And, just like that, it was over. This is HUGE news folks. In bureaucrat speak, this is a near-complete cave-in to the actual facts: No symptoms? No problem. Vaccinated or unvaccinated? Same guidance. Exposed? No need to even quarantine. Students exposed? They can stay in class, what the hell...

peakprosperity.com
(fair use applies)
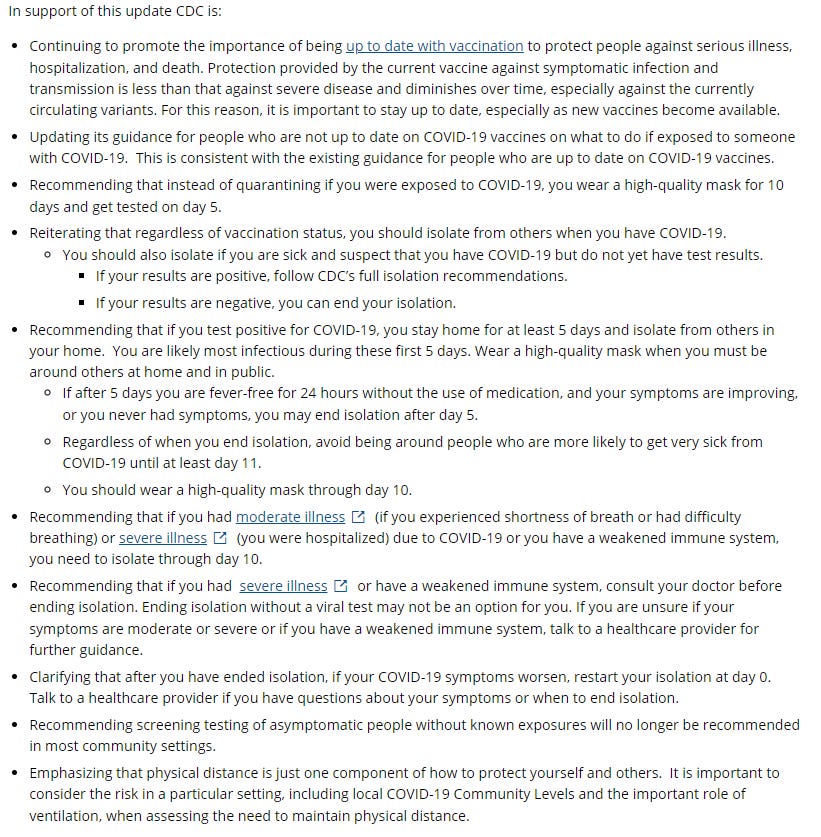
WOW!!! CDC Completely Reverses Course. IT’S OVER!
By Chris Martenson on
Friday, August 12th, 2022
And, just like that, it was over.
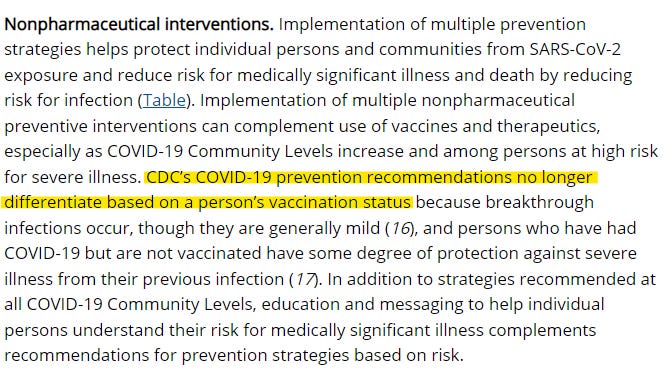
This is HUGE news folks. In bureaucrat speak, this is a near-complete cave-in to the actual facts:
- No symptoms? No problem.
- Vaccinated or unvaccinated? Same guidance.
- Exposed? No need to even quarantine.
- Students exposed? They can stay in class, what the hell, right?
If you managed to maintain your integrity through this awful period of time, congratulations!
You are one of the rock stars of this story. You are a solid individual who has courage and stood firm and tall when it mattered most.
As for the people who didn’t, some can be forgiven. But many cannot.
Those who could have and “should” have known better? The doctors who failed to utilize known and proven early treatments to save lives? The public health authorities that locked people down and forced masks onto children’s faces without a shred of supporting science to back those decisions? Medical hospital administrators who took the monetary bait and forced patients onto toxic and deadly regimens of Remdesivir and ventilators (again, without any supporting evidence!). The NIH treatment panel that still –
to this day –
does not recommend vitamin D, or any of the other actual safe and effective early treatments?
Sorry,
not sorry, those people need to suffer real and lasting public consequences. Some doctors should lose their licenses. Some bureaucrats need to lose their jobs while others need to go to trial.
I feel most acutely for those who got caught up and suffered terribly as a result. I feel truly awful for all the people prevented from being at a loved one’s passing, or who ,as a condition of continued employment, were coerced into getting Covid jabs they neither wanted nor needed.
There are far too many tragic cases out there. Far too many young lives were lost and continue to be lost. I am angry that it happened and at the petty, ignorant bureaucrats who forced it to happen. “Sudden Adult Death Syndrome” is a thing now, and the attempts to normalize it by the press have left me thinking that those companies and journalists who engaged in this ought to be barred for life from ever being in the business again.
Here are a few out of many such candidates:
One prominent case of an avoidable tragedy was that of 17-year-old Sean Hartman:
Dan Hartman is sure that his hockey-loving son died from a COVID vaccination, but he’s being told very little about what happened. The Ontario dad says he wants answers about the sudden death of 17-year-old Sean.
“I cannot grieve him properly without the truth. It’s different if someone dies in a car accident or disease or suicide. This is none of them—this is unknown,” said Hartman in an interview on NTD’s “The Nation Speaks” program aired on July 30.
According to the Beeton Athletic Association Cash Draw’s tribute to Sean, he began playing hockey at age 5 and went on to play for the TNT Tornadoes in New Tecumseth, Ontario, for three years before returning to his hometown of Beeton in his major Bantam year.
Due to the COVID-19 pandemic, the Ontario Minor Hockey Association implemented a policy that required players aged 12 and over to be vaccinated or risk not being able to play.
Hartman said that Sean decided to get the shot last August in order to continue playing, as hockey was his passion. In Ontario, there is no minimum age of consent under the Health Care Consent Act, which means youth of Sean’s age can get vaccinated without parental consent.
“So, on August 25, he had the Pfizer vaccine. And on August 29, he went to the emergency [room]—he had brown circles around his eyes, and a rash and he was vomiting,” Hartman said.
“They sent him home with only Advil. The doctor didn’t do two blood tests that he should have done. I’ve been told by another doctor that he should have done them. And on the morning of September 27, he was found dead on the floor beside his bed.”
There are thousands and thousands of similar and tragic cases. Too many.
All along the way, I have been saying the same thing as Drs. McCullough, Malone, Urso, Kory, Marik, Rose, and Steve Kirsch among many others; the Covid vaccines should
never have been put into every possible person.
There should have been an age and risk stratification approach. Only some people should have gotten them, but never into healthy children.
Never.
The demonization of even simple and entirely appropriate questioning was horrific and continues on to this day, as
I outlined in a recent video on “Fact Checkers” wherein I covered
a truly horrific New York Times article by Sheera Frenkel. In it, Ms. Frenkel went overboard on hyperbolic, emotionally-laden verbiage in a brazen attempt to mischaracterize any questioning by parents as being entirely due to misinformation, conspiracy theories, and a black-and-white stance as “anti-vaxers.”
Well, if hesitant parents are anti-vaxers, then we have to say that those folks are in the vast majority (and rightly so) while it is Ms. Frenkel and the New York Times who are in a tiny minority that is horribly out of alignment with the data.
Far from being fringe, the view that children do not need the Covid-19 jab, it turns out, represents either a significant minority (for older age cohorts) or indeed an overwhelming majority (for younger) of parents both within the U.S., the UK and elsewhere.
Are the 95% of U.S. parents who have declined to get their 0-5 year olds vaccinated for Covid-19 ‘anti-vax?’ What about the 89% of UK parents who as of the end of July had declined vaccination for their 5-11 year olds?
Of course they aren’t. They are simply recognising the reality that the extreme age discrimination of Covid makes vaccination unnecessary for the vast majority of otherwise healthy kids, as does infection-acquired immunity.
How it ever came to be that “the Left” became the biggest cheerleaders of court-proven corrupt pharma companies is for the psychologists and social scientists to unravel. Maybe we could include some ethicists and prosecutors as well.
Early Treatments
More importantly and tellingly in this sad saga, early treatments should have been discovered and wisely used, as they were in many other countries.
The simple fact that the pair of charts displayed below
weren’t ever a healthy and vigorous topic of discussion speaks volumes about just how bad the corruption really was.
For more than a year, Uttar Pradesh has been kicking the ass of every western nation in dealing with Covid and they did it with simple, effective early treatment packages that looked like this:
The kit included:
- Ivermectin
- Azithromycin (Z-pac)
- Doxycycline
- Zinc
- Vitamins D & C
It’s plain as day that this approach worked and worked very well, not just at keeping deaths down, but cases too. With fewer cases that were less serious, it’s a pretty safe bet that they managed to keep long Covid down as well.
Dr. Pierre Kory recently penned an exquisitely good piece on exactly how Uttar Pradesh accomplished their astonishing feat. It all began with a leader who was unafraid to begin by rooting out corruption:
Uttar Pradesh (UP) is a state in the north of India with a population of 231 million people. It’s the home of the Taj Mahal. If it were a country, it would be the sixth largest in the world.
In my view, the foundation of UP’s historic achievement rests on the integrity of its Chief Minister (CM) Yogi Adityanath. He is a Hindu monk and known for his policy of zero tolerance against corruption. The importance of this quality cannot be overstated, especially given the last 2 years of unceasing corruptions of medical science and public health policy that continuously emerge each day.
Since taking office as CM over three and half years ago, he took action against 775 corrupt officials in UP from the Indian Administrative Service and the Indian Police Service. His leadership during COVID should serve as a historically inspiring example to politicians. They should take note of how honest, forthright policies designed with the singular goal of serving and protecting the public good can succeed in politics.
In March of 2020, Yogi Adityanath convened (and chaired throughout) a committee of 11 senior government officials tasked with managing different aspects like surveillance and contact tracing, testing and treatment, sanitization, containment, enforcement, doorstep delivery, issues of migrants, communication strategy etc.
Note that UP started out strong right from the beginning. Early on in the pandemic, in March 2020, taking the lead from India’s national protocol, UP immediately adopted hydroxychloroquine for use in prevention of COVID for all its Health Care Workers as well as household contacts of all laboratory confirmed cases.
Recall that HCQ’s promise in treatment had been known since the original SARS pandemic, a fact long ago highlighted by Anthony Fauci. Yet in COVID, when its threat to Pharma as an effective treatment became reality, Fauci essentially led the first Disinformation campaign against a repurposed drug in the pandemic. His campaign is described in RFK Jr’s book, The Real Anthony Fauci in the deeply referenced first section of Chapter 1, called “Killing Hydroxychloroquine.”
Then, in August 2020, UP broke from the Feds and switched their protocol to ivermectin after an “experiment” in UP’s Agra, a city of 1.6 million inhabitants. The head of the state’s Rapid Response Team units, Dr. Anshul Pareek, had decided to conduct a study of ivermectin as a preventive agent based on a report from a veterinarian (to be fair, it was also based on other promising clinical reports in humans).
UP immediately started administering ivermectin to close contacts of positive cases in the district and noticed profoundly positive results. Based on these observations, the state health authorities gave the green light to use off-label ivermectin not only in prevention… but in treatment. This was their protocol for use of ivermectin:
- Close contacts of COVID-19 patients
- Health care workers
- General care of COVID-19 patients
Notice that UP’s government did what my colleagues and I had been imploring since the pandemic began. Employ a risk/benefit decision-making analysis in an emergency. Like you do in war. Even if the view was that the clinical trials evidence for HCQ or IVM was “insufficient,” the evidence for harm was near nil, while the evidence for harm of widespread untreated COVID was obviously catastrophic.
[continued next post]