
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
CORONA Main Coronavirus thread
- Thread starter Heliobas Disciple
- Start date
-
- Tags
- coronavirus

jward
passin' thru

NEWS MAKER
@NEWS_MAKER
5m
Over 3000 People 'UNABLE TO PERFORM NORMAL DAILY ACTIVITIES, UNABLE TO WORK, REQUIRED CARE FROM DOCTOR OR HEALTH CARE PROFESSIONAL' after taking covid vaccine per CDC https://cdc.gov/vaccines/acip/

PanBear
Veteran Member
VUI-202012/01
Covid-19: New coronavirus variant is identified in UK
BMJ 2020; 371 doi: Covid-19: New coronavirus variant is identified in UK
(Published 16 December 2020)
Cite this as: BMJ 2020;371:m4857
England’s health secretary, Matt Hancock, has told parliament that a new variant of covid-19 has been identified and may be driving infections in the south east, leading to headlines about “mutant covid.” Jacqui Wise answers some common questions
What do we know about this new SARS-CoV-2 variant?
It’s been snappily named VUI-202012/01 (the first “Variant Under Investigation” in December 2020) and is defined by a set of 17 changes or mutations. One of the most significant is an N501Y mutation in the spike protein that the virus uses to bind to the human ACE2 receptor. Changes in this part of spike protein may, in theory, result in the virus becoming more infectious and spreading more easily between people.
How was the variant detected?
It was picked up by the Covid-19 Genomics UK (COG-UK) consortium, which undertakes random genetic sequencing of positive covid-19 samples around the UK. The consortium is a partnership of the UK’s four public health agencies, as well as the Wellcome Sanger Institute and 12 academic institutions.
Since being set up in April 2020 the consortium has sequenced 140 000 virus genomes from people infected with covid-19. It uses the data to track outbreaks, identify variant viruses, and publish a weekly report (Data - COG-UK Consortium).
How common is it?
As of 13 December, 1108 cases with this variant had been identified in the UK in nearly 60 different local authorities, although the true number will be much higher. These cases were predominantly in the south east of England, but there have been recent reports from further afield, including Wales and Scotland.
Nick Loman, professor of microbial genomics and bioinformation at the University of Birmingham, told a briefing by the Science Media Centre on 15 December that the variant was first spotted in late September and now accounts for 20% of viruses sequenced in Norfolk, 10% in Essex, and 3% in Suffolk. “There are no data to suggest it had been imported from abroad, so it is likely to have evolved in the UK,” he said.
Does this variant spread more quickly?
Matt Hancock told the House of Commons on 14 December that initial analysis showed that the new variant “may be associated” with the recent rise in cases in southeast England. However, this is not the same as saying that it is causing the rise.
Loman explained, “This variant is strongly associated with where we are seeing increasing rates of covid-19. It’s a correlation, but we can’t say it is causation. But there is striking growth in this variant, which is why we are worried, and it needs urgent follow-up and investigation.”
Is mutation to be expected?
SARS-CoV-2 is an RNA virus, and mutations arise naturally as the virus replicates. Many thousands of mutations have already arisen, but only a very small minority are likely to be important and to change the virus in an appreciable way. COG-UK says that there are currently around 4000 mutations in the spike protein.
Sharon Peacock, director of COG-UK, told the Science Media Centre briefing, “Mutations are expected and are a natural part of evolution. Many thousands of mutations have already arisen, and the vast majority have no effect on the virus but can be useful as a barcode to monitor outbreaks.”
Is the new variant more dangerous?
We don’t know yet. Mutations that make viruses more infectious don’t necessarily make them more dangerous. A number of variants have already been detected in the UK. For example, the D614G variant is believed to have increased the ability of the virus to be transmitted and is now the most common type circulating in the UK, although it doesn’t seem to result in more severe disease.
Public Health England’s laboratory at Porton Down is currently working to find any evidence that the new variant increases or decreases the severity of disease. Susan Hopkins, joint medical adviser for NHS Test and Trace and Public Health England, said, “There is currently no evidence that this strain causes more severe illness, although it is being detected in a wide geography, especially where there are increased cases being detected.”
Will the vaccine still work?
The new variant has mutations to the spike protein that the three leading vaccines are targeting. However, vaccines produce antibodies against many regions in the spike protein, so it’s unlikely that a single change would make the vaccine less effective.
Over time, as more mutations occur, the vaccine may need to be altered. This happens with seasonal flu, which mutates every year, and the vaccine is adjusted accordingly. The SARS-CoV-2 virus doesn’t mutate as quickly as the flu virus, and the vaccines that have so far proved effective in trials are types that can easily be tweaked if necessary.
Peacock said, “With this variant there is no evidence that it will evade the vaccination or a human immune response. But if there is an instance of vaccine failure or reinfection then that case should be treated as high priority for genetic sequencing.”
This article is made freely available for use in accordance with BMJ's website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
Coronavirus (covid-19) Hub usage terms

 www.bmj.com
www.bmj.com
Covid-19: New coronavirus variant is identified in UK
BMJ 2020; 371 doi: Covid-19: New coronavirus variant is identified in UK
(Published 16 December 2020)
Cite this as: BMJ 2020;371:m4857
England’s health secretary, Matt Hancock, has told parliament that a new variant of covid-19 has been identified and may be driving infections in the south east, leading to headlines about “mutant covid.” Jacqui Wise answers some common questions
What do we know about this new SARS-CoV-2 variant?
It’s been snappily named VUI-202012/01 (the first “Variant Under Investigation” in December 2020) and is defined by a set of 17 changes or mutations. One of the most significant is an N501Y mutation in the spike protein that the virus uses to bind to the human ACE2 receptor. Changes in this part of spike protein may, in theory, result in the virus becoming more infectious and spreading more easily between people.
How was the variant detected?
It was picked up by the Covid-19 Genomics UK (COG-UK) consortium, which undertakes random genetic sequencing of positive covid-19 samples around the UK. The consortium is a partnership of the UK’s four public health agencies, as well as the Wellcome Sanger Institute and 12 academic institutions.
Since being set up in April 2020 the consortium has sequenced 140 000 virus genomes from people infected with covid-19. It uses the data to track outbreaks, identify variant viruses, and publish a weekly report (Data - COG-UK Consortium).
How common is it?
As of 13 December, 1108 cases with this variant had been identified in the UK in nearly 60 different local authorities, although the true number will be much higher. These cases were predominantly in the south east of England, but there have been recent reports from further afield, including Wales and Scotland.
Nick Loman, professor of microbial genomics and bioinformation at the University of Birmingham, told a briefing by the Science Media Centre on 15 December that the variant was first spotted in late September and now accounts for 20% of viruses sequenced in Norfolk, 10% in Essex, and 3% in Suffolk. “There are no data to suggest it had been imported from abroad, so it is likely to have evolved in the UK,” he said.
Does this variant spread more quickly?
Matt Hancock told the House of Commons on 14 December that initial analysis showed that the new variant “may be associated” with the recent rise in cases in southeast England. However, this is not the same as saying that it is causing the rise.
Loman explained, “This variant is strongly associated with where we are seeing increasing rates of covid-19. It’s a correlation, but we can’t say it is causation. But there is striking growth in this variant, which is why we are worried, and it needs urgent follow-up and investigation.”
Is mutation to be expected?
SARS-CoV-2 is an RNA virus, and mutations arise naturally as the virus replicates. Many thousands of mutations have already arisen, but only a very small minority are likely to be important and to change the virus in an appreciable way. COG-UK says that there are currently around 4000 mutations in the spike protein.
Sharon Peacock, director of COG-UK, told the Science Media Centre briefing, “Mutations are expected and are a natural part of evolution. Many thousands of mutations have already arisen, and the vast majority have no effect on the virus but can be useful as a barcode to monitor outbreaks.”
Is the new variant more dangerous?
We don’t know yet. Mutations that make viruses more infectious don’t necessarily make them more dangerous. A number of variants have already been detected in the UK. For example, the D614G variant is believed to have increased the ability of the virus to be transmitted and is now the most common type circulating in the UK, although it doesn’t seem to result in more severe disease.
Public Health England’s laboratory at Porton Down is currently working to find any evidence that the new variant increases or decreases the severity of disease. Susan Hopkins, joint medical adviser for NHS Test and Trace and Public Health England, said, “There is currently no evidence that this strain causes more severe illness, although it is being detected in a wide geography, especially where there are increased cases being detected.”
Will the vaccine still work?
The new variant has mutations to the spike protein that the three leading vaccines are targeting. However, vaccines produce antibodies against many regions in the spike protein, so it’s unlikely that a single change would make the vaccine less effective.
Over time, as more mutations occur, the vaccine may need to be altered. This happens with seasonal flu, which mutates every year, and the vaccine is adjusted accordingly. The SARS-CoV-2 virus doesn’t mutate as quickly as the flu virus, and the vaccines that have so far proved effective in trials are types that can easily be tweaked if necessary.
Peacock said, “With this variant there is no evidence that it will evade the vaccination or a human immune response. But if there is an instance of vaccine failure or reinfection then that case should be treated as high priority for genetic sequencing.”
This article is made freely available for use in accordance with BMJ's website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
Coronavirus (covid-19) Hub usage terms
Covid-19: New coronavirus variant is identified in UK
England’s health secretary, Matt Hancock, has told parliament that a new variant of covid-19 has been identified and may be driving infections in the south east, leading to headlines about “mutant covid.” Jacqui Wise answers some common questions It’s been snappily named VUI-202012/01 (the...
PanBear
Veteran Member
(fair use)
SCMP
Hong Kong fourth wave: 109 Covid-19 cases confirmed as officials vow manpower boost to ensure more efficient quarantine process
Target of quarantining close contacts of coronavirus patients within two days follows emergency interdepartmental meeting, city’s No 2 official says
Of Saturday’s infections, 102 were locally transmitted, including 42 from unknown sources
Gigi Choy
Kanis Leung
Published: 12:25pm, 19 Dec, 2020

A quarantine centre at Hong Kong’s Penny Bay on Lantau Island. Photo: Winson Wong
Hong Kong would draw resources from multiple departments to meet the manpower needs necessary to ensure the close contacts of Covid-19 patients were quarantined within two days, officials said on Saturday, as 109 new coronavirus cases were confirmed.
Of the new infections, 102 were locally transmitted, including 42 from unknown sources. The official count now stands at 8,078 cases, with 129 related deaths. About 70 preliminary-positive cases were also logged.
Officials admitted that a strain on resources after the recent surge in Covid-19 cases had led to delays in quarantining people.
Chief Secretary Matthew Cheung Kin-chung said the new target of quarantining coronavirus patients’ close contacts within two days was set at an emergency interdepartmental meeting, and that a coordination mechanism would also be put in place to streamline large-scale evacuations of housing estates.
The pledge came after a 62-year-old woman ordered to undergo a screening was found dead in her home before she could be moved into isolation as planned. A postmortem test confirmed she had Covid-19, sparking concerns over delays in the city’s quarantine efforts.
“I feel sad about her passing … We admit that we hurried through things and were careless. We won’t defend ourselves,” Cheung told a radio show. “We need to prevent similar incidents from happening again.”
The Department of Health on Saturday afternoon said it had transferred more than 480 close contacts to quarantine centres in a 24-hour operation.
The department had earlier pointed out it had handled evacuations of residents from five housing blocks over the past two weeks, in addition to dealing with an “exponential increase” in the number of close contacts.
“Most of the staff responsible for transferring close contacts to quarantine centres were mobilised to provide on-site support in the evacuation exercises. As a result, some close contacts could not be promptly transferred to the centres,” a spokesman said.
Secretary for Food and Health Sophia Chan Siu-chee admitted on the same radio programme there was room for improvement in some procedures, while acknowledging the Department of Health would need to send close contacts of Covid-19 patients to quarantine centres at a faster pace, and improve overall coordination.
She said health officers had already reconsidered manpower arrangements, and more resources from other departments had been deployed to carry out the work.
“More manpower and vehicles have been arranged. Even the Fire Services Department is helping out now on the provision of vehicles. The procedures should be smoother,” she said.
The minister said health officers should have a target of transferring close contacts to quarantine centres within a day, adding the department would need to request help if it faced staff shortages.
She said if staff found they could not handle some cases, they would have to seek assistance from police as soon as possible.
The sense of urgency follows the recording of multiple infections at five residential buildings, prompting health authorities to distribute specimen bottles at Fu Yan House at Fu Shan Estate in Diamond Hill, Shek Wing House at Shek Lei (II) Estate in Kwai Chung, Ping Shing House at Ping Tin Estate in Lam Tin, Skypark in Mong Kok, and Block D of Kwan Yick Building Phase II in Sai Wan.
Mandatory testing was also ordered at King Tsui Court in Chai Wan and Block 6 of Richland Gardens in Kowloon Bay.
Meanwhile, existing clusters of known infections also continued to grow.
Five more cases were linked to the Yata department store in Sha Tin, two each to Billy Music Classroom at New Trend Centre in San Po Kong and a Lohas Park building site in Tseung Kwan O, and one each at Kwai Tung House at Tung Tau Estate in Wong Tai Sin, Ming Lai House at Choi Wan Estate (II) in Ngau Chi Wan, and a construction site at the Tseung Kwan O-Lam Tin Tunnel.
An additional case was also added to the city’s single largest cluster of infections – tied to Hong Kong dancing venues – which now stands at more than 700.

 www.scmp.com
www.scmp.com
SCMP
Hong Kong fourth wave: 109 Covid-19 cases confirmed as officials vow manpower boost to ensure more efficient quarantine process
Target of quarantining close contacts of coronavirus patients within two days follows emergency interdepartmental meeting, city’s No 2 official says
Of Saturday’s infections, 102 were locally transmitted, including 42 from unknown sources
Gigi Choy
Kanis Leung
Published: 12:25pm, 19 Dec, 2020
A quarantine centre at Hong Kong’s Penny Bay on Lantau Island. Photo: Winson Wong
Hong Kong would draw resources from multiple departments to meet the manpower needs necessary to ensure the close contacts of Covid-19 patients were quarantined within two days, officials said on Saturday, as 109 new coronavirus cases were confirmed.
Of the new infections, 102 were locally transmitted, including 42 from unknown sources. The official count now stands at 8,078 cases, with 129 related deaths. About 70 preliminary-positive cases were also logged.
Officials admitted that a strain on resources after the recent surge in Covid-19 cases had led to delays in quarantining people.
Chief Secretary Matthew Cheung Kin-chung said the new target of quarantining coronavirus patients’ close contacts within two days was set at an emergency interdepartmental meeting, and that a coordination mechanism would also be put in place to streamline large-scale evacuations of housing estates.
The pledge came after a 62-year-old woman ordered to undergo a screening was found dead in her home before she could be moved into isolation as planned. A postmortem test confirmed she had Covid-19, sparking concerns over delays in the city’s quarantine efforts.
“I feel sad about her passing … We admit that we hurried through things and were careless. We won’t defend ourselves,” Cheung told a radio show. “We need to prevent similar incidents from happening again.”
The Department of Health on Saturday afternoon said it had transferred more than 480 close contacts to quarantine centres in a 24-hour operation.
The department had earlier pointed out it had handled evacuations of residents from five housing blocks over the past two weeks, in addition to dealing with an “exponential increase” in the number of close contacts.
“Most of the staff responsible for transferring close contacts to quarantine centres were mobilised to provide on-site support in the evacuation exercises. As a result, some close contacts could not be promptly transferred to the centres,” a spokesman said.
Secretary for Food and Health Sophia Chan Siu-chee admitted on the same radio programme there was room for improvement in some procedures, while acknowledging the Department of Health would need to send close contacts of Covid-19 patients to quarantine centres at a faster pace, and improve overall coordination.
She said health officers had already reconsidered manpower arrangements, and more resources from other departments had been deployed to carry out the work.
“More manpower and vehicles have been arranged. Even the Fire Services Department is helping out now on the provision of vehicles. The procedures should be smoother,” she said.
The minister said health officers should have a target of transferring close contacts to quarantine centres within a day, adding the department would need to request help if it faced staff shortages.
She said if staff found they could not handle some cases, they would have to seek assistance from police as soon as possible.
The sense of urgency follows the recording of multiple infections at five residential buildings, prompting health authorities to distribute specimen bottles at Fu Yan House at Fu Shan Estate in Diamond Hill, Shek Wing House at Shek Lei (II) Estate in Kwai Chung, Ping Shing House at Ping Tin Estate in Lam Tin, Skypark in Mong Kok, and Block D of Kwan Yick Building Phase II in Sai Wan.
Mandatory testing was also ordered at King Tsui Court in Chai Wan and Block 6 of Richland Gardens in Kowloon Bay.
Meanwhile, existing clusters of known infections also continued to grow.
Five more cases were linked to the Yata department store in Sha Tin, two each to Billy Music Classroom at New Trend Centre in San Po Kong and a Lohas Park building site in Tseung Kwan O, and one each at Kwai Tung House at Tung Tau Estate in Wong Tai Sin, Ming Lai House at Choi Wan Estate (II) in Ngau Chi Wan, and a construction site at the Tseung Kwan O-Lam Tin Tunnel.
An additional case was also added to the city’s single largest cluster of infections – tied to Hong Kong dancing venues – which now stands at more than 700.
Hong Kong boosts manpower to speed quarantine process, as 109 Covid-19 cases logged
Target of quarantining close contacts of coronavirus patients within two days follows emergency interdepartmental meeting, city’s No 2 official says.
jward
passin' thru
Those headlines will be out at the first sign that they're needed, imho : (How many days before these headlines come out on our east coast?
Anyone taking five dollar bets?

marsh
On TB every waking moment
First talk is about the vaccine
View: https://www.youtube.com/watch?v=qUnmLk0QiQo
LIVE
LIVE: Turning Point USA day 2: Dan Bongino, Michael Knowles, Benny Johnson, and more | Epoch Times
•Started streaming 112 minutes ago

The Epoch Times
LIVE
LIVE: Turning Point USA day 2: Dan Bongino, Michael Knowles, Benny Johnson, and more | Epoch Times
•Started streaming 112 minutes ago
The Epoch Times
marsh
On TB every waking moment
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
 www.zerohedge.com
www.zerohedge.com
CDC Issues New Guidelines, Launches Probe After 1000s Negatively-Affected Following COVID-19 Vaccination
SUNDAY, DEC 20, 2020 - 9:50
Thousands of people have been unable to work or perform daily activities, or required care from a healthcare professional, after getting the new COVID-19 vaccine, according to new data from the Centers for Disease Control and Prevention (CDC).

As of Dec. 18, 3,150 people reported what the agency terms “Health Impact Events” after getting vaccinated.
The definition of the term is: “unable to perform normal daily activities, unable to work, required care from doctor or health care professional.”
As The Epoch Times' Zachary Stieber reports, the people reporting the negative effects reported them through V-safe, a smartphone application. The tool uses text messages and web surveys to provide personalized health check-ins and allows users to quickly tell the CDC if they are experiencing side effects.
The CDC and Pfizer, which produces the vaccine with BioNTech, didn’t respond to request for comments.
The information was presented by Dr. Thomas Clark, a CDC epidemiologist, to the Advisory Committee on Immunization Practices, an independent panel that provides recommendations to the agency, on Saturday.

(slideshow on website)
The CDC said that 272,001 doses of the vaccine were administered as of Dec. 19. That means most people who were vaccinated did not experience negative effects.
The CDC has identified six case reports of anaphylaxis, or severe allergic reaction, that occurred following vaccination with the new vaccine, Clark reported. Other case reports were reviewed and determined not to be of anaphylaxis.
In an update on Friday, the agency stressed that anyone who has ever had a severe allergic reaction to any ingredient in a COVID-19 vaccine should not get that vaccine. People with severe allergic reactions to other vaccines should consult their doctor about getting the new vaccine while those with a history of anaphylaxis not related to vaccines “may still get vaccinated.”
“CDC recommends that people with a history of severe allergic reactions not related to vaccines or injectable medications - such as allergies to food, pet, venom, environmental, or latex - may still get vaccinated," the CDC said.
Anyone who experiences anaphylaxis after getting the first vaccine should not get the second shot, the CDC said. COVID-19 vaccines are meant to be given across two doses, spaced about three weeks apart."People with a history of allergies to oral medications or a family history of severe allergic reactions, or who might have a milder allergy to vaccines (no anaphylaxis) - may also still get vaccinated.”
At least five healthcare workers in Alaska experienced adverse reactions after getting the Pfizer vaccine, the Anchorage Daily News reported. One of two experiencing adverse reactions at the Bartlett Regional Hospital required treatment at the hospital for at least two nights.
An Illinois hospital halted vaccinations after four workers suffered adverse reactions.
Dr. Peter Marks, the director of Food and Drug Administration’s Center for Biologics Evaluation and Research, told reporters in a call on Thursday night that the agency is working with the CDC, and colleagues in the United Kingdom, on probing the allergic reactions.
“We’ll be looking at all of the data we can from each of these reactions to sort out exactly what happened. And we’ll also be looking to try to understand which components of the vaccine might be helping to produce them,” he said.
A container of 5 doses of COVID-19 vaccine sits on a table at Roseland Community Hospital in Chicago, Ill., on Dec. 18, 2020. (Scott Olson/Getty Images)
Noting that he was speculating, Marks said it’s known that polyethylene glycol - a component present in both the Pfizer vaccine and one from Moderna that regulators approved earlier in the day - can be associated, uncommonly, with allergic reactions.
“So that could be a culprit here. And that’s why we’ll be watching very closely,” he said. “But we just don’t know at this point.”
They go away after a day. According to the FDA website, the most commonly reported side effects include tiredness, headache, muscle pain, and chills. The agency said they go away after several days.Both vaccines have “systemic side effects,” which are “generally mild,” Marks said.
One volunteer in Pfizer’s late-stage clinical trial experienced an allergic reaction. Two people in Moderna’s phase 3 clinical trial experienced anaphylactic reactions, the company said during a meeting on Thursday. But the data showed the benefits outweigh the risk, FDA officials said, as they granted emergency use authorization to the vaccines about seven days apart.
People who get a COVID-19 vaccine should be monitored for at least 15 minutes after getting vaccinated, according to the CDC.
If someone experiences a severe allergic reaction against getting a COVID-19 vaccine, vaccination providers are supposed to provide rapid care and call for emergency medical services. The person should continue to be monitored in a medical facility for at least several hours.
marsh
On TB every waking moment
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
Scientists Warn UK COVID Mutation "Unlike Anything We Have Seen"; Cali Cases Near 2MM As Apple Closes Stores: Live Updates
SUNDAY, DEC 20, 2020 - 11:55
Summary:
- Allergic reactions prompt CDC investigation
- Global cases top 76MM
- UK alarmed at new mutations making virus more infectious
- Apple shuts California stores
- Scientists warn UK mutaiton "unlike anything we've seen"
- Poland announces holiday lockdown measures
- Italy sees decline in daily deaths
Like we noted last night, Boris Johnson has placed London (and parts of southeast England) on an even more restrictive lockdown as scientists have warned about a new mutated strain of SARS-CoV-2 - what the press and Health Secretary Matt Hancock have taken to calling "a new variant" - that's purportedly 70% more infectious than the original COVID-19
We're not epidemiologists, but that certainly sounds to us like a notable differentiation in the profile of the virus. Maybe even significantnt enough to prompt scientists to worry whether the conspicuously high efficacy numbers given for the Pfizer and Moderna vaccines might not apply to other strains of the virus.

After a nurse fainted on live TV upon being vaccinated with her first dose of the Pfizer vaccine, health authorities have received reports of at least six patients who went into anaphylactic shock after receiving the vaccine. That kind of an allergic reaction, which could be deadly, has been attributed to an ingrediant in the shot. According to the CDC, as of Dec. 18, 3,150 people reported what the agency terms "Health Impact Events" after getting vaccinated, most of which were less severe than the allergic reactions.
Meanwhile, one week after the first doses of the Pfizer vaccine were loaded on to trucks in Michigan, the newly-approved Moderna vaccine will begin distribution across the US starting Sunday, after a CDC panel recommended its use for people 18 and older. Unfortunately for all the last-minute shoppers in the Golden State, Apple is temporarily closing all of its retail stores in California as the COVID-19 pandemic continues to surge across the state. On Saturday, New York state’s case numbers etreated from the record set Friday. On Saturday, Moderna voted to recommend the vaccine to anyone age 18 and older.
On Sunday, as concerns about allergies erupted in the national press, the CDC acknowledged that it had been made aware of the allergic reactions to the vaccine, and would investigate, along with issuing new guidelines, about these and other "health-impact events". Events like these also occurred during the trials, though the link to the vaccines in each case was kept under wraps.

Circling back to the situation in the UK, the FT on Sunday published a lengthy feature where scientists commented on the data where the new viral "variant" is causing havoc. In the second paragraph, the reporter acknowledged the alarming speed of the mutations seen in the virus's genetic code.
The variant’s most remarkable feature is the number of mutations that have shaped it. Sir Patrick Vallance, the government’s chief scientific adviser, said 23 letters of the viral genetic code have changed, many of which are associated with the spike protein that the virus uses to get into human cells. Coronaviruses do not usually mutate so quickly, typically accumulating about two genetic changes per month.
After appearing in Kent in late September, the mutation was responsible for 28% of infections in London by early November and in the week ending Dec. 9 accounted for 62%."This new variant is very concerning, and is unlike anything we have seen so far in the pandemic," said Jeffrey Barrett, director of the Covid Genomics Initiative at the Wellcome Sanger Institute.
Yesterday, the government moved London and the surrounding area to "Tier 4" because of worries about the new strain.

UK PM Boris Johnson has pledged to give 350K people their first doses of the vaccine in two weeks. What's more, the UK drug regulator is expected to approve the AstraZeneca-Oxford vaccine before the end of the year, despite its flaws and the many questions surrounding the research.
Looking to the international numbers, cases passed 76MM as of Sunday morning, with deaths topping 1.6MM.
In the US, hospitalizations, deaths and new cases were all off their record highs from the past week.

Here's the latest news on the COVID-19 outbreak from overnight and Sunday morning.
- New York state reported 9.9K cases, the day after it set a record since the start of the pandemic of 12.7K new infections, Governor Andrew Cuomo said in statement. Hospitalizations and the positive-test rate fell slightly. The state reported more than 100 fatalities for the third consecutive day.
- California added 43.6K new Covid-19 cases yesterday, surpassing the 1.8MM mark, while deaths climbed by 272 for a total of 22,432, according to the health department’s website. The number of intensive-care unit beds in the state rose by 50 to 1.3K despite an increase in hospital admissions of 433 to 17.4K.
- France registered 17,565 new cases on Saturday, with the rolling seven-day average climbing for a fourth day to 13,605 cases, the highest in three weeks. The share of positive tests fell to 5.6% from 5.9% a day earlier. Deaths linked to the virus increased by 189 to 60,418, health authorities reported.
- Italy saw the number of daily deaths from coronavirus decline to 553 on Saturday against 674 the previous day. There were 16,308 new cases against 17,992 on Friday.
- Poland, which announced tough new lockdown measures for the holiday season, reported 11.3K new coronavirus cases on Saturday, compared with 11,013 on Friday. ;
- The Oxford-AstraZeneca Covid-19 vaccine is expected to be approved for use in the U.K. before the end of the year, the Telegraph reported, citing senior Whitehall sources.
We noted yesterday that India, despite successfully slowing the pace of its COVID-19 outbreak, has become the second country after the US to surpass the 10MM case mark. The world’s second most populous nation achieved the unwanted record on Saturday after notching 25,000 cases daily over the past week, down from a peak of almost 100,000 new infections per day in September. India has recorded more than 145K deaths from the virus, the third-highest tally after the US and Brazil. And in the most crowded urban slums, studies show that up to half the population has already developed COVID antibodies.
marsh
On TB every waking moment
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
2020: The Year We Let Ourselves Be Infantilised And Dehumanised
SATURDAY, DEC 19, 2020 - 23:30
Authored by Rob Slane via TheBlogMire.com,
Read Part 1 here...
I recently wrote a satirical speech by our Prime Minister, in which I imagined him coming up with all sorts of absurd rules for the Christmas season. It was really hard. Not because I was unable to come up with hundreds of such rules, were I minded to do so, but because the whole point of satire is to raise the absurdities up a step or two, in order to highlight the ridiculousness of what is happening. But how do you do this when the real-life absurdities have already been turned up to 11 on the amplifier? I kid you not when I tell you that my original list included a rule against playing certain board games over Christmas — which I rejected — only to see a few days later SAGE coming out and advising against the playing of board games.

We have now had nearly nine months of being treated like utter imbeciles. A once great country with a once free people has been reduced to the level of being governed by pathetic, childish slogans. And for some reason we have allowed ourselves to be infantilised.
I am utterly baffled as to how people can have sat through some of these slogans being introduced without responding with howls of laughter.
What on earth is this actually supposed to mean?“Stay Alert. Control the Virus. Save Lives.”
Stay Alert? For what? Are we supposed to be on our guard for a virus that is approximately 120 nanometres, or around 1,000th the width of a human hair? Are we to carry an electron microscope around with us wherever we go, just in case? One of my favourite signs is an electronic one I sometimes see on my occasional drives into the office. On one day, it says, “Stay Alert. Control the Virus.” On another, it says, “Stay Alert. Watch out for Cyclists.” It should be noted that cyclists are considerably bigger than 120nm and even often wearing the kind of hi-vis jackets that coronaviruses refuse to wear.
Control the Virus? Say what? You mean they actually think we’re stupid enough to think they’re clever enough to devise schemes that can actually control those little invisible 120 nm virus particles that are in the air and on surfaces. Apparently so.
Save Lives? I am yet to hear a convincing argument as to how I and my family, not having any symptoms and thus not being infected by the virus, can possibly stop the spread of said virus that we don’t have by staying at home or wearing a piece of cloth over or respiratory passages, such that we save lives.
More recently, it has been decided that the slogans were maybe a bit too high-brow and needed to be simplified further, this time into monosyllables: “Hands. Face. Space.”
Although I tend to avoid watching Comrade Johnson and Co as they spout this nonsense at their regular stand-ups, on the occasions when I have had that misfortune, it has felt eerily like suddenly being thrust into the world’s largest Kindergarten with teacher talking down to his little charges as if they were really, really stupid.
I won’t sport with your intelligence by mentioning all the other mind-numbing slogans we’ve been fed this year, suffice it to say that phrases such as “social bubble” and “Covid-secure” would be deeply funny were it not for the seriousness of the situation into which those coming up with such tripe have placed us (as an aside, are such buildings for which it is claimed that they are “Covid-secure” also “Flu-Secure” and “Cold-Secure”?)
But the infantilising of an entire population is by no means the worst thing they have done to us. Worse by far has been the dehumanising of millions of people, which has been done via a number of enormously destructive methods.
Chief of them is the idea that we must all avoid each other. I cannot even begin to think how destructive this has become. In a normal society, if you or I have symptoms of a particularly nasty seasonal respiratory illness, which is what Covid-19 is, we would avoid one another.
Obviously. But the idea of perfectly healthy people avoiding other perfectly healthy people must qualify as one of the most absurd concepts ever dreamt up. Not only is it self-evidently unnecessary, it is bound to have long-terms consequences for the way we view one another, the way we relate to one another, the way we behave around one another. It turns us from seeing one another as humans, made in the Image of God, to walking virus carriers and a potential risk. Some people now literally behave as if they are navigating their way through a crowd of potential terrorists, rather than simply walking through a group of fellow humans.
People avoidance is not just deeply destructive from a psychological and social perspective, it is also deeply cruel. The idea that a grandparent cannot have contact with their children or grandchildren is just obscene. And the very thought of the elderly being left to fester away in care homes, rather than being allowed contact with their families is sick. Yet that’s what we’ve done, or allowed to be done.
And of course, I cannot leave off talking about dehumanisation without mentioning masks. These wretched things were introduced in the Summer, long after the epidemic had waned, at a time when they could not possibly have done any good, even if they had been capable of doing any good. Why were they introduced? Partly to keep the fear-narrative going, even though there was extraordinarily little risk of dying of a seasonal respiratory virus at that time of the year. But even more important, they are a sign of submission. They are a, “we can do with you what we like moment.” They are nothing to do with health. They are a psychological mask, and even more than the social distancing, they have served to alter the way we see one another and are seen by others.
Millions of people humiliated by the Marketing Team of Covid-19 and their infantile slogans. Millions of people dehumanised by having their faces, their smiles, their laughter, their thoughtfulness etc covered to make them into expressionless drones. That was the year we just lived through. Will 2021 be the year a critical mass try to escape the Kindergarten and return to being human?
marsh
On TB every waking moment
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
China To Vaccinate 50MM People Before Lunar New Year
SATURDAY, DEC 19, 2020 - 23:00
Although China hasn't reported any numbers related to its internal plans to vaccinate its population (which, at 1.4BN, won't exactly be a walk in the park), there have been reports claiming Beijing has already vaccinated at least 1MM people as part of its "emergency" vaccination plans.

Meanwhile, in China, the CCP will focus first on vaccinating health-care workers - or at least those who haven't already been infected or vaccinated (anybody who tries refusing the vaccine in China, well, good luck) - before moving on to other high-risk industries. But in terms of numbers, China plans to inoculate 50 million people with two experimental jabs before February’s Lunar New Year holiday season, leading up to vaccinations for the broader public by spring, people familiar with the matter said.
That's even faster than the forecasts published by Goldman Sachs and other Wall Street banks.
Chinese health officials have discussed rolling out vaccinations in two batches before Jan. 15 and Feb. 5 in a conference call earlier this week, according to WSJ's anonymous sources.
Officials from the National Health Commission held a call with local municipal officials on Tuesday, ordering them to start implementing plans for mass vaccinations. China expects to produce about 600MM doses by the end of the year, most of which will likely be exported, according to WSJ (not exactly a vote of confidence in SinoVac).
Of course, China has agreements with drug companies, even as its homemade drugs are being doled out to even poorer countries.

Still, in China, authorities are reviewing clinical data for the homegrown vaccines and close to approving them for use by the Chinese public, health officials and industry experts said.
The 100 million doses to be doled out in the coming weeks are part of the country’s emergency plan, because they would only be administered to people considered to be at high risk of infection, according to one person close to the matter. At two doses per person, the vaccinations would cover 50 million recipients.
The central province of Sichuan said this month that it has already received more than 100K doses of Chinese vaccines, and that it plans to inoculate more than 2MM people by the end of the year, according to its official Weibo social messaging account and a statement on its website. Central Hunan province plans to begin emergency vaccinations as early as the end of this year, the government said in a statement online.
marsh
On TB every waking moment
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
California Reports Record COVID Cases And Deaths... Despite Strictest Lockdown
SATURDAY, DEC 19, 2020 - 22:30
Authored by Jon Miltimore via The Foundation for Economic Education,
On December 4, a bipartisan group of California legislators sent Gov. Gavin Newsom a letter urging him to reconsider his order closing outdoor playgrounds as part of his regional stay-at-home order.
“While we must appropriately consider best practices to reduce the risk of COVID-19 transmission, we also must ensure the children across the state are not unfairly deprived of their opportunities for outdoor access and play,” the legislators wrote.

Newsom’s order closing outdoor playgrounds—a response many see as senseless and ineffective, which prompted the governor to rescind it—is just one example of the hardline approach California public officials have taken in their attempt to mitigate the spread of the coronavirus.

Other restrictions include a 10 p.m. curfew, bans on outdoor dining and religious gatherings, as well as school closures. Surveys in recent months have shown California’s restrictions are some of the strictest in the US.
Sadly, but perhaps predictably, the regulations do not appear to be working. State data show California is smashing its previous highs in both COVID-19 cases and deaths.
To put these numbers into perspective, the number of deaths California reported on Wednesday was more than double the daily high in any previous month.“California broke its statewide records for both coronavirus cases reported and deaths reported in a single day on Wednesday,” The Hill reports.
“The state reported 51,724 COVID-19 cases on Wednesday, breaking the previous record of 42,088 cases, which was just set on Monday, according to a Los Angeles Times tally.”

California is hardly the only state suffering from a sharp rise in COVID-19 mortality. But the figures reinforce emerging evidence that suggests lockdowns and other government restrictions are doing little to tame the coronavirus.
As I recently noted, an abundance of academic research suggests there is little to no correlation between lockdown stringency and COVID mortality rates. This includes a study published on July 21 in The Lancet, research from Tel Aviv University published in October, and a study published in Frontiers in Public Health in November.
‘I’m Not Sure We Know What We’re Doing’
Newsom’s decision to reimpose lockdowns in light of the evidence we have today has left some California public officials puzzled.
"During the first Shelter in Place order, which I wholeheartedly endorsed, the virus was brand new and had the capability of spreading exponentially due to zero immunity and people's complete lack of awareness," San Mateo County Health Officer Scott Morrow recently observed on the county’s website.
Morrow implied that many of the actions being taken suggest California officials have learned little since the spring.“[That order] was very much consistent with my long-held views about the judicious use of power.…However, I very quickly rescinded my initial orders shuttering society and focused my new orders on the personal behaviors that are driving the pandemic… .”
Morrow was blunt in his appraisal of the restrictions being imposed across the Golden State.“Just because one has the legal authority to do something, doesn't mean one has to use it, or that using it is the best course of action,” he wrote.
“What I believed back in May, and what I believe now, is the power and authority to control this pandemic lies primarily in your hands, not mine."
“I’m not sure we know what we’re doing,” he wrote. “I look at surrounding counties who have been much more restrictive than I have been, and wonder what it’s bought them.”


Morrow appears to have gleaned an insight once observed by the economist Milton Friedman.
With every passing week the results of government lockdowns become more clear. They cause tremendous and widespread harms—no one disagrees on this point—but the supposed benefits of the policies remain tenuous. Despite the bevy of evidence they possess, lawmakers continue to embrace restrictions because of bad incentives.“One of the great mistakes is to judge policies and programs by their intentions rather than their results,” Friedman famously observed.
The Costs of Abandoning Freedom
The great economist Ludwig von Mises noted long ago that a great deal of modern social conflict is a struggle over who gets to design the world, individuals or authorities. Mises believed that individuals, if left to their own devices, would generally make rational decisions based on their own self interest. This is why he saw few things as dangerous as central planners who seek to supplant individual planning with their own (despite their knowledge limitations) in an effort to create a more perfect society.
The Washington Post reported yesterday that nearly 8 million Americans have slipped into poverty since summer. When one considers the damage government lockdowns have wrought compared to the positive results they’ve achieved, one begins to see why Mises saw the unchecked power of authorities as such a threat.“The planner is a potential dictator who wants to deprive all other people of the power to plan and act according to their own plans,” Mises wrote in Socialism: An Economic and Sociological Analysis.
“He aims at one thing only: the exclusive absolute pre-eminence of his own plan.”
marsh
On TB every waking moment

Rand Paul Blisters Fauci — ‘Masks Are All About Submission’…
MARLOW: You have a terrific speech … and you started with something that I wasn’t anticipating, but I absolutely loved, and that’s some actual science about the mask mandates. You broke it d…
www.citizenfreepress.com
Rand Paul Blisters Fauci — ‘Masks Are All About Submission’…
Posted by Kane on December 20, 2020 3:24 pm
2:42 min
MARLOW: You have a terrific speech … and you started with something that I wasn’t anticipating, but I absolutely loved, and that’s some actual science about the mask mandates. You broke it down in a very clear way. Talk to us about it.
PAUL: It’d be one thing if we were told you have to give up your liberty, you have to give up your freedom, we’re going to save your life. But what if you have to give up all your freedoms and they’re wrong on the science?
Every one of the mandates — and you look in country after country, state after state — you look at when the mask mandates went in — the incidents went up exponentially after the mandates. Restaurants, nobody can eat in a restaurant, there’s no science behind any of that.
Middle seat missing on the airplane, you really think you’re like 12 inches from the other guy instead of six inches, it really makes a difference? None of it really makes any sense, and there’s no epidemiological evidence. You know, it’s like, ‘Wash your hands, stand six feet apart.’
There’s no evidence that that slowed down the [spread]. … The trajectory of the virus hasn’t been altered at all by any of these things. I think the vaccine will, and this is why I really despise people like the CNN Doctor [Sanjay] Gupta, who I think is committing television malpractice by saying, ‘Oh, your mask is a much better thing than the vaccine.’ Well, no, it isn’t. The masks aren’t working at all. The thing’s going through the roof and people are dying. Why would you want to discourage someone from taking a vaccine and say, ‘Oh wear the mask.’?
And the masks are different, too. The N95 mask actually does work to a certain extent, if worn properly and used [with] sterile technique. In the hospital, our doctors — I have a brother and sister who are doctors, they wear the N95 mask, and it’s kept them from getting infected — but there’s no value to the cloth mask, at all. It’s like wearing your underwear. You might as well cut your underwear up and wear your underwear as protection. It doesn’t work.
MARLOW: That’s why I call it a face diaper. So you’ve got a public who has accepted this, though, by and large, because we’ve been told by everyone we have to accept it. Have we lost track of the Constitution? Have we forgotten about the Constitution?
PAUL: Well, that’s why I like this youth group here. What are they asked to give up? They’re being asked to give up their graduation from high school, their graduation from college, their wedding, and if we’re not careful, it’s gonna be their five-year wedding anniversary or their ten-year anniversary. We’re still gonna be wearing masks.
Paul highlighted Director of the National Institute of Allergy and Infectious Diseases Dr. Anthony Fauci’s ongoing advocacy for mask-wearing as a protective measure for public health.
“If Fauci has his way, you’ll never give up on the mask,” warned Paul. “It’s all about submission. They want you to submit to their will, whether there’s any science. In fact, like on schools, I’ve been telling Fauci for six months, the evidence is that if you open schools, you will not get a surge. The whole world accepts it, except for Dr. Fauci. He finally accepted it last week, six months after I started showing him the evidence.”
marsh
On TB every waking moment

6 severe allergic reactions reported from more than 250K COVID-19 vaccine shots
The half-dozen cases of allergic reaction were reported as of Friday night and included one person with a history of vaccination reactions.
 www.wcvb.com
www.wcvb.com
6 severe allergic reactions reported from more than 250K COVID-19 vaccine shots
1K Shares

1:25 min video on website
TRANSCRIPT:
that concludes the vote. It looks like we have a favorable vote. An advisory panel is now recommending emergency use authorization of a second coronavirus vaccine in the United States. Madonna's Cove in 19 vaccine could be hitting arms across the country as soon as Monday. It looks to be roughly 95% effective at preventing disease, including 100% effective it's severe disease, about 95% effective in preventing disease and people who are over 65 across different ethnic backgrounds. Racial backgrounds This is confusion stirs surrounding distribution of the Pfizer vaccine, with states being told by the federal government that they will receive fewer doses next week. The White House says shipments are being held back for the second dose. The Pfizer vaccine goes out into shipments. So half of the vaccines are 2.9 million going out this week. Another 2.9 million would be held back for the second dose for those patients to receive in 21 to 28 days. Now, with the nation facing its deadliest day since the beginning of the pandemic on Wednesday, the stress of constantly being surrounded by death day after day is taking a serious toll on health care workers on the front lines. We're already seeing a lot of PTSD like symptoms on, especially the bedside providers, both physicians and nurses. As the waves continue, I'm Melissa Raney reporting.
_____________________
U.S. health officials closely tracking possible side effects of the first authorized COVID-19 vaccine say they have seen six cases of severe allergic reaction out of more than a quarter million shots given.
The Centers for Disease Control and Prevention said more than 272,000 shots of the Pfizer vaccine were given nationwide as of Saturday morning. The half-dozen cases of allergic reaction were reported as of Friday night, and included one person with a history of vaccination reactions.
Health officials are keeping close watch for such side effects.
U.S. vaccine recipients are supposed to hang around after their injections in case signs of an allergy appear. The CDC says all cases occurred within the recommended observation window and were promptly treated.
U.S. health officials closely tracking possible side effects of the first authorized COVID-19 vaccine say they have seen six cases of severe allergic reaction out of more than a quarter million shots given.
The Centers for Disease Control and Prevention said more than 272,000 shots of the Pfizer vaccine were given nationwide as of Saturday morning. The half-dozen cases of allergic reaction were reported as of Friday night, and included one person with a history of vaccination reactions.
Health officials are keeping close watch for such side effects.
The numbers were discussed at a meeting of a committee that advises the CDC on vaccines. The group on Saturday endorsed Moderna’s COVID-19 vaccine, which was granted emergency authorization on Friday.
Less severe side effects have also been rare. Among the first 215,000 people to get vaccinated in the U.S., fewer than 1.5% of them had problems that left them unable to perform their normal activities or required medical care.
Many vaccines can cause temporary discomfort, such as a sore arm or certain flu-like symptoms. COVID-19 vaccines tend to cause more of those reactions than a flu shot, and some hospitals are staggering the times their employees get vaccinated to avoid staffing problems.
The numbers were discussed at a meeting of a committee that advises the CDC on vaccines. The group on Saturday endorsed Moderna’s COVID-19 vaccine, which was granted emergency authorization on Friday.

Last edited:
marsh
On TB every waking moment

GOP congressman says he’s more worried about COVID-19 vaccine than disease itself
GOP Rep. Ken Buck (Colo.) this week said he will not be taking the coronavirus vaccine, explaining that he is “more concerned about the safety of the vaccine” than the “side effects of the disease.…
 thehill.com
thehill.com
BY CELINE CASTRONUOVO - 12/19/20 12:56 PM EST 697
5,910
GOP Rep. Ken Buck (Colo.) this week said he will not be taking the coronavirus vaccine, explaining that he is “more concerned about the safety of the vaccine” than the “side effects of the disease.”
“It is my choice,” Buck told Fox Business host Neil Cavuto on Friday. “I’m an American and I have the freedom to decide if I’m going to take a vaccine or not and, in this case, I’m not going to take the vaccine.”
The comments come as both health officials and social media companies alike are attempting to combat misinformation on the safety of the vaccine, with health experts saying that at least 70 percent of the country needs to be vaccinated in order to achieve herd immunity and end the outbreak that has infected more than 17.4 million Americans and killed more than 300,000.
However, Buck said on Friday, “I’m more concerned about the safety of the vaccine than I am the side effects of the disease.”
“I’m a healthy person and I think most Americans are healthy,” the 61-year-old GOP congressman continued. “I think what we should do is we should focus on the at-risk populations in America, make sure those are the people that get this vaccine first. Make sure that the health care workers who want the vaccine get the vaccine as soon as possible.
“But, I am not going to take a vaccine,” Buck repeated.
“I think it is one of those issues that Americans have to make that decision for themselves and I hope that we don’t get to the point where either corporations or the government are requiring this vaccine. I think that is a terrible mistake in this country,” he added.
Buck tweeted on Friday that the coronavirus vaccine is "an incredible feat that should be applauded," adding that he encourages "frontline workers, healthcare professionals, and at-risk populations to get the vaccine" first and that "members of Congress should not get special treatment."
A spokesperson for Buck reiterated these sentiments in a statement to The Hill Saturday, writing that Buck "doesn’t think that members of Congress should skip the line and receive the vaccine before our front line workers."
"He encourages those at risk to get the vaccine immediately," the spokesperson added.
Health care workers and politicians this week started receiving the first doses of the Pfizer and BioNTech vaccine, which final data showed to be 95 percent effective at preventing COVID-19.
Both House Speaker Nancy Pelosi (D-Calif.) and Senate Majority Leader Mitch McConnell (R-Ky.) received the vaccine Friday.
"Just received the safe, effective COVID vaccine following continuity-of-government protocols. Vaccines are how we beat this virus," McConnell tweeted.
Earlier on Friday, Vice President Pence was vaccinated on camera. President-elect Biden">Joe Biden is expected to publicly receive the vaccine on Monday.
House Minority Leader Kevin McCarthy (R-Calif.) said Friday that he expects to get vaccinated soon, as well.
- Surgeon general: Immigration status should not be barrier to...
- CDC panel recommends people 75 and older, certain front-line...
Anthony Fauci, the country's top infectious diseases doctor, said in a Dec. 15 NPR interview that as many people as possible should get a coronavirus vaccine, adding that “it would be terrible, with a tool as good as that, if people don't utilize that tool.”
marsh
On TB every waking moment

EEOC guidance: Yes, employers can require the COVID-19 vaccine
The Equal Employment Opportunity Commission has determined that employers can require workers to get vaccinated against COVID-19 and offered guidance on exceptions. Employers have been hoping for c…
 www.chicagotribune.com
www.chicagotribune.com
EEOC guidance: Yes, employers can require the COVID-19 vaccine
By ALEXIA ELEJALDE-RUIZ
CHICAGO TRIBUNE |
DEC 17, 2020 AT 1:36 PM
/cloudfront-us-east-1.images.arcpublishing.com/tronc/NPMAHTNLOBBJNNWEBCDGX4QBWE.jpg)
Lorna Herrera, of Mundelein, cheers after getting the COVID-19 vaccination from Gina Gallagher at Amita Health St. Alexius Medical Center on Dec. 18, 2020, in Hoffman Estates. Herrera works in housekeeping and cleaned the hospital room of the first COVID-19 patient in Illinois. (Stacey Wescott / Chicago Tribune)
The Equal Employment Opportunity Commission has determined that employers can require workers to get vaccinated against COVID-19 and offered guidance on exceptions.
Employers have been hoping for clarity from the agency as they mull whether to mandate vaccination even as many people remain concerned about the safety of a vaccine developed so quickly and not tested on certain populations.
The guidelines, published Wednesday, mostly confirm what attorneys have been advising clients as vaccines begin to be distributed.
In essence, the EEOC said employers can require that employees get inoculated as a condition of going to work, unless an employee declines because of a disability or a sincerely held religious belief.

Nicole Costa, pharmacy manager at Amita Health Presence Medical Center in Joliet, prepares the COVID-19 vaccine to be administered to medical personnel on Dec. 16, 2020. (Zbigniew Bzdak / Chicago Tribune)
In such cases, the employer must offer a reasonable accommodation to the employee, such as working remotely, as long as the accommodation doesn’t cause “undue hardship” for the employer. If there is no accommodation possible, then an employer may prohibit the employee from entering the premises but not necessarily fire the worker. The employer must see if the employee has any other rights under federal or local laws, including the ability to take unpaid leave under the Family and Medical Leave Act.
Under the Americans with Disabilities Act, before an employer can exclude a worker from the physical worksite, the employer must determine if the unvaccinated employee presents a significant risk in harm to health or safety that cannot be eliminated or reduced through reasonable accommodations.
The EEOC also clarified the applicability of certain laws to COVID-19 vaccine mandates. Vaccination, it says, does not constitute a “medical examination” under the ADA that would require an employer show “it is job-related or consistent with business necessity.”
However, the Centers for Disease Control and Prevention recommends asking screening questions before administering a vaccine to ensure there is no medical reason that would prevent a person from receiving it, and that is a “medical inquiry” that would have to meet the “business necessity” standard. That doesn’t apply if the vaccine is voluntary or if a third-party provider without a contract with the employer, like a pharmacy, administers the vaccine.
“In other words, an employer can avoid this standard if it requires employees to get vaccinated through their own means — going to a pharmacy or a primary care physician,” said Nathaniel Glasser, an attorney with Epstein Becker Green who represents employers.
Employers can ask workers if they have received the vaccine without implicating the ADA or the Genetic Information Nondiscrimination Act.
The complete guidance can be found here.
jward
passin' thru
Josh Caplan
@joshdcaplan
1h
TELEGRAPH: Tier 4 restrictions could remain in place until Easter, U.K. government admits
@joshdcaplan
1h
TELEGRAPH: Tier 4 restrictions could remain in place until Easter, U.K. government admits
jward
passin' thru


marsh
On TB every waking moment
WOAH: 25 BRAND NEW Studies Completely DISCREDIT Dr. Fauci
The Daily Fodder is a news website focused on news, nothing more.
WOAH: 25 BRAND NEW Studies Completely DISCREDIT Dr. Fauci
American Institute For Economic Research-December 19, 2020
The use of universal lockdowns in the event of the appearance of a new pathogen has no precedent. It has been a science experiment in real time, with most of the human population used as lab rats. The costs are legion.
The question is whether lockdowns worked to control the virus in a way that is scientifically verifiable. Based on the following studies, the answer is no and for a variety of reasons: bad data, no correlations, no causal demonstration, anomalous exceptions, and so on. There is no relationship between lockdowns (or whatever else people want to call them to mask their true nature) and virus control.
Perhaps this is a shocking revelation, given that universal social and economic controls are becoming the new orthodoxy. In a saner world, the burden of proof really should belong to the lockdowners, since it is they who overthrew 100 years of public-health wisdom and replaced it with an untested, top-down imposition on freedom and human rights. They never accepted that burden. They took it as axiomatic that a virus could be intimidated and frightened by credentials, edicts, speeches, and masked gendarmes.
The pro-lockdown evidence is shockingly thin, and based largely on comparing real-world outcomes against dire computer-generated forecasts derived from empirically untested models, and then merely positing that stringencies and “nonpharmaceutical interventions” account for the difference between the fictionalized vs. the real outcome. The anti-lockdown studies, on the other hand, are evidence-based, robust, and thorough, grappling with the data we have (with all its flaws) and looking at the results in light of controls on the population.
Much of the following list has been put together by data engineer Ivor Cummins, who has waged a year-long educational effort to upend intellectual support for lockdowns. AIER has added its own and the summaries. The upshot is that the virus is going to do as viruses do, same as always in the history of infectious disease. We have extremely limited control over them, and that which we do have is bound up with time and place. Fear, panic, and coercion are not ideal strategies for managing viruses. Intelligence and medical therapeutics fare much better.
(These studies are focused only on lockdown and their relationship to virus control. They do not get into the myriad associated issues that have vexed the world such as mask mandates, PCR-testing issues, death misclassification problem, or any particular issues associated with travel restrictions, restaurant closures, and hundreds of other particulars about which whole libraries will be written in the future.)
1. “A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes” by Rabail Chaudhry, George Dranitsaris, Talha Mubashir, Justyna Bartoszko, Sheila Riazi. EClinicalMedicine 25 (2020) 100464. “[F]ull lockdowns and wide-spread COVID-19 testing were not associated with reductions in the number of critical cases or overall mortality.”
2. “Was Germany’s Corona Lockdown Necessary?” by Christof Kuhbandner, Stefan Homburg, Harald Walach, Stefan Hockertz. Advance: Sage Preprint, June 23, 2020. “Official data from Germany’s RKI agency suggest strongly that the spread of the coronavirus in Germany receded autonomously, before any interventions became effective. Several reasons for such an autonomous decline have been suggested. One is that differences in host susceptibility and behavior can result in herd immunity at a relatively low prevalence level. Accounting for individual variation in susceptibility or exposure to the coronavirus yields a maximum of 17% to 20% of the population that needs to be infected to reach herd immunity, an estimate that is empirically supported by the cohort of the Diamond Princess cruise ship. Another reason is that seasonality may also play an important role in dissipation.”
3. “Estimation of the current development of the SARS-CoV-2 epidemic in Germany” by Matthias an der Heiden, Osamah Hamouda. Robert Koch-Institut, April 22, 2020. “In general, however, not all infected people develop symptoms, not all those who develop symptoms go to a doctor’s office, not all who go to the doctor are tested and not all who test positive are also recorded in a data collection system. In addition, there is a certain amount of time between all these individual steps, so that no survey system, no matter how good, can make a statement about the current infection process without additional assumptions and calculations.”
4. Did COVID-19 infections decline before UK lockdown? by Simon N. Wood. Cornell University pre-print, August 8, 2020. “A Bayesian inverse problem approach applied to UK data on COVID-19 deaths and the disease duration distribution suggests that infections were in decline before full UK lockdown (24 March 2020), and that infections in Sweden started to decline only a day or two later. An analysis of UK data using the model of Flaxman et al. (2020, Nature 584) gives the same result under relaxation of its prior assumptions on R.”
5. “Comment on Flaxman et al. (2020): The illusory effects of non-pharmaceutical interventions on COVID-19 in Europe” by Stefan Homburg and Christof Kuhbandner. June 17, 2020. Advance, Sage Pre-Print. “In a recent article, Flaxman et al. allege that non-pharmaceutical interventions imposed by 11 European countries saved millions of lives. We show that their methods involve circular reasoning. The purported effects are pure artefacts, which contradict the data.
Moreover, we demonstrate that the United Kingdom’s lockdown was both superfluous and ineffective.”
6. Professor Ben Israel’s Analysis of virus transmission. April 16, 2020. “Some may claim that the decline in the number of additional patients every day is a result of the tight lockdown imposed by the government and health authorities. Examining the data of different countries around the world casts a heavy question mark on the above statement. It turns out that a similar pattern – rapid increase in infections that reaches a peak in the sixth week and declines from the eighth week – is common to all countries in which the disease was discovered, regardless of their response policies: some imposed a severe and immediate lockdown that included not only ‘social distancing’ and banning crowding, but also shutout of economy (like Israel); some ‘ignored’ the infection and continued almost a normal life (such as Taiwan, Korea or Sweden), and some initially adopted a lenient policy but soon reversed to a complete lockdown (such as Italy or the State of New York). Nonetheless, the data shows similar time constants amongst all these countries in regard to the initial rapid growth and the decline of the disease.”
7. “Impact of non-pharmaceutical interventions against COVID-19 in Europe: a quasi-experimental study” by Paul Raymond Hunter, Felipe Colon-Gonzalez, Julii Suzanne Brainard, Steve Rushton. MedRxiv Pre-print May 1, 2020. “The current epidemic of COVID-19 is unparalleled in recent history as are the social distancing interventions that have led to a significant halt on the economic and social life of so many countries. However, there is very little empirical evidence about which social distancing measures have the most impact… From both sets of modelling, we found that closure of education facilities, prohibiting mass gatherings and closure of some non-essential businesses were associated with reduced incidence whereas stay at home orders and closure of all non-businesses was not associated with any independent additional impact.”
8. “Full lockdown policies in Western Europe countries have no evident impacts on the COVID-19 epidemic” by Thomas Meunier. MedRxiv Pre-print May 1, 2020. “This phenomenological study assesses the impacts of full lockdown strategies applied in Italy, France, Spain and United Kingdom, on the slowdown of the 2020 COVID-19 outbreak. Comparing the trajectory of the epidemic before and after the lockdown, we find no evidence of any discontinuity in the growth rate, doubling time, and reproduction number trends. Extrapolating pre-lockdown growth rate trends, we provide estimates of the death toll in the absence of any lockdown policies, and show that these strategies might not have saved any life in western Europe. We also show that neighboring countries applying less restrictive social distancing measures (as opposed to police-enforced home containment) experience a very similar time evolution of the epidemic.”
9. “Trajectory of COVID-19 epidemic in Europe” by Marco Colombo, Joseph Mellor, Helen M Colhoun, M. Gabriela M. Gomes, Paul M McKeigue. MedRxiv Pre-print. Posted September 28, 2020. “The classic Susceptible-Infected-Recovered model formulated by Kermack and McKendrick assumes that all individuals in the population are equally susceptible to infection.
From fitting such a model to the trajectory of mortality from COVID-19 in 11 European countries up to 4 May 2020 Flaxman et al. concluded that ‘major non-pharmaceutical interventions — and lockdowns in particular — have had a large effect on reducing transmission’. We show that relaxing the assumption of homogeneity to allow for individual variation in susceptibility or connectivity gives a model that has better fit to the data and more accurate 14-day forward prediction of mortality. Allowing for heterogeneity reduces the estimate of ‘counterfactual’ deaths that would have occurred if there had been no interventions from 3.2 million to 262,000, implying that most of the slowing and reversal of COVID-19 mortality is explained by the build-up of herd immunity. The estimate of the herd immunity threshold depends on the value specified for the infection fatality ratio (IFR): a value of 0.3% for the IFR gives 15% for the average herd immunity threshold.”
10. “Effect of school closures on mortality from coronavirus disease 2019: old and new predictions” by Ken Rice, Ben Wynne, Victoria Martin, Graeme J Ackland. British Medical Journal, September 15, 2020. “The findings of this study suggest that prompt interventions were shown to be highly effective at reducing peak demand for intensive care unit (ICU) beds but also prolong the epidemic, in some cases resulting in more deaths long term. This happens because covid-19 related mortality is highly skewed towards older age groups. In the absence of an effective vaccination programme, none of the proposed mitigation strategies in the UK would reduce the predicted total number of deaths below 200 000.”
11. “Modeling social distancing strategies to prevent SARS-CoV2 spread in Israel- A Cost-effectiveness analysis” by Amir Shlomai, Ari Leshno, Ella H Sklan, Moshe Leshno. MedRxiv Pre-Print. September 20, 2020. “A nationwide lockdown is expected to save on average 274 (median 124, interquartile range (IQR): 71-221) lives compared to the ‘testing, tracing, and isolation’ approach. However, the ICER will be on average $45,104,156 (median $ 49.6 million, IQR: 22.7-220.1) to prevent one case of death. Conclusions: A national lockdown has a moderate advantage in saving lives with tremendous costs and possible overwhelming economic effects. These findings should assist decision-makers in dealing with additional waves of this pandemic.”
12. Too Little of a Good Thing A Paradox of Moderate Infection Control, by Ted Cohen and Marc Lipsitch. Epidemiology. 2008 Jul; 19(4): 588–589. “The link between limiting pathogen exposure and improving public health is not always so straightforward. Reducing the risk that each member of a community will be exposed to a pathogen has the attendant effect of increasing the average age at which infections occur. For pathogens that inflict greater morbidity at older ages, interventions that reduce but do not eliminate exposure can paradoxically increase the number of cases of severe disease by shifting the burden of infection toward older individuals.”
Part 1 of 2
marsh
On TB every waking moment
Part 2 of 2
13. “Smart Thinking, Lockdown and COVID-19: Implications for Public Policy” by Morris Altman. Journal of Behavioral Economics for Policy, 2020. “The response to COVID-19 has been overwhelmingly to lockdown much of the world’s economies in order to minimize death rates as well as the immediate negative effects of COVID-19. I argue that such policy is too often de-contextualized as it ignores policy externalities, assumes death rate calculations are appropriately accurate and, and as well, assumes focusing on direct Covid-19 effects to maximize human welfare is appropriate. As a result of this approach current policy can be misdirected and with highly negative effects on human welfare. Moreover, such policies can inadvertently result in not minimizing death rates (incorporating externalities) at all, especially in the long run. Such misdirected and sub-optimal policy is a product of policy makers using inappropriate mental models which are lacking in a number of key areas; the failure to take a more comprehensive macro perspective to address the virus, using bad heuristics or decision-making tools, relatedly not recognizing the differential effects of the virus, and adopting herding strategy (follow-the-leader) when developing policy. Improving the decision-making environment, inclusive of providing more comprehensive governance and improving mental models could have lockdowns throughout the world thus yielding much higher levels of human welfare.”
14. “SARS-CoV-2 waves in Europe: A 2-stratum SEIRS model solution” by Levan Djaparidze and Federico Lois. MedRxiv pre-print, October 23, 2020. “We found that 180-day of mandatory isolations to healthy <60 (i.e. schools and workplaces closed) produces more final deaths if the vaccination date is later than (Madrid: Feb 23 2021; Catalonia: Dec 28 2020; Paris: Jan 14 2021; London: Jan 22 2021). We also modeled how average isolation levels change the probability of getting infected for a single individual that isolates differently than average. That led us to realize disease damages to third parties due to virus spreading can be calculated and to postulate that an individual has the right to avoid isolation during epidemics (SARS-CoV-2 or any other).”
15. “Did Lockdown Work? An Economist’s Cross-Country Comparison” by Christian Bjørnskov. SSRN working paper, August 2, 2020. “The lockdowns in most Western countries have thrown the world into the most severe recession since World War II and the most rapidly developing recession ever seen in mature market economies. They have also caused an erosion of fundamental rights and the separation of powers in a large part of the world as both democratic and autocratic regimes have misused their emergency powers and ignored constitutional limits to policy-making (Bjørnskov and Voigt, 2020). It is therefore important to evaluate whether and to which extent the lockdowns have worked as officially intended: to suppress the spread of the SARS-CoV-2 virus and prevent deaths associated with it. Comparing weekly mortality in 24 European countries, the findings in this paper suggest that more severe lockdown policies have not been associated with lower mortality. In other words, the lockdowns have not worked as intended.”
16.”Four Stylized Facts about COVID-19” (alt-link) by Andrew Atkeson, Karen Kopecky, and Tao Zha. NBER working paper 27719, August 2020. “One of the central policy questions regarding the COVID-19 pandemic is the question of which non-pharmeceutical interventions governments might use to influence the transmission of the disease. Our ability to identify empirically which NPI’s have what impact on disease transmission depends on there being enough independent variation in both NPI’s and disease transmission across locations as well as our having robust procedures for controlling for other observed and unobserved factors that might be influencing disease transmission. The facts that we document in this paper cast doubt on this premise…. The existing literature has concluded that NPI policy and social distancing have been essential to reducing the spread of COVID-19 and the number of deaths due to this deadly pandemic. The stylized facts established in this paper challenge this conclusion.”
17. “How does Belarus have one of the lowest death rates in Europe?” by Kata Karáth. British Medical Journal, September 15, 2020. “Belarus’s beleaguered government remains unfazed by covid-19. President Aleksander Lukashenko, who has been in power since 1994, has flatly denied the seriousness of the pandemic, refusing to impose a lockdown, close schools, or cancel mass events like the Belarusian football league or the Victory Day parade. Yet the country’s death rate is among the lowest in Europe—just over 700 in a population of 9.5 million with over 73 000 confirmed cases.”
18. “Association between living with children and outcomes from COVID-19: an OpenSAFELY cohort study of 12 million adults in England” by Harriet Forbes, Caroline E Morton, Seb Bacon et al., by MedRxiv, November 2, 2020. “Among 9,157,814 adults ≤65 years, living with children 0-11 years was not associated with increased risks of recorded SARS-CoV-2 infection, COVID-19 related hospital or ICU admission but was associated with reduced risk of COVID-19 death (HR 0.75, 95%CI 0.62-0.92). Living with children aged 12-18 years was associated with a small increased risk of recorded SARS-CoV-2 infection (HR 1.08, 95%CI 1.03-1.13), but not associated with other COVID-19 outcomes. Living with children of any age was also associated with lower risk of dying from non-COVID-19 causes. Among 2,567,671 adults >65 years there was no association between living with children and outcomes related to SARS-CoV-2. We observed no consistent changes in risk following school closure.”
19. “Exploring inter-country coronavirus mortality“ By Trevor Nell, Ian McGorian, Nick Hudson. Pandata, July 7, 2020. “For each country put forward as an example, usually in some pairwise comparison and with an attendant single cause explanation, there are a host of countries that fail the expectation. We set out to model the disease with every expectation of failure. In choosing variables it was obvious from the outset that there would be contradictory outcomes in the real world. But there were certain variables that appeared to be reliable markers as they had surfaced in much of the media and pre-print papers. These included age, co-morbidity prevalence and the seemingly light population mortality rates in poorer countries than that in richer countries. Even the worst among developing nations—a clutch of countries in equatorial Latin America—have seen lighter overall population mortality than the developed world. Our aim therefore was not to develop the final answer, rather to seek common cause variables that would go some way to providing an explanation and stimulating discussion. There are some very obvious outliers in this theory, not the least of these being Japan. We test and find wanting the popular notions that lockdowns with their attendant social distancing and various other NPIs confer protection.”
20. “Covid-19 Mortality: A Matter of Vulnerability Among Nations Facing Limited Margins of Adaptation” by Quentin De Larochelambert, Andy Marc, Juliana Antero, Eric Le Bourg, and Jean-François Toussaint. Frontiers in Public Health, 19 November 2020. “Higher Covid death rates are observed in the [25/65°] latitude and in the [−35/−125°] longitude ranges. The national criteria most associated with death rate are life expectancy and its slowdown, public health context (metabolic and non-communicable diseases (NCD) burden vs. infectious diseases prevalence), economy (growth national product, financial support), and environment (temperature, ultra-violet index). Stringency of the measures settled to fight pandemia, including lockdown, did not appear to be linked with death rate. Countries that already experienced a stagnation or regression of life expectancy, with high income and NCD rates, had the highest price to pay.
This burden was not alleviated by more stringent public decisions. Inherent factors have predetermined the Covid-19 mortality: understanding them may improve prevention strategies by increasing population resilience through better physical fitness and immunity.”
21. “States with the Fewest Coronavirus Restrictions” by Adam McCann. WalletHub, Oct 6, 2020. This study assesses and ranks stringencies in the United States by states. The results are plotted against deaths per capita and unemployment. The graphics reveal no relationship in stringency level as it relates to the death rates, but finds a clear relationship between stringency and unemployment.
22. The Mystery of Taiwan: Commentary on the Lancet Study of Taiwan and New Zealand, by Amelia Janaskie. American Institute for Economic Research, November 2, 2020. “The Taiwanese case reveals something extraordinary about pandemic response. As much as public-health authorities imagine that the trajectory of a new virus can be influenced or even controlled by policies and responses, the current and past experiences of coronavirus illustrate a different point. The severity of a new virus might have far more to do with endogenous factors within a population rather than the political response. According to the lockdown narrative, Taiwan did almost everything ‘wrong’ but generated what might in fact be the best results in terms of public health of any country in the world.”
23. “Predicting the Trajectory of Any COVID19 Epidemic From the Best Straight Line” by Michael Levitt, Andrea Scaiewicz, Francesco Zonta. MedRxiv, Pre-print, June 30, 2020. “Comparison of locations with over 50 deaths shows all outbreaks have a common feature: H(t) defined as loge(X(t)/X(t-1)) decreases linearly on a log scale, where X(t) is the total number of Cases or Deaths on day, t (we use ln for loge). The downward slopes vary by about a factor of three with time constants (1/slope) of between 1 and 3 weeks; this suggests it may be possible to predict when an outbreak will end. Is it possible to go beyond this and perform early prediction of the outcome in terms of the eventual plateau number of total confirmed cases or deaths? We test this hypothesis by showing that the trajectory of cases or deaths in any outbreak can be converted into a straight line. Specifically Y(t)≡−ln(ln(N/X(t)),is a straight line for the correct plateau value N, which is determined by a new method, Best-Line Fitting (BLF). BLF involves a straight-line facilitation extrapolation needed for prediction; it is blindingly fast and amenable to optimization. We find that in some locations that entire trajectory can be predicted early, whereas others take longer to follow this simple functional form.”
13. “Smart Thinking, Lockdown and COVID-19: Implications for Public Policy” by Morris Altman. Journal of Behavioral Economics for Policy, 2020. “The response to COVID-19 has been overwhelmingly to lockdown much of the world’s economies in order to minimize death rates as well as the immediate negative effects of COVID-19. I argue that such policy is too often de-contextualized as it ignores policy externalities, assumes death rate calculations are appropriately accurate and, and as well, assumes focusing on direct Covid-19 effects to maximize human welfare is appropriate. As a result of this approach current policy can be misdirected and with highly negative effects on human welfare. Moreover, such policies can inadvertently result in not minimizing death rates (incorporating externalities) at all, especially in the long run. Such misdirected and sub-optimal policy is a product of policy makers using inappropriate mental models which are lacking in a number of key areas; the failure to take a more comprehensive macro perspective to address the virus, using bad heuristics or decision-making tools, relatedly not recognizing the differential effects of the virus, and adopting herding strategy (follow-the-leader) when developing policy. Improving the decision-making environment, inclusive of providing more comprehensive governance and improving mental models could have lockdowns throughout the world thus yielding much higher levels of human welfare.”
14. “SARS-CoV-2 waves in Europe: A 2-stratum SEIRS model solution” by Levan Djaparidze and Federico Lois. MedRxiv pre-print, October 23, 2020. “We found that 180-day of mandatory isolations to healthy <60 (i.e. schools and workplaces closed) produces more final deaths if the vaccination date is later than (Madrid: Feb 23 2021; Catalonia: Dec 28 2020; Paris: Jan 14 2021; London: Jan 22 2021). We also modeled how average isolation levels change the probability of getting infected for a single individual that isolates differently than average. That led us to realize disease damages to third parties due to virus spreading can be calculated and to postulate that an individual has the right to avoid isolation during epidemics (SARS-CoV-2 or any other).”
15. “Did Lockdown Work? An Economist’s Cross-Country Comparison” by Christian Bjørnskov. SSRN working paper, August 2, 2020. “The lockdowns in most Western countries have thrown the world into the most severe recession since World War II and the most rapidly developing recession ever seen in mature market economies. They have also caused an erosion of fundamental rights and the separation of powers in a large part of the world as both democratic and autocratic regimes have misused their emergency powers and ignored constitutional limits to policy-making (Bjørnskov and Voigt, 2020). It is therefore important to evaluate whether and to which extent the lockdowns have worked as officially intended: to suppress the spread of the SARS-CoV-2 virus and prevent deaths associated with it. Comparing weekly mortality in 24 European countries, the findings in this paper suggest that more severe lockdown policies have not been associated with lower mortality. In other words, the lockdowns have not worked as intended.”
16.”Four Stylized Facts about COVID-19” (alt-link) by Andrew Atkeson, Karen Kopecky, and Tao Zha. NBER working paper 27719, August 2020. “One of the central policy questions regarding the COVID-19 pandemic is the question of which non-pharmeceutical interventions governments might use to influence the transmission of the disease. Our ability to identify empirically which NPI’s have what impact on disease transmission depends on there being enough independent variation in both NPI’s and disease transmission across locations as well as our having robust procedures for controlling for other observed and unobserved factors that might be influencing disease transmission. The facts that we document in this paper cast doubt on this premise…. The existing literature has concluded that NPI policy and social distancing have been essential to reducing the spread of COVID-19 and the number of deaths due to this deadly pandemic. The stylized facts established in this paper challenge this conclusion.”
17. “How does Belarus have one of the lowest death rates in Europe?” by Kata Karáth. British Medical Journal, September 15, 2020. “Belarus’s beleaguered government remains unfazed by covid-19. President Aleksander Lukashenko, who has been in power since 1994, has flatly denied the seriousness of the pandemic, refusing to impose a lockdown, close schools, or cancel mass events like the Belarusian football league or the Victory Day parade. Yet the country’s death rate is among the lowest in Europe—just over 700 in a population of 9.5 million with over 73 000 confirmed cases.”
18. “Association between living with children and outcomes from COVID-19: an OpenSAFELY cohort study of 12 million adults in England” by Harriet Forbes, Caroline E Morton, Seb Bacon et al., by MedRxiv, November 2, 2020. “Among 9,157,814 adults ≤65 years, living with children 0-11 years was not associated with increased risks of recorded SARS-CoV-2 infection, COVID-19 related hospital or ICU admission but was associated with reduced risk of COVID-19 death (HR 0.75, 95%CI 0.62-0.92). Living with children aged 12-18 years was associated with a small increased risk of recorded SARS-CoV-2 infection (HR 1.08, 95%CI 1.03-1.13), but not associated with other COVID-19 outcomes. Living with children of any age was also associated with lower risk of dying from non-COVID-19 causes. Among 2,567,671 adults >65 years there was no association between living with children and outcomes related to SARS-CoV-2. We observed no consistent changes in risk following school closure.”
19. “Exploring inter-country coronavirus mortality“ By Trevor Nell, Ian McGorian, Nick Hudson. Pandata, July 7, 2020. “For each country put forward as an example, usually in some pairwise comparison and with an attendant single cause explanation, there are a host of countries that fail the expectation. We set out to model the disease with every expectation of failure. In choosing variables it was obvious from the outset that there would be contradictory outcomes in the real world. But there were certain variables that appeared to be reliable markers as they had surfaced in much of the media and pre-print papers. These included age, co-morbidity prevalence and the seemingly light population mortality rates in poorer countries than that in richer countries. Even the worst among developing nations—a clutch of countries in equatorial Latin America—have seen lighter overall population mortality than the developed world. Our aim therefore was not to develop the final answer, rather to seek common cause variables that would go some way to providing an explanation and stimulating discussion. There are some very obvious outliers in this theory, not the least of these being Japan. We test and find wanting the popular notions that lockdowns with their attendant social distancing and various other NPIs confer protection.”
20. “Covid-19 Mortality: A Matter of Vulnerability Among Nations Facing Limited Margins of Adaptation” by Quentin De Larochelambert, Andy Marc, Juliana Antero, Eric Le Bourg, and Jean-François Toussaint. Frontiers in Public Health, 19 November 2020. “Higher Covid death rates are observed in the [25/65°] latitude and in the [−35/−125°] longitude ranges. The national criteria most associated with death rate are life expectancy and its slowdown, public health context (metabolic and non-communicable diseases (NCD) burden vs. infectious diseases prevalence), economy (growth national product, financial support), and environment (temperature, ultra-violet index). Stringency of the measures settled to fight pandemia, including lockdown, did not appear to be linked with death rate. Countries that already experienced a stagnation or regression of life expectancy, with high income and NCD rates, had the highest price to pay.
This burden was not alleviated by more stringent public decisions. Inherent factors have predetermined the Covid-19 mortality: understanding them may improve prevention strategies by increasing population resilience through better physical fitness and immunity.”
21. “States with the Fewest Coronavirus Restrictions” by Adam McCann. WalletHub, Oct 6, 2020. This study assesses and ranks stringencies in the United States by states. The results are plotted against deaths per capita and unemployment. The graphics reveal no relationship in stringency level as it relates to the death rates, but finds a clear relationship between stringency and unemployment.
22. The Mystery of Taiwan: Commentary on the Lancet Study of Taiwan and New Zealand, by Amelia Janaskie. American Institute for Economic Research, November 2, 2020. “The Taiwanese case reveals something extraordinary about pandemic response. As much as public-health authorities imagine that the trajectory of a new virus can be influenced or even controlled by policies and responses, the current and past experiences of coronavirus illustrate a different point. The severity of a new virus might have far more to do with endogenous factors within a population rather than the political response. According to the lockdown narrative, Taiwan did almost everything ‘wrong’ but generated what might in fact be the best results in terms of public health of any country in the world.”
23. “Predicting the Trajectory of Any COVID19 Epidemic From the Best Straight Line” by Michael Levitt, Andrea Scaiewicz, Francesco Zonta. MedRxiv, Pre-print, June 30, 2020. “Comparison of locations with over 50 deaths shows all outbreaks have a common feature: H(t) defined as loge(X(t)/X(t-1)) decreases linearly on a log scale, where X(t) is the total number of Cases or Deaths on day, t (we use ln for loge). The downward slopes vary by about a factor of three with time constants (1/slope) of between 1 and 3 weeks; this suggests it may be possible to predict when an outbreak will end. Is it possible to go beyond this and perform early prediction of the outcome in terms of the eventual plateau number of total confirmed cases or deaths? We test this hypothesis by showing that the trajectory of cases or deaths in any outbreak can be converted into a straight line. Specifically Y(t)≡−ln(ln(N/X(t)),is a straight line for the correct plateau value N, which is determined by a new method, Best-Line Fitting (BLF). BLF involves a straight-line facilitation extrapolation needed for prediction; it is blindingly fast and amenable to optimization. We find that in some locations that entire trajectory can be predicted early, whereas others take longer to follow this simple functional form.”
onetimer
Veteran Member
This is not the UK strain
New more worrisome South Africa strain: the new 501.V2 variant has troubling details:
—seems to spread faster
—higher viral load
—possibly more severe among young adults
—2 of 3 mutations in 501.V2 **reduce virus sensitivity to some antibodies**
View: https://twitter.com/DrEricDing/status/1340517608643317761?s=19
New more worrisome South Africa strain: the new 501.V2 variant has troubling details:
—seems to spread faster
—higher viral load
—possibly more severe among young adults
—2 of 3 mutations in 501.V2 **reduce virus sensitivity to some antibodies**
View: https://twitter.com/DrEricDing/status/1340517608643317761?s=19
marsh
On TB every waking moment
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
Stanford SJWs Left 100s Of Frontline Doctors Without Priority Access To COVID Vaccine
SUNDAY, DEC 20, 2020 - 17:00
Even before the vaccine rollout in the US started, scientists and bioethicists warned that attempts to prioritize those most in need of a vaccine - that is, frontline health-care workers and residents in long-term care facilities, would ultimately prove flawed, as those with money and influence find ways to cut the line.

Though we have yet to hear reports of an actual black market for vaccine doses (perhaps since the supply so far is being controlled pretty tightly) there have been reports of "mistakes" and "errors" that led to high-level doctors and other individuals in positions of influence receiving the vaccine before nurses and doctors.
ProPublica has reported on one example whereby hundreds of residents at Stanford Medicine were passed over despite assignments that required frequent face-to-face contact with people infected with COVID-19.
Instead, "high-ranking doctors who carry a lower risk of patient transmission" received priority treatment, one doctor complained.
Others complained of what appeared to be random errors perpetrated by the algorithms tasked with determining which nurses deserved priority. It all begs the question: why even resort to these algorithms? Why not just let the top managers decide? Well, the funny thing about algorithms and other "quantitative" methodologies is they allow people to distance themselves from outcomes that involve extremely serious consequences."Residents are patient-facing, we’re the ones who have been asked to intubate, yet some attendings who have been face-timing us from home are being vaccinated before us," said Dr. Sarah Johnson, a third-year OB-GYN resident who has delivered babies from COVID-positive patients during the pandemic. "This is the final straw to say, 'We don’t actually care about you.'"
Additionally, in this time of heightened sensitivity to issues of racial equality and social justice, algorithms have been forced to prioritize elements like race in a way that could skew the results in unanticipated ways.
People's lives hang in the balance. In one instance, an algorithm assigned a higher priority to an operating room nurse working elective surgeries, over an ER nurse regularly dealing with the infected.
When they asked about the algorithm tasked with determining the first 5K allocations, they were told that, for some obscure bureaucratic reason, they would receive a lower priority.Another resident, who asked not to be named, said a nurse who works in an operating room for elective surgeries has been notified she’ll get the vaccine in the first wave. “We test people for COVID before elective surgeries, so by definition, we will know if those patients have COVID,” he said, so to him, it didn’t make sense that that nurse would be prioritized.
Ultimately, only 7 of the 1K+ residents made the priority list.An algorithm chose who would be the first 5,000 in line. The residents said they were told they were at a disadvantage because they did not have an assigned “location” to plug into the calculation and because they are young, according to an email sent by a chief resident to his peers. Residents are the lowest-ranking doctors in a hospital. Stanford Medicine has about 1,300 across all disciplines.
A letter sent by the Stanford leadership explained that the algorithm was meant to "ensure equity and justice".Only seven made the priority vaccination list, despite the fact that this week, residents were asked to volunteer for ICU coverage in anticipation of a surge in COVID-19 cases.
Apparently, it accomplished this while also leaving residents and nurses exposed.In a letter to Stanford leadership sent on Thursday, the chief resident council wrote, “While leadership is pointing to an error in an algorithm meant to ensure equity and justice, our understanding is this error was identified on Tuesday and a decision was made not to revise the vaccine allocation scheme before its release today.” The council asked for a timeline for vaccination of the residents and transparency regarding the algorithm.
Just another reminder that social justice warriors should be careful what they wish for.In response to the residents’ protests, Dr. Niraj Sehgal, chief medical officer, sent an email saying, “Please know that the perceived lack of priority for residents and fellows was not the intent at all.” He added that with the anticipated authorization of Moderna’s vaccine, “we’re increasingly confident in getting everyone vaccinated, including all of you.” He signed off with “heartfelt apologies.”
PanBear
Veteran Member
Dr. Ali Nouri
1/The UK #SARSCoV2 variant reported to be 70% more transmissible harbors a set of mutations in the Spike protein––the part of the virus that touches the human ACE2 receptor and allows the virus entry into our cells. One mutation, N501Y, allows Spike to bind ACE2 more tightly
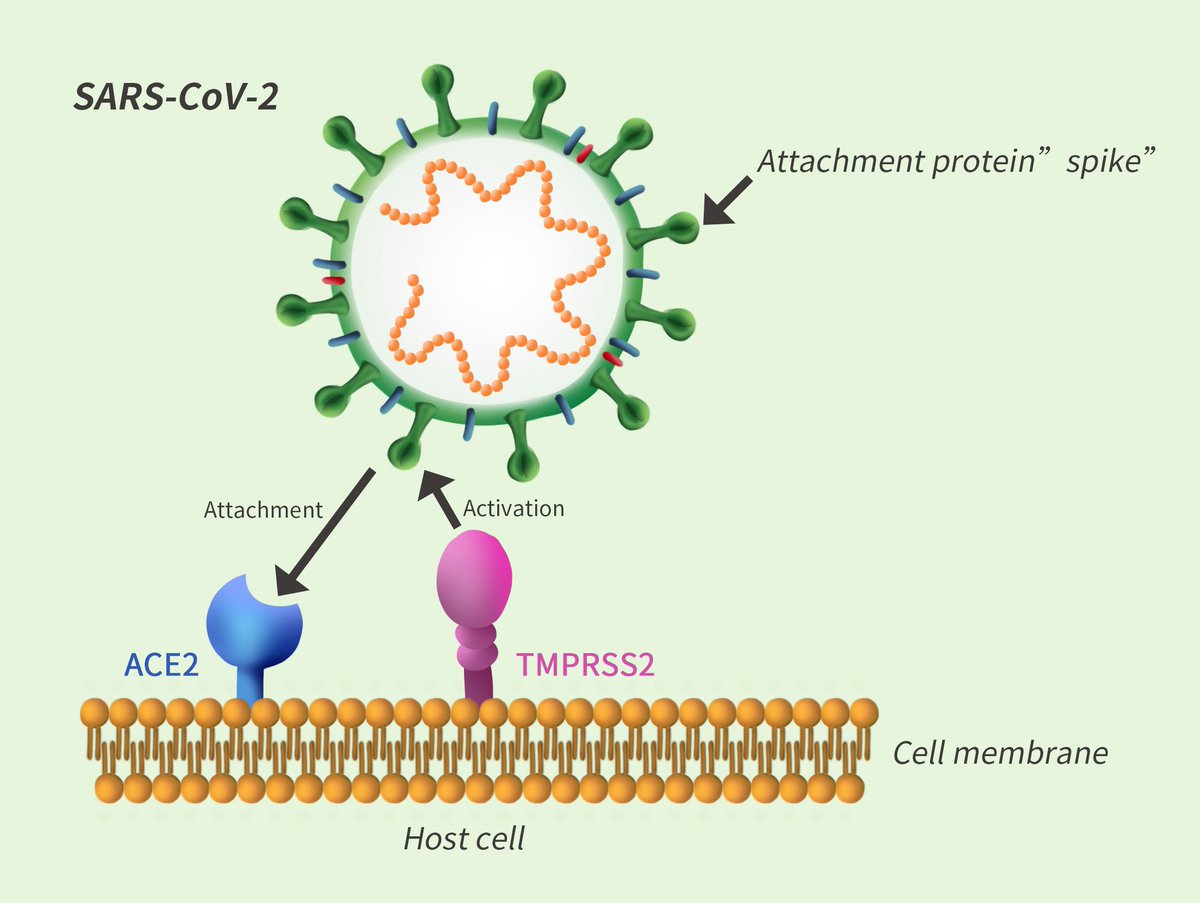
2/Another mutation, P681H, is near Spike's "Furin cleavage site" Unclear what the mutation does, but the location is significant because it's where enzymes "process" Spike, helping virus infect airway cells & enable efficient human-to-human transmission: SARS-CoV-2 D614G Variant Exhibits Enhanced Replication ex vivo and Earlier Transmission in vivo

3/these mutations are accumulating in the backdrop of another mutation, D614G, which has become dominant, globally, and has enhanced infectivity and replication fitness. It's even been shown, experimentally, to transmit faster through droplets & aerosols in hamsters.
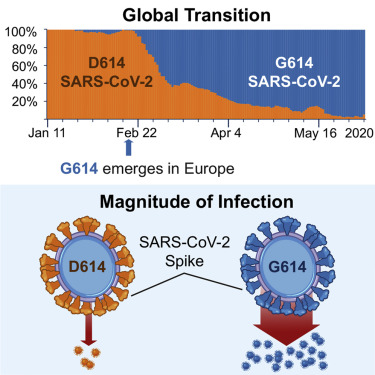
4/In that experiment, naive hamsters caught the virus faster from hamsters that carried the D614G variant, vs hamsters that carried the original (WT) strain. So one would also expect earlier transmission of D614G in humans.
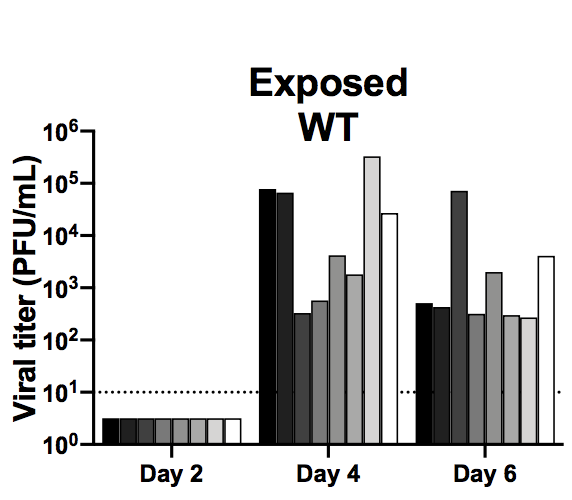
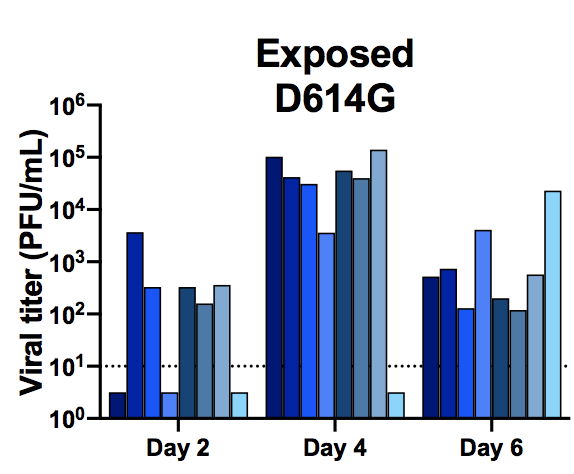

 www.biorxiv.org
www.biorxiv.org
5/These are just a few of the many mutations this virus is accumulating. Every time it replicates, we give it the opportunity to mutate. And if those mutations render drugs and vaccines ineffective, which is possible, we'll be in a lot more trouble.
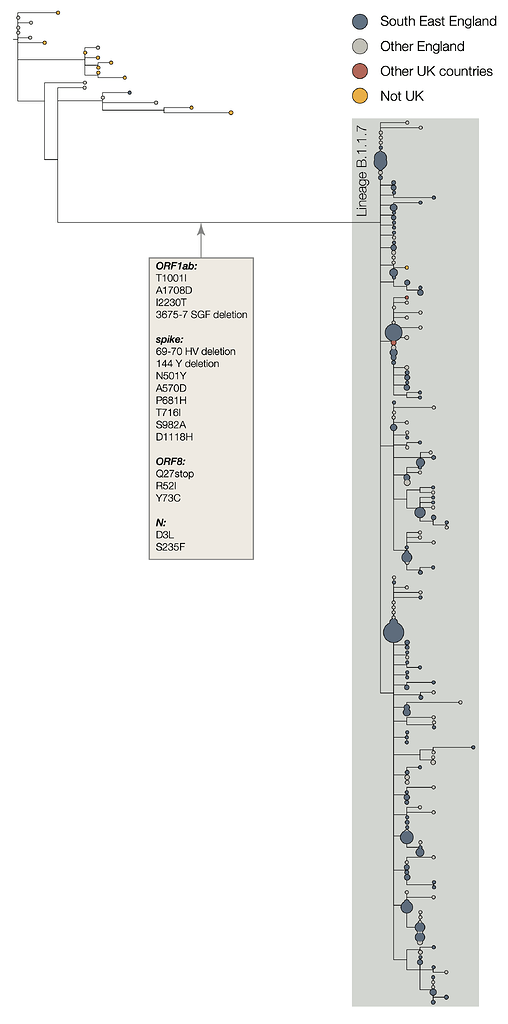
 virological.org
virological.org
1/The UK #SARSCoV2 variant reported to be 70% more transmissible harbors a set of mutations in the Spike protein––the part of the virus that touches the human ACE2 receptor and allows the virus entry into our cells. One mutation, N501Y, allows Spike to bind ACE2 more tightly
2/Another mutation, P681H, is near Spike's "Furin cleavage site" Unclear what the mutation does, but the location is significant because it's where enzymes "process" Spike, helping virus infect airway cells & enable efficient human-to-human transmission: SARS-CoV-2 D614G Variant Exhibits Enhanced Replication ex vivo and Earlier Transmission in vivo
3/these mutations are accumulating in the backdrop of another mutation, D614G, which has become dominant, globally, and has enhanced infectivity and replication fitness. It's even been shown, experimentally, to transmit faster through droplets & aerosols in hamsters.
4/In that experiment, naive hamsters caught the virus faster from hamsters that carried the D614G variant, vs hamsters that carried the original (WT) strain. So one would also expect earlier transmission of D614G in humans.
SARS-CoV-2 D614G Variant Exhibits Enhanced Replication ex vivo and Earlier Transmission in vivo
The D614G substitution in the S protein is most prevalent SARS-CoV-2 strain circulating globally, but its effects in viral pathogenesis and transmission remain unclear. We engineered SARS-CoV-2 variants harboring the D614G substitution with or without nanoluciferase. The D614G variant replicates...
www.biorxiv.org
5/These are just a few of the many mutations this virus is accumulating. Every time it replicates, we give it the opportunity to mutate. And if those mutations render drugs and vaccines ineffective, which is possible, we'll be in a lot more trouble.
Preliminary genomic characterisation of an emergent SARS-CoV-2 lineage in the UK defined by a novel set of spike mutations
Preliminary genomic characterisation of an emergent SARS-CoV-2 lineage in the UK defined by a novel set of spike mutations Report written by: Andrew Rambaut1, Nick Loman2, Oliver Pybus3, Wendy Barclay4, Jeff Barrett5, Alesandro Carabelli6, Tom Connor7, Tom Peacock4, David L Robertson8, Erik...
virological.org
marsh
On TB every waking moment

Dr. Scott Gottlieb says new UK Covid strain 'will not slip past our vaccines very easily'
Existing Covid vaccines will likely provide protection against the new strain of coronavirus circulating in Britain, the former FDA chief told CNBC.
Dr. Scott Gottlieb says new UK Covid strain ‘will not slip past our vaccines very easily’
PUBLISHED MON, DEC 21 20209:13 AM ESTUPDATED MON, DEC 21 202010:12 AM EST
Kevin Stankiewicz@KEVIN_STANK
KEY POINTS
- A new strain of coronavirus circulating in the U.K. is believed to be more than 70% more transmissible than existing variants.
- However, Dr. Scott Gottlieb said existing Covid-19 vaccines are likely to provide protection against it.
- The virus mutation also does not appear to have made it more deadly, according to the former FDA chief.
VIDEO on website 3:20 min
Former FDA chief Gottlieb on new Covid strain: Eventually will have to update vaccines
Dr. Scott Gottlieb told CNBC on Monday that existing Covid-19 vaccines will likely provide protection against the new strain of the coronavirus circulating in the U.K.
British Prime Minister Boris Johnson on Saturday implemented strict lockdowns in London and large parts of southern England in response to rising coronavirus infections. He said the growth in cases appeared to be stemming from a new variant of the coronavirus that is about 70% more transmissible than existing strains.
Gottlieb, a former U.S. Food and Drug Administration commissioner, said on “Squawk Box” that the evidence does suggest the new variant transmits more easily. But, he cautioned, “it doesn’t seem to have mutated the surface proteins of the virus in a way that they would slip past our vaccines or prior immunity. In fact, we don’t think that that’s the case.”
Gottlieb, a board member of Pfizer, which makes one of two Covid vaccines to receive limited FDA approval, has also said the mutation does not seem to be more deadly than previous variants during the pandemic.
The fact the coronavirus has mutated is not surprising, Gottlieb said.
“Some viruses like flu evolve their surface proteins very quickly, and that’s why we need a different flu vaccine every season,” said Gottlieb, who led the FDA in the Trump administration from 2017 to 2019. “Some viruses can’t really change their surface proteins, like measles. This [coronavirus] seems to fall some place in between. It’s not going to change its surface proteins very rapidly, that spike protein, but it will change it over time.”
The developments around the new strain come as vaccine rollout picks up steam in Britain and U.S. alike. On Friday, the FDA approved Moderna’s Covid-19 vaccine for emergency use, paving the way for distribution to begin this week.
Gottlieb sought to assure people that the existing vaccines would be effective against new strains — which also have been detected in a patient in Italy and in South Africa. The pandemic has infected almost 77 million people worldwide and killed nearly 1.7 million people, according to data compiled by Johns Hopkins University.
“It’s probably a good thing that we used the entire spike protein in our vaccines because what we’re getting is what we call a polyclonal response. We’re developing antibodies to many different regions of that protein, so even if one part of that protein were mutated and some antibodies no longer recognize it, there would be antibodies to other parts of that protein,” Gottlieb explained. Antibodies help fight infections. “So this probably will not slip past our vaccines very easily, but eventually we will have to update the vaccines.”
WATCH NOW
VIDEO 3:07 min on website
New Covid-19 strain has ‘more mutations’ than any other variant, immunologist says
Disclosure: Scott Gottlieb is a CNBC contributor and is a member of the boards of Pfizer, genetic testing start-up Tempus and biotech company Illumina. Pfizer has a manufacturing agreement with Gilead for remdesivir. Gottlieb also serves as co-chair of Norwegian Cruise Line Holdings′ and Royal Caribbean’s “Healthy Sail Panel.”
marsh
On TB every waking moment
24:48 min
SARS-CoV-2 UK variant: Does it matter?
•Dec 21, 2020

Vincent Racaniello
Vincent explains the properties of the SARS-CoV-2 UK variant and why claims that it is more transmissible are not supported by experimental data.
marsh
On TB every waking moment
3:19 min
Trump 2020 Advisory Board Member, Bruce LeVell, on Businesses Coping with Covid-19
•Dec 21, 2020

One America News Network
marsh
On TB every waking moment
58:03 min
COVID-19: What Physicians Need to Know
•Dec 21, 2020

Centers for Disease Control and Prevention (CDC)
Check out the recording of Project Firstline’s infection control training collaborative kickoff event, hosted by the American Medical Association (AMA). Listen in as AMA President, Dr. Susan
marsh
On TB every waking moment
59:22 min
What Clinicians Need to Know About Pfizer-BioNTech and Moderna Vaccines
•Dec 21, 2020
Centers for Disease Control and Prevention (CDC)
This COCA Call will give clinicians an overview of the Pfizer-BioNTech and Moderna COVID-19 vaccines. Clinicians will learn about vaccine characteristics and administration, vaccinating special populations, and contraindications. They will also get answers to a number of clinical questions CDC has received about these new vaccines.
marsh
On TB every waking moment

Slaoui: ‘Very unlikely’ for new coronavirus variant to be resistant to vaccine’s immunity - Washington Examiner
Dr. Moncef Slaoui expressed hopeful news about the coronavirus vaccine's strength, even against the new variant spreading in southern England. Slaoui, head of Operation Warp Speed's coronavirus vaccine program, told CNN's Jake Tapper on Sunday that it's unlikely the new variant would be...
 www.washingtonexaminer.com
www.washingtonexaminer.com
Slaoui: 'Very unlikely' for new coronavirus variant to be resistant to vaccine's immunity
by Mica Soellner, Breaking News Reporter |
| December 20, 2020 03:29 PM
Dr. Moncef Slaoui expressed hopeful news about the coronavirus vaccine's strength, even against the new variant spreading in southern England.
Slaoui, head of Operation Warp Speed's coronavirus vaccine program, told CNN's Jake Tapper on Sunday that it's unlikely the new variant would be resistant to the vaccines being developed. The Pfizer vaccine began distribution in the United States last week.
"As of now, I don’t think there has been a single variant that would be resistant to the vaccine," Slaoui said. "We can’t exclude it, but it’s not there now. This particular variant in the U.K., I think, is very unlikely to have escaped the vaccine immunity."
German Health Minister Jens Spahn echoed the sentiment about vaccine strength, saying he believes the vaccines will be effective against the new virus strain, according to AFP.
Largely concentrated in the United Kingdom, the new strain has prompted several countries within the European Union to halt flights to and from the nation. British Prime Minister Boris Johnson tightened restrictions in London and its surrounding areas after revelations of the new variant came to light.
Video on website 2:04 min
Federal officials suggest the vaccine could be distributed to the U.S. general public by April. Its distribution has begun going out to healthcare workers across the country. The elderly population in care homes is next in line as a high-priority group.
Worldwide, COVID-19 has infected more than 75 million people and killed over 1.5 million.
marsh
On TB every waking moment

Some states prioritize blacks, Hispanics over whites for COVID-19 vaccines, report says
"Systemic health and social inequities have put many people from racial and ethnic minority groups at increased risk,"
Some states prioritize blacks, Hispanics over whites for COVID-19 vaccines, report says
"Systemic health and social inequities have put many people from racial and ethnic minority groups at increased risk,"
By Joseph Curl
Updated: December 20, 2020 - 10:51pm
Half of U.S. states have laid out plans to prioritize black and Hispanic patients over whites as the rollout of two COVID-19 vaccines gathers steam, according to a new report.
According to an analysis by The Daily Mail, 25 states have "committed to a focus on racial and ethnic communities as they decided which groups should be prioritized in receiving a coronavirus vaccine dose." The moves follow guidance to do so by the Centers for Disease Control and Prevention (CDC).
"Some states have made even more specific plans to prioritize communities of color, with 12 states specifically mentioning efforts to partner with healthcare providers in areas with a large minority population to reach 'diverse populations,' according to the Kaiser Family Foundation," the Mail reported.
Maine, for instance, enacted a "Racial/Ethnic Minority COVID-19 Vaccination Plan" that will give preference to groups that "have experienced rates of disease that far exceed their representation in the population as a whole."
"Long-standing systemic health and social inequities have put many people from racial and ethnic minority groups at increased risk of getting sick and dying from COVID-19," the CDC wrote in July. "The term 'racial and ethnic minority groups' includes people of color with a wide variety of backgrounds and experiences. But some experiences are common to many people within these groups, and social determinants of health have historically prevented them from having fair opportunities for economic, physical, and emotional health."
On Nov. 30, the CDC released more guidance, saying "race and ethnicity are risk markers for other underlying conditions that affect health including socioeconomic status, access to health care, and exposure to the virus related to occupation, e.g., frontline, essential, and critical infrastructure workers."
According to the agency's data, blacks were 3.7 times more likely than whites to require hospitalization to treat the virus, while Hispanics were 1.2 times more likely. American Indians and Alaska natives, meanwhile, were also more likely to require hospitalization than whites.
In addition, black and Hispanic people are almost three times more likely to die from COVID-19 than whites.
The CDC's Advisory Committee on Immunization Practices (ACIP) on Dec. 2 voted to direct that healthcare workers and residents of long-term care facilities will be the first to get the shots in the initial rollout — once federal regulators authorize use of a vaccine. The recommendation was approved by CDC Director Robert Redfield.
But state governors have final say on how the vaccines get distributed.
Said the Mail:
"A recent study from the National Governors Association also showed that 'many states have incorporated health equity principles in their vaccination plans to varying degrees.' It reported that California, Louisiana, New Mexico, North Carolina, and Indiana have listed fairness, equity, or both as key principles for vaccine distribution. Oregon is also emphasizing health equity as a central pillar of its rollout, while North Carolina 'specifically cited historically marginalized populations as an early-phase critical population group.'"
marsh
On TB every waking moment

Nurse faints shortly after receiving COVID vaccine, blames oversensitivity to pain
“Overreactive vagal response” allegedly caused her to pass out
Nurse faints shortly after receiving COVID vaccine, blames oversensitivity to pain
“Overreactive vagal response” allegedly caused her to pass out
Image

An injection of a COVID-19 vaccine
(Xinhua News Agency/Getty)
By Daniel Payne
Updated: December 19, 2020 - 11:44am
A nurse made headlines this week when she passed out very shortly after receiving an injection of a COVID-19 vaccine, an incident she blamed on a chronic oversensitivity to pain.
Tiffany Dover at CHI Memorial Hospital in Chattanooga, TN, fainted reportedly less than 20 minutes after receiving a shot of the Pfizer COVID vaccine. “I’m sorry, I’m feeling a little dizzy,” Dover said during a press conference shortly before she collapsed on the floor.
View: https://twitter.com/i/status/1339822042841899011
1:10 min
After recovering, Dover told media that she suffers from a condition in which even modest amounts of pain can cause her to pass out.
“I have a history of having an overreactive vagal response,” she said, “and so with that, if I have pain from anything—a hangnail or if I stub my toe—I can just pass out.”
The hospital in a statement echoed that explanation. “The fainting episode is not an adverse reaction to the vaccine,” one doctor said, arguing that it was “related to her medical condition.”
A "vagal reaction," according to medical authorities, is defined as "a response in your body that causes your pulse to slow down or the blood vessels to expand," often following "sudden fear, severe pain, emotional stress, overexertion, overheating, hunger, nausea or vomiting, prolonged standing, or standing up after sitting or lying for a long time."
marsh
On TB every waking moment


New Study Shows Mask Mandates Had Zero Effect in Florida or Nationwide, But the Lie Continues

Scott Morefield
|
Posted: Dec 21, 2020 12:01 AM
The opinions expressed by columnists are their own and do not necessarily represent the views of Townhall.com.

Source: AP Photo/Alex Brandon
Obviously, no amount of evidence, data, trends, facts, studies, or science will ever convince most ‘public health officials’ that masks aren’t doing squat to stop the spread of COVID-19. Cases and deaths continue to spike (yes, many of these are super-sensitive PCR test-driven numbers, but still) despite the fact that well over 90% of the country are complying with their absurd mandates. Yet, predictably, the virus keeps going right on virusing, as highly contagious respiratory viruses, unfortunately, tend to do, especially once cold weather hits.
Nevertheless, those of us who are mask skeptics have a difficult chore in front of us. Given that most of the country is under a mask mandate of some form or another, we can point to spikes all day AFTER these mandates were put in place only to have our opponents simply say, “Look how bad it would have been WITHOUT masks!”
It’s a tough argument to counter given the fact that our overlords have sold masking as a low-cost, easy “solution” that’s totally worth it even if they “save one life,” or something (nevermind the health risks - let’s censor docs who talk about those!). So, how DO we prove that things wouldn’t have been worse without masks? One way is to look at data from the few free states remaining.
In Florida, for example, most counties have so far bravely refused to implement mask mandates while others, usually in high population centers, have done so. Justin Hart and the team at Rational Ground (follow them on Twitter here - it’s worth it) just released a comprehensive data analysis of masked vs non-masked counties in the state. A total of 22 of 67 counties in the state have implemented a mask order at some point during the period of May 1 through December 15. It may not sound like many, but these include almost all of Florida’s largest metro areas. To be more than fair, if an area added a mask order at some point during the outbreak, the study’s authors gave a 14 day period to allow time for cases to begin subsiding. “Cases were summed for both mandate and non-mandate jurisdictions and adjusted per 100,000 people for days the mandates were or were not in effect,” wrote the authors, describing the methodology used.
If masks did even close to as advertised, one would expect to see the counties that went maskless to be absolute dumpster fires next to the counties that implemented mandates, right? At the very least, the numbers should favor the masked areas by more than a percentage point or two. So, how did it go? Yep, it was the Mask Cult’s worse nightmare:
“When counties DID have a mandate in effect, there were 667,239 cases over 3,137 days with an average of 23 cases per 100,000 per day. When counties DID NOT have a countywide order, there were 438,687 cases over 12,139 days with an average of 22 cases per 100,000 per day.”
In other words, counties with mask-mandates in place actually did WORSE than those that refused to implement them. (Yeah, color me shocked.) The authors even accounted for population density in their analysis, suggesting that it didn’t have an impact on the numbers because four of the 12 most populous counties in Florida never had a countywide order. “When the eight DID have an order in effect, there were 64 cases per 1,000. In periods 11 of 12 DID NOT have one, there were 40,” they wrote.
“But that’s just Florida,” you say. “They’re weirdos anyway. Surely masks have worked in the rest of the country.” Well, I’m glad you asked! The good folks at Rational Ground went on to compare national numbers, pitting the states that resisted the urge to impose a statewide mask mandate against those that masked up. How did those compare?
“When states DID have a mandate in effect, there were 9,605,256 cases over 5,907 total days and averaged 27 cases per 100,000 per day. When states DID NOT have a statewide order there were 5,781,716 cases over 5,772 total days averaging 17 cases per 100,000 people per day.”
So there you have it, incontrovertible data evidence that mask mandates do little to nothing to stop or even slightly curb the spread of COVID-19. If masks were the answer, wouldn’t you expect to see a drop in cases not long after mask mandates are implemented? At the very least, wouldn’t you expect to see cases level off and STAY leveled off? What you would NOT expect would be what has actually happened, for cases to spike as they have done since November seemingly all across the country, regardless of whether or not a mandatory masking policy was in place.
Further, wouldn’t you also expect states and areas that MASKED HARRDERRR than anyone else, states like California that have the ‘bold leadership’ to insist the plebes under their control mask up outside on hiking trails and sitting alone in parks, to have the lowest case counts of all? Just look at the latest per capita numbers there compared to Florida and tell me with a straight face that mask mandates ‘work.’ As Dave Rubin adeptly pointed out earlier this month, Florida’s numbers “should be ten times higher” than California’s. I mean, nobody is asking for masks to work perfectly, but hell, shouldn’t we expect SOME performance?
Numbers and data like this get down to the brass tacks. We can pit our doctors, scientists, and epidemiologists against their doctors, scientists, and epidemiologists on the actual science behind whether forcing people to put a moist, bacteria & virus-laden piece of cloth over the holes through which they breathe actually works to contain a virus that’s infinitesimally smaller than its threads (and yes, there are plenty of doctors, scientists, and epidemiologists on Team Reality too, and a bunch of them are on this must-follow Twitter list!), but if mask-mandates aren’t actually WORKING to curb the spread, why do we have them in place?
It’s complete and utter nonsense, of course. You know it, I know it, and the powers-that-be likely know it too. So why do they insist on continuing the charade? Whatever it is, it has NOTHING to do with either public health or real science.
marsh
On TB every waking moment

Leftists Hijacking Vaccination Rollout | RealClearPolitics
You were warned about this first in July. Now, it's happening. On Sunday, the federal Advisory Committee on Immunization Practices recommended that seniors...
Leftists Hijacking Vaccination Rollout
.
By Betsy McCaughey
December 21, 2020
You were warned about this first in July. Now, it's happening. On Sunday, the federal Advisory Committee on Immunization Practices recommended that seniors ages 65 to 74 be moved toward the back of the line for the COVID-19 vaccine.
The reason, says ACIP, is that "racial and ethnic minority groups [are] under-represented" in this age group. Put another way: Seniors are too white.
Vaccines are already being administered to health workers and nursing home residents. The question is this: Who comes next? ACIP wants to push 87 million essential workers -- such as transit workers, supermarket employees and uniformed public servants -- to the front of the line, forcing 32 million seniors to wait.
Vaccinating a majority of 87 million essential workers will consume the vaccine supply for several months.
Thousands of seniors will die needlessly if this decision goes into effect. ACIP actually admits as many as 6.5% more elderly will die over the next six months but dismisses that loss of life as "minimal." Not if it's your grandma.
A person 65 or older is at least 90 times more at risk of dying from COVID-19 than a young working-age person. Vaccinating the elderly first is the obvious strategy to save the most lives. ACIP says its twisted priorities are based in "fairness, equity and justice." What the committee really means is "wokeness."
Committee member Peter Szilagyi, from the University of California, Los Angeles, defends ACIP's move, because "essential workers" include "a high proportion of minority, low-income and low-education workers."
These left-wing academics are exploiting the pandemic as a launching pad for their redistributionist agenda. The lives of seniors -- who need the vaccine the most -- be damned.
Harald Schmidt, from the University of Pennsylvania, explains that "older populations are whiter." He says "society is structured in a way that enables them to live longer. Instead of giving additional health benefits to ... them, we can start to level the playing field a bit."
What's alarming is that Schmidt's call to level the playing field is widely shared. Dr. Douglas White, an ethicist at the University of Pittsburgh, says that if COVID-19 therapeutics are in short supply, they should go to patients from disadvantaged groups first. What's next? Requiring that when emergency rooms are packed, minorities and poor people get helped ahead of the elderly?
Medicine is no place for social engineering. It's frightening.
In Britain, vaccines are being administered with one unambiguous goal -- saving the most lives. Those over 80 are first in line, and then those in their 60s and 70s, followed by younger people with high-risk health conditions. Britain's health service explains, "The optimal strategy for minimizing future deaths" is "to offer vaccination to older age groups first."
The National Academies of Science, Engineering and Medicine, and the World Health Organization agree. But in America, the academic left has hijacked vaccination.
The bogus excuse is "structural racism" in American health care. The New York Times points to a "documented history of [minorities] receiving unequal care."
In the distant past, yes, but there is almost no evidence of racism in medicine today. A recent article in Scientific American could cite only two studies in more than 20 years documenting unequal care. New research from NYU Langone shows that Black COVID-19 patients "if anything ... do a little better" than white patients in the hospital. A larger study comparing Black and white COVID patients in 92 hospitals in 12 states found almost identical survival rates, though Blacks again did slightly better.
The persistent and unproven claims of racism in medicine are a slap in the face to the overwhelming majority of nurses, doctors and other medical personnel who provide care to their patients based on medical need, not race.
Medical need should be the only standard for dispensing vaccines, as well. By that standard, all people 65 and over should be top priority. Beware of arguments to level the playing field. They are malevolent and have no place in medicine. This time, seniors are the victims. Next time, it could be you.
marsh
On TB every waking moment
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
Are We Facing A Future Where Life Only Goes "Back To Normal" For Rich People?
MONDAY, DEC 21, 2020 - 17:00
Authored by Daisy Luther via The Organic Prepper blog,
As jobs and businesses vanish, and prices go up, Americans could soon face another expense – the expense of proving that they’re “healthy.”

While the government tells us that the Covid vaccinations are going to be “free,” are they really? Let’s take a look.
How much will it actually cost to get vaccinated against Covid?
While the government is paying for the vaccine itself, it will still cost money for most people to get injected with it.
However, providers will be able to bill you an administrative fee for giving the shot to patients, according to the Centers for Disease Control and Prevention.
This would be similar to paying a charge when you visit the doctor’s office, or for specialized vaccine delivery, such as infusion, a process in which a substance — like medication, a chemotherapy drug or hydration — enters the bloodstream intravenously.
If you don’t have insurance, the medical provider you used should be reimbursed for any COVID-19 treatment you receive through the CARES Act Provider Relief Fund, at no cost to you.
So it’s kind of free, sort of, unless somebody charges you but then you might be able to get your money back. Multiply by your number of family members.…If you receive a bill for administration fees, it’s still unclear whether or not those will be covered in full. It’s a good idea to contact your local provider or health insurance company for more details on whether you’ll be charged additional fees before receiving a vaccine. It might be that you have more than one option for immunization, including finding a medical provider that would give you the vaccine free of charge, or offer a more straightforward approach to reimbursement if you’re charged. (source)
And what about all the apps for proving you’ve gotten vaccinated? Will that be government-funded or will people pay a few bucks to the app store to download it onto their smartphones? What about people who don’t have phones? What about those who can no longer afford phone service?
I think it’s pretty easy to see that this could become an escalating expense for some and completely unaffordable for others. If you’ve never been in a position where an added $5 expense could make or break your grocery bill, then it may be difficult for you to understand how tough this could be on families who have suddenly found themselves living in ever-deepening poverty.
How will you manage if you can’t prove that you’re covid-free?
Soon, all sorts of businesses and services may require people to prove that they don’t have covid with a recent test (probably not a free one once people are doing the tests for recreational purposes) or proof of vaccination.
But that’s not all. Schools and workplaces may make proof of health mandatory as well. So what happens if you can’t afford your vaccine or documentation? Does that mean your kids can’t go to school and that you can’t go to work? What if you’ve been out of work for months but to get a new job, you must show your proof of health and/or vaccination?
And what about public transit? I’m not talking about flights to Europe – I’m talking about taking the bus or an Uber so you can get to work? What about entering stores? As private businesses, they have the right to choose those with whom they do business as long as discrimination can’t be proven. How can a poor person get from Point A to Point B if they can’t afford vaccination and proof of vaccination?
Who needs a social credit system when you can just shut down entire sectors of society because they can’t provide proof they’ve gotten their shots? You know, like the little rabies tag your dog gets for his collar after he’s vaccinated by the vet.
The transfer of wealth has been enormous…and will continue to be.
Covid and the subsequent government restrictions have all but wiped out the middle class, sweeping millions of formerly financially comfortable families into debt and poverty as they struggle to survive. Countless businesses have collapsed under the weighty mandates. Chapter 11 Bankruptcies are up by 48% this year. Meanwhile, enormous corporations like Walmart, Home Depot, and Amazon have seen soaring profits.
Jim Cramer, a financial analyst for CNBC calls it one of the greatest transfer of wealth in history.
The coronavirus pandemic and corresponding lockdown made way for “one of the greatest wealth transfers in history,” CNBC’s Jim Cramer said Thursday.
The stock market is rising as big business rebounds from state-ordered stoppage of nonessential activity, while small businesses drop like flies, the “Mad Money” host said.
Cramer believes that the recovery of the stock market has little or nothing to do with the recovery of the economy at large – for which his outlook is grim. Although he supports another stimulus package for small businesses, it’s unlikely to be enough.“The bigger the business, the more it moves the major averages, and that matters because this is the first recession where big business … is coming through virtually unscathed, if not going for the gold,” he added. (source)
“The companies that took the money just got a big break: they only need to spend 60% on their employees to get the loans forgiven, down from the original 75%. That’s important, as most small businesses fail because they can’t afford to pay the rent,” Cramer said.
And he’s right – what good will paying the rent do (aside from short-term good for the property owner) if nobody is allowed to patronize the business due to more government-mandated shutdowns?“But, in the end, the stimulus package probably won’t be enough, for one simple reason,” he said. “It’s not going to work because of social distancing.” (source)
What happens next?
As these giant companies rake in the profit and Mom & Pop businesses go under, what happens next? Finding a job right now is next to impossible and it will soon be even harder as the second wave of lockdowns intensifies. More businesses will go under. More jobs will disappear.
And then the much-vaunted vaccine will arrive to save the day (also making a hefty profit for Big Pharma – don’t leave them out when you think about this transfer of wealth.) It’ll save the day for those who can afford it, anyway. And for those who can afford to prove they’ve gotten it.
Poor folks aren’t going to go straight to the front of the line. As it stands, senior government officials are at the front of the line, then healthcare workers, then employees and residents of nursing homes. Next will be essential workers, those with comorbidities, and the elderly. Each state’s governor will decide the pecking order. Dr. Anthony Fauci says that the ordinary person shouldn’t expect a vaccination until April, May, or June of 2021.The rollout of the vaccine isn’t going to happen overnight either. There are over 330 million people in the US, but Pfizer says it expects to send the US 25 million doses by the end of 2020, or enough to vaccinate about 12.5 million Americans, as each recipient will need two doses. That’s roughly the populations of New York City and Los Angeles combined. Moderna, which has a similar type of vaccine as Pfizer, says it will be able to make about 15 million vaccine doses at first, which can treat 7.5 million people (again, two shots per person). (source)
Oh – or if you have the option of making a $25,000 donation to a hospital, you might be able to bump the line and get your vaccination before the peons do.
So don’t expect all this to happen quickly. Don’t expect the jobs to come back, the businesses to reopen, and life to return to normal when the calendar flips to 2021.
And unless you’re rich, you might not ever see that pre-covid normal again.
PanBear
Veteran Member
damn.
i just tried to show someone the clip of the nurse fainting after her shot..
and wouldn't you know it, twitter has deleted it.
anyone know where it is on the alternative vid sites?
her you go ...
Tiffany Dover
1:09
Next will be essential workers,Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
Are We Facing A Future Where Life Only Goes "Back To Normal" For Rich People?
MONDAY, DEC 21, 2020 - 17:00
Authored by Daisy Luther via The Organic Prepper blog,
As jobs and businesses vanish, and prices go up, Americans could soon face another expense – the expense of proving that they’re “healthy.”

While the government tells us that the Covid vaccinations are going to be “free,” are they really? Let’s take a look.
How much will it actually cost to get vaccinated against Covid?
While the government is paying for the vaccine itself, it will still cost money for most people to get injected with it.
So it’s kind of free, sort of, unless somebody charges you but then you might be able to get your money back. Multiply by your number of family members.
And what about all the apps for proving you’ve gotten vaccinated? Will that be government-funded or will people pay a few bucks to the app store to download it onto their smartphones? What about people who don’t have phones? What about those who can no longer afford phone service?
I think it’s pretty easy to see that this could become an escalating expense for some and completely unaffordable for others. If you’ve never been in a position where an added $5 expense could make or break your grocery bill, then it may be difficult for you to understand how tough this could be on families who have suddenly found themselves living in ever-deepening poverty.
How will you manage if you can’t prove that you’re covid-free?
Soon, all sorts of businesses and services may require people to prove that they don’t have covid with a recent test (probably not a free one once people are doing the tests for recreational purposes) or proof of vaccination.
But that’s not all. Schools and workplaces may make proof of health mandatory as well. So what happens if you can’t afford your vaccine or documentation? Does that mean your kids can’t go to school and that you can’t go to work? What if you’ve been out of work for months but to get a new job, you must show your proof of health and/or vaccination?
And what about public transit? I’m not talking about flights to Europe – I’m talking about taking the bus or an Uber so you can get to work? What about entering stores? As private businesses, they have the right to choose those with whom they do business as long as discrimination can’t be proven. How can a poor person get from Point A to Point B if they can’t afford vaccination and proof of vaccination?
Who needs a social credit system when you can just shut down entire sectors of society because they can’t provide proof they’ve gotten their shots? You know, like the little rabies tag your dog gets for his collar after he’s vaccinated by the vet.
The transfer of wealth has been enormous…and will continue to be.
Covid and the subsequent government restrictions have all but wiped out the middle class, sweeping millions of formerly financially comfortable families into debt and poverty as they struggle to survive. Countless businesses have collapsed under the weighty mandates. Chapter 11 Bankruptcies are up by 48% this year. Meanwhile, enormous corporations like Walmart, Home Depot, and Amazon have seen soaring profits.
Jim Cramer, a financial analyst for CNBC calls it one of the greatest transfer of wealth in history.
Cramer believes that the recovery of the stock market has little or nothing to do with the recovery of the economy at large – for which his outlook is grim. Although he supports another stimulus package for small businesses, it’s unlikely to be enough.
And he’s right – what good will paying the rent do (aside from short-term good for the property owner) if nobody is allowed to patronize the business due to more government-mandated shutdowns?
What happens next?
As these giant companies rake in the profit and Mom & Pop businesses go under, what happens next? Finding a job right now is next to impossible and it will soon be even harder as the second wave of lockdowns intensifies. More businesses will go under. More jobs will disappear.
And then the much-vaunted vaccine will arrive to save the day (also making a hefty profit for Big Pharma – don’t leave them out when you think about this transfer of wealth.) It’ll save the day for those who can afford it, anyway. And for those who can afford to prove they’ve gotten it.
Poor folks aren’t going to go straight to the front of the line. As it stands, senior government officials are at the front of the line, then healthcare workers, then employees and residents of nursing homes. Next will be essential workers, those with comorbidities, and the elderly. Each state’s governor will decide the pecking order. Dr. Anthony Fauci says that the ordinary person shouldn’t expect a vaccination until April, May, or June of 2021.
Oh – or if you have the option of making a $25,000 donation to a hospital, you might be able to bump the line and get your vaccination before the peons do.
So don’t expect all this to happen quickly. Don’t expect the jobs to come back, the businesses to reopen, and life to return to normal when the calendar flips to 2021.
And unless you’re rich, you might not ever see that pre-covid normal again.
The first run on this showed few Blacks, too many Whites. So they are going to redefine essential workers to get more Blacks. You old folks can wait because you are predominately White.
Jubilee on Earth
Veteran Member
New Study Shows Mask Mandates Had Zero Effect in Florida or Nationwide, But the Lie Continues
Scott Morefield
|
Posted: Dec 21, 2020 12:01 AM
The opinions expressed by columnists are their own and do not necessarily represent the views of Townhall.com.
Source: AP Photo/Alex Brandon
Obviously, no amount of evidence, data, trends, facts, studies, or science will ever convince most ‘public health officials’ that masks aren’t doing squat to stop the spread of COVID-19. Cases and deaths continue to spike (yes, many of these are super-sensitive PCR test-driven numbers, but still) despite the fact that well over 90% of the country are complying with their absurd mandates. Yet, predictably, the virus keeps going right on virusing, as highly contagious respiratory viruses, unfortunately, tend to do, especially once cold weather hits.
Nevertheless, those of us who are mask skeptics have a difficult chore in front of us. Given that most of the country is under a mask mandate of some form or another, we can point to spikes all day AFTER these mandates were put in place only to have our opponents simply say, “Look how bad it would have been WITHOUT masks!”
It’s a tough argument to counter given the fact that our overlords have sold masking as a low-cost, easy “solution” that’s totally worth it even if they “save one life,” or something (nevermind the health risks - let’s censor docs who talk about those!). So, how DO we prove that things wouldn’t have been worse without masks? One way is to look at data from the few free states remaining.
In Florida, for example, most counties have so far bravely refused to implement mask mandates while others, usually in high population centers, have done so. Justin Hart and the team at Rational Ground (follow them on Twitter here - it’s worth it) just released a comprehensive data analysis of masked vs non-masked counties in the state. A total of 22 of 67 counties in the state have implemented a mask order at some point during the period of May 1 through December 15. It may not sound like many, but these include almost all of Florida’s largest metro areas. To be more than fair, if an area added a mask order at some point during the outbreak, the study’s authors gave a 14 day period to allow time for cases to begin subsiding. “Cases were summed for both mandate and non-mandate jurisdictions and adjusted per 100,000 people for days the mandates were or were not in effect,” wrote the authors, describing the methodology used.
If masks did even close to as advertised, one would expect to see the counties that went maskless to be absolute dumpster fires next to the counties that implemented mandates, right? At the very least, the numbers should favor the masked areas by more than a percentage point or two. So, how did it go? Yep, it was the Mask Cult’s worse nightmare:
“When counties DID have a mandate in effect, there were 667,239 cases over 3,137 days with an average of 23 cases per 100,000 per day. When counties DID NOT have a countywide order, there were 438,687 cases over 12,139 days with an average of 22 cases per 100,000 per day.”
In other words, counties with mask-mandates in place actually did WORSE than those that refused to implement them. (Yeah, color me shocked.) The authors even accounted for population density in their analysis, suggesting that it didn’t have an impact on the numbers because four of the 12 most populous counties in Florida never had a countywide order. “When the eight DID have an order in effect, there were 64 cases per 1,000. In periods 11 of 12 DID NOT have one, there were 40,” they wrote.
“But that’s just Florida,” you say. “They’re weirdos anyway. Surely masks have worked in the rest of the country.” Well, I’m glad you asked! The good folks at Rational Ground went on to compare national numbers, pitting the states that resisted the urge to impose a statewide mask mandate against those that masked up. How did those compare?
“When states DID have a mandate in effect, there were 9,605,256 cases over 5,907 total days and averaged 27 cases per 100,000 per day. When states DID NOT have a statewide order there were 5,781,716 cases over 5,772 total days averaging 17 cases per 100,000 people per day.”
So there you have it, incontrovertible data evidence that mask mandates do little to nothing to stop or even slightly curb the spread of COVID-19. If masks were the answer, wouldn’t you expect to see a drop in cases not long after mask mandates are implemented? At the very least, wouldn’t you expect to see cases level off and STAY leveled off? What you would NOT expect would be what has actually happened, for cases to spike as they have done since November seemingly all across the country, regardless of whether or not a mandatory masking policy was in place.
Further, wouldn’t you also expect states and areas that MASKED HARRDERRR than anyone else, states like California that have the ‘bold leadership’ to insist the plebes under their control mask up outside on hiking trails and sitting alone in parks, to have the lowest case counts of all? Just look at the latest per capita numbers there compared to Florida and tell me with a straight face that mask mandates ‘work.’ As Dave Rubin adeptly pointed out earlier this month, Florida’s numbers “should be ten times higher” than California’s. I mean, nobody is asking for masks to work perfectly, but hell, shouldn’t we expect SOME performance?
Numbers and data like this get down to the brass tacks. We can pit our doctors, scientists, and epidemiologists against their doctors, scientists, and epidemiologists on the actual science behind whether forcing people to put a moist, bacteria & virus-laden piece of cloth over the holes through which they breathe actually works to contain a virus that’s infinitesimally smaller than its threads (and yes, there are plenty of doctors, scientists, and epidemiologists on Team Reality too, and a bunch of them are on this must-follow Twitter list!), but if mask-mandates aren’t actually WORKING to curb the spread, why do we have them in place?
It’s complete and utter nonsense, of course. You know it, I know it, and the powers-that-be likely know it too. So why do they insist on continuing the charade? Whatever it is, it has NOTHING to do with either public health or real science.
Yep, Michigan is a great case study for that. The mask mandate has been in place since July. You cannot even pop into a gas station for a second without a mask. Every business has a big sign on the doors. Even back in the summer they were required at the outdoor farmers markets and such.
Yet despite a very compliant state population doing their part to “slow the curve,” we are still the 10th in the country in number of cases. If the masks worked that well, we should be way lower on the list.