Heliobas Disciple
TB Fanatic
[CONTINUED FROM POST ABOVE]
September 2021 - Scotland launched it’s first investigation into an abnormal spike in newborn baby deaths that was triggered by surpassing a threshold in infant deaths that hadn’t been seen since the 1980’s. (Note- this spike did not occur in 2020, the Year of Covid)
Ashmedai over at Resisting the Intellectual Literati wrote an extensive report on fertility issues and the vaccine back in September 2021.
Resisting the Intellectual Illiteratti
Is There a Plausible Basis For Fertility Concerns?
In my own community, the most prominent concern on the minds of many of the vaccine hesitant, especially young women of childbearing age, is the fear of an adverse effect on fertility. Possibly because of this, fertility concerns have also been derisively dismissed by the doctors with more passion and vengeance than for any other type of adverse effect…
Read more
8 months ago · 49 likes · 40 comments · Ashmedai
August 2021- NPR reported on a survey out of the University of Chicago to investigate reports of changes in menstrual cycles after the vaccine. They received 140,000 responses.,
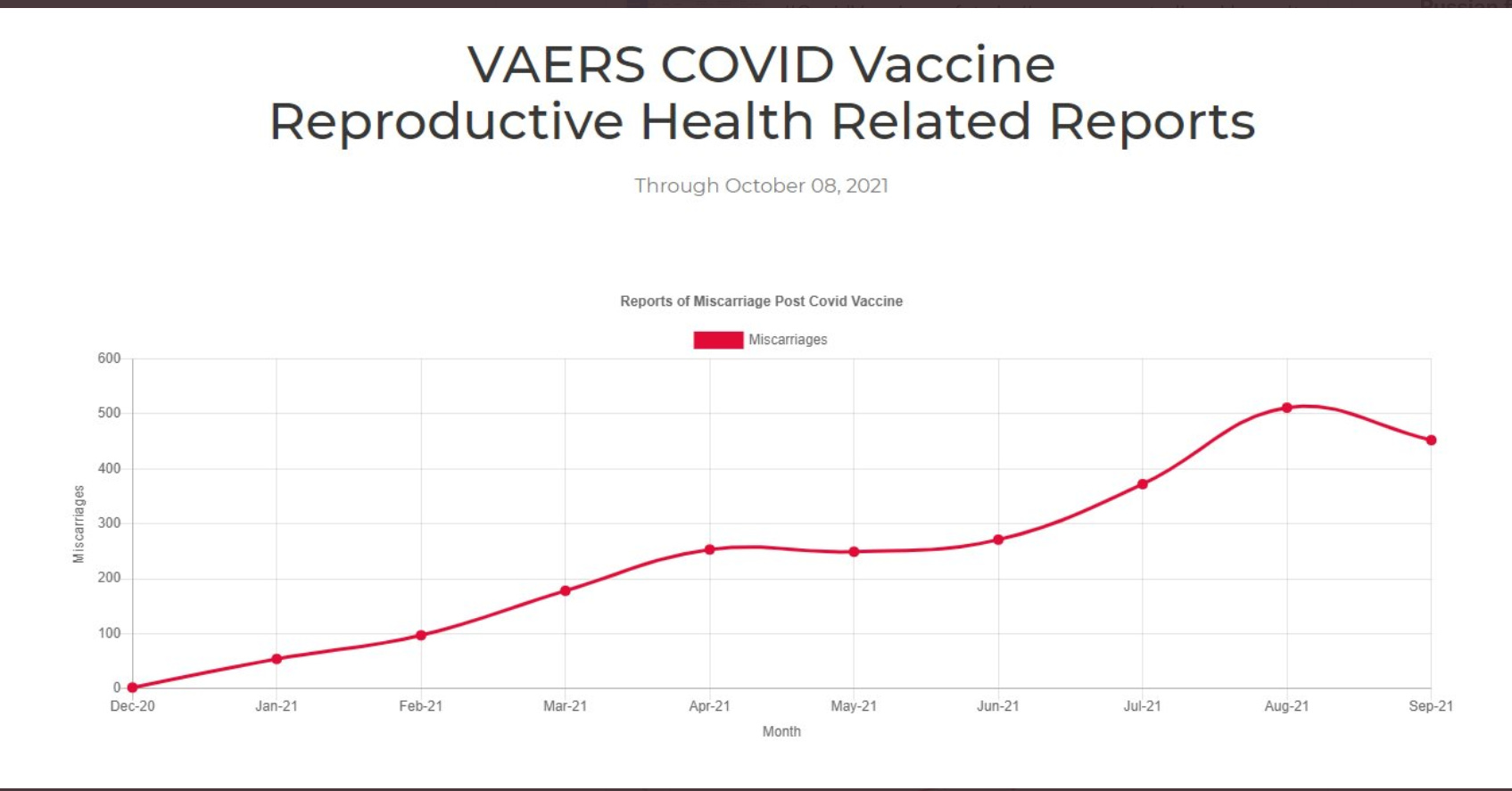
October 2021- VAERS looked like this:

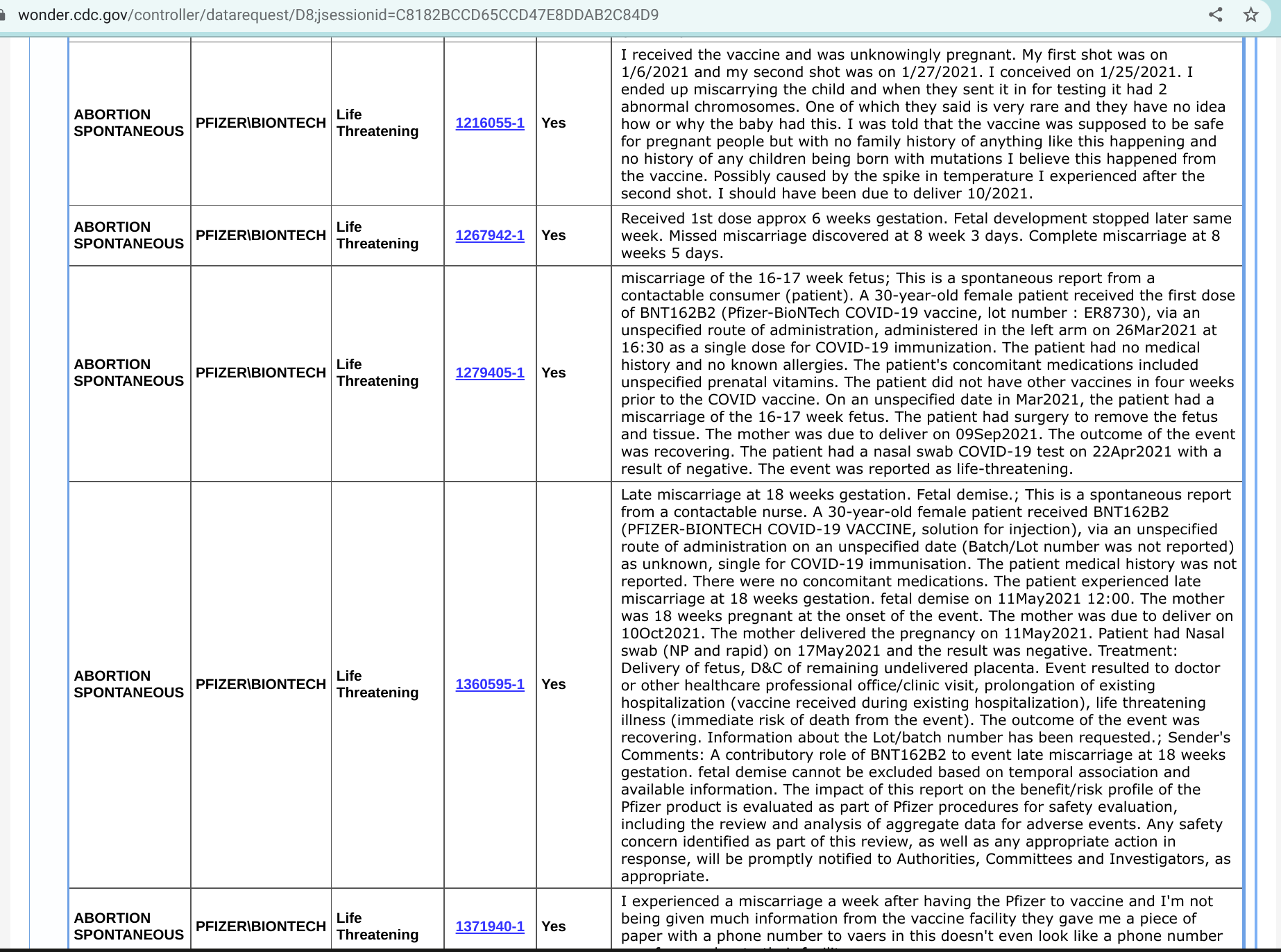
I ran my own VAERS report using only a few pregnancy-related keywords. The list is 769 events long, and here’s a screenshot of just a few from the first page:
December 2021 - IVF clinics reported unusual issues after the mass vaccination campaign began. Steve Kirsch covered it thoroughly.
Steve Kirsch's newsletter
IVF clinics started having serious problems right after the vaccines started rolling out
I just got off the phone with a woman who works at a large IVF clinic. She has to remain nameless to avoid being fired for speaking out. Nobody is supposed to know about the serious problems happening in the IVF clinics. Let me tell you what is really going on and the scientific study that explains it…
Read more
5 months ago · 498 likes · 457 comments · Steve Kirsch
January 2022- NIH funded a study that was released that reported a slight causal relationship between the Covid-19 vaccines and a lengthier menstrual cycle.
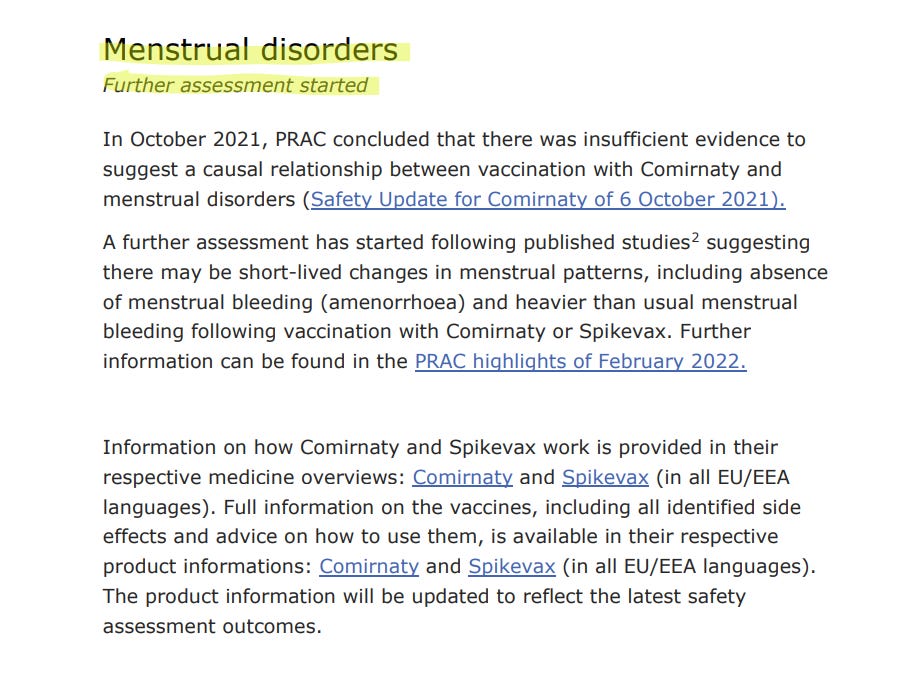
February 2022- An EU health agency announced an investigation between Covid-19 and disruptions in menstrual cycles based on reports coming in.

Josh Guetzkow reported on data from Rambam Hospital in Haifa, Israel. Vaccinated mothers were experiencing spontaneous abortions/miscarriages/stillbirths at a rate that’s 34% higher than their unvaccinated counterparts.
Jackanapes Junction
Stillbirths, Miscarriages and Abortions in Vaccinated vs. Unvaccinated Women
Data from Rambam hospital in Haifa reveal a stillbirth, miscarriage and abortion (SBMA) rate of 6% among women who never received a COVID-19 vaccine, compared to 8% among women who were vaccinated with at least one dose (and never had a SARS-Cov-2 infection…
Read more
4 months ago · 58 likes · 62 comments · Josh Guetzkow
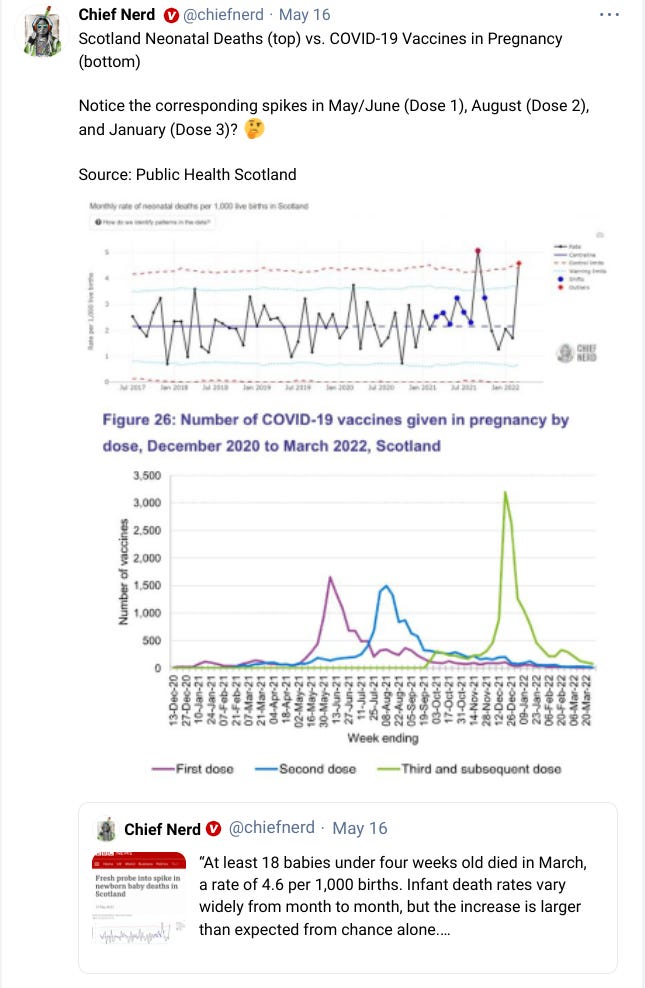
March 2022- A 2nd investigation was launched in Scotland due to the high rate of infant deaths, totaling 18 for the month of March.

Pfizer, what say you?
After spending days reading reports about the horrible negative effects of fertility that are coming out in droves, I had to at least try and get some sort of response from Pfizer. After sitting on hold for a while, a gentleman named Ron got on the line. When I asked if the Covid-19 vaccine is safe for a pregnant woman to take, he read me the entire safety warning from Pfizer’s website. I then told him that I know many women who have had serious disruptions to their menstrual cycle, as well as numerous women who experienced miscarriages late term, shortly after getting one of the Pfizer vaccines. I asked him what he knows about the safety and efficacy of the vaccine, given all the new information that’s come out from the FOIA requests.
He responded that he can pass me along to his managers, but first he has to read another statement, this time from the CDC. He proceeded to verbally read it for 10 minutes while I waited patiently. When he finished, surprised that I was still on the line, he asked if I had any more questions. I said yes, and asked if he wanted to be a whistleblower. He said he noted my response and passed me along to Olivia, which was pretty much a repeat of the first conversation.
I left contact information with both of them just in case, but somehow I highly doubt we’ll get a response. I did note to both of them that should they want to get on the right side of this scandal and begin to help those who are suffering, they should do so before the entire thing crumbles down.
Now What?
We’re now in May 2022. The claims of safety and efficacy don’t match their own internal documents that they tried to hide for 75 years. Yet academic institutions and public health agencies continue to insist it’s recommended for pregnant women to receive Covid-19 vaccines and boosters. Until when? Until the wave of misery gets so large that it’s no longer deniable? No one is coming to save us. Groups like DailyClout, VSRF, America’s Frontline Doctors, Children’s Health Defense, and ICAN are sources of inspiration that there are still good men out there, as well as a source of hope that through their strength and efforts, we’ll come out of the other side of this with some integrity still left in some medical professionals.”
SOURCE
September 2021 - Scotland launched it’s first investigation into an abnormal spike in newborn baby deaths that was triggered by surpassing a threshold in infant deaths that hadn’t been seen since the 1980’s. (Note- this spike did not occur in 2020, the Year of Covid)
Ashmedai over at Resisting the Intellectual Literati wrote an extensive report on fertility issues and the vaccine back in September 2021.
Resisting the Intellectual Illiteratti
Is There a Plausible Basis For Fertility Concerns?
In my own community, the most prominent concern on the minds of many of the vaccine hesitant, especially young women of childbearing age, is the fear of an adverse effect on fertility. Possibly because of this, fertility concerns have also been derisively dismissed by the doctors with more passion and vengeance than for any other type of adverse effect…
Read more
8 months ago · 49 likes · 40 comments · Ashmedai
August 2021- NPR reported on a survey out of the University of Chicago to investigate reports of changes in menstrual cycles after the vaccine. They received 140,000 responses.,
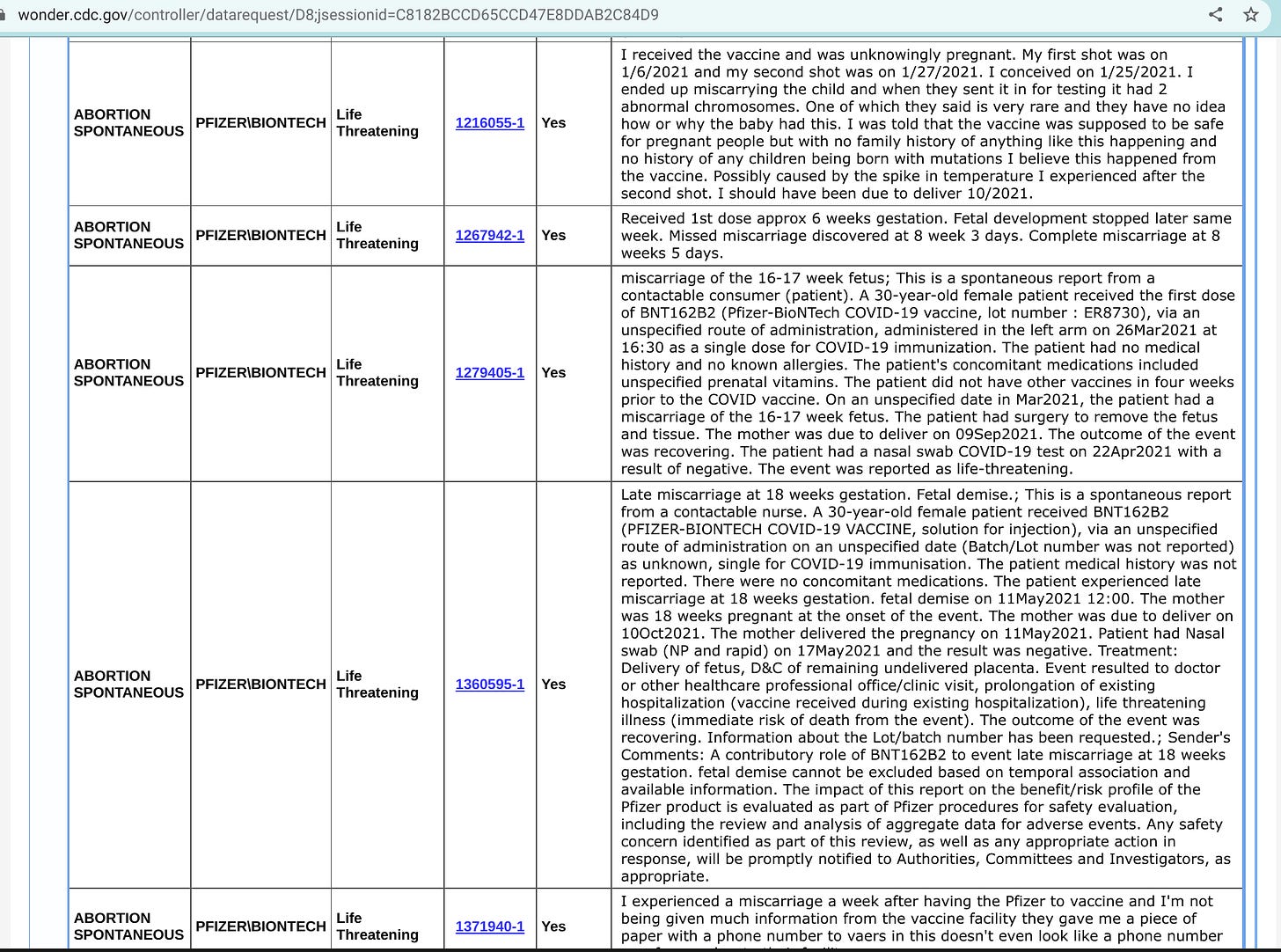
October 2021- VAERS looked like this:
I ran my own VAERS report using only a few pregnancy-related keywords. The list is 769 events long, and here’s a screenshot of just a few from the first page:
December 2021 - IVF clinics reported unusual issues after the mass vaccination campaign began. Steve Kirsch covered it thoroughly.
Steve Kirsch's newsletter
IVF clinics started having serious problems right after the vaccines started rolling out
I just got off the phone with a woman who works at a large IVF clinic. She has to remain nameless to avoid being fired for speaking out. Nobody is supposed to know about the serious problems happening in the IVF clinics. Let me tell you what is really going on and the scientific study that explains it…
Read more
5 months ago · 498 likes · 457 comments · Steve Kirsch
January 2022- NIH funded a study that was released that reported a slight causal relationship between the Covid-19 vaccines and a lengthier menstrual cycle.

February 2022- An EU health agency announced an investigation between Covid-19 and disruptions in menstrual cycles based on reports coming in.
Josh Guetzkow reported on data from Rambam Hospital in Haifa, Israel. Vaccinated mothers were experiencing spontaneous abortions/miscarriages/stillbirths at a rate that’s 34% higher than their unvaccinated counterparts.
Jackanapes Junction
Stillbirths, Miscarriages and Abortions in Vaccinated vs. Unvaccinated Women
Data from Rambam hospital in Haifa reveal a stillbirth, miscarriage and abortion (SBMA) rate of 6% among women who never received a COVID-19 vaccine, compared to 8% among women who were vaccinated with at least one dose (and never had a SARS-Cov-2 infection…
Read more
4 months ago · 58 likes · 62 comments · Josh Guetzkow
March 2022- A 2nd investigation was launched in Scotland due to the high rate of infant deaths, totaling 18 for the month of March.
Pfizer, what say you?
After spending days reading reports about the horrible negative effects of fertility that are coming out in droves, I had to at least try and get some sort of response from Pfizer. After sitting on hold for a while, a gentleman named Ron got on the line. When I asked if the Covid-19 vaccine is safe for a pregnant woman to take, he read me the entire safety warning from Pfizer’s website. I then told him that I know many women who have had serious disruptions to their menstrual cycle, as well as numerous women who experienced miscarriages late term, shortly after getting one of the Pfizer vaccines. I asked him what he knows about the safety and efficacy of the vaccine, given all the new information that’s come out from the FOIA requests.
He responded that he can pass me along to his managers, but first he has to read another statement, this time from the CDC. He proceeded to verbally read it for 10 minutes while I waited patiently. When he finished, surprised that I was still on the line, he asked if I had any more questions. I said yes, and asked if he wanted to be a whistleblower. He said he noted my response and passed me along to Olivia, which was pretty much a repeat of the first conversation.
I left contact information with both of them just in case, but somehow I highly doubt we’ll get a response. I did note to both of them that should they want to get on the right side of this scandal and begin to help those who are suffering, they should do so before the entire thing crumbles down.
Now What?
We’re now in May 2022. The claims of safety and efficacy don’t match their own internal documents that they tried to hide for 75 years. Yet academic institutions and public health agencies continue to insist it’s recommended for pregnant women to receive Covid-19 vaccines and boosters. Until when? Until the wave of misery gets so large that it’s no longer deniable? No one is coming to save us. Groups like DailyClout, VSRF, America’s Frontline Doctors, Children’s Health Defense, and ICAN are sources of inspiration that there are still good men out there, as well as a source of hope that through their strength and efforts, we’ll come out of the other side of this with some integrity still left in some medical professionals.”
SOURCE