Since the rollout of mRNA COVID-19 vaccines, many researchers have speculated on the possibility of transmission of vaccine ...

www.theepochtimes.com
(fair use applies)
New Pre-Print Study Implies Airborne COVID-19 Antibodies Post-Vaccination
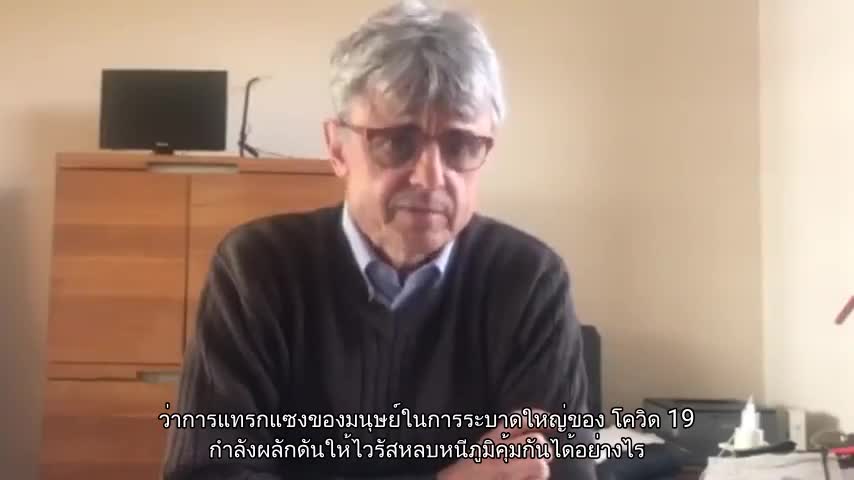
Doctor ventures into controversial issue of COVID 'vaccine shedding'
BY Marina Zhang
September 13, 2022
Since the rollout of mRNA COVID-19 vaccines, many researchers have speculated on the possibility of transmission of vaccine particles from the vaccinated to the unvaccinated, more commonly known as “vaccine shedding.”
Though these speculations are routinely fact-checked, anecdotal stories of unvaccinated people who become infected with COVID-19 or have experienced strange symptoms after contact with friends or family who were vaccinated have persisted.
Several doctors have also speculated about possible transmission as new findings in support of these ideas emerge.
A recent pre-print study has attracted media attention as the results of the study may be interpreted as suggestive of vaccine transmission via shedding.
New Pre-Print Study Implies Airborne Antibodies From Vaccine
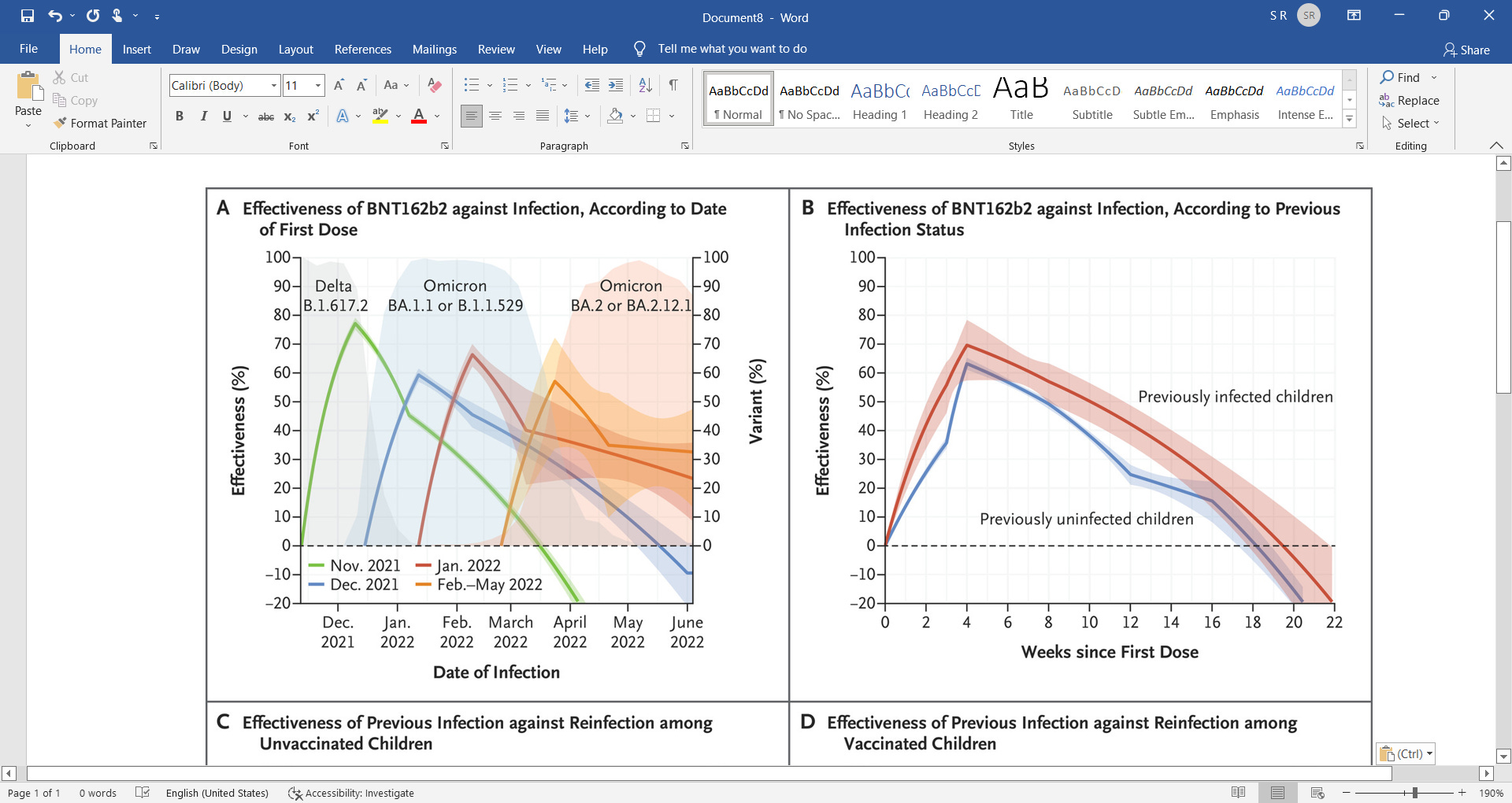
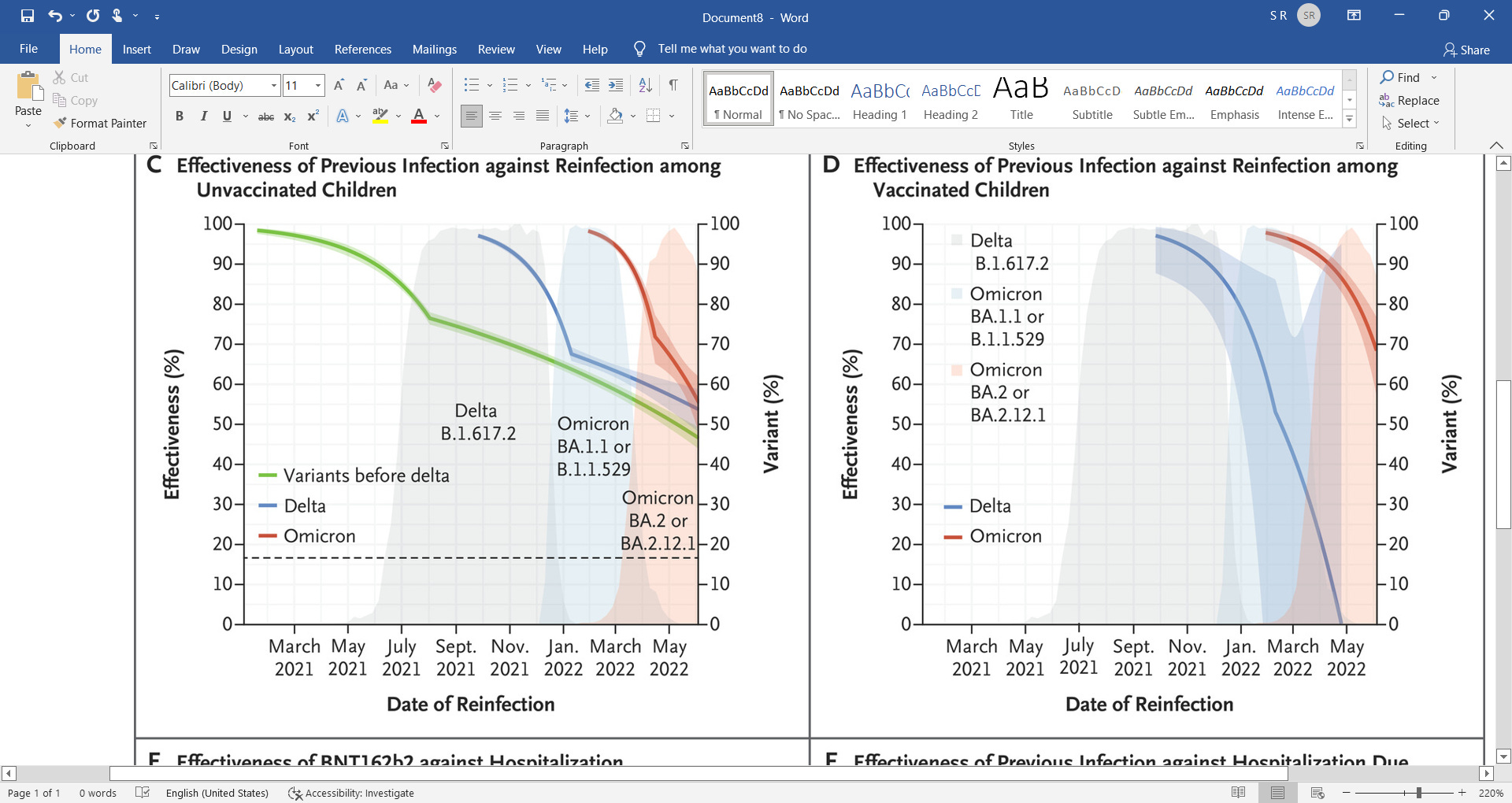
A new pre-print study published by the University of Colorado concluded that antibodies can be transmitted through aerosols.
In the study, unvaccinated children living in either vaccinated or unvaccinated households were nasal swabbed for COVID-19 antibodies.
The authors, led by Dr. Ross Kedl, found that children living with vaccinated parents have higher concentration of COVID-19 antibodies in their swabs than children living in unvaccinated households.
Antibodies are immune markers, and each person’s collection of antibodies is a reflection of immunization and infection history. The presence of each antibody indicates that the person may have been exposed to a particular infection or vaccine the antibody fights against.
Therefore, a person is only supposed to display antibodies to COVID-19 if they have been infected or vaccinated. Yet, these children have not been vaccinated against nor infected with COVID-19. Why do they have antibodies?
The authors of the study reasoned that the vaccinated parents likely passed their antibodies to the children. They produced antibodies from the vaccine, these antibodies accumulated in the nasal cavities and became airborne. Their children then breathed the antibodies in, accumulating COVID-19 antibodies in their nasal cavities.
This is a plausible speculation as it is well documented that bodily fluids including breastmilk, saliva, tears, and sweat contain antibodies. Mothers are also recommended to breastfeed their babies, as it provides their babies with antibodies, protecting them from infection.
Still, though we know that antibodies can be present in bodily fluids, we do not know if antibodies can become airborne.
To support their speculation that antibodies may be airborne, the authors tested face masks from vaccinated individuals and found COVID-19 antibodies on the masks.
The authors argued that since everyone breathes into their masks, the COVID-19 antibodies found on the masks could be evidence that antibodies can be aerosolized, and therefore transmitted to others.
Though, the authors acknowledged that antibodies could have come off from saliva and sweat.
However, internal medicine practitioner and integrative and chelating specialist Dr. Ana Maria Mihalcea questioned the conclusion.
She told The Epoch Times that the study leaves a lot open to interpretation, and the same findings can also be used to support speculations of vaccine shedding.
“[The study] says that the antibodies are being transferred,” she said. “But could it be that the spike protein has been transferred [through contact through skin] and the child has mounted its own antibody response? I don’t think that that’s really clear.”
What Do We Know About Transmission?
Vaccine shedding, dubbed as “transmission” by Dr. Sherri Tenpenny, has remained a controversial topic in the discourse on COVID-19 vaccines as there has yet to be any study that proves or shows conclusive proof of shedding.
One topic of debate is that vaccine shedding may not be the most accurate definition for what clinicians suspect are happening.
Vaccine shedding specifically refers to the spreading of virus and viral particles after vaccination. Viral shedding has been observed with vaccines for oral forms of polio vaccines, rotaviruses, adenoviruses, influenza, and many more.
Shedding only happens for vaccines containing live and attenuated viruses.
After vaccination, viruses can be detected in fecal samples of the vaccinated, and those who come into contact with them may be infected if the shed viral particles are infectious.
However, the mRNA Pfizer and Moderna COVID-19 injections do not use live coronaviruses, rather only the spike protein mRNA is shipped into the cells inside a lipid nanoparticle.
Therefore, they cannot shed viruses, as there is no virus.
J&J and AstraZeneca both use weakened live adenoviruses (not coronavirus) to transport spike protein DNA. However, these viruses have been edited so that they cannot replicate in our cells, therefore, we also should not be able to shed COVID-19 vaccine adenoviruses either.
What about spike proteins then? As mentioned above, there are no studies that provide conclusive proof of spike protein transmission, though health experts are unwilling to rule out the possibility.
Many doctors have spoken up about the possibility of transmission of the particles contained in the COVID-19 injections from vaccinated individuals into the unvaccinated, causing possible symptoms.
Curious Clinical Findings
Though there has been no study that gives proof of transmission, many doctors have observed strange occurrences in unvaccinated individuals after spending time with people who are vaccinated.
“What I’ve seen with unvaccinated individuals who would come into the office with symptoms of things like headaches, feeling unwell, myalgia (meaning muscle aches), and a lot of times women who got in contact with vaccinated people develop hemorrhaging and menstrual irregularities, but very unusual in terms of large clotting and bleeding,” Dr. Mihalcea told The Epoch Times.
She shared a recent case of two unvaccinated menopausal women who started hemorrhaging after sitting together with a recently vaccinated individual for two hours in a car ride.
“The vaccinated person had just gotten their shot a week earlier, and the two unvaccinated women when they got out of the car after a two hour car ride, they both started bleeding.”
Mihalcea cited Pfizer clinical trials as another indication of possible vaccine transmission or shedding.
The Pfizer clinical trials (pdf) listed vaccine exposure during pregnancy (EDP) as an event that needed to be reported and monitored.
Though exposure could occur by participating in the study and getting vaccinated, or getting exposed through a vaccinated male partner through sexual contact, Mihalcea expressed concern at Pfizer’s listing of EDP through “environmental exposure.”
The Pfizer document said that examples of environmental exposure during pregnancy includes, “a female family member or healthcare provider reports that she is pregnant after having been exposed to the study intervention by inhalation or skin contact.”
This means that pregnant women may be exposed to the injection if breathing near or touching someone who was vaccinated.
EDP through environmental exposure would also be counted if, “a male family member or healthcare provider who has been exposed to the study intervention by inhalation or skin contact then exposes his female partner prior to or around the time of conception.”
This statement suggests that someone can be exposed to the vaccine through breathing or skin contact with someone who was vaccinated, and then pass it to someone else.
Findings from peer-reviewed research published in the Gazette of Medical Sciences also seem to be in support of vaccine transmission.
The study, which is based on a survey conducted by My Cycle Story, documented a spike in occurrences of decidual cast shedding and miscarriages in women after COVID-19 vaccines started rolling out.
One poignant testimony (pdf) in the study told of a woman of unknown vaccination status who experienced decidual cast shedding after her husband spent 20 minutes with people who were vaccinated.
Decidual cast shedding is a rare event. Around 40 cases have been documented in the medical literature, and it occurs when the thick mucus lining of the uterus sheds in nearly the exact shape of the inside of the uterus, creating a triangular cast.
This event is so rare that very few studies have been published about it, yet My Cycle Story reported 292 out of 6,092 women surveyed have experienced it following the rollout of COVID-19 vaccines. The study was also supplemented with testimonies from women who previously had successful pregnancies but began to suffer miscarriages after visiting friends and family who were vaccinated.
Though these cases may be a coincidence, Mihalcea’s own observations of unvaccinated patients developing various COVID-associated and strange conditions following contact with someone who was vaccinated made her suspicious that transmission was happening.
At the same time, other findings were also emerging that solidified Mihalcea’s suspicions.
A Canadian doctor, Dr. Charles Hoffe, announced in July 2021, that he found over 60 percent of his vaccinated patients had elevated D-dimer levels, and made his findings into a video.
D-dimer testing is often done to check for blood clots. Though elevated D-dimer levels are not conclusive of blood clots, they definitely indicate that possibility.
Mihalcea started doing her own D-dimer tests on unvaccinated patients who were concerned about vaccine transmission or showing conditions suggestive of possible transmission.
“I started seeing a huge amounts of [unvaccinated] people of all ages who had abnormal D-dimer testing, indicating the possibility for micro clotting,” Mihalcea said.
Mihalcea also published a video explaining elevated D-dimer levels in her patients, suggesting possible transmission from vaccinated to unvaccinated individuals.
She told The Epoch Times that, since the vaccine rollout, she has treated many long COVID patients and cases of suspected transmission. She said that she has treated around 90 to 100 cases of suspected transmission, and brought their levels of D-dimers back down through her treatment regimen.
She has also since bought a microscope with which to analyze her patients’ blood through a prick test, by taking a prick of their blood and examining it under the microscope.
Blood analysis is normally done by pathologists, and many primary care physicians may choose to not analyze their patients’ blood, but Mihalcea, and many other doctors, have decided to investigate themselves.
Her treatment regime involved a series of supplements and pharmaceuticals, namely, ivermectin and hydroxychloroquine, both of which are effective antivirals for the COVID-19 virus. She also prescribes quercetin which reduces inflammation, glutathione has detox effects, blood thinners such as aspirin to prevent blood clotting, and vitamins to boost the immune system including vitamins D and C.
She said she later found vitamin C infusions, and chelating therapies, which remove heavy metals, also improved her patients’ symptoms and brought their D-dimer levels back to normal.
Doctors’ Speculations on What Is Happening
Clinicians do not know how and why unvaccinated people are developing these symptoms; however, many suspect it could be transmission of vaccine particles from the vaccinated to the unvaccinated.
Dr. Sherri Tenpenny said on the JD Rucker podcast that she and many doctors have come to the conclusion that the spike protein, made in human cells from the mRNA and adenovirus COVID-19 vaccines, are what is being transmitted from vaccinated to unvaccinated.
A study on cells in the laboratory has found that after exposure to spike protein DNA, cells derived from human embryonic kidney cells would make the spike proteins and then pack them into cellular sacs called exosomes.
Exosomes have been found in sweat and tears and have been previously studied as an option to impart immunity through skin contact.
Mihalcea said that exosomes could be transmitting spike proteins from infected cells since other studies have found that exosomes can be shed in sweat and tears, and this makes the possibility of transmission through skin contact and aerosols plausible.
Nonetheless, Mihalcea highlighted that since clinicians have no idea what is in the injection vials, if transmission is occurring, there also may be other things being transmitted apart from spike proteins.
Studies have long shown that the quality of vaccine vials can vary between batches.
The same applies to COVID-19 vaccines.
How Bad is My Batch, a website that compiles vaccine adverse event reports from Vaccine Adverse Event Reporting System (VAERS), has shown that the number of adverse effects can drastically vary between different batches of COVID-19 injections.
The website states that 5 percent of the Pfizer batches appear to have produced 90 percent of the Pfizer-associated adverse reactions, and that some batches are associated with 30 times the number of deaths and disabilities compared to other batches.
Mihalcea said that this variability reflects possible differences in injection content, and therefore every patient who reports vaccine transmission may respond differently.
“We cannot respond to this problem of shedding if every vial or every batch is not the same. There are certain batches that have very substantial side effects. That means that different batches don’t shed at all and other batches shed a lot.”
Recent peer-reviewed studies from Germany and Italy found that in mRNA-vaccinated people reporting post-vaccination symptoms, over 90 percent of the vaccinated had metal nanoparticles that resembled graphene oxide in their blood.
Vaccine manufacturers have assured that graphene is not in the COVID-19 vaccinations, and therefore the source of these nanoparticles is unknown.
Blood analyses by Dr. Phillipe Van Waldenberg have also found graphene oxide in the blood of both vaccinated and unvaccinated individuals.
Waldenberg first spotted “tube-like” graphene oxide particles in his vaccinated patients who were reporting symptoms of fatigue, dizziness, memory problems, and even paralysis, and late-onset heavy menstruation in menopausal women.
However, he later found these particles in unvaccinated individuals reporting paralysis symptoms as well.
Graphene oxide nanoparticles are used in biotechnology for cancer treatment and drug delivery. However, the material can be toxic to humans if inhaled, with varying levels of toxicity depending on its dosage, entry method, and pharmacokinetics.
Waldenberg reported his findings on Loving Life TV, speculating that transmission of graphene oxide is occurring between vaccinated and unvaccinated people. He said that one of his patients is an unvaccinated boy who reported paralysis in his limbs after his mother was vaccinated.
Should Unvaccinated Individuals Be Concerned?
If the things Mihalcea and many other doctors are saying are true, then the possibility of transmission poses significant health concerns for the unvaccinated.
Mihalcea recommended the unvaccinated to boost their immune systems through supplements. More importantly, however, she said that everyone should maintain a healthy mindset, including having no fear.
“When people are afraid, their immune system is adversely affected … If you’re depressed or you’re anxious, you actually shorten your telomeres (DNA which prevent aging) which means you’re aging much, much faster, including your immune system. So part of being healthy is also not being afraid.”
Social stress and anxiety have been associated with the shortening of telomeres, which increases aging, including aging of the immune system. Therefore, maintaining health mentally and emotionally is imperative for physical well-being.
To prevent transmission and its symptoms, Mihalcea advised unvaccinated people to boost their immune system by taking supplements such as vitamins C and D.
Nevertheless, Mihalcea said that the extent of transmission and the health symptoms have greatly varied. After treatment, some people’s D-dimers remained low even in contact with vaccinated people, and some people’s D-dimers went back up.
For the people who may be concerned about possible transmission or are experiencing suspected symptoms, “find physicians who are more open-minded,” said Mihalcea.
Some people’s primary care doctors who believe COVID vaccines cannot be the cause of their patients’ concerns may not be able to give suitable advice and support. Therefore Mihalecea advised people to find doctors “who are more open-minded and have a lot of information.”
Rebuttal and Controversy
Injection particle transmission, colloquially known as vaccine shedding, remains a controversial topic for COVID-19 injections.
Since there has been no study of nor precedent for transmission of mRNA and adenovirus DNA vaccinations, many doctors are waiting for more science to be published, discussing their clinical observation and piecing together findings from limited science.
Since many of these observations are anecdotal, and have not been through rigorous scientific reviewing, many of their statements and observations on vaccine transmission have been routinely fact-checked.
The public and doctors are still waiting for more research and discussion so that they can better understand these symptoms, and until more studies emerge, transmission between vaccinated and unvaccinated individuals will remain a theory that cannot be proven nor disproven.















































")







 ️The Swedish government has decided to donate more than 500,000 doses of the Pfizer/BioNTech coronavirus vaccine to Ukraine, announced the head of the Swedish Foreign Ministry, Ann Linde.
️The Swedish government has decided to donate more than 500,000 doses of the Pfizer/BioNTech coronavirus vaccine to Ukraine, announced the head of the Swedish Foreign Ministry, Ann Linde.