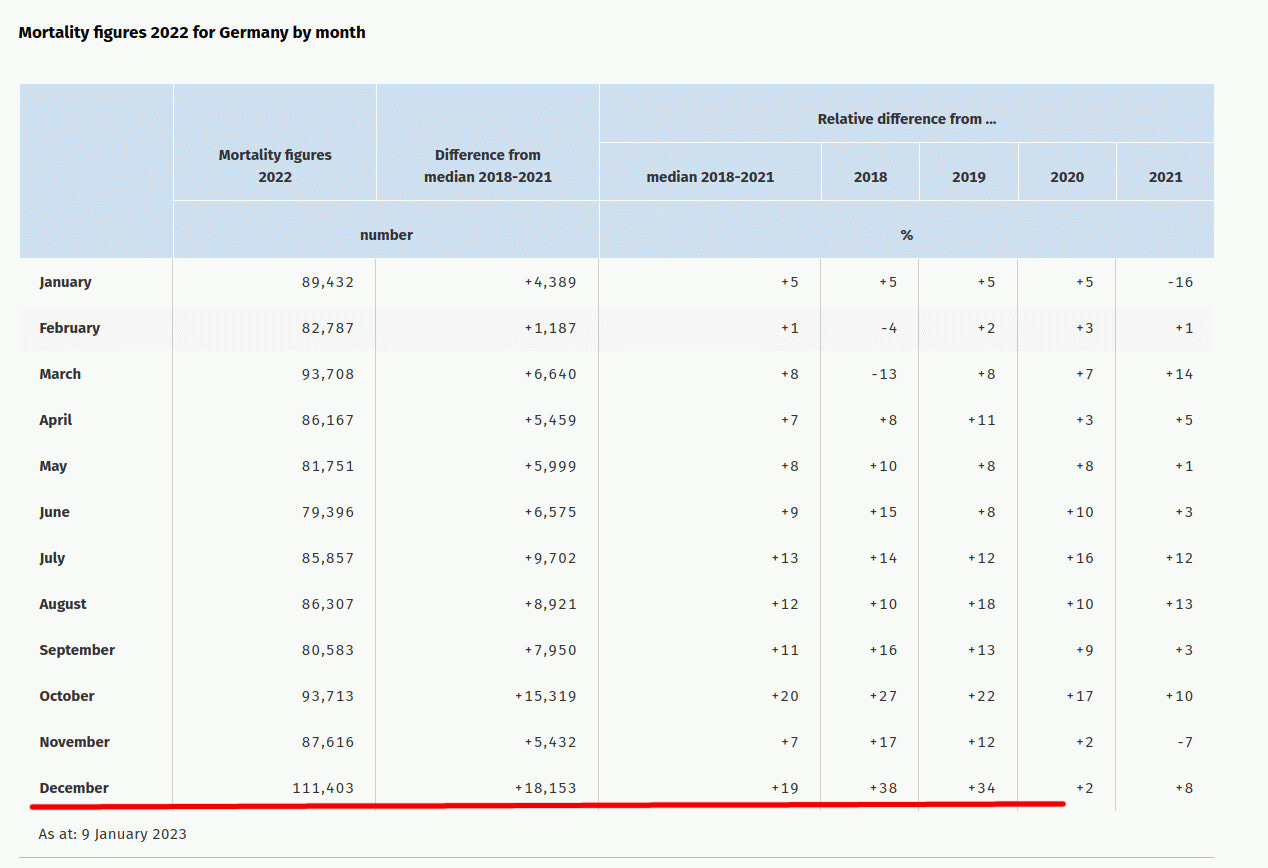
- Excess mortality in Germany in December is 36% above the 2018-2019 average.
The strange part is that Covid deaths explain only a small part of excess mortality.
For example, Germany saw 18,153 excess deaths in December. (DeStatis understates the excess number by including high-mortality 2020 and 2021 into the “previous years average”) Per Worldometer, Germany experienced 3,356 Covid deaths during the same months.
What explains the remaining 14,797 deaths? What killed almost 15 thousand Germans in December? Since there was nothing significant in the previous two years other than Covid and Covid vaccines, we can only blame these two causes, jointly or separately.
- We may be undercounting Covid deaths.
- We may see deaths from Covid vaccines that are NOT related to Covid infections.
- We may be observing vaccine-enabled reinfections with Covid that make people die at excess rates. The sudden and unexplained deaths occur due to longer Covid illnesses enabled by immune tolerance and the resulting organ damage. Such deaths are NOT recorded as Covid deaths.
Igor’s Newsletter
Booster-Caused IgG4 Immune Tolerance Explains Excess Mortality and "Chronic Covid"
Booster-Caused IgG4 Immune Tolerance Explains Excess Mortality and "Chronic Covid"
Whatever is happening is a national emergency in all European countries. The lack of attention from health authorities is stunning. The refrain from rare newspaper articles like this one is, “we have no idea why people are dying, and we do not care, but we are sure it is not the vaccines.” Enjoy this stupid passage:
The article tries to convince the readers that we should only look at the immediate, officially recognized deaths that happen within a few days of vaccination (and were intentionally undercounted).
However, excess mortality of 23% was seen even in the Pfizer trial, where 21 people died in the vaccine arm, and only 17 died in the placebo arm within six months of their vaccinations.

Without individual-level data, which the authorities are refusing to provide or look at, we cannot figure out what is happening. We can only make guesses.
Meanwhile, people are dying.
Nobody seems to care about this besides a few people on Substack and Twitter. The problem is that deaths are increasing instead of decreasing, and excess mortality threatens me, you, and our loved ones.
Too many people see it as a political contest to blame or exonerate their favorite party.
I am appealing to everyone to see it as a threat to ourselves and our families instead of treating it as a blame game. We must address excess mortality out of pure self-preservation.
Do you think our authorities will seriously investigate deaths, or will they try to sweep them under the rug?
Do you think Jeff Zients will help the White House investigate the situation honestly?
Please SHARE this article. We need to make as much noise as possible!
Zoner
Veteran Member
Yes, that article shows we aren't too far away. Sadly, Geert will be proven right eventually. I just got my extra supply of Ivermectin and other supplements for antivirals and long covid. And staying close to Jesus. He is the only Light I'm seeing...Exactly. This is what Geert was saying early on, the more cases there are, the more opportunity for variants to emerge from the 'soup'. This has been my worry with what's going on in China, not that they may have started out with the Geert variant, but that they will spawn it.... See next post about all the variants now being found in China and Japan.
HD
Tristan
Has No Life - Lives on TB
Dr. Campbell goes over European Excess Deaths data...
View: https://www.youtube.com/watch?v=ku2Fv7xnL1o
rt: 13:09
To quote the song by Frieda: "There's something going on!"
rt: 13:09
To quote the song by Frieda: "There's something going on!"
naegling62
Veteran Member

Heliobas Disciple
TB Fanatic

US proposes once-a-year COVID shots for most Americans
WASHINGTON (AP) — U.S. health officials want to make COVID-19 vaccinations more like the annual flu shot. The Food and Drug Administration on Monday proposed a simplified approach for future vaccination efforts, allowing most adults and children to get a once-a-year shot to protect against the...
apnews.com
US proposes once-a-year COVID shots for most Americans
By MATTHEW PERRONE
Jan 24 2023
WASHINGTON (AP) — U.S. health officials want to make COVID-19 vaccinations more like the annual flu shot.
The Food and Drug Administration on Monday proposed a simplified approach for future vaccination efforts, allowing most adults and children to get a once-a-year shot to protect against the mutating virus.
This means Americans would no longer have to keep track of how many shots they’ve received or how many months it’s been since their last booster.
The proposal comes as boosters have become a hard sell. While more than 80% of the U.S. population has had at least one vaccine dose, only 16% of those eligible have received the latest boosters authorized in August.
The FDA will ask its panel of outside vaccine experts to weigh in at a meeting Thursday. The agency is expected to take their advice into consideration while deciding future vaccine requirements for manufacturers.
In documents posted online, FDA scientists say many Americans now have “sufficient preexisting immunity” against the coronavirus because of vaccination, infection or a combination of the two. That baseline of protection should be enough to move to an annual booster against the latest strains in circulation and make COVID-19 vaccinations more like the yearly flu shot, according to the agency.
For adults with weakened immune systems and very small children, a two-dose combination may be needed for protection. FDA scientists and vaccine companies would study vaccination, infection rates and other data to decide who should receive a single shot versus a two-dose series.
FDA will also ask its panel to vote on whether all vaccines should target the same strains. That step would be needed to make the shots interchangeable, doing away with the current complicated system of primary vaccinations and boosters.
The initial shots from Pfizer and Moderna — called the primary series — target the strain of the virus that first emerged in 2020 and quickly swept across the world. The updated boosters launched last fall were also tweaked to target omicron relatives that had been dominant.
Under FDA’s proposal, the agency, independent experts and manufacturers would decide annually on which strains to target by the early summer, allowing several months to produce and launch updated shots before the fall. That’s roughly the same approach long used to select the strains for the annual flu shot.
Ultimately, FDA officials say moving to an annual schedule would make it easier to promote future vaccination campaigns, which could ultimately boost vaccination rates nationwide.
The original two-dose COVID shots have offered strong protection against severe disease and death no matter the variant, but protection against mild infection wanes. Experts continue to debate whether the latest round of boosters significantly enhanced protection, particularly for younger, healthy Americans.
Heliobas Disciple
TB Fanatic

80 Percent of Chinese Population Infected With COVID: Top Chinese Health Official
About 80 percent of China's 1.4 billion population have been infected with COVID-19, a top Chinese health official said on Saturday.
www.theepochtimes.com
80 Percent of Chinese Population Infected With COVID: Top Chinese Health Official
By Aldgra Fredly
January 23, 2023
Eighty percent of people in China have been infected with COVID-19 amid Lunar New Year celebrations, a top Chinese health official said on Jan. 21.
China has seen a surge in COVID-19 cases across the country. Most of the population has been infected, according to officials and studies, and crematoriums and hospitals have been overwhelmed. But the regime’s continuing coverup of the death toll makes it difficult to ascertain the true scale of the outbreak.
Wu Zunyou, chief epidemiologist of China’s Disease Control and Prevention Center, stated in a Weibo post that 80 percent of the population had been infected in the latest outbreak. His comment aligns with statements made by other Chinese officials in recent weeks and a study showing that 900 million Chinese had been infected.
The explosive outbreak raised concerns about the possibility of a second wave in the coming months amid the Lunar New Year travel rush. The Ministry of Transport expected more than 5 billion passenger trips during the festive season.
More than 1.1 million people in China traveled by air nationwide on Jan. 20, and 800,000 people took domestic flights on Lunar New Year’s Eve on Jan. 21, double the number from the previous year, South China Morning Post reported.
Overcrowded Hospitals, Funeral Homes
Overcrowded hospitals and funeral homes suggest that China is battling a severe outbreak with a high death toll.
Lew Mon-hung, a former member of the CCP’s political advisory body, said that “all outpatient departments and emergency departments of hospitals are crowded with people and with no beds left for people to stay in the hospital.”
“The funeral homes are overwhelmed, and the dead bodies pile up,” Lew said, according to an earlier report by The Epoch Times.
He pointed out that the daily infection rate has increased to 1 million in Zhejiang Province. Officials in Qingdao city acknowledged that its daily infection rate had increased to 500,000.
The confirmed cases in Dongguan city in central Guangdong Province increased by 250 million to 300 million. The densely populated provinces of Sichuan and Henan have recorded an infection rate of more than 80 percent.
“My relatives, my brother and sister, and my mother in Guangzhou were all infected. A one- to two-kilometer line [about one mile] was outside the Guangzhou Galaxy Martyr Cemetery, waiting to register for cremation,” Lew said.
“Not only did the people form long lines outside the funeral homes in different places in China, but they also needed to wait half a month, or even over a month, to get their relatives to be cremated.”
Lew claimed that there is currently a coffin shortage in China. He said that normal civilians, who were forced to turn to scalpers, “had to pay 38,500 yuan [$5,700] to move the body to a funeral home.”
Families are sometimes forced to store the corpses of loved ones at home or in their vehicles, an anonymous Shanghai resident told The Epoch Times. Shanghai resident Zhang Pei (a pseudonym) told The Epoch Times that a friend paid an extra $5,000 to obtain timely cremation for an elderly family member.
Shanghai resident Wu Fangyan (a pseudonym) said on Jan. 13 that “hospitals are still crowded. Only one medication is given for each visit, and the one medication does not reduce the fever, so you must go back in the afternoon and wait in line for hours.”
Wu expressed frustration that doctors are unwilling to give more than one dose of medicine.
“Sometimes you can’t even get [one dose of] medicine after lining up for hours.”
“The government’s attitude toward us is to ignore whether we can survive or not.” The strong survive and the rest die, Wu said.
Heliobas Disciple
TB Fanatic
Opinion | The Deceptive Campaign for Bivalent Covid Boosters
Studies show they fail to live up to their promise, but vaccine makers and experts keep pushing them.
 www.wsj.com
www.wsj.com
The Deceptive Campaign for Bivalent Covid Boosters
Studies show they fail to live up to their promise, but vaccine makers and experts keep pushing them.
By Allysia Finley - WALL STREET JOURNAL
Jan. 22, 2023 3:10 pm ET
You might have heard a radio advertisement warning that if you’ve had Covid, you could get it again and experience even worse symptoms. The message, sponsored by the Health and Human Services Department, claims that updated bivalent vaccines will improve your protection.
This is deceptive advertising. But the public-health establishment’s praise for the bivalent shots shouldn’t come as a surprise. Federal agencies took the unprecedented step of ordering vaccine makers to produce them and recommending them without data supporting their safety or efficacy.
The idea of updating mRNA Covid shots every season originally held promise. One advantage of mRNA technology is that manufacturers can tweak the genetic sequence and rapidly produce new vaccines targeting new variants. Hence the bivalent boosters targeting the BA.4 and BA.5 Omicron variants along with the original Wuhan strain.
But three scientific problems have arisen. First, the virus is evolving much faster than the vaccines can be updated. Second, vaccines have hard-wired our immune systems to respond to the original Wuhan strain, so we churn out fewer antibodies that neutralize variants targeted by updated vaccines. Third, antibodies rapidly wane after a few months.
Two studies in the New England Journal of Medicine this month showed that bivalent boosters increase neutralizing antibodies against the BA.4 and BA.5 variants, but not significantly more than the original boosters. In one study, antibody levels after the bivalent boosters were 11 times as high against the Wuhan variant as BA.5.
The authors posit that immune imprinting “may pose a greater challenge than is currently appreciated for inducing robust immunity against SARS-CoV-2 variants.” This isn’t unique to Covid or mRNA vaccines, though boosters may amplify the effect. Our first exposure as children to the flu—whether by infection or vaccination—affects our future response to different strains.
The original Covid vaccines and boosters trained our memory B-cells to produce antibodies against the Wuhan variant. As the University of Pennsylvania’s Paul Offit explains in a New England Journal of Medicine article, previously vaccinated people who received the bivalent booster were “primed” to respond to the Wuhan strain and mounted an inferior antibody response to other variants.
The studies’ findings contradict November press releases from Pfizer and Moderna asserting that their bivalents produced a response to the BA.4 and BA.5 variants four to six times that of the original boosters. These claims are misleading. Neither vaccine maker conducted a randomized trial. They tested the original boosters last winter, long before the BA.5 surge and 4½ to six months after trial participants had received their third shots. The bivalents, by contrast, were tested after BA.5 began to surge, 9½ to 11 months after recipients had received their third shots.
A longer interval between shots would increase the antibody boost to the BA.5 variant. So would a prior infection with the BA.5 variant. In other words, people who received the bivalent boosters in August would have been primed to produce more antibodies in response to BA.5.
The vaccine makers designed their studies to get the results they wanted. Public-health authorities didn’t raise an eyebrow, but why would they? They have a vested interest in promoting the bivalents.
The Food and Drug Administration ordered the vaccine makers in June to update the boosters against BA.4 and BA.5 and rushed in late August to authorize the bivalents before clinical data were available. The Centers for Disease Control and Prevention recommended the bivalents for all adults without any evidence that they were effective or needed.
Vaccine makers could have performed small randomized trials last summer and early fall that tested the bivalents against the original boosters and a placebo group.
Results could have been available by the end of September. But the public-health authorities didn’t want to wait—and now we know why.
The CDC published a study in November that estimated the bivalents were only 22% to 43% effective against infection during the BA.5 wave—their peak efficacy. As antibodies waned and new variants took over later in the fall, their protection against infection probably dropped to zero.
Another CDC study, in December, reported that seniors who received bivalents were 84% less likely to be hospitalized than the unvaccinated, and 73% less likely than those who had received two or more doses of the original vaccine. But neither study controlled for important confounding factors—for one, that the small minority who got bivalents were probably also more likely than those who hadn’t to follow other Covid precautions or seek out treatments such as Paxlovid.
FDA Commissioner Robert Califf tweeted on Jan. 11 that “COVID-19 vaccines have been associated with a significant reduction in hospitalization and death” (my emphasis). He should know that correlation doesn’t prove causation. A study found the unvaccinated were significantly more likely to get into car accidents, but that doesn’t mean vaccines prevent crashes.
Many of the same experts who trashed observational studies supporting hydroxychloroquine and ivermectin now flog intrinsically flawed studies on bivalent boosters. After zealously promoting the bivalents, they may be seeking vindication. But science isn’t about vindication.
Covid vaccines mitigated severe illness while most Americans gained immunity through natural infection, which substantially boosts protection. There’s a growing consensus that we need better vaccines and treatments to protect those still at risk. But we also need honest public-health leaders.
Heliobas Disciple
TB Fanatic
Here is a substack discussing the article in the post above this from the Wall St Journal.
 (fair use applies)
(fair use applies)
Original Antigenic Sin Hits the Mainstream
WSJ catching up again
NE - nakedemperor.substack.com
12 hr ago
One of the first things I wrote about on Substack, in December 2021, was Original Antigenic Sin (OAS). The article titled “The New Normal - Pandemics of the Vaccinated? Are we beginning to see further evidence of ADE or OAS occurring in the UK data?” did exactly what is says on the tin, explored whether OAS was being seen in the UK data. I can’t remember how long I had been talking about it before then but it was at least six months.
Now, almost two years since I first started reading about the phenomenon, it seems the concept is acceptable enough to enter mainstream consciousness. The Overton window of discourse has shifted.
Allysia Finley at the Wall Street Journal has written another interesting and critical article, this time including OAS. She doesn’t call it OAS, she calls it immune priming, but it’s OAS.
The article called “The Deceptive Campaign for Bivalent Covid Boosters”, looks at the misleading claims that you could get worse Covid symptoms unless you get your bivalent booster. These arguments are interesting enough but the scattering of OAS information throughout the piece is what caught my eye.
When I was at school I was told to put any bad news in the middle of a letter, sandwiching it between more positive information to distract from the negative. Allysia was clearly taught the same thing as OAS is mentioned in between two not-quite-as-bad facts.
In fact it is worse than Allysia points out. Not only have vaccinated people hard-wired their immune systems to respond to the original Wuhan strain, they have hard-wired them to a small portion of that strain - the spike protein. Whilst immune priming also happens when you get infected naturally, the hard-wiring is to all parts of the virus. When priming is only to the spike protein, all the virus needs to do is mutate the spike and suddenly you have no defences but you still produce defences to the original spike.
And to any new readers who are thinking “but the FDA must have spotted that deception, right?”. Wrong. Ms. Finley gives you the answer, they “didn’t raise an eyebrow, but why would they? They have a vested interest in promoting the bivalents.”
In reality, it is worse than that, as seen in the recent Cleveland Study

A few more years and we’ll be reading in the MSM how they’ve noticed a switch to IgG4 after booster 17.

Original Antigenic Sin Hits the Mainstream
WSJ catching up again
NE - nakedemperor.substack.com
12 hr ago
One of the first things I wrote about on Substack, in December 2021, was Original Antigenic Sin (OAS). The article titled “The New Normal - Pandemics of the Vaccinated? Are we beginning to see further evidence of ADE or OAS occurring in the UK data?” did exactly what is says on the tin, explored whether OAS was being seen in the UK data. I can’t remember how long I had been talking about it before then but it was at least six months.
Now, almost two years since I first started reading about the phenomenon, it seems the concept is acceptable enough to enter mainstream consciousness. The Overton window of discourse has shifted.
Allysia Finley at the Wall Street Journal has written another interesting and critical article, this time including OAS. She doesn’t call it OAS, she calls it immune priming, but it’s OAS.
The article called “The Deceptive Campaign for Bivalent Covid Boosters”, looks at the misleading claims that you could get worse Covid symptoms unless you get your bivalent booster. These arguments are interesting enough but the scattering of OAS information throughout the piece is what caught my eye.
When I was at school I was told to put any bad news in the middle of a letter, sandwiching it between more positive information to distract from the negative. Allysia was clearly taught the same thing as OAS is mentioned in between two not-quite-as-bad facts.
But three scientific problems have arisen. First, the virus is evolving much faster than the vaccines can be updated. Second, vaccines have hard-wired our immune systems to respond to the original Wuhan strain, so we churn out fewer antibodies that neutralize variants targeted by updated vaccines. Third, antibodies rapidly wane after a few months.
In fact it is worse than Allysia points out. Not only have vaccinated people hard-wired their immune systems to respond to the original Wuhan strain, they have hard-wired them to a small portion of that strain - the spike protein. Whilst immune priming also happens when you get infected naturally, the hard-wiring is to all parts of the virus. When priming is only to the spike protein, all the virus needs to do is mutate the spike and suddenly you have no defences but you still produce defences to the original spike.
The authors [in studies in the New England Journal of Medicine] posit that immune imprinting “may pose a greater challenge than is currently appreciated for inducing robust immunity against SARS-CoV-2 variants.”
The original Covid vaccines and boosters trained our memory B-cells to produce antibodies against the Wuhan variant. As the University of Pennsylvania’s Paul Offit explains in a New England Journal of Medicine article, previously vaccinated people who received the bivalent booster were “primed” to respond to the Wuhan strain and mounted an inferior antibody response to other variants.
Allysia goes on to show how these finding contradict the pharmaceutical press releases because “the vaccine makers designed their studies to get the results they wanted”.And to any new readers who are thinking “but the FDA must have spotted that deception, right?”. Wrong. Ms. Finley gives you the answer, they “didn’t raise an eyebrow, but why would they? They have a vested interest in promoting the bivalents.”
The Centers for Disease Control and Prevention recommended the bivalents for all adults without any evidence that they were effective or needed.
The article points out that a CDC study showed the bivalents were only 22% to 43% effective during their peak efficacy. “As antibodies waned and new variants took over later in the fall, their protection against infection probably dropped to zero.”In reality, it is worse than that, as seen in the recent Cleveland Study
The risk of COVID-19 also varied by the number of COVID-19 vaccine doses previously received. The higher the number of vaccines previously received, the higher the risk of contracting COVID-19.

A few more years and we’ll be reading in the MSM how they’ve noticed a switch to IgG4 after booster 17.
Heliobas Disciple
TB Fanatic

Africa Is Starkly Unvaccinated
Africa is starkly unvaccinated, and starkly unvanquished by COVID. Let's study that victory with utmost diligence.
 colleenhuber.substack.com
colleenhuber.substack.com
Africa Is Starkly Unvaccinated
Africa is starkly unvaccinated, and starkly unvanquished by COVID. Let's study that victory with utmost diligence.
Colleen Huber NMD
Jan 15
Africa as a whole is very strikingly unvaccinated, according to Johns Hopkins University, Our World in Data.

Coronavirus (COVID-19) Vaccinations
Let’s keep in mind that most striking continent on an otherwise bleak world map, [1] as we examine the following map, which shows Africa’s burden of COVID cases since the beginning of COVID. [2]
Here is Africa’s relative share of COVID cases since the beginning of COVID:
COVID-19 Map - Johns Hopkins Coronavirus Resource Center
The data reports that can be expected three years into a pandemic
One would reasonably expect a worldwide pandemic that began three years ago to have been recorded with some ballpark accuracy in case counts, and morbidity and mortality data throughout the world by now, as each hemisphere has been through three winters. One would also expect that a worldwide vaccine campaign that peaked over a year ago to have resulted in reliable vaccine uptake maps. One would expect a general consensus regarding such data. So let’s accept the above maps as not (or not yet) disputed, and as reliable documentation of historical events of pinnacle importance, events that behoove humanity to understand well, and to understand as thoroughly as if our future well-being depends on it.
One who has faith in the practice of vaccination would have also expected that vaccines carrying the name of the pandemic to have mitigated case counts of the same disease. How then is the overall experience of the African continent to be understood?
Africa was not the only part of the world where reported COVID cases have been low. Prior to vaccination, numerous countries were barely impacted at all by COVID. Let’s zoom out from Africa now to examine events in other countries.
Former US Dept of Justice adviser Gavin de Becker wrote an article on Children’s Health Defense [3] that also appears in a book by Edward Dowd, Cause Unknown; in it he looks at COVID mortality in various nations, primarily in Asia, but also in Africa, Europe, Latin America and the Middle East, after COVID began, as well as before and after the launch of their vaccination campaigns. Three of de Becker’s timelines are as follows. De Becker indicates with a syringe pointer the date at which each of the following countries began their COVID vaccine campaigns.
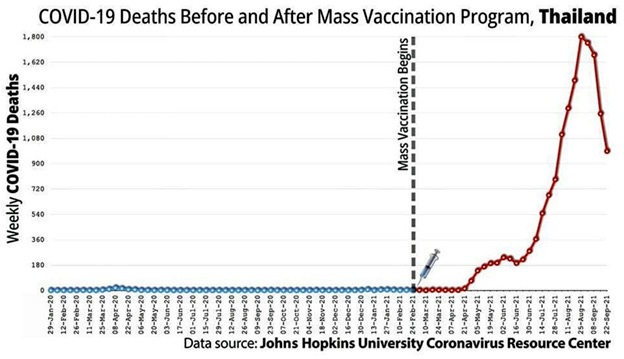
Gavin de Becker, Seeing Is Believing: What the Data Reveal About Deaths Following COVID Vaccine Rollouts Around the World
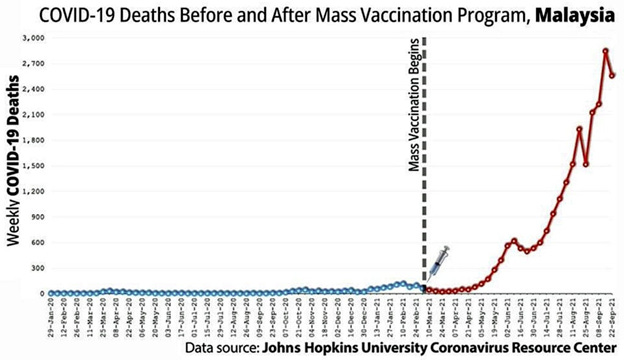
Gavin de Becker, Seeing Is Believing: What the Data Reveal About Deaths Following COVID Vaccine Rollouts Around the World
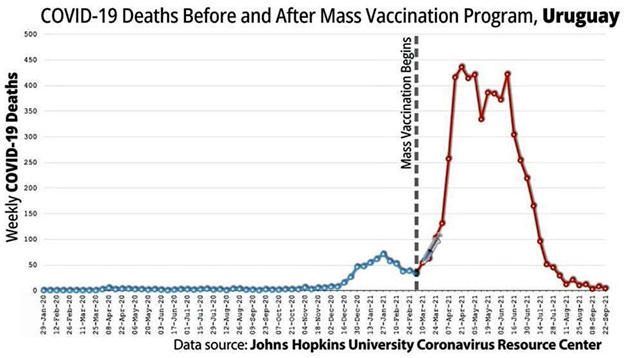
Gavin de Becker, Seeing Is Believing: What the Data Reveal About Deaths Following COVID Vaccine Rollouts Around the World
De Becker notes that “the reality displayed on the graphs you’ve seen is undeniable, cannot be unseen, and is available to anyone [4] more interested and more industrious than media and governments have been.”
Elusive truth in morbidity and mortality data: the PCR problem
De Becker’s article, as the Johns Hopkins data, necessarily relies on reports that are fraught with much difficulty, for the reasons I review below, primarily the wildly misapplied PCR “test” to COVID diagnosis. However, because that alleged test is primarily how the world has evaluated and tallied COVID cases and deaths for three years, we are necessarily dependent on and limited to the derived data from this alleged test for any meaningful assessment of COVID epidemiology.COVID-19 diagnoses have been troublesome from the beginning. It has been noted, including at Johns Hopkins University, which produces the most university-based statistical data on COVID, that reported deaths from flu, pneumonia, heart disease and diabetes decreased significantly in 2020, while COVID-19 deaths became the cause of death listed for now over six million lost lives around the world. Flu and pneumonia as primary causes of death nearly disappeared. For every lost life and every grieving family, the signs and symptoms of this respiratory disease phenomenon occurred, and then it is a matter of disagreement as to whether we will call those deaths flu, pneumonia or COVID, with no particular loss of life any less tragic for the bereaved from one diagnosis from the others. Cardiovascular mortality reports also dropped precipitously, without any credible reason for the change. Another unexplained surprise to epidemiologists was that those deceased with a COVID cause of death exceeded the average age of life expectancy in the US. Genevieve Briand of Johns Hopkins University discusses these anomalies. [5]
Flu and pneumonia had always been among the most threatening diseases for seniors. And then the mortality reports changed. There are two major influences that created an alleged 2020 pandemic out of what was otherwise a typical flu year. The following two factors led to false reporting of US mortality data for COVID:
First domino falls
The first was a manufacturing technique that wound up being wildly misappropriated as a diagnostic test, despite the prior protests of its inventor, the late Kary Mullis, PhD. [6] The essence of the world’s confusion and fear of COVID stems from the testing itself. Reverse-transcriptase, polymerase chain reaction (RT-PCR) is a method for producing more RNA nucleic acid sequences. Essentially, PCR does what it was designed by Mullis to do: It matches or aligns specific genetic signatures between a given test reagent and a sample. As the test is run in consecutive cycles, each cycle multiplies the sample. So that sample then grows exponentially. The PCR is simply incapable to determine if the introduced sample contains adequate viral particles or virions to rise to the threshold of causing an infection. For those who have worked with PCR, it is understood that any PCR process run through 20 or more cycles is useless for detection. The CDC acknowledged that 33 cycles or more are unlikely to detect active virus. Yet for all of 2020, throughout the US, the number of cycles used in “COVID-19 testing” have been above 37 and often well into the 40’s. [7] Boris Borovoy and I discuss problems related to this misuse of PCR. [8] The misplaced faith in this manufacturing technique as a test of anything having to do with contagion was the misjudgment at the core of worldwide disaster.
From such a simple decision and widespread acquiescence to create a test out of a non-test, whether by error, misunderstanding or possibly worse on the part of some: deliberate misuse of an industrial process, a new world may be in its birth from this practice. This misuse, born of widespread misunderstanding of PCR, became the pretext for the estimated four trillion dollar COVID industry.
Second domino falls
The second factor that fired up the COVID engines, so to speak, at least in the United States, was the financially-incentivized COVID cause of death. Under the US CARES Act, hospitals were compensated more than twice as much money [9] for a COVID case than a flu or pneumonia case, [10] and the most lethal treatments were compensated even further. [11] Many US hospitals made millions of dollars from this shift in diagnosis during treatment and on death certificates.Other forensic evidence shows lack of a pandemic in 2020. Wall Street seems to need and to have greater reliance on accurate data than governments. COVID is primarily a pathogenic disease of the respiratory tract, with dyspnea (shortness of breath) noted as one of the most common symptoms along with coughing, in which acute and late-stage care often involves supplemental oxygen. Oxygen use would be the most reliable artifact of COVID care. Therefore, we looked at sales of medical oxygen, by revenue of the top companies that produce it, in 2020 vs 2019. We then noted that their sales decreased in that time. Meanwhile, sales by six of the top oxygen concentrator producers trading on the NYSE had increased by less than one percentage point from 2019 to 2020. [12] This is the 0.93% in the last line of the following table. In the same time, the world’s population grew by 1.05%. [13]
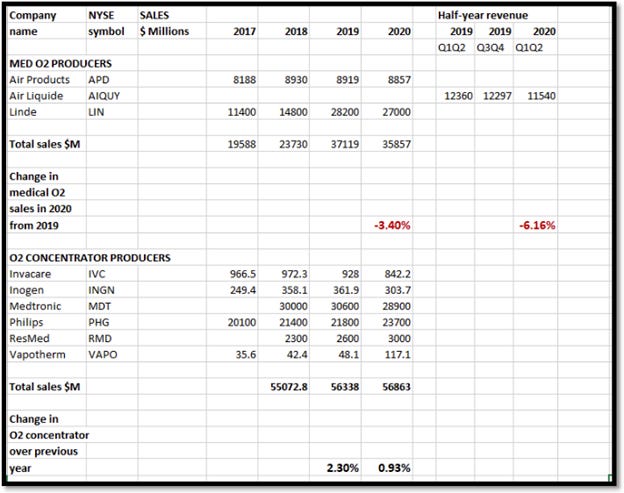
C Huber, B Borovoy. Data that disprove the COVID-19 pandemic. Dec 19, 2020. PDMJ. PDMJ: Primary Doctor Medical Journal
For whatever other wealth distribution occurred during what is widely considered to be the peak pandemic year of 2020, the New York Stock Exchange does not reflect the primary medical need of the pandemic patients to have made impact on the revenue of the main companies supplying that medical demand.
[continued next post]
Heliobas Disciple
TB Fanatic
[continued from post above]
As fortune would have it, the unpatented and relatively inexpensive half-century old drug ivermectin, whose inventors won the Nobel Prize for Medicine in 2015, [14] also has been the most effective medicine against COVID, [15] due in part to its specific effect against RNA transcriptase, as well as its blocking effect on all three parts of the trimeric spike protein, and other mechanisms. [16]
Hydroxychloroquine is also used widely throughout at least equatorial regions of Africa as a prophylactic against parasites, but which fortunately has now been studied extensively and used successfully as both prevention and treatment of COVID disease, and as inhibitor of SARS-CoV-2 replication and activity. This is shown in over 380 studies conducted in 55 countries. [17]
Africa led the way and inspires the world. Are the politicians and “public health experts” of the rest of the world humble enough to admit their grotesque errors, even crimes, and to learn from the peoples of the African nations, their experiences and lessons on handling a pandemic?
Or will ethnocentrism or a hostile and racist pride, or the sheer greed stimulated by the lucrative COVIDmania boondoggle, prevent the rest of the world’s willingness to learn from the African experience? Will such provincial and purchased attitudes bury the 21st century’s most important lesson to date?
[1] Johns Hopkins University. Our world in data. Jan 15 2023 update. Coronavirus (COVID-19) Vaccinations
[2] Johns Hopkins University. Coronavirus Resource Center. COVID-19 Map - Johns Hopkins Coronavirus Resource Center
[3] G de Becker. Seeing is believing: What the data reveal about deaths following COVID vaccine rollouts around the world. Jan 9 2023. The Defender. Seeing Is Believing: What the Data Reveal About Deaths Following COVID Vaccine Rollouts Around the World
[4] Johns Hopkins University. Coronavirus Resource Center. See the latest data in your region - Johns Hopkins Coronavirus Resource Center
[5] G Briand. COVID-19 deaths: A look at US data. Mar 18, 2021. PDMJ: Primary Doctor Medical Journal
[6] K Mullis, interviewed. Every scary thing you’re being told depends on the unreliable PCR test. English Rose. Bitchute video. Every Scary Thing You're Being Told, Depends On the Unreliable PCR Test | English Rose
[7] A Mandavilli. Your coronavirus test is positive. Maybe it shouldn’t be. New York Times. Aug 29, 2020. https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
[8] C Huber, B Borovoy. Data that disprove the COVID-19 pandemic. Dec 19, 2020. PDMJ. PDMJ: Primary Doctor Medical Journal
[9] M Rogers. USA Today. Fact check: Hospitals get paid more if patients listed as COVID-19, on ventilators. Apr 24 2020. Fact check: Hospitals get paid more if patients listed as COVID-19, on ventilators
[10] American Hospital Association. Special Bulletin: Senate passes the Coronavirus Aid, Relief and Economic Security Act. Special Bulletin: Senate Passes the Coronavirus Aid, Relief, and Economic Security (CARES) Act | AHA
[11] S Begley. With ventilators running out, doctors say the machines are overused for COVID-19. STAT. Apr 8 2020. With ventilators running out, doctors say the machines are overused for Covid-19
[12] C Huber, B Borovoy. Data that disprove the COVID-19 pandemic. Dec 19, 2020. PDMJ. PDMJ: Primary Doctor Medical Journal
[13] Worldometer. World population. World Population Clock: 8 Billion People (LIVE, 2023) - Worldometer
[14] M Turkia. A timeline of ivermecting-related events in the COVID-19 pandemic [preprint]. Mar 2021. https://www.researchgate.net/public...Events_in_the_COVID-19_Pandemic_March_24_2021
[15] L Clay, J Druce, et al. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Jun 2020. Antiviral Res. https://www.sciencedirect.com/science/article/pii/S0166354220302011?via=ihub
[16] C Huber. Ivermectin is safe and effective: the evidence. Sep 9 2021.
The Defeat Of COVID
Ivermectin is safe and effective: The evidence
Ivermectin is on the World Health Organization (WHO) List of Essential Medicines and is approved by the US Food and Drug Administration (FDA). This well-tolerated but potent anti-parasitic medicine has been prescribed billions of times in its 36-year history against a wide range of parasites. It is a drug in the avermectin family, so named because thos…
Read more
a year ago · 46 likes · 28 comments · Colleen Huber NMD
[17] Science Direct. COVID-19 treatment studies for hydroxychloroquine. Updated Jan 15 2023. https://www.sciencedirect.com/science/article/pii/S0166354220302011
[18] C Huber. Thank you x 3, Africa. Jun 4 2022.
The Defeat Of COVID
Thank you x 3, Africa!
Last week in Davos, the 47 African countries – almost the entire 54-country African continent - were unified at the WHO meeting, led by Botswana, as seen in the video linked below. These 47 countries that are members of the World Health Organization (WHO) were joined by a number of other large and small countries across the globe, in registering a tac…
Read more
7 months ago · 124 likes · 57 comments · Colleen Huber NMD
Thank you x 3, Africa!
[19] J Roguski. 100 reasons. Jan 5 2023.
James Roguski
100 Reasons
Please watch the video or listen to the audio and follow along with the transcript below…
Read more
10 days ago · 220 likes · 31 comments
How Africa defeated COVID so decisively without vaccines
Part of the African continent’s success is no doubt due to a fortunate accident of microbiology, infectious diseases, pharmacology and immunology. It so happens that two of the most effective treatments for COVID, ivermectin and hydroxychloroquine, are also routine prophylactic weekly medicines throughout equatorial Africa, because they happen to be known for a half-century as the most effective, applicable and safest anti-parasite medications. So the population, particularly through about 31 countries, the tropical middle rectangle roughly, of Africa already were well-equipped prior to COVID events launching in late 2019 to early 2020.As fortune would have it, the unpatented and relatively inexpensive half-century old drug ivermectin, whose inventors won the Nobel Prize for Medicine in 2015, [14] also has been the most effective medicine against COVID, [15] due in part to its specific effect against RNA transcriptase, as well as its blocking effect on all three parts of the trimeric spike protein, and other mechanisms. [16]
Hydroxychloroquine is also used widely throughout at least equatorial regions of Africa as a prophylactic against parasites, but which fortunately has now been studied extensively and used successfully as both prevention and treatment of COVID disease, and as inhibitor of SARS-CoV-2 replication and activity. This is shown in over 380 studies conducted in 55 countries. [17]
Africa leads again
This is not the first piece of evidence that Africa is leading the world away from a microbial-pretext tyranny. Last summer, Africa stood alone in being the continent, led by Botswana, to pull the worlds’ people back from the precipice, while pushing the World Health Organization (WHO) back from their attempted tyranny over all world governments. [18] This danger is by no means past, and new efforts for WHO dominance over the world are ominously re-grouping at this time. [19]Africa led the way and inspires the world. Are the politicians and “public health experts” of the rest of the world humble enough to admit their grotesque errors, even crimes, and to learn from the peoples of the African nations, their experiences and lessons on handling a pandemic?
Or will ethnocentrism or a hostile and racist pride, or the sheer greed stimulated by the lucrative COVIDmania boondoggle, prevent the rest of the world’s willingness to learn from the African experience? Will such provincial and purchased attitudes bury the 21st century’s most important lesson to date?
[1] Johns Hopkins University. Our world in data. Jan 15 2023 update. Coronavirus (COVID-19) Vaccinations
[2] Johns Hopkins University. Coronavirus Resource Center. COVID-19 Map - Johns Hopkins Coronavirus Resource Center
[3] G de Becker. Seeing is believing: What the data reveal about deaths following COVID vaccine rollouts around the world. Jan 9 2023. The Defender. Seeing Is Believing: What the Data Reveal About Deaths Following COVID Vaccine Rollouts Around the World
[4] Johns Hopkins University. Coronavirus Resource Center. See the latest data in your region - Johns Hopkins Coronavirus Resource Center
[5] G Briand. COVID-19 deaths: A look at US data. Mar 18, 2021. PDMJ: Primary Doctor Medical Journal
[6] K Mullis, interviewed. Every scary thing you’re being told depends on the unreliable PCR test. English Rose. Bitchute video. Every Scary Thing You're Being Told, Depends On the Unreliable PCR Test | English Rose
[7] A Mandavilli. Your coronavirus test is positive. Maybe it shouldn’t be. New York Times. Aug 29, 2020. https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
[8] C Huber, B Borovoy. Data that disprove the COVID-19 pandemic. Dec 19, 2020. PDMJ. PDMJ: Primary Doctor Medical Journal
[9] M Rogers. USA Today. Fact check: Hospitals get paid more if patients listed as COVID-19, on ventilators. Apr 24 2020. Fact check: Hospitals get paid more if patients listed as COVID-19, on ventilators
[10] American Hospital Association. Special Bulletin: Senate passes the Coronavirus Aid, Relief and Economic Security Act. Special Bulletin: Senate Passes the Coronavirus Aid, Relief, and Economic Security (CARES) Act | AHA
[11] S Begley. With ventilators running out, doctors say the machines are overused for COVID-19. STAT. Apr 8 2020. With ventilators running out, doctors say the machines are overused for Covid-19
[12] C Huber, B Borovoy. Data that disprove the COVID-19 pandemic. Dec 19, 2020. PDMJ. PDMJ: Primary Doctor Medical Journal
[13] Worldometer. World population. World Population Clock: 8 Billion People (LIVE, 2023) - Worldometer
[14] M Turkia. A timeline of ivermecting-related events in the COVID-19 pandemic [preprint]. Mar 2021. https://www.researchgate.net/public...Events_in_the_COVID-19_Pandemic_March_24_2021
[15] L Clay, J Druce, et al. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Jun 2020. Antiviral Res. https://www.sciencedirect.com/science/article/pii/S0166354220302011?via=ihub
[16] C Huber. Ivermectin is safe and effective: the evidence. Sep 9 2021.
The Defeat Of COVID
Ivermectin is safe and effective: The evidence
Ivermectin is on the World Health Organization (WHO) List of Essential Medicines and is approved by the US Food and Drug Administration (FDA). This well-tolerated but potent anti-parasitic medicine has been prescribed billions of times in its 36-year history against a wide range of parasites. It is a drug in the avermectin family, so named because thos…
Read more
a year ago · 46 likes · 28 comments · Colleen Huber NMD
[17] Science Direct. COVID-19 treatment studies for hydroxychloroquine. Updated Jan 15 2023. https://www.sciencedirect.com/science/article/pii/S0166354220302011
[18] C Huber. Thank you x 3, Africa. Jun 4 2022.
The Defeat Of COVID
Thank you x 3, Africa!
Last week in Davos, the 47 African countries – almost the entire 54-country African continent - were unified at the WHO meeting, led by Botswana, as seen in the video linked below. These 47 countries that are members of the World Health Organization (WHO) were joined by a number of other large and small countries across the globe, in registering a tac…
Read more
7 months ago · 124 likes · 57 comments · Colleen Huber NMD
Thank you x 3, Africa!
[19] J Roguski. 100 reasons. Jan 5 2023.
James Roguski
100 Reasons
Please watch the video or listen to the audio and follow along with the transcript below…
Read more
10 days ago · 220 likes · 31 comments
naegling62
Veteran Member

Heliobas Disciple
TB Fanatic
Senator Cruz needs to work on this too while he's at it:

 www.foxnews.com
(fair use applies)
www.foxnews.com
(fair use applies)
Service members forced to pay back signing bonuses after being fired over COVID vax: ‘Kick in the face’
Troops say mental health impacted by military's treatment
Kelly Laco
January 24, 2023 5:00am EST
U.S. service members who were fired for refusing to comply with the Pentagon's COVID-19 vaccine mandate are now being forced to pay back their original recruitment bonuses, which they tell Fox News Digital is a "kick in the face" after years of dedicating their lives to protecting the country.
One former Army soldier who was fired for refusing to get the COVID-19 vaccine last May told Fox News Digital that he would have to pay back his original signing bonus upon his termination from the military because he did not complete the commitment in his contract.
The soldier had signed a contract with the Army for six years and received a $7,000 bonus. However, because he fell short of the six years, the military notified him that he owed the government a prorated amount of slightly over $4,000. In order to pay it back, he ended up having to "sell" 60 of his unused vacation days to cover the amount owed.
He said that effects on his mental health have been extremely negative because the way he was treated by the military was a "final kick in the face."
"I've deployed multiple times, and I feel like the last thing I had was selling leave days that I earned and was never able to take due to me being deployed or needing that time to prepare for the training cycle. I was about to enter a new world with no income, and that extra bit would have been a nice buffer in my rainy day fund to keep me afloat until I was able to find new employment," he said.
"The Department of Defense continues to fall short on reestablishing trust for wrongdoings, and this is yet another example of that," another service member told Fox News Digital, who said the recoupment of signing bonuses is the "icing on the cake" of the Pentagon's recent treatment of troops.
"The appalling treatment these individuals endured broke the trust that is owed to our citizens and our volunteers. America’s sons and daughters," the Army member said in a statement. "Until true efforts are made to establish trust, the recruiting and retention shortfalls will only continue. The individuals who make public statements that they are unsure what has contributed to the current recruiting and retention shortfalls need to take a look in the mirror; and perhaps they should resign for the betterment of our Nation."
The push by the Pentagon to recoup signing bonuses from fired service members comes after President Biden signed the fiscal year 2023 National Defense Authorization Act, which included a provision, cleared by the House and the Senate, to repeal the administration's military vaccine mandate. This month, Secretary of Defense Lloyd Austin signed a memo that will update the records and remove letters of reprimand from troops whose exemption requests to the vaccine were denied.
Lawmakers are pressuring the Pentagon to do more and provide back pay for the roughly 8,400 U.S. troops fired after refusing to get the COVID-19 vaccine. However, the Pentagon has said back pay for troops fired for refusing the COVID-19 vaccine is not an issue the DOD is "pursuing."
Reinstatement is a priority for some Republicans who have said the strict mandate is one reason why military recruitment is at a "record low."
A spokesperson for the Pentagon did not respond to Fox News Digital's request for comment. An Army spokesperson referred the inquiry to the Pentagon.
Service members forced to pay back signing bonuses after being fired over COVID vax: ‘Kick in the face’
Unvaccinated service members fired for failing to comply with the Pentagon's vaccine mandate are being forced to pay the government thousands to recoup their original signing bonuses.
www.foxnews.com
Service members forced to pay back signing bonuses after being fired over COVID vax: ‘Kick in the face’
Troops say mental health impacted by military's treatment
Kelly Laco
January 24, 2023 5:00am EST
U.S. service members who were fired for refusing to comply with the Pentagon's COVID-19 vaccine mandate are now being forced to pay back their original recruitment bonuses, which they tell Fox News Digital is a "kick in the face" after years of dedicating their lives to protecting the country.
One former Army soldier who was fired for refusing to get the COVID-19 vaccine last May told Fox News Digital that he would have to pay back his original signing bonus upon his termination from the military because he did not complete the commitment in his contract.
The soldier had signed a contract with the Army for six years and received a $7,000 bonus. However, because he fell short of the six years, the military notified him that he owed the government a prorated amount of slightly over $4,000. In order to pay it back, he ended up having to "sell" 60 of his unused vacation days to cover the amount owed.
He said that effects on his mental health have been extremely negative because the way he was treated by the military was a "final kick in the face."
"I've deployed multiple times, and I feel like the last thing I had was selling leave days that I earned and was never able to take due to me being deployed or needing that time to prepare for the training cycle. I was about to enter a new world with no income, and that extra bit would have been a nice buffer in my rainy day fund to keep me afloat until I was able to find new employment," he said.
"The Department of Defense continues to fall short on reestablishing trust for wrongdoings, and this is yet another example of that," another service member told Fox News Digital, who said the recoupment of signing bonuses is the "icing on the cake" of the Pentagon's recent treatment of troops.
"The appalling treatment these individuals endured broke the trust that is owed to our citizens and our volunteers. America’s sons and daughters," the Army member said in a statement. "Until true efforts are made to establish trust, the recruiting and retention shortfalls will only continue. The individuals who make public statements that they are unsure what has contributed to the current recruiting and retention shortfalls need to take a look in the mirror; and perhaps they should resign for the betterment of our Nation."
The push by the Pentagon to recoup signing bonuses from fired service members comes after President Biden signed the fiscal year 2023 National Defense Authorization Act, which included a provision, cleared by the House and the Senate, to repeal the administration's military vaccine mandate. This month, Secretary of Defense Lloyd Austin signed a memo that will update the records and remove letters of reprimand from troops whose exemption requests to the vaccine were denied.
Lawmakers are pressuring the Pentagon to do more and provide back pay for the roughly 8,400 U.S. troops fired after refusing to get the COVID-19 vaccine. However, the Pentagon has said back pay for troops fired for refusing the COVID-19 vaccine is not an issue the DOD is "pursuing."
Reinstatement is a priority for some Republicans who have said the strict mandate is one reason why military recruitment is at a "record low."
A spokesperson for the Pentagon did not respond to Fox News Digital's request for comment. An Army spokesperson referred the inquiry to the Pentagon.
Heliobas Disciple
TB Fanatic

Bill Gates warns Australia next pandemic could be man-made and brutal
Mr Gates told the Lowy Institute think tank in Sydney on Monday that political leaders needed to set aside their differences and work together to prepare for the next virus.
Bill Gates warns Australia to prepare for the next pandemic - which could be man-made and far more brutal than Covid
By Aidan Wondracz For Daily Mail Australia and Australian Associated Press
Published: 18:23 EST, 23 January 2023 | Updated: 18:35 EST, 23 January 2023
- Bill Gates warned Australia to prepare for pandemic
- Tech billionaire said next one could be man-made
Mr Gates told the Lowy Institute think tank in Sydney on Monday that political leaders needed to set aside their differences and work together to prepare for the next virus.
He called for greater global cooperation using the Covid-19 pandemic as an example of how countries could improve on their response if they worked together.
'Compare the economic cost of being prepared for the next one to the cost of this one, over $US10trillion economic loss,' he said.
'With the pandemic we were foolish not to have the tools, the practice and global capacity to be on standby like we do with fire or earthquakes.'
Mr Gates praised Australia's policies in helping to keep infection rates low before vaccines were rolled out.
'Some of the things that stand out are that Australia and about seven other countries did population scale diagnostics early on and had quarantine policies,' he said.
'That meant you kept the level of infection low in that first year when there were no vaccines.'
The Microsoft founder turned philanthropist said a stable international order based on mutual political will is needed in order to deal with future pandemics.
'The one thing that still hangs in the balance is will we have the global capacity and at the regional and country levels that would mean that when an (infectious disease) threat comes up we act in such a way that it doesn't go global,' Mr Gates said.
'We need to be doing every five years a comprehensive exercise at both country and regional levels of pandemic preparedness and you need a global group that's scoring everybody.'
Mr Gates has promised to donate half of his fortune to good causes and to try and bring equality to the health, energy and education industries.
'There is this huge failure of market capitalism to look at some of the needs of the poorest. Their voice in the marketplace is very small,' he said.
'You can literally save lives for $US1,000 and there isn't much around that should be as fulfilling as that.'
He criticised the United States under Donald Trump's leadership threatening to withdraw from the World Health Organisation and withholding funding.
Mr Gates advocated for a bolstering of resources to the international health body.
He also said US policy, and by extension Australia's, towards China needed a more conciliatory and cooperative political approach in tackling major problems such as climate change.
'I see China's rise as a huge win for the world ... the current mentality of the US to China, and which is reciprocated, is kind of a lose-lose mentality'.
'That could be very self-fulfilling in a very negative way'.
Mr Gates on Saturday met with Prime Minister Anthony Albanese at Kirribilli House in Sydney to discuss climate change, health and energy challenges.
Zoner
Veteran Member
I didn't see this 2nd warning that Geert sent to the WHO posted on December 24th. It's an important read imho.
View: https://twitter.com/RobertB63886025/status/1618242994808946689?s=20&t=V6VmN4x6mTZ6bM2aXUtaGA
View: https://twitter.com/RobertB63886025/status/1618242994808946689?s=20&t=V6VmN4x6mTZ6bM2aXUtaGA
psychgirl
Has No Life - Lives on TB
Think anyone will listen to him?I didn't see this 2nd warning that Geert sent to the WHO posted on December 24th. It's an important read imho.
View: https://twitter.com/RobertB63886025/status/1618242994808946689?s=20&t=V6VmN4x6mTZ6bM2aXUtaGA

I think it’s too late anyway.
alpha
Veteran Member
Latest News, Events, and Happenings from the FLCCC
| ||||||
|
Zoner
Veteran Member
Right!? He tried...Think anyone will listen to him?
I think it’s too late anyway.
Zoner
Veteran Member
Ed Dowd is a very smart man.
Latest News, Events, and Happenings from the FLCCC
The Epidemic of Sudden Death
Ed Dowd, an investment executive and author of the new book ‘Cause Unknown’, joined Dr. Paul Marik and Dr. Pierre Kory for a gripping discussion on ‘The Epidemic of Sudden Death’ we are witnessing.
The webinar was eye-opening and engrossing. Here’s just one statistical example: Ed and his team did an analysis of the correlation between vaccine uptake and disabilities and found the R-Squared is 0.9. That blew Dr. Kory’s mind.
What does that mean? Watch the update to find out why this correlation is so phenomenal.
Click Here To Watch
Long Story Short
In this episode, Dr. Been looks at clusters of long COVID symptoms (fatigue, cognitive, and respiratory) and how often they seem to occur. The findings are fascinating.
Watch Here
Heliobas Disciple
TB Fanatic
This is really interesting and very relevant. If this is Covid, NK's 'herd immunity' experiment failed. That's not good....

 justthenews.com
(fair use applies)
justthenews.com
(fair use applies)
North Korea orders capital lockdown over 'respiratory' illness
Residents are instructed to check their temperatures four times a day and report the results to a hospital by phone.
By Madeleine Hubbard
Updated: January 25, 2023 - 11:38am
Officials in North Korea reportedly ordered a five-day lockdown for residents of the capital Pyongyang starting Wednesday because of increasing cases of an unspecified respiratory illness.
The Russian embassy posted a notice on Facebook from the North Korean government stating, as translated, that "for 5 days, a special anti-epidemic period has been established" due to an "increase in winter cases of recurrent flu and other respiratory diseases."
The lockdown may be extended by three days, the notice also states.
Residents are instructed to check their temperatures four times a day and report the results to a hospital by phone.
Pyongyang residents appeared to stock up on goods one day before the lockdown, according to South Korea-based NK News.
North Korea did not specify whether the respiratory illness was COVID-19, over which the Communist country declared victory in August. North Korea enacted stringent COVID restrictions in May, when the country reported its first-ever coronavirus case.
North Korea's neighbor, China, experienced an explosion of COVID cases earlier this month after easing lockdown restrictions.
North Korea orders capital lockdown over 'respiratory' illness
Residents are instructed to check their temperatures four times a day and report the results to a hospital by phone.
North Korea orders capital lockdown over 'respiratory' illness
Residents are instructed to check their temperatures four times a day and report the results to a hospital by phone.
By Madeleine Hubbard
Updated: January 25, 2023 - 11:38am
Officials in North Korea reportedly ordered a five-day lockdown for residents of the capital Pyongyang starting Wednesday because of increasing cases of an unspecified respiratory illness.
The Russian embassy posted a notice on Facebook from the North Korean government stating, as translated, that "for 5 days, a special anti-epidemic period has been established" due to an "increase in winter cases of recurrent flu and other respiratory diseases."
The lockdown may be extended by three days, the notice also states.
Residents are instructed to check their temperatures four times a day and report the results to a hospital by phone.
Pyongyang residents appeared to stock up on goods one day before the lockdown, according to South Korea-based NK News.
North Korea did not specify whether the respiratory illness was COVID-19, over which the Communist country declared victory in August. North Korea enacted stringent COVID restrictions in May, when the country reported its first-ever coronavirus case.
North Korea's neighbor, China, experienced an explosion of COVID cases earlier this month after easing lockdown restrictions.
Heliobas Disciple
TB Fanatic
COVID Toll: Big Jump in Cardiovascular-Related Deaths Reported by American Heart Association
American Heart Association 2023 Statistical Update reports the largest increase in the number of CVD deaths in the U.S. in years, highest among Asian, Black, and Hispanic populations. More people died from cardiovascular-related causes in 2020, the first year of the COVID-19 pandemic, than in a
scitechdaily.com
COVID Toll: Big Jump in Cardiovascular-Related Deaths Reported by American Heart Association
By American Heart Association
January 25, 2023
The number of deaths from cardiovascular disease in the US increased during the first year of the COVID-19 pandemic, from 874,613 in 2019 to 928,741 in 2020. This represents the largest single-year increase since 2015 and is higher than the previous record of 910,000 in 2003, according to the Heart Disease and Stroke Statistics — 2023 Update of the American Heart Association.
American Heart Association 2023 Statistical Update reports the largest increase in the number of CVD deaths in the U.S. in years, highest among Asian, Black, and Hispanic populations.
- More people died from cardiovascular-related causes in 2020, the first year of the COVID-19 pandemic, than in any year since 2003, according to data reported in the American Heart Association’s 2023 Statistical Update.
- The largest increases in deaths were seen among Asian, Black, and Hispanic people.
- While the pandemic’s effects on death rates may be noticed for several years, lessons learned offer major opportunities to address structural and societal issues that drive health disparities, according to Association leaders.
During the first year of the COVID-19 pandemic, the number of people dying from cardiovascular disease (CVD) in the U.S. escalated from 874,613 CVD-related deaths recorded in 2019 to 928,741 in 2020. The rise in the number of CVD deaths in 2020 represents the largest single-year increase since 2015 and topped the previous high of 910,000 recorded in 2003, according to the latest available data from the Heart Disease and Stroke Statistics — 2023 Update of the American Heart Association, a global force for healthier lives for all, and published today in the Association’s flagship, peer-reviewed journal Circulation.
While the total number of CVD-related deaths increased from 2019 to 2020, what may be even more telling is that our age-adjusted mortality rate increased for the first time in many years and by a fairly substantial 4.6%,” said the volunteer chair of the Statistical Update writing group Connie W. Tsao, M.D., M.P.H., FAHA, an assistant professor of medicine at Harvard Medical School and attending staff cardiologist at Beth Israel Deaconess Medical Center in Boston. “The age-adjusted mortality rate takes into consideration that the total population may have more older adults from one year to another, in which case you might expect higher rates of death among older people. So even though our total number of deaths have been slowly increasing over the past decade, we have seen a decline each year in our age-adjusted rates – until 2020. I think that is very indicative of what has been going on within our country – and the world – in light of people of all ages being impacted by the COVID-19 pandemic, especially before vaccines were available to slow the spread.”
The biggest increases in the overall number of CVD-related deaths were seen among Asian, Black, and Hispanic people, populations most impacted in the early days of the pandemic, and brought to focus increasing structural and societal disparities.
“We know that COVID-19 took a tremendous toll, and preliminary data from the U.S. Centers for Disease Control and Prevention (CDC) have shown that there was a substantial increase in the loss of lives from all causes since the start of the pandemic. That this likely translated to an increase in overall cardiovascular deaths, while disheartening, is not surprising. In fact, the Association predicted this trend, which is now official,” said the American Heart Association’s volunteer president, Michelle A. Albert, M.D., M.P.H., FAHA, the Walter A. Haas-Lucie Stern Endowed Chair in Cardiology, a professor of medicine at the University of California at San Francisco (UCSF) and Admissions Dean for UCSF Medical School. “COVID-19 has both direct and indirect impacts on cardiovascular health. As we learned, the virus is associated with new clotting and inflammation. We also know that many people who had new or existing heart disease and stroke symptoms were reluctant to seek medical care, particularly in the early days of the pandemic. This resulted in people presenting with more advanced stages of cardiovascular conditions and needing more acute or urgent treatment for what may have been manageable chronic conditions. And, sadly, appears to have cost many their lives.”
According to Albert, who also is the director of the CeNter for the StUdy of AdveRsiTy and CardiovascUlaR DiseasE (NURTURE Center) at UCSF and a renowned leader in health equity and adversity research, the larger increases in the number of coronary heart disease deaths among adults of Asian, Black, and Hispanic populations appear to correlate with the people most often infected with COVID-19.
“People from communities of color were among those more highly impacted, especially early on, often due to a disproportionate burden of cardiovascular risk factors such as hypertension and obesity. Additionally, there are socioeconomic considerations, as well as the ongoing impact of structural racism on multiple factors including limiting the ability to access quality health care,” Albert said. “The American Heart Association responded quickly at the beginning of the pandemic to address the impact of COVID-19 and focus on equitable health for all. The Association launched the first-ever rapid response research grants calling on the research community to quickly turn around transformative science; established a COVID-19 CVD hospital registry through the Get With The Guidelines® quality initiative; and also made an unprecedented pledge to aggressively address social determinants while working to support and improve the equitable health of all communities. We are empowering real change that will save lives.”
Cardiovascular disease, overall, includes coronary heart disease, stroke, heart failure, and hypertension/high blood pressure. Coronary heart disease includes clogged arteries or atherosclerosis of the heart, which can cause a heart attack. Known generally as ‘heart disease’, coronary heart disease remains the #1 cause of death in the U.S. Stroke continues to rank fifth among all causes of death behind heart disease, cancer, COVID-19 and unintentional injuries/accidents. COVID-19 appeared in the list of leading causes of death for the first time in 2020, the most recent year for which final statistics are available from the U.S. Centers for Disease Control and Prevention (CDC).
Appropriately, this year’s statistical update includes many references to COVID-19 and its impact on cardiovascular disease. Data points and scientific research findings are inserted throughout most chapters of the document, including those related to the risk factors for heart disease and stroke such as obesity, diabetes and high blood pressure, all of which also put people at increased risk for COVID. Many of the studies noted identify specific gender, race and ethnicity disparities.
However, disparities don’t only occur among age, sex and racial/ethnic groups, according to a special commentary authored by members of the Statistical Update writing committee. While the Statistical Update has been including various social determinants of health data in its report, the commentary noted that data from other underrepresented populations, such as LGBTQ people and people living in rural vs. urban areas of the U.S. are still lacking. The commentary authors call out the lack of scientific research and cumulative data on the impacts of social identity and social determinants.
“We know that to address discrimination and disparities that impact health, we must better recognize and understand the unique experiences of individuals and populations. This year’s writing group made a concerted effort to gather information on specific social factors related to health risk and outcomes, including sexual orientation, gender identity, urbanization, and socioeconomic position,” Tsao said. “However, the data are lacking because these communities are grossly underrepresented in clinical and epidemiological research. We are hopeful that this gap in literature will be filled in coming years as it will be critical to the American Heart Association’s goal to achieve cardiovascular health equity for all in the U.S. and globally.”
Global data
Cardiovascular disease continues to be the #1 killer globally, taking the lives of more than 19 million people around the world each year, including people of all ages, genders and nationalities. Yet, the risk factors that lead to heart disease and stroke continue to disproportionately impact certain populations in the U.S. as well as around the world.
Supplemental tables in this year’s statistical update look at the trend of overall CVD-related deaths globally and regionally, and also provide the number and proportion of deaths caused by various cardiovascular diagnoses. Additionally, the supplemental tables compared all-cause deaths and CVD-related deaths attributable to various risk factors, as well as age-standardized disability-adjusted life years, or DALYs, in various countries and regions. Of special note:
- Globally, ischemic heart disease and stroke represent the top two causes of CVD-related deaths and account for 16.2% and 11.6% of all causes of deaths, respectively. These rates have increased across the world over the past decade in all but two regions – North America and Europe/Central Asia. Note that ischemic heart disease is the term used in global data sources and is also known as coronary heart disease.
- In 1990, ischemic heart disease represented 28.2% of all deaths in North America, dropping to 18.7% of all deaths in 2019. Stroke dropped from 7.3% of all deaths in North America in 1990 to 6.4% of all deaths in 2019.
- In the region of Europe and Central Asia, ischemic heart disease dropped from 27.2% of all causes of death in 1990 to 24.4% in 2019, while stroke represented 15.1% of all causes of death in 1990 and dropped to 12.5% in 2019.
- The region of East Asia and Pacific is the only region where stroke represents the highest proportion of CVD-related deaths, with the proportion of deaths increasing from 14.8% in 1990 to 18.3% in 2019. During this same time period, the proportion of deaths caused by ischemic heart disease nearly doubled from 8.1% to 15.6%.
- The region of Sub-Saharan Africa noted the lowest proportion of CVD-related deaths as a percentage of all causes of death. Stroke was the leading cause of CVD-related deaths in the region of Sub-Saharan Africa in 1990, representing 3.6% of all causes, followed by ischemic heart disease (3.1%). In 2019, ischemic heart disease and stroke were both at 5.4% of total deaths.
Reference: “Heart disease and stroke statistics—2023 update: A report from the American Heart Association” 25 January 2023, Circulation.
DOI: 10.1161/CIR.0000000000001123
The annual update represents a compilation of the newest, most relevant statistics on heart disease, stroke, and risk factors impacting cardiovascular health. It tracks trends related to ideal cardiovascular health, social determinants of health, global cardiovascular health, cardiovascular health genetics, and health care costs. Tsao emphasized the importance of this surveillance as a critical resource for the lay public, policymakers, media professionals, clinicians, healthcare administrators, researchers, health advocates, and others seeking the best available data on these factors and conditions.
This statistical update was prepared by a volunteer writing group on behalf of the American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee.
Heliobas Disciple
TB Fanatic

Did China Make a Mistake by Ending COVID Restrictions?
Commentary Never forget that the New York Times kicked off disease panic in the United States in late ...
www.theepochtimes.com
Did China Make a Mistake by Ending COVID Restrictions?
Jeffrey A. Tucker
January 25, 2023
Commentary
Never forget that the New York Times kicked off disease panic in the United States in late February 2020, about a month after China had locked down Wuhan and violated its citizens’ rights to associate on a massive scale. Two weeks earlier, the World Health Organization sponsored a Western junket that was attended by Fauci’s deputy assistant and others. They came back and declared that lockdowns are great and should be adopted by all governments.
The first media outlet in the United States to amplify this China communist propaganda was the New York Times. On Feb. 27, 2020, Donald G. McNeil, the lead virus reporter who was later fired for unrelated reasons, predicted mass death from this virus unless the United States locks down just like China.
The next day, the newspaper published his op-ed arguing for the “medieval” method of virus control. On the same day, the paper ran an article by Peter Dazsak, head of EcoHealth Analysis, which was Fauci’s third-party funding choice to get cash to the Wuhan Institute of Virology for gain-of-function research.
This is a grim history, and one might suppose the newspaper would have moved on. But no! Just yesterday, the same paper ran a piece by Michael V. Callahan, an infectious disease specialist who has been working in China and Southeast Asia for ten years. Listen to what he actually typed:
“China rolled back its longstanding pandemic strategy ‘zero Covid,’ which had protected the country for nearly three years, in early December. This reversal came after historic public protests calling for an ease in restrictions …. The timing could not have been worse.”
Can you even imagine such a thing appearing in any paper, much less the New York Times? We are really being told that this grotesque experiment in mega-totalitarianism that treated the entire population like lab rats was really a successful effort that “protected the country.”
Protected the country! In other words, what we have here is an ongoing effort by the top organ of the mainstream press continuing to shill for the Chinese Communist Party (CCP). It’s astonishing really, and not only because it is utterly inhumane. It is also a fact that China’s lockdown did not protect the country. What it did was weaken immune systems and make China more vulnerable than ever.
Pretending for a moment that Xi Jinping’s policies were not just a grotesque push for massive power, it was never clear what the exit strategy for zero COVID was supposed to be. Stay locked down forever, as in some dystopian movie? And then what happens on the first exposure to anything? We know from history. Half the native population in the United States died from disease when exposed to colonial travelers. It’s happened to countless native tribes around the world. This is an extremely bad idea, and it is a wonder that a supposed civilized country could ever consider such a thing, and yet most countries in the world did.
Xi actually seemed to believe that he could make a virus go away by muscling his people with enough force and intimidation. It’s arrogance for the ages. But the New York Times was all for it—was and still is!
What is it that Dr. Callahan desires now? He wants the United States to help out this poor country that mistakenly allowed its countrymen to have a modicum of freedom back. His great idea is to export “successful strategies from the United States’ Operation Warp Speed playbook, which accelerated the delivery of mRNA vaccines from the manufacturer into people’s arms. This huge logistical challenge can be revised for the rapid deployment of a new Chinese-made mRNA vaccine.”
What to say to this idea? The CCP is evil but not crazy.
In any case, it appears that China, even after three years of lockdown crazy, is going to deal with this virus the old-fashioned way: get it and shake it off. China’s epidemiologists are now saying that upwards of 80 percent of the population has already been exposed and thus acquired some level of protection. This is how it works: exposure and then protection. It’s what should have happened three years ago. This is how the entire planet will deal with COVID. It adds one more coronavirus to the four that are already endemic.
Let’s turn to Dr. Callahan himself. Why exactly is he the one to author an article urging the United States to work with China to get mRNA shots into billions of arms? Well, the scientist Robert Malone explains his own contact with this man, who might have been responsible for among the first communications from China to the U.S. that warned of a coming virus.
Dr. Malone writes:
“on approximately 04 January 2020 I received an unexpected phone call from Dr. Michael Callahan (known to me to have been a CIA agent, and separately confirmed to me by NY Times reporter Davey Alba in February 2022 as a ‘former’ CIA agent). During this call, Dr. Callahan revealed to me that he was calling from China, and that he was in the country under cover of his Harvard Professor appointment. Further information regarding Dr. Callahan can be found in this article by Raul Diego, with research support by Whitney Webb, entitled ‘DARPA’s Man in Wuhan.’ It is important to know that Callahan has provided advice in the White House to at least three US Presidents, including Obama and Trump. On 04 January 2020, Dr. Callahan told me that there was a novel coronavirus circulating in the Wuhan region, it was looking like a significant biothreat, and I should get ‘my team’ engaged in seeking ways to mitigate the risk of this new agent.”
Malone explains further and more deeply how he comes to the following conclusion concerning Callahan:
“Based on this timeline and history, as well as my own direct personal communication with Dr. Callahan, I strongly suspect that both the gross clinical mismanagement of ventilatory support during the first phase of the outbreak (responsible for up to 30,000 deaths) as well as the stunningly poor management practices of Nursing Home and Extended Care facilities throughout the USA can be directly traced to the influence of Dr. Michael Callahan, DARPA’s Man in Wuhan and arguably the top U.S. Government/CIA expert in both biowarfare and gain of function research.”
If this is the case, let’s just say there are many unquestioned questions, including how it comes to be that Callahan raided the pages of the New York Times only yesterday to praise the CCP’s handling of the virus, adding only that China needs to work with the United States to mass vaccinate its population, even though that strategy has worked nowhere in the world and in fact only prolonged the pandemic and increased infections.
But these days, it seems like facts do not matter anymore, at least not at the New York Times, which has been shilling for the virus police here and abroad for fully three years.
A final fascinating note. Dr. Callahan has written exactly one previous piece for the New York Times, on June 10, 2021. In this article, he is pushing for a “kill shot” for all variants of COVID, which he swears is possible provided the United States collaborates with labs around the world. Then he throws in this little barb at Trump:
“Unfortunately, the changes in U.S. political leadership in 2016 as well as budget changes led to the demise of research collaborations in nine countries, including China, Russia, Indonesia and Nigeria. The Biden administration’s re-engagement in global health signals an opportunity to restart Prophecy or a similar program.”
If Malone is correct that Callahan is CIA, this little observation on his part suggests a thing or two about what might ultimately be the underlying politics of the COVID response in the first place: it was always in part an effort to oust the president.
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times.
Tristan
Has No Life - Lives on TB
Dr. Campbell's update on Excess Mortality in the 'Advanced' Countries:
View: https://www.youtube.com/watch?v=av4Ej6om0WI
rt: 16:21
Summary: It don't look good, and it might be getting worse.
rt: 16:21
Summary: It don't look good, and it might be getting worse.
Heliobas Disciple
TB Fanatic
'Extremely disconcerting': NIH didn't track U.S. funds going to Chinese virus research, watchdog finds
The National Institutes of Health failed to provide adequate oversight of an American organization that funded controversial research at the Wuhan Institute of Virology in China, a new government report says.
'Extremely disconcerting': NIH didn't track U.S. funds going to Chinese virus research, watchdog finds
Alexander Nazaryan·Senior White House Correspondent
Thu, January 26, 2023, 7:48 PM EST
The National Institutes of Health failed to provide adequate oversight of an American organization that funded controversial research at the Wuhan Institute of Virology in China, according to a new government report that is sure to raise new questions about the origins of the COVID-19 pandemic.
The report is evidence of “major failures in past NIH oversight of high-risk research on enhanced potential pandemic pathogens,” Rutgers molecular biologist Richard Ebright told Yahoo News in an email.
Issued by the inspector general of the federal Department of Health and Human Services, the new report says nothing about the origins of the coronavirus. For the most part, it concerns research that took place well before the first cases of what came to be known as SARS-CoV-2 were discovered in China in late 2019.
But it does note that the American organization in question, the EcoHealth Alliance, should have been more rigorously scrutinized by federal officials regarding assurances that its partner lab in Wuhan was not using U.S. funds to conduct gain-of-function research, which boosts viruses to study how they might evolve in nature.
“The entire picture starts to look extremely disconcerting,” mathematical biologist Alex Washburne told Yahoo News. He said that a project on coronaviruses originating in bats, for which the EcoHealth Alliance had given a grant to the Wuhan Institute of Virology, “was clearly gain-of-function research.”
Republicans seized on the findings, with Sen. Rand Paul of Kentucky — a skeptic of virtually every aspect of the official coronavirus narrative — charging that the NIH “failed to conduct adequate oversight.”
China hawks will also be emboldened, accusing President Biden of not being forceful enough with the East Asian superpower.
But it is the NIH that is bound to face the most intense scrutiny. In a Twitter message, House Republicans promised that “oversight & accountability” are coming to the federal biomedical establishment, which has been celebrated by some but demonized by others.
The new report is likely to feature prominently in hearings they plan to hold.
Politics aside, Wednesday’s report raises important questions about how federal funds are monitored when they flow to foreign governments and organizations. Though the context is different, similar questions have been asked about the billions of dollars in U.S. military and civilian support to Ukraine.
“It’s a damning indictment of N.I.H.,” Georgetown University public health law expert Lawrence Gostin told the New York Times.
The new report examines a series of grants — $8 million total, awarded during both the Obama and Trump administrations — to EcoHealth Alliance, a New York-based nonprofit that subsequently sent a total of $598,611 to the Wuhan virology lab between 2015 and 2019.
The HHS inspector general, Christi Grimm, found that the “NIH did not effectively monitor or take timely action to address EcoHealth’s compliance with some requirements” to report research being conducted in Wuhan with U.S. funds.
“Deficiencies in complying with those procedures limited NIH and EcoHealth’s ability to effectively monitor Federal grant awards and subawards to understand the nature of the research conducted, identify potential problem areas, and take corrective action,” Grimm concluded.
The NIH “raised concerns” about some of the research EcoHealth was funding in China but ultimately did not put a halt to any of the work, Grimm wrote in her 64-page report. Crucially, EcoHealth failed to produce a progress report about its subgrants in the summer of 2019, just months before the advent of the coronavirus.
Despite these concerns, EcoHealth continues to work with the federal government; the organization was recently the recipient of $3 million from the Department of Defense to study viruses in the Philippines.
In a statement, EcoHealth said it “welcomes” the inspector general’s “oversight and collaborated fully and transparently with this audit.” The organization also provided point-by-point responses to the inspector general’s findings that defended its work in China.
Since the first months of the pandemic, EcoHealth Alliance has been at the center of both legitimate and conspiratorial inquiries into how, and where, the coronavirus originated. Although it was originally thought that the virus originated at a wildlife market, no explanation has been sufficiently convincing to allow for anything approaching scientific consensus.
One attempted explanation is the so-called lab leak theory, which claims that the virus escaped from a laboratory — with the Wuhan Institute of Virology being the most likely candidate — into the general population. The hypothesis was initially dismissed as a conspiracy theory but has since been acknowledged as plausible by many experts.
Evidence, however, remains circumstantial, and most scientists subscribe to a model of pathogenesis involving an animal-to-person “spillover.” Ebola and HIV took the same route to becoming infectious diseases in the human population.
Wednesday’s report could invigorate investigators who continue to believe that China is hiding crucial evidence, including about a potential accident.
When the pandemic began, EcoHealth president Peter Daszak argued that criticizing the zoonotic spillover hypothesis — that is, the notion that the coronavirus came from an animal, possibly one sold at a wildlife market — would only stoke xenophobia.
Daszak compelled members of the scientific community to sign a letter, published in February 2020 in the Lancet — one of the world’s most esteemed medical journals — criticizing the suggestion that a laboratory accident (a not-uncommon occurrence in either China or the West) could have been involved.
“We stand together to strongly condemn conspiracy theories suggesting that COVID-19 does not have a natural origin,” the letter said. “Conspiracy theories do nothing but create fear, rumours, and prejudice that jeopardise our global collaboration in the fight against this virus.”
But after the extent of EcoHealth Alliance’s work in China became known in 2021, the Lancet had to publish an addendum acknowledging Daszak’s potential conflict of interest in defending China.
The new report comes as House Republicans prepare to probe several aspects of the nation’s pandemic response, including how the virus originated. Among the lawmakers named to the committee is far-right Rep. Marjorie Taylor Greene of Georgia, who has suggested that the coronavirus was the result of a bioweapons experiment. She has accused Dr. Anthony Fauci of complicity in those experiments — of which no evidence exists — and called for his firing as the nation’s top infectious disease expert.
Fauci, who retired at the end of last year, has defended working with Chinese partners. But he has also conceded that much about how the virus came to be remains unknown.
“I have a completely open mind,” he said in November.