COVID-19 Drugs: Fluvoxamine, an inexpensive anti-depressant drug is now emerging as a potential candidate to be repurposed to treat COVID-19. Speculations are adrift that Canada might be the first country to approve its usage to treat COVID-19 followed by the United States, India, Brazil and...
www.thailandmedical.news
(fair use applies)
EMPHASIS IN ORIGINAL ARTICLE (not added by me)
Fluvoxamine- An ‘Inexpensive’ Anti-Depressant Emerging As A Leading Drug Candidate To be Repurposed To Treat COVID-19
Aug 14, 2021
Fluvoxamine, an inexpensive anti-depressant drug is now emerging as a potential candidate to be repurposed to treat COVID-19.
Speculations are adrift that Canada might be the first country to approve its usage to treat COVID-19 followed by the United States, India, Brazil and South Africa.
Fluvoxamine, sold under the brand name Luvox among others, is an antidepressant of the selective serotonin reuptake inhibitor (SSRI) class which is used primarily for the treatment of depression disorder and obsessive–compulsive disorder (OCD). It is also used to treat anxiety disorders, such as panic disorder, social anxiety disorder, and post-traumatic stress disorder.
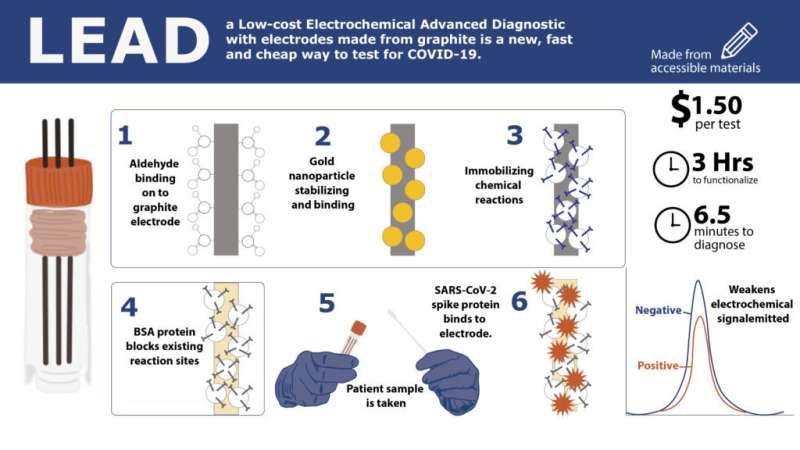
Initially fluvoxamine was identified through computational silico studies for its binding ability to both the human ACE2 receptors and also to the spike proteins of the SARS-CoV-2 coronavirus thus preventing binding between the two and acting to a certain degree as an antiviral.
Blocking the interactions between human ACE2 and coronavirus spike glycoprotein by selected drugs: a computational perspective
Vitro studies also confirmed its ability to reduce Sars-CoV-2 viral loads through interference with the ACE2/TMPRSS2 receptors.
Antidepressant and antipsychotic drugs reduce viral infection by SARS-CoV-2 and fluoxetine show antiviral activity against the novel variants in vitro
Another study showed that fluvoxamine could also act as an antiviral via affecting the membrane of the SARS-CoV-2 coronavirus and even suggested its usage as a prophylaxis.
Low-dose fluvoxamine modulates endocytic trafficking of SARS-CoV-2 spike protein: a potential mechanism for anti-COVID-19 protection by antidepressants
However it should be noted that fluvoxamine, an FDA-approved antidepressant, works best by being an S1R agonist. Although fluvoxamine may inhibit SARS-CoV-2 by interfering with endosomal viral trafficking, most studies suggest that its main benefit is likely to be as an inhibitor of excess cytokine production.
Fluvoxamine: A Review of Its Mechanism of Action and Its Role in COVID-19
Fluvoxamine has also been shown to modulate the response to bacterial sepsis in a beneficial manner in a mouse model, preventing inflammation as well as sepsis hence its usage is beneficial in COVID-19.
Modulation of the sigma-1 receptor-IRE1 pathway is beneficial in preclinical models of inflammation and sepsis - PubMed
This study published in the Science Translational Medicine journal mechanistically explained that S1R (ER-resident protein sigma-1 receptor]) restricts the endonuclease activity of the ER (endoplasmic reticulum) stress sensor IRE1 and cytokine expression but does not inhibit the classical inflammatory signaling pathways. These findings have substantial clinical implications as it shows that fluvoxamine, an antidepressant therapeutic with high affinity for S1R, protects mice from lethal septic shock and dampens the inflammatory response in human blood leukocytes. The s ame cytokine storm that is mentioned in this study is also an inflammation-causing symptom in COVID-19.
In a double-blind, randomized, placebo-controlled study of 152 outpatients with confirmed SARS-CoV-2 infection, none of 80 patients receiving fluvoxamine compared to 6 of 72 patients receiving placebo experienced clinical deterioration over 15 days (P = 0.009). Effect of Fluvoxamine vs Placebo on Clinical Deterioration in Outpatients With Symptomatic COVID-19
The results of this study prompted another case study during a late 2020 COVID-19 outbreak at a horse racing track in California. Sixty-five track workers volunteered to receive 50 mg of fluvoxamine twice a day, and the 48 who declined were used as comparison. Similar to the first study, none who received fluvoxamine had clinical deterioration after 14 days; whereas, 12.5% of those who didn't receive fluvoxamine did and 60% still had symptoms, according to the results published in Open Forum Infectious Diseases. Prospective Cohort of Fluvoxamine for Early Treatment of Coronavirus Disease 19
A larger study of fluvoxamine in 1,100 patients is currently underway (NCT04668950) and also another 3 more clinical trials are underway in various countries.
Numerous other studies are also suggesting repurposing Sigma-1 Receptor Ligands such as fluvoxamine for COVID-19 therapy.
Repurposing Sigma-1 Receptor Ligands for COVID-19 Therapy?
Nevertheless, in the race to find treatments to prevent and treat coronavirus infections, fluvoxamine could be a useful addition. If given during the initial fever and coughing phase of COVID-19, the drug could reduce the number of patients who develop the dangerous second phase of COVID-19, characterized by the cytokine storm and subsequent lung damage.
Given that the drug’s therapeutic effects in COVID-19 may be mediated via the S1R, it would certainly be worth studying in detail its effectiveness.
Another study led by the Duke Clinical Research Institute is looking at whether three existing medications would treat mild-to-moderate COVID-19 effectively.
The three repurposed medications, already approved by the U.S. Food and Drug Administration for other uses, are: 1)Ivermectin, used to treat parasitic infections; 2)Fluticasone, an inhaled steroid commonly prescribed for asthma and chronic obstructive pulmonary disease; and 3)Fluvoxamine, a selective serotonin reuptake inhibitor (SSRI), often prescribed for depression.
Nationwide Clinical Study Expands Platform to Test Medications to Treat Mild-to-Moderate COVID-19 - DCRI
However the first drug Ivermectin is already being discounted as a lot of emerging data is showing that it does not work with the newer variants.
Meanwhile a new Canadian led trial involving fluvoxamine to treat COVID-19 that was just completed by researchers from McMaster University is creating a stir in both the medical community and also the media.
Various Canadian media are calling the trial results which are going to be published soon as “Among the most important findings since the COVID pandemic began.”
The inexpensive anti-depressant curbed the number of COVID-19 patients ending up in hospital by 30 per cent, making it a potential breakthrough treatment for a virus that continues to spread widely, the Canadian-led clinical trial is reporting.
Once confirmed by more research, the drug, fluvoxamine, would be one of the most effective and convenient to treat the virus outside of pricey new “monoclonal antibodies.” They typically have to be administered in a hospital, as opposed to a pill taken orally at home.
The drug fluvoxamine is given early in the course of the disease, potentially staving off more severe outcomes and their cost to the health-care system.
This relatively large, randomized controlled study was carried out in Brazil and spearheaded by co-principal investigator Dr Ed Mills and other researchers associated with McMaster University in Ontario. It was part of their larger trial that is testing a number of potential drug treatments against COVID.
The study team looked at the rate of hospitalization among patients with test-confirmed infection. Most of the eight studied drugs, including much-debated candidates such as hydroxychloroquine and ivermectin, showed no detectable benefits.
However the study found that 77 of the 739 subjects who were randomly selected to receive fluvoxamine ended up spending less than six hours in an emergency department or being admitted to hospital, compared to 108 of the 733 who were administered a placebo.
The trial’s independent data-safety monitoring board, which keeps an eye on results that are blinded to the actual researchers, ordered the trial stopped after seeing the positive numbers, said Dr Mills.
It confirms smaller, earlier studies that had shown promise for the drug fluvoxamine that was used to treat obsessive-compulsive disorder and its anti-inflammatory properties that is beneficial for COVID-19.
Dr Mills, a part-time professor at McMaster told Thailand Medical News, “This is among the most important findings since the COVID pandemic began.”
He added, “You have a Canadian-led study that has the potential to change guidance around the world for a very cheap treatment. This is a massive finding of benefit to public health.”
The drug fluvoxamine costing about US$4 per 10-day course, could be especially important in poorer countries with low vaccination rates and that lack the ability to acquire more expensive therapies, he said.
The study team including co-principal investigator Dr. Gilmar Reis of Brazil’s Pontificia Universidade Catòlica de Minas Gerais plan to post a paper outlining their results on a pre-print site and submit it to a journal for publication within days, the study findings are already being peer reviewed.
The study team had already presented their findings to a meeting of the National Institutes of Health (NIH) in the U.S. last week and to World Health Organization experts. And the team includes world-renowned clinical trial experts from McMaster, including Dr Gordon Guyatt, credited with coining the term “evidence-based medicine.”
Dr David Boulware, an infectious disease specialist at the University of Minnesota and national co-chair of the NIH’s own trial investigating potential COVID treatments commented, “This is really the first large trial that shows a benefit for fluvoxamine or any oral medication. It’s inexpensive, it’s generic and it’s going to be used. So in that sense it’s a world-wide drug.”
Dr Boulware, who was co-author of one of the earlier, small studies of fluvoxamine and COVID, said some of the monocolonal antibody treatments given emergency approval by regulators have greater effectiveness, but their high cost and mode of administration limit how widely they are used.
Head of the infectious disease department at Queen’s University’s medical school, Dr Gerald Evans said, “This trial did back up those earlier studies and was headed by respected researchers. The findings are impressive. Everything that I’ve seen does suggest it’s an honest, true signal. This is the first drug that has shown a consistent benefit for COVID 19, which separates it from others being studied including Ivermectin which is now deemed to be ineffective.”
However before the trial studies were released, those in the inner circles including Thailand Medical News started to stockpile on the drug and already it was noticed that there is a short supply of the drug and prices are already starting to skyrocket.
Thailand Medical News found that in New York the drugs were going now at US$320 for sixty tablets and supplies were short and a doctor’s prescription was needed.
In Sydney and Thailand, a doctor‘s prescription was also needed and prices were going for US$180 for sixty tablets in Australia while in Thailand it was going for US$60. However there are no longer supplies available in Thailand nor in Australia.
There were numerous sites selling so called generic versions in Thailand, India and also from Pakistan but most were found to either be substandard or fake.
Hence the question arises, who is controlling the supply of these drugs and why is there all of a sudden a shortage.
If the demand for fluvoxamine does increase, it is expected to cause extreme drug shortages in the US market.
It was reported that in 1994, fluvoxamine became the US Food & Drug Administration's (FDA's) first approved SSRI, although it has been used internationally in clinical practice since 1983.
Solvay was the first and exclusive manufacturer, selling fluvoxamine under the brand name Luvox.
The U.S.FDA currently reports that seven companies that still hold approved abbreviated new drug applications to manufacture fluvoxamine, and several other firms have entered and exited the market over the past decade.
Unlike many other generic drugs that are made primarily in India, much of the fluvoxamine is produced in US facilities.
In India, it was found that one two companies are currently making generic fluvoxamine but the quality is inferior plus the U.S FDA had discovered contaminants in them before had had recalled these products and subsequently banned these Indian products in 2014.
Thailand Medical News checked and found that there are at least five manufacturers in the United States who still make the active pharmaceutical ingredient known as fluvoxamine. However their production is extremely small.
Drug shortages are less likely to occur when there are multiple active ingredient manufacturers, when some of that production is based in the United States, and when there is continued strong demand for the drug.
Already demand for fluvoxamine continues to be substantial for OCD, as well as off-label for social anxiety disorder and other conditions.
Drugs.com lists the cost for a bottle of 100 25-mg oral tablets around $79, but the US market demand was enough to pull in approximately US$28 million in sales from September 2018 to September 2019, according to Upsher Smith, one of the drug's generic manufacturers.
However despite the promising role of fluvoxamine to treat COVID-19, if nothing is done to scale up fluvoxamine production and to keep prices down, the whole purpose of finding cheap therapeutic solutions to treat COVID-19 would be pointless as already it is difficult for common people to find a bottle of fluvoxamine anywhere around the world at present!
For more on
Fluvoxamine and COVID-19, keep on logging to Thailand Medical News. (Please note that I do not have the luxury of having an editor to peruse through all my writings which might not be perfect grammatically and also I do not have the luxury of time on my side as I also handle numerous other websites, research and community projects. Thailand Medical News is basically a one man show! I would however appreciate your help in donating to support all these efforts.
Sponsorship - Thailand Medical News Do not be a ‘Cheap Charlie’ and simply read and ignore the plea for help. Those who cannot donate, do not send me emails with your negative comments about the standard or my writing skills as you know what you could do with those and also hopefully you will end up as one of the COVID-19 statistical figures! Thank You.)
Do not attempt to self-prescibe or self-treat using fluvoxamine. Always consult a licensed medical doctor first. (Provided he or she knows anything about SARS-CoV-2 and COVID-19!)


























 receives a Covid-19 vaccination at Martin Luther King Jr. (MLK) Community Hospital on January 6, 2021 in the Willowbrook neighborhood of Los Angeles, California. - Deep within a South Los Angeles hospital, a row of elderly Hispanic men in induced comas lay hooked up …")