Part 2 of 3
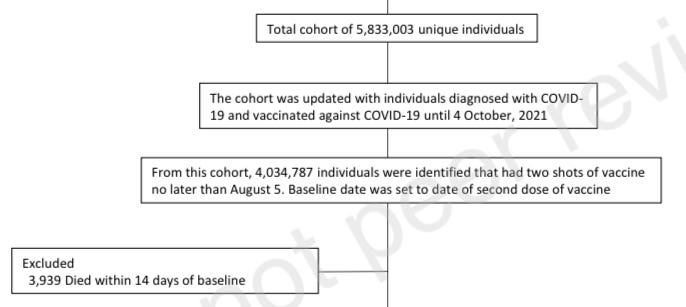
The number of post-COVID-19 myocarditis and pericarditis adverse events by sex (a) and the administered vaccine dose (b). The x-axes show the adverse event counts for each COVID-19 vaccine shown on the y-axes. Considering VAERS reports processed as of 2 September 2021

And although apologists for Big Pharma at the
New York Times and elsewhere are consistently trying to downplay this condition as
"mild and temporary", there are serious justifiable concerns over the long-term health effects that this may have:

Young male mortality on the rise
Unsurprisingly, ever since the vaccine rollout for younger adults and adolescents, several countries have witnessed a disturbing rise in excess mortality amongst young males.
In Austria, a massive increase in excess mortality for 2021 has been found in young men aged 15 and above. Compared with the previous year, deaths are up 32% for ages 15-24 and 21% for ages 25-34. A less drastic increase was also demonstrated in males aged 35-44.

© Report24.news
These deaths cannot be attributed to COVID, because the mortality rate among females has shown the exact opposite trend, with fewer deaths being reported for all ages.
England and Wales have also witnessed a similar trend among male children aged 10-14.
The Exposé compiled official ONS data which reveals that since the rollout of the COVID vaccine for children aged 12+, there has been an 86% rise of deaths in males compared with 2020. Astoundingly, week 40 saw a 600% increase, followed by week 41 which showed a equally disturbing 200% increase.

© Office for National Statistics UK
Deaths of male children 2020-2021
Another investigation by The Exposé looked at deaths among teens aged 15-19 since the beginning of vaccine administration for this age group. It showed a staggering 63% increase for males, along with 16% for females.
Remarkably, the third week of June found a 500% increase in male deaths, along with 700% in the week ending September 3rd. In contrast, the same period only found a 17% increase among female deaths:

© The Expose
At this point, the data is quite clear that something is killing children, adolescents, and young adults at a much higher rate than before mass-vaccination campaigns were introduced. The data also shows that males are being disproportionately affected by vaccine injury, and this is reflected in the available mortality statistics.
In order to attempt to make sense of these findings and understand why this is happening, we first need to examine the underlying mechanisms behind how the vaccines inflict such damage.
Mechanisms of vaccine injury and death
The overwhelming majority of vaccine reactions have been documented after administration of the mRNA-based formulations (Pfizer and Moderna). However, a significant portion also occur with adenoviral DNA vector vaccines (J&J and AstraZeneca). It's worth noting that all of these 'vaccines' share important similarities which will eventually help to explain the severity and frequency of adverse events:
- Each of the above vaccines are based on novel technology which is different from traditional inactivated viral vaccines
- Each of the above vaccines are designed to instruct human cells to synthesize foreign SARS-CoV-2 spike protein (which I will refer to as SPIKE)
To give a brief overview of the mechanism of action in these types of technology:
The adenoviral DNA vector vaccines contain DNA which codes for SPIKE encased within a non-replicating virus (a chimpanzee adenovirus). After injection, the viral vector penetrates the cell, enters the nucleus and yields messenger RNA (genetic instructions for protein synthesis). This mRNA is then used as a template by our own cellular machinery to start synthesising spike protein. SPIKE fragments then migrate to the surface of the cell, where they are later identified as foreign by the adaptive immune system, which begins generating protective antibodies against this protein. The aim is to provide future immunological memory through antibody formation against any virus which also expresses SPIKE.
On the other hand, mRNA based 'vaccines' do not use an adenovirus vector, but instead encapsulate modified mRNA within a lipid nanoparticle emulsion containing polyethylene glycol, and this functions to facilitate mRNA delivery into the cell. In a roundabout similar way to the adenovirus DNA vector, the newly-delivered mRNA provides the necessary instructions for the cell to begin synthesising copious amounts of foreign SPIKE, which then migrate to the cell surface and initiate an adaptive immune response. Once again, this is with the aim of enhancing long-term antibody production against any future viral threat.

© Martínez-Flores, D. et al. (2021) "SARS-CoV-2 Vaccines Based on the Spike Glycoprotein and Implications of New Viral Variants", Frontiers in Immunology, 12. doi: 10.3389/fimmu.2021.701501.
Each of the above vaccines are injected into the arm, the contents of which were originally assumed to stay within the deltoid muscle and perhaps the local lymph nodes whilst evoking antibody production. Researchers believed that SPIKE protein did not enter into systemic circulation.
However, more recent evidence showed the exact opposite to be true, demonstrating measurable levels of SPIKE in the blood of mRNA vaccine recipients.
In fact, another
pharmacokinetic study in Japan using Pfizer's vaccine technology showed mRNA-containing lipid nanoparticles in practically every organ, including the brain, heart, liver, adrenal glands, kidneys, intestine, sex organs, and spleen, where they stayed for much longer than was originally expected.
This means that SPIKE is literally being expressed in tissues all throughout the body, in much higher levels than would ever be present in viral infection, and it sticks around.
Why is this relevant? SPIKE protein was originally considered to be a perfect antigen because of its supposed lack of ability to cause harm to host tissues. According to the CDC,
modified SPIKE protein is a "harmless antigen".
But the bulk of evidence now shows that, far from being a "harmless antigen", SPIKE is in fact an extremely toxic molecule capable of initiating severe, systemic inflammation. Ongoing exposure to this poison might help to explain most, if not all, of the vaccine adverse events and deaths.
Toxicity of SPIKE protein
Upon contact with cells, SPIKE has a very high affinity for angiotensin converting enzyme (ACE2) receptors, ubiquitously expressed on the surface of numerous cell types located in the lung, brain, blood vessels, heart, and many other organs. In COVID-19 infection, ACE2 receptor binding is considered to be the primary mechanism of viral entry into the cell. After binding, ACE2 is internalized and degraded, which causes a loss of receptor function. Ordinarily, ACE2 is involved in systemic regulation of the cardiovascular system and serves as an important regulator of renin-angiotensin system (RAS). A
large number of studies have demonstrated anti-inflammatory, antioxidant, anti-apoptotic and anti-fibrotic properties of ACE2 receptor function, and it is considered highly protective against cardiovascular injury of all sorts, including myocarditis.

González-Rayas, J. et al. (2020) "COVID-19 and ACE -inhibitors and angiotensin receptor blockers-: The need to differentiate between early infection and acute lung injury", Revista Colombiana de Cardiología, 27(3), pp. 129-131. doi: 10.1016/j.rccar.2020.04.005.
ACE2 receptor binding not only disables/blocks its ordinary function, but initiates cell signalling cascades which stimulate pro-inflammatory gene expression and trigger the inflammatory response. SPIKE protein alone is capable of causing widespread vascular inflammation.

© Suzuki, Y. and Gychka, S. (2021) "SARS-CoV-2 Spike Protein Elicits Cell Signaling in Human Host Cells: Implications for Possible Consequences of COVID-19 Vaccines", Vaccines, 9(1), p. 36. doi: 10.3390/vaccines9010036.
Any tissue or cell which expresses ACE2 receptors is therefore extremely vulnerable to the effects of this protein. In endothelial cells lining the blood vessels, SPIKE triggers an inflammatory cascade resulting in
vascular endothelial dysfunction,
impaired nitric oxide bioavailability which reduces the capacity for vasodilation, and induces vasculitis. SPIKE was recently shown to
increase vascular endothelial permeability through disrupting tight junction barrier proteins, and this effect is thought to further increase damage to the cardiovascular system and systemic inflammation.
Activation of the complement pathway and other inflammatory mediators triggers a systemic procoagulant state. SPIKE binding with ACE2 on platelets was shown to cause dose-dependent platelet aggregation, potentially leading to lethal thrombosis (blood-clotting). Microangiopathy (disease of the small blood vessels) is not limited to the pulmonary capillaries but can occur throughout the entire vascular system and affect every organ including the brain, liver, and heart.

© Angeli, F. et al. (2021) "SARS-CoV-2 vaccines: Lights and shadows", European Journal of Internal Medicine, 88, pp. 1-8. doi: 10.1016/j.ejim.2021.04.019
Schematic mechanism of action of mRNA and adenoviral vector DNA vaccines and their potential cardiovascular interactions throughout the activation of the immune system and the interaction between free-floating Spike proteins and ACE2
Even short-term exposure to spike protein was shown to produce
long-term changes in gene expression which facilitates chronic inflammation.
SPIKE was also shown to contain a superantigenic region capable of activating T-cells, resulting in massive production of proinflammatory cytokines including IFNγ, TNFα, and IL-2. This systemic "hyperinflammatory" cytokine storm response is responsible for multi-organ tissue damage. This protein was
recently shown to literally strip the lipids away from cell membranes in the absence of ACE2 receptors, demonstrating a direct destructive effect of SPIKE on cell membranes.
SPIKE not only binds with ACE2, but has been shown to enhance systemic inflammation through binding Toll-like receptor 4 (TLR4). TLR4 detects pathogen-associated molecular patterns such as bacterial lipopolysaccharide and, like other TLRs, is responsible for modulating the innate immune response. TLR4 can drive hyperinflammation through activating proinflammatory transcription factors such as NF-Kappa Beta. A
recent animal study demonstrated increased generation of proinflammatory cytokines, cardiac hypertrophy (enlarged heart), and decreased cardiac systolic function in mice treated with SPIKE, and the authors conclude that TLR4 activation might be one of the driving mechanisms behind cardiac injury.
SPIKE was recently shown to
bind with integrin proteins in the lung, and
Neuropilin-1, a transmembrane protein in the brain involved in neuronal development and axonal growth. The effects of this are not yet known.
SPIKE also has high affinity for monoamine oxidases, equal to its affinity for ACE2. MAOs (A and B) are a class of enzyme intrinsically involved in the regulation of neurochemicals. These function to metabolize (break down) amine neurotransmitters such as dopamine, serotonin, noadrenaline, and phenylethylamine. Functional abnormalities in MAO have been associated with behavioural/neuropsychiatric disorders and some neurodegenerative conditions.
SPIKE-MAO complex formation was shown to significantly reduce enzyme activity by lowering enzyme affinity toward its substrate neurotransmitters. This is expected to lead to an excess of amine neurotransmitters which is likely to significantly alter overall neurochemical balance and mood/cognition/brain function.
Another major point of concern is the theoretical ability of SPIKE to trigger autoimmunity.
Vaccine-induced autoimmunity has been demonstrated for several other conditions. This is thought to occur through cross-reactivity between foreign vaccine-derived antigens with host proteins.
Part 2 of 3





















































































")