I bet he thinks that because he is the House majority whip he has more clout than a mere governor. And, of course, he's a democrat. They think they get to tell everyone else how to live their lives, institutions and businesses.My comment: How does a representative from South Carolina have any say over what a governor of another state runs their state? I never heard of this before....
~~~~~~~~~~~~~~~~~~~~~
(fair use applies) BOLDING MINE
Clyburn hits DeSantis: Reverse or explain ‘inexplicable’ decision over child COVID-19 vaccines
House Majority Whip James Clyburn (D-S.C.) demanded that Florida Gov. Ron DeSantis (R) reverse or explain his decision after he declined to order COVID-19 vaccines for children under 5 years of age. In a letter sent Friday, Clyburn, the chairman of the the House Select Subcommittee on the...news.yahoo.com
Clyburn hits DeSantis: Reverse or explain ‘inexplicable’ decision over child COVID-19 vaccines
Sarakshi Rai - The Hill
Fri, June 17, 2022, 12:43 PM
House Majority Whip James Clyburn (D-S.C.) demanded that Florida Gov. Ron DeSantis (R) reverse or explain his decision after he declined to order COVID-19 vaccines for children under 5 years of age.
In a letter sent Friday, Clyburn, the chairman of the the House Select Subcommittee on the Coronavirus Crisis, added that he was concerned by DeSantis’s public comments that he is opposed to dedicating any state resources to vaccinating young children against COVID-19.
He stressed that every state but Florida ordered vaccines after the Food and Drug Administration (FDA) on Friday gave the green light to COVID-19 vaccines for children ages 5 and younger.
Clyburn said that because of the governor’s “deliberate inaction,” pediatricians and family doctors across Florida are currently unable to order doses.
“There is not going to be any state programs that are going to be trying to get COVID jabs to infants and toddlers and newborns,” DeSantis said on Thursday. “That’s not something that we think is appropriate, and so that’s not where we are going to be utilizing our resources.”
Clyburn argued that DeSantis’s opposition would prohibit families from accessing vaccines at federal vaccination sites even if they order vaccines directly from the federal government.
“Your decision to reject these vaccines could deny Florida parents the ability to make their own decisions on what is best for the health of their children—and could deny some Florida children the ability to live long and healthy lives,” he wrote.
Clyburn also pushed back on the Florida governor’s statements that his administration was “affirmatively against the Covid vaccine for young kids” because they “have zero risk of getting anything.”
He stressed that despite COVID-19 infections posing less of a risk to younger children, the risk factor is “significantly above zero.”
The House majority whip stated that more than 2,600 American children under the age of 5 have been hospitalized with COVID-19, and 442 have died from the disease.
“Even mild coronavirus infections can cause serious long-term effects for children, such as multisystem inflammatory syndrome—a rare but potentially deadly inflammatory disorder—and long COVID, which can cause severe fatigue, cognitive difficulties, muscle and joint pain, and other symptoms that persist for months,” he added.

You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
CORONA Main Coronavirus thread
- Thread starter Heliobas Disciple
- Start date
-
- Tags
- coronavirus
Craftypatches
Veteran Member
I had Covid 2 weeks ago and yesterday I got run down from lack of sleep and having a garage sale and now the Covid has come back and I tested positive again. Can it return if you have a weakening in your immune system?
Heliobas Disciple
TB Fanatic
Here's the article referred to in that tweet:

New Covid wave explained as 'more dangerous' virus circulating in 3 UK hotspots
The latest Office for National Statistics figures suggest a rise in Covid cases across England and Northern Ireland since the start of June, driven by BA.4 and BA.5 Omicron strains
 www.mirror.co.uk
www.mirror.co.uk
New Covid wave explained as virus now 'more dangerous' and top 3 UK hotspots revealed
The latest Office for National Statistics figures suggest a rise in Covid cases across England and Northern Ireland since the start of June, driven by BA.4 and BA.5 Omicron strains
By Ryan Merrifield News Reporter
12:24, 15 Jun 2022 | Updated19:31, 15 Jun 2022
Britain could be facing a new wave of Covid infections driven by Omicron subvariants BA.4 and BA.5, with three counties in particular seeing a massive surge.
Data from the Office for National Statistics (ONS) up to June 2 indicates England and Northern Ireland are starting to see a rise in cases.
However the trends were unclear for Wales and Scotland.
Infection levels are estimated to have risen in London, north-west England and south-east England, with early signs of an increase in eastern England.
Rutland in the East Midlands appears to be have seen the biggest recent surge.
The county, which is bounded to the west and north by Leicestershire, to the northeast by Lincolnshire and the southeast by Northamptonshire, has seen a jump of 233% in cases over the last 14 days.
In data collected by the New York Times from Data for the UK Department for Health and Social Care, Public Health England and the Chief Medical Officer Directorate, it shows the infection rate is 31 per 100,000.
Other areas to see a surge include North East Lincolnshire with 132% and Middlesbrough with 179%.
Experts worry these latest mutations may have evolved to infect lung tissue, as did the earliest forms of the virus, making them more dangerous.
BA.4 and BA.5 - first detected in Africa in January and February - were designated as variants of concern in the UK on May 20.
Though the bulk of infections appear to continue to be down to the dominant BA.2 variant.
The UK Health Security Agency is also monitoring BA.5.1 - an offshoot of BA.5 - and the BA.2.12.1 subvariant, which remains the dominant strain in the US.
Some 797,500 people in private households in England were likely to test positive for Covid-19 in the week ending June 2, the equivalent of about one in 70, the ONS said.
This is up week on week from 784,100, which was also about one in 70.
Wales has seen Covid-19 infections increase very slightly to 40,500 people, up from 39,600, though both estimates are equivalent to around one in 75 people and the ONS describes the trend here as "uncertain".
Immunity from the booster vaccines is waning in the majority of the population, with only over-75s and extremely vulnerable groups offered the spring dose.
Meanwhile, infection from BA.1 or BA.2 may not protect against the newest variants.
“It looks as though these things are switching back to the more dangerous form of infection, so going lower down in the lung,” Dr Stephen Griffin, a virologist at the University of Leeds, told the Guardian.
In response to whether the virus is on the verge of turning into the common cold, he added: "It clearly isn’t, and there’s no pressure on it to do that, really."
Separate figures show the recent fall in the number of people in hospital with the virus may have come to a halt.
Some 4,602 patients in England had Covid-19 on June 13, up 12% on the previous week, while in Wales the figure looks to have levelled off at around 250 to 260.
Patient numbers in both nations had previously been on a steady downwards trend since early April, following the peak of the Omicron BA.2 wave.
But they remain well below the levels reached in all previous waves of the virus.
Despite the rise in cases, the ONS figures show a 55% week-on-week drop in Covid-related deaths in the seven days up to June 3, with 186 fatalities registered in that time mentioning the virus on the death certificate.
It's the lowest number since July 2021.
However, the latest total covers a period that includes the bank holidays marking the Queen's Platinum Jubilee on June 2 and 3, when most register offices were closed.
This means fewer deaths were registered than would normally be the case.
The disruption to registrations caused by the bank holidays is likely to have exaggerated the size of the week-on-week drop in registrations.
But it is the fifth week in a row the figures have shown a decrease, suggesting Covid-19 deaths are continuing on a clear downwards trend.
Heliobas Disciple
TB Fanatic
OK, so this was interesting. My first impression was he was a podcaster reading someone else's study so i did some digging. Took me about 15 or so minutes and I got to the bottom of it to my satisfaction. Indeed, he was reading from someone else's post - supposedly written by a Dr. Rob Oswald. But Rob Oswald did not write it, it was written by someone anonymous and attributed to him to give the post credibility. I don't know if what he was saying was true or not (more on that next) but as to who said it - that part is not true.
I know this is from Snopes, not everyone's favorite debunking site - but it has all the info in one place so I'm using it:
Did Dr. Rob Oswald Claim COVID-19 Was a Hoax?
Purveyors of misinformation often falsely attach trusted names to fraudulent claims in order to make their misinformation appear more credible.
 www.snopes.com
www.snopes.com
Did Dr. Rob Oswald Claim COVID-19 Was a Hoax?
Purveyors of misinformation often falsely attach trusted names to fraudulent claims in order to make their misinformation appear more credible.
Dan Evon
Published: 28 December 2020
Claim: Virologist Dr. Rob Oswald wrote a lengthy Facebook post calling COVID-19 a hoax.
Rating: Misattributed
Origin:
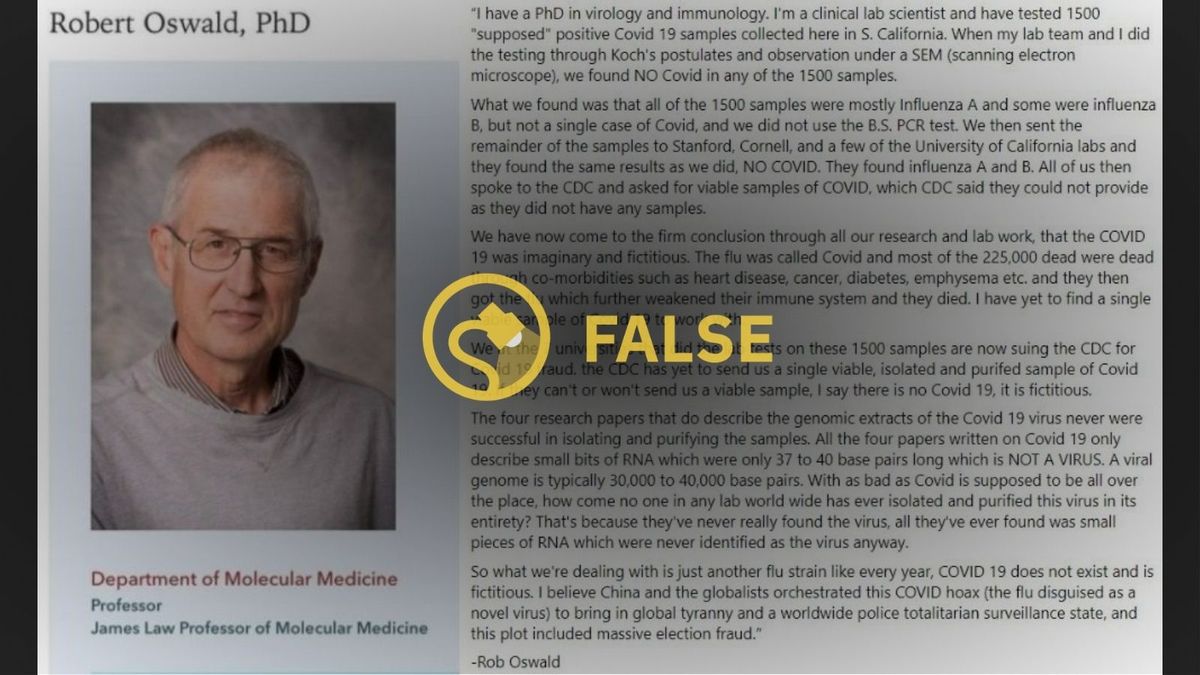
In December 2020, a lengthy message arguing that “COVID 19 does not exist” was widely circulated on social media. This post proved popular in part because it was attributed to a person who seemingly had the credentials to make such a determination: Dr. Rob Oswald, a virologist and immunologist at Cornell University’s Department of Molecular Medicine.

Here’s the introductory paragraph of this viral message:
“I have a PhD in virology and immunology. I’m a clinical lab scientist and have tested 1500 “supposed” positive Covid 19 samples collected here in S. California. When my lab team and I did the testing through Koch’s postulates and observation under a SEM (scanning electron microscope), we found NO Covid in any of the 1500 samples.
While the included image in this viral post does show a real person named Oswald, he did not write this post.
Purveyors of misinformation often falsely attach trusted names to fraudulent claims in order to make their misinformation appear more credible. If a doctor wrote this post, then the logic goes, there must be something to it. But Oswald had nothing to do with the viral message posted above.
This text has been circulating online since at least Dec. 6, when an anonymous Blogger named “Sojourner” posted it in the comments section of an article published at Wadeburleson.org. At the time, the text was not attributed to Oswald or any other medical professional, and the post’s apparent author, Sojourner, noted in another comment that he/she was “not a professional,” was “merely a hillbilly,” and had simply copied and pasted the message.
Since many people may not find an anonymous message posted by a “hillbilly” to be credible, subsequent versions of this post falsely claimed that the message had originated with a reputable source, Oswald. But that, of course, is not the case.
Shortly after this message went viral, Oswald updated his webpage at Cornell University to include a statement about COVID-19. He wrote:
COVID-19 is real. Any Facebook post that suggests otherwise is a hoax and is not true. Wear a mask, practice social distancing, and get the vaccine when it becomes available.
When we reached out to Oswald, he elaborated and told us that he was “horrified by the contents” of this message, and that this post was not connected to him or Cornell University.
Oswald said:
I certainly did not write this and am rather horrified by the contents.
[…]It lists the author as a virologist and immunologist living in southern California–neither of these descriptions fit me. Also, it mentions Cornell and a supposed lawsuit against the CDC. Cornell has been at the forefront of COVID research and testing, committing huge resources into maintaining the spread of the virus. To attempt to link Cornell to the contents of this letter is disappointing to say the least.
In addition to saying that neither he nor the university had anything to do with this message, Oswald also explained that the contents of this viral message were also dubious.
Oswald said:
The contents are just completely wrong. The virus is incredibly well studied with many full genome sequences from patients, contrary to the suggestion that only 40 or so nucleotides have been sequenced. You can see the vast extent of the work as compiled by the National Library of Medicine: NCBI SARS-CoV-2 Resources
Not only that, but the molecular structure of at least the spike protein of the virus has been solved by cryo-EM (one of our former students is an author on this work): https://science.sciencemag.org/content/367/6483/1260
So to suggest that no virus actually exists is just false.
~~~~~~~~~~~~
I also found two videos about this.The first one the doctor in it debunks it, the second one he debates the podcaster in the first video. I haven't watched either, I went through this exercise because I like to get to the bottom of things I see posted and to have as much info as possible to weigh everything presented. Everyone who is interested should watch the videos and come to their own conclusion. I am not a scientist and not taking sides, I just wanted to clarify what was in that first video
")
Derek Knauss (actually Patrick Gunnels) does not know how to test for COVID
6 min 16 sec
Debunk the Funk with Dr. Wilson
Where you can contact me: https://www.facebook.com/DocWilsonDeb... I've revised the title of this video to reflect the fact that the man in the video is not "Derek Knauss," nor is he a doctor of any kind. He is a man named Patrick Gunnels and was likely reading a bogus blog post that was falsely attributed to Dr. Rob Oswald. https://www.snopes.com/fact-check/rob... Koch’s postulates for viruses: https://www.thelastamericanvagabond.c... Real high-resolution images of purified SARS-CoV-2 virus: https://science.sciencemag.org/conten... Scanning electron microscopy is not enough to differentiate between Influenza viruses and coronaviruses: https://www.frontiersin.org/articles/... https://www.thermofisher.com/blog/mic... SARS-CoV-2 isolate samples are available for researchers to buy: https://www.cdc.gov/coronavirus/2019-... https://www.beiresources.org/BEIHighl... Full genome sequence of SARS-CoV-2: https://www.ncbi.nlm.nih.gov/pmc/arti... Song used in outro: Funky Party by Lobo Loco Opinions are my own.
COVID Conversations Ep. 1: Dr. Wilson vs. Patrick Gunnels (aka "Derek Knauss") - Is SARS-CoV-2 real?
55 min 01 sec
Debunk the Funk with Dr. Wilson
Of course SARS-CoV-2 is real. But can I convince Patrick of that? So, previously I made a video debunking "Derek Knauss." Turns out, the guy in the video is actually named Patrick Gunnels and the video was him just reading a forum post. Still unclear why people clipped his original video and called him "Derek Knauss." Anyway, he doesn't think SARS-CoV-2 is real. Here is my debate with him. Here are some links to support what I say in this debate. Original isolation: https://www.nejm.org/doi/full/10.1056... All isolates that have been sequenced since then: https://nextstrain.org/ncov/global Some more information on PCR: https://virologydownunder.com/putting... Kary Mullis's original PCR patent which states diagnostics as an application: https://patentimages.storage.googleap... UPDATE on Patrick's comments about Drosten's credentials (information courtesy of Thomas Mohr, thanks Thomas): Doctorate of Christian Drosten: this is a misconception of the academic system of Germany prior and post the "Bologna Process" (https://en.wikipedia.org/wiki/Bologna...) which is the harmonization of degrees within Europe. Drosten has an MD, which requires a thesis (in Germany). Prior to the Bologna Process an MD was equal to a PhD - that applies to Drosten. Now it is equal to an MSc. That means Drosten never held a PhD, because he had the (then) equally ranking degree of an MD. If one looks at full professors from medical facilities of Austrian and German Universities, many of the older guys do have "only" an MD. In pre-Bologna times, they where not required to do a PhD due to equality of degrees. However, this is what the University of Frankfurt has to say with regard to his degree: https://aktuelles.uni-frankfurt.de/ak... Relevant quote: "Es bestehen – auch nach mehrfacher Überprüfung – keine Zweifel daran, dass das Promotionsverfahren des Herrn Prof. Dr. Drosten ordnungsgemäß durchgeführt wurde." Translation: After several reviews there are no doubts that the promotion of Prof. Dr. Drosten was carried out according to the regulations of the university. If the Germans do *several* reviews, one can be sure it is correct. Their reputation for punctuality and exactness is well earned for a reason. And: Quote: "Der Ablauf des Promotionsverfahren von Prof. Dr. Drosten ist durch eine im Archiv lagernde Promotionsakte vollständig dokumentiert." Translation: The promotion of Prof. Dr. Drosten is fully documented by files of the university archive. As a German native speaker (Austrian) I can confirm that the wording is a very strong refutation to the claim of a "fake" degree. In other words, Gunnels failed to apply due diligence in his research by failing to (a) consulting the only relevant source, namely the University of Frankfurt and (b) investigating the European academic system.
Last edited:
Heliobas Disciple
TB Fanatic
Posting this for Profit of Doom:

 www.anhinternational.org
(fair use applies)
www.anhinternational.org
(fair use applies)
Breaking News: Unvaxxed ‘Control group’: first release of survey data
Date: 9 June 2022
Find out how over 300,000 health-aware unvaxxed people from around the world have fared with COVID-19, choices & discrimination
**UPDATE** - ResearchGate removed the study preprint on Friday 17th June without warning. To read the survey analysis please click here.
There have been very few studies looking at how those who've elected to rely on natural immunity and natural products, as compared with those who've consented to covid-19 genetic vaccines, the latter who may, or may not have, also tried to optimise their immune systems, fare when it comes to COVID-19. The few that have been done often mix vaccinated with unvaccinated, as shown in the case of UK data by Prof Norman Fenton and his group at Queen Mary, University of London.
That changes with the first release of the analysis of survey data from the international 'Control Group' project - also known as the Vax Control Group.
The citizen-led project was initiated by an Eastbourne (UK) cooperative, the Control Group Cooperative - and it's had over 300,000 subscribers.
Rob Verkerk PhD of ANH has led a team including Dr Naseeba Kathrada (GP, South Africa, Caring Healthcare Workers Coalition), Christof Plothe DO (Integrative & osteopathic practitioner, Germany) and Dr Kat Lindley (Family Physician, USA) that has collated, analysed and interpreted the first 5months of survey data from 'control group' participants.
The survey data offer important revelations, including:
>>> Read our press release below or download here
>>> Download and read preprint report on survey findings on ResearchGate
>>> View below the introductory video from Rob Verkerk - or download here.
PLEASE SHARE WIDELY!
PRESS RELEASE
For immediate release
June 9, 2022
No jab, lower hospitalisations – finds international survey
An international survey of a health-aware, ‘Control Group’ that includes over 300,000 people who have chosen to avoid COVID-19 vaccination, shows participants place minimal burden on health systems through their strong reliance on natural immunity, self-care and the use of natural health supplements to help prevent or even treat COVID-19. Yet this group faces unfounded discrimination, job losses and mental health issues intensified by its marginalisation by mainstream society.
The survey of participants in the ‘Control Group’ includes a sub-group from the over 305,000 participants from more than 175 countries who have joined the citizen-led project and opted to not receive COVID-19 vaccines. The findings just uploaded to the preprint server ResearchGate, show that during the 5-month survey period (September 2021 through to February 2022 inclusive), participants suffered low rates of severe COVID-19 disease, were infrequently hospitalised, and used natural health products extensively both for prevention and for treatment of mild to moderate COVID-19.
Data from these first five months of the Control Group survey were analysed and interpreted by an independent, international team led by Robert Verkerk PhD, a multi-disciplinary scientist and the founder, executive and scientific director of the non-profit Alliance for Natural Health International. Co-authors included three practicing clinicians, Dr Naseeba Kathrada from South Africa, Christof Plothe DO from Germany and Dr Katarina Lindley from the USA. The authors came together to assess the survey data through their collaboration in recent months with the World Council for Health, a non-profit, global coalition of health-focused organizations and civil society groups.
The survey findings were based on a sub-cohort of approximately 18,500 Control Group participants who had completed questionnaires on a monthly basis over the first five months of the survey. Among the wide-ranging data collected, the survey captured reasons why participants avoided vaccines, with distrust of governments and pharmaceutical companies as well as concerns over adverse reactions from insufficiently tested vaccines being high on the list.
Participants reported extensive mental health problems that may have been compounded by the stigmatisation and discrimination facing those who shunned COVID-19 vaccines. It also found that women, despite being unvaccinated for COVID-19, suffered menstrual and bleeding abnormalities that may have been associated with viral exposure, shedding, spike protein exposure or pandemic-related behavioural changes. Those who never wore masks reported the lowest levels of COVID-19 disease.
Given the participants are self-selected and have self-reported, the survey findings need to be interpreted with care when comparing them with national statistics or studies based on randomly selected populations.
The UK-based Control Group project was established in mid-2021 as a citizen-led cooperative that aims to evaluate long-term health outcomes among the COVID-19 vaccine-free as well as linking its members to country support networks and online community groups.
The full survey report can be downloaded from ResearchGate here.
ENDS.
CONTACT
For further information about the survey and findings, contact Rob Verkerk PhD using one of the following methods:
Telephone: +44 (0)1484 646 600
Email: science@anhinternational.org
NOTES TO EDITOR
Download the survey report on ResearchGate via the following link:
Cite report as follows:
Verkerk R, Kathrada N, Plothe C, Lindley K. Self-reported outcomes, choices and discrimination among a global COVID-19 unvaccinated cohort. ResearchGate. Preprint uploaded June 8, 2022. DOI: 10.13140/RG.2.2.28855.19369.
Breaking News: Unvaxxed ‘Control group’: first release of survey data
Find out how over 300,000 health-aware unvaxxed people from around the world have fared with COVID-19, choices & discrimination
www.anhinternational.org
Breaking News: Unvaxxed ‘Control group’: first release of survey data
Date: 9 June 2022
Find out how over 300,000 health-aware unvaxxed people from around the world have fared with COVID-19, choices & discrimination
**UPDATE** - ResearchGate removed the study preprint on Friday 17th June without warning. To read the survey analysis please click here.
There have been very few studies looking at how those who've elected to rely on natural immunity and natural products, as compared with those who've consented to covid-19 genetic vaccines, the latter who may, or may not have, also tried to optimise their immune systems, fare when it comes to COVID-19. The few that have been done often mix vaccinated with unvaccinated, as shown in the case of UK data by Prof Norman Fenton and his group at Queen Mary, University of London.
That changes with the first release of the analysis of survey data from the international 'Control Group' project - also known as the Vax Control Group.
The citizen-led project was initiated by an Eastbourne (UK) cooperative, the Control Group Cooperative - and it's had over 300,000 subscribers.
Rob Verkerk PhD of ANH has led a team including Dr Naseeba Kathrada (GP, South Africa, Caring Healthcare Workers Coalition), Christof Plothe DO (Integrative & osteopathic practitioner, Germany) and Dr Kat Lindley (Family Physician, USA) that has collated, analysed and interpreted the first 5months of survey data from 'control group' participants.
The survey data offer important revelations, including:
- Primary reasons given for avoiding vaccines included preference for natural medicine interventions, distrust of pharmaceutical interventions, distrust of government information, poor/limited trial study data and fear of long-term adverse reactions
- The unvaccinated 'control group' participants don't place a disproportionate burden on health systems - in fact quite the opposite, they have experienced very low hospitalisation rates and severe covid-19 disease is rare
- They are more likely to self-care, using natural products like vitamin D, vitamin C, zinc and quercetin
- Many have used ivermectin and hydroxychloriquine
- Women have suffered menstrual and bleeding abnormalities despite being unvaccinated, possibly owing to spike protein exposure and shedding
- Their mental health burden has been considerable, possibly aggravated by their stigmatisation by mainstream, 'vaccinated' society
- They have been heavily discriminated against because of their decision to exercise their right to informed consent and refuse the administration of 'genetic vaccines'
>>> Read our press release below or download here
>>> Download and read preprint report on survey findings on ResearchGate
>>> View below the introductory video from Rob Verkerk - or download here.
PLEASE SHARE WIDELY!
PRESS RELEASE
For immediate release
June 9, 2022
No jab, lower hospitalisations – finds international survey
An international survey of a health-aware, ‘Control Group’ that includes over 300,000 people who have chosen to avoid COVID-19 vaccination, shows participants place minimal burden on health systems through their strong reliance on natural immunity, self-care and the use of natural health supplements to help prevent or even treat COVID-19. Yet this group faces unfounded discrimination, job losses and mental health issues intensified by its marginalisation by mainstream society.
The survey of participants in the ‘Control Group’ includes a sub-group from the over 305,000 participants from more than 175 countries who have joined the citizen-led project and opted to not receive COVID-19 vaccines. The findings just uploaded to the preprint server ResearchGate, show that during the 5-month survey period (September 2021 through to February 2022 inclusive), participants suffered low rates of severe COVID-19 disease, were infrequently hospitalised, and used natural health products extensively both for prevention and for treatment of mild to moderate COVID-19.
Data from these first five months of the Control Group survey were analysed and interpreted by an independent, international team led by Robert Verkerk PhD, a multi-disciplinary scientist and the founder, executive and scientific director of the non-profit Alliance for Natural Health International. Co-authors included three practicing clinicians, Dr Naseeba Kathrada from South Africa, Christof Plothe DO from Germany and Dr Katarina Lindley from the USA. The authors came together to assess the survey data through their collaboration in recent months with the World Council for Health, a non-profit, global coalition of health-focused organizations and civil society groups.
The survey findings were based on a sub-cohort of approximately 18,500 Control Group participants who had completed questionnaires on a monthly basis over the first five months of the survey. Among the wide-ranging data collected, the survey captured reasons why participants avoided vaccines, with distrust of governments and pharmaceutical companies as well as concerns over adverse reactions from insufficiently tested vaccines being high on the list.
Participants reported extensive mental health problems that may have been compounded by the stigmatisation and discrimination facing those who shunned COVID-19 vaccines. It also found that women, despite being unvaccinated for COVID-19, suffered menstrual and bleeding abnormalities that may have been associated with viral exposure, shedding, spike protein exposure or pandemic-related behavioural changes. Those who never wore masks reported the lowest levels of COVID-19 disease.
Given the participants are self-selected and have self-reported, the survey findings need to be interpreted with care when comparing them with national statistics or studies based on randomly selected populations.
The UK-based Control Group project was established in mid-2021 as a citizen-led cooperative that aims to evaluate long-term health outcomes among the COVID-19 vaccine-free as well as linking its members to country support networks and online community groups.
The full survey report can be downloaded from ResearchGate here.
ENDS.
CONTACT
For further information about the survey and findings, contact Rob Verkerk PhD using one of the following methods:
Telephone: +44 (0)1484 646 600
Email: science@anhinternational.org
NOTES TO EDITOR
Download the survey report on ResearchGate via the following link:
Cite report as follows:
Verkerk R, Kathrada N, Plothe C, Lindley K. Self-reported outcomes, choices and discrimination among a global COVID-19 unvaccinated cohort. ResearchGate. Preprint uploaded June 8, 2022. DOI: 10.13140/RG.2.2.28855.19369.
Heliobas Disciple
TB Fanatic
Part 2 of above post:
 www.anhinternational.org
(fair use applies)
www.anhinternational.org
(fair use applies)
BREAKING NEWS: Censors remove control group report from preprint server
Date: 17 June 2022
ResearchGate censors spring into action when reads spike after news of report is heard outside the echo chamber of the unvaccinated. Help overcome scientific censorship
Content Sections
By Rob Verkerk PhD, founder, scientific & executive director, ANH-Intl
Last week we announced we’d analysed a sample of the survey data from over 300,000 people in 175 countries who had elected to not receive covid-19 vaccines as part of an initiative of the Control Group Cooperative.
We uploaded the 41-page, entirely transparent report to the preprint site ResearchGate. The report included 21 pages of survey findings, a description of the Methods used, annexes that included all the questions that were presented to cooperative members, an introduction and a discussion, the latter including an outline of five limitations of the survey. The report made clear that the survey design and data collection was conducted entirely independently of the analysis and reporting, which was also entirely unpaid. Together that amounts to saying the work was both independent and transparent, something we’ve seen far too little of in vaccine research.
Today at around midday UK time, I received a letter from ResearchGate letting me know the survey report had been removed from its website. It seems there is a different course of action when science that does not support the mainstream narrative is heard outside the echo chamber of those who’ve exercised their right to refuse covid-19 ‘vaccines’. Yet another reminder of how censorship works in the post-covid world when research findings challenge the narrative.
>>> Download a PDF of the preprint article ResearchGate censored
Why did ResearchGate pull the preprint?
ResearchGate said that the article breached its Terms and Conditions.
Its message was sent by an individual identified as “Sam” and the key sentiments are shown in the following extract:
An extract of my response is as follows:
No doubt, the fact that the ResearchGate article was getting considerable airplay in a wide range of media, including the UK’s Daily Mail and MSN (the latter had already pulled its article) was among the reasons for the article being pulled.
Children’s Health Defense, Technocracy News and many other new media actors also covered the release of the findings.
Another likely factor triggering censorship was that ResearchGate would have become aware of a large spike in views. I had around 4,500 reads of my work on ResearchGate when I uploaded the preprint a week ago. Yesterday, I was recognised by ResearchGate for my “nice work” when they sent me an email letting me know I’d achieved 20,000 reads (see below).
>>> Download a PDF of the preprint article ResearchGate censored
What were the summary findings?
So what are they not wanting you to know?
The report includes data summaries from self-reported data independently collected between September 2021 and February 2022 inclusive from an international, self-selected, COVID-19 unvaccinated population via a UK-based cooperative, namely the Control Group Cooperative. The summaries were derived from a cohort of 18,497 participants who provided data each consecutive month, the largest proportions coming from Europe, North America and Australasia.
The findings do however suggest the urgent need for prospective observational studies, including unvaccinated, partially vaccinated and fully vaccinated, subjects, investigating long-term outcomes, behaviours, choices, and attitudinal or discriminatory responses to vaccination status.
What were the limitations of the survey?
These are detailed in the Discussion, as follows:
PLEASE CIRCULATE WIDELY TO HELP OVERCOME SCIENTIFIC CENSORSHIP!
BREAKING NEWS: Censors remove control group report from preprint server
ResearchGate censors spring into action when reads spike after news of report is heard outside the echo chamber of the unvaccinated. Help overcome scientific censorship
www.anhinternational.org
BREAKING NEWS: Censors remove control group report from preprint server
Date: 17 June 2022
ResearchGate censors spring into action when reads spike after news of report is heard outside the echo chamber of the unvaccinated. Help overcome scientific censorship
Content Sections
By Rob Verkerk PhD, founder, scientific & executive director, ANH-Intl
Last week we announced we’d analysed a sample of the survey data from over 300,000 people in 175 countries who had elected to not receive covid-19 vaccines as part of an initiative of the Control Group Cooperative.
We uploaded the 41-page, entirely transparent report to the preprint site ResearchGate. The report included 21 pages of survey findings, a description of the Methods used, annexes that included all the questions that were presented to cooperative members, an introduction and a discussion, the latter including an outline of five limitations of the survey. The report made clear that the survey design and data collection was conducted entirely independently of the analysis and reporting, which was also entirely unpaid. Together that amounts to saying the work was both independent and transparent, something we’ve seen far too little of in vaccine research.
Today at around midday UK time, I received a letter from ResearchGate letting me know the survey report had been removed from its website. It seems there is a different course of action when science that does not support the mainstream narrative is heard outside the echo chamber of those who’ve exercised their right to refuse covid-19 ‘vaccines’. Yet another reminder of how censorship works in the post-covid world when research findings challenge the narrative.
>>> Download a PDF of the preprint article ResearchGate censored
Why did ResearchGate pull the preprint?
ResearchGate said that the article breached its Terms and Conditions.
Its message was sent by an individual identified as “Sam” and the key sentiments are shown in the following extract:
“In connection with using or accessing the Service, you shall not … Act unprofessionally or inappropriately, including by posting broad, vague, irrelevant, untargeted, off-topic, or non-scientific content, potentially harmful or potentially dangerous content, or by misusing the Service and its features
As stated in our Terms of Service, ResearchGate reserves the right to remove any content posted by you when we deem it to be necessary or appropriate, including if we determine that the content may expose us to harm, potential legal liability, or is in breach of our Terms.”
An extract of my response is as follows:
“Thank you for your email, Sam.
We had looked at your Terms & Conditions and hadn't considered that the survey findings were in breach of them. We are clearly disappointed in your decision. We were very clear in our report that the survey findings were self-selected and self-reported, we outlined 5 limitations in our Discussion, and the work was both transparent and independent of the Control Group Cooperative that designed the survey and collected the data.
However, I do understand that you must have been under considerable pressure to remove the report once the findings were discussed by the mainstream media.
It's yet another sad day for efforts to prevent open scientific discourse.
I have long respected the contribution ResearchGate makes to open and transparent discourse within the scientific community and I hope this doesn't represent part of a general narrowing of your approach to openness in science. We have been invited to submit the findings to a peer reviewed journal in a more consolidated form so will continue on this path.”
No doubt, the fact that the ResearchGate article was getting considerable airplay in a wide range of media, including the UK’s Daily Mail and MSN (the latter had already pulled its article) was among the reasons for the article being pulled.
Children’s Health Defense, Technocracy News and many other new media actors also covered the release of the findings.
Another likely factor triggering censorship was that ResearchGate would have become aware of a large spike in views. I had around 4,500 reads of my work on ResearchGate when I uploaded the preprint a week ago. Yesterday, I was recognised by ResearchGate for my “nice work” when they sent me an email letting me know I’d achieved 20,000 reads (see below).
>>> Download a PDF of the preprint article ResearchGate censored
What were the summary findings?
So what are they not wanting you to know?
The report includes data summaries from self-reported data independently collected between September 2021 and February 2022 inclusive from an international, self-selected, COVID-19 unvaccinated population via a UK-based cooperative, namely the Control Group Cooperative. The summaries were derived from a cohort of 18,497 participants who provided data each consecutive month, the largest proportions coming from Europe, North America and Australasia.
- The cohort was 60% female with an age-structure skewed towards the 40-69y age band.
- Primary reasons given for avoiding COVID-19 vaccines were reported as preference for natural medicine interventions, distrust of pharmaceutical interventions, distrust of government information, poor/limited trial study data and fear of long-term adverse reactions.
- Respondents between the ages of 20-49y reported the greatest incidence of COVID-19 disease (10-12%), peaking in January 2022. Those >70y reported the lowest incidence (4.0% females, 3.7% males).
- Just 0.4% of the cohort reported hospitalisation (as in- or out-patients).
- Some 64% of the cohort reported taking vitamin D, vitamin C, zinc or quercetin, or any combination, routinely for prevention, with 71% self-administering vitamin D, C and zinc for treatment of COVID-19 disease, although self-administration reduced dramatically among those hospitalised.
- Fatigue, cough, muscle/body aches and fever were the four most common COVID-19 symptoms reported, the 50 to 69y age band reporting the most symptomatic disease.
- Approximately 40% of the cohort reported mild to moderate mental health issues. Menstrual abnormalities in the form of irregular periods were reported by 36% of women in the 20-49y age band.
- Reported job losses were greatest in Australia and New Zealand at 29% of participants, followed by 13% in North America. Between 20% and 50% of respondents, depending on region, reported being personal targets of hate owing to their COVID-19 vaccination status.
- Between 57% and 61% of respondents in Southern Europe and Western Europe, Australia/New Zealand and South America, reported being targets of state/country victimisation.
The findings do however suggest the urgent need for prospective observational studies, including unvaccinated, partially vaccinated and fully vaccinated, subjects, investigating long-term outcomes, behaviours, choices, and attitudinal or discriminatory responses to vaccination status.
What were the limitations of the survey?
These are detailed in the Discussion, as follows:
- the respondents are self-selected and therefore not randomly selected;
- the data are self-reported and therefore have not been verified independently;
- the ~18,500 participant cohort may have been biased towards the most diligent, health-conscious participants given they all completed monthly surveys (although a number of cross-checks with the main ~300,000 cohort suggests this bias is likely low)
- there is no available comparative ‘control’ population that includes individuals who have consented to one or more COVID-19 vaccines of different types; and;
- the questionnaire design is limited and does not account for multiple variables that affect health status, such as socioeconomic status, urban, peri-urban or rural residence, diet, or lifestyle.
PLEASE CIRCULATE WIDELY TO HELP OVERCOME SCIENTIFIC CENSORSHIP!
Heliobas Disciple
TB Fanatic
America is now the only country in the world that authorizes COVID shots for infants
Jordan Schachtel
3 minutes
It appears that the United States just became the only country in the world to “vaccinate” babies and toddlers with COVID injections.
Share
Despite what you are reading in the press, the U.S. seems to be, as of Friday, the only country in the world to partake in experimental COVID therapeutics for infants.
On Friday, the FDA authorized mRNA COVID shots (both Pfizer and Moderna) under emergency use authorization for children under 5 years old, all the way down to 6 months of age. As you’ll see in a moment, this is unprecedented anywhere in the world.
The approval made its way through the halls of the federal bureaucracy, regardless of any studies showing a positive benefit for injecting young children with mRNA shots, which, even in adults, do not effectively prevent coronavirus infection.
Making matters worse, our deceitful corporate press is actively engaged in a cover up operation to make it seem like the new policy is not particularly unique, when in fact, it is exclusively unique.
Many corporate press reports, in hailing the announcement, churned out stenography today that made a quick mention of the fact that “a dozen countries, including China, already vaccinate kids under 5.”
But when you break down the data further, a true scandal arises.
As of a couple weeks ago there were only 7 countries where kids under 5 were given COVID injections, though the WHO now claims that number is 12.
The seven countries on record are:
-Argentina
-Bahrain
-Chile
-China
-Cuba
-UAE
-Venezuela
(the territory of Hong Kong, which uses the Chinese-made shots, is sometimes listed as the eighth country on record)
But that’s only the beginning of the madness.
Venezuela and Cuba are the only countries that allow for COVID shots between the ages of two and three. The rest of the countries only go as young as three.
Moreover, none of the nations are using mRNA. 5 out of 7 are using Chinese manufactured inactivated vaccines. Cuba and Venezuela are using the Cuban homebrew shot.
And NONE of these countries are allowing for COVID shots between the ages of 6 months to two years, which means that the United States has become the only country in the world to allow for experimental COVID injections shots for babies and 2 year old toddlers.

America is now the only country in the world that authorizes COVID shots for infants
Not what the corporate press told you.dossier.substack.com
I posted this early this morning but it's so important it's worth repeating (and it's a page up so can't hurt to dupe it)
And btw, I should've posted this when I posted the substack - Taiwan joined the club. They are now also going to be boosting their babies as well.
 (see next post)
(see next post)HD
Last edited:
Heliobas Disciple
TB Fanatic
Here's the news on Taiwan:

 focustaiwan.tw
(fair use applies)
focustaiwan.tw
(fair use applies)
CORONAVIRUS/Taiwan grants EUA to Moderna COVID-19 vaccine for children under 6
06/17/2022 11:15 PM
Taipei, June 17 (CNA) An emergency use authorization (EUA) has been granted to Moderna's COVID-19 vaccine for children aged between 6 months and 5 years, Taiwan's Food and Drug Administration (FDA) said in a statement released on Friday.
An expert panel was convened on Friday to review the EUA request submitted by the American biotechnology company for its COVID-19 vaccine for young children, considering the ongoing outbreak and the growing number of young children who have developed severe infections, according to the FDA.
The Moderna vaccine will be administered in two 0.25 milliliter doses, each containing 25 micrograms of mRNA, with a minimum interval of 28 days, the FDA said.
In comparison, each dose given to people aged 12 and above contains 100 micrograms of mRNA, and 50 micrograms for children aged 6-11.
According to Moderna, its interim results from the Phase 2/3 study for the age group of 6 months to 5 years showed a robust neutralizing antibody response consistent with that of young adults, even at the lower 25-microgram dose.
The Moderna vaccine was first rolled out to people who were 18 and above in Taiwan in June 2021, high school students two month later, and to children aged 6-11 in May this year.
The schedule for the rollout of the Mooderna vaccine will be decided by the Advisory Committee on Immunization Practices convened by the Centers for Disease Control (CDC), the FDA said.
More doses of the Moderna vaccine have been administered in Taiwan than the government has officially received because recipients of the Moderna booster shot are given half the standard dose of the first and second jab.
On Friday, Taiwan reported 55,261 new COVID-19 infections -- 55,187 locally transmitted and 74 contracted abroad, bringing the total domestic cases for this year to 3,162,445.
While 4,739, or 0.15 percent, of this year's domestic cases have been classified as severe infections, 52 of these cases involve children aged 9 and below, according to CDC data.
Among these patients with severe infections, 4,015 have passed away, including 15 children who were 9 years or younger, CDC data showed.
(By Chang Ming-hsuan and Kay Liu)
 focustaiwan.tw
(fair use applies)
focustaiwan.tw
(fair use applies)
CORONAVIRUS/Taiwan to roll out Moderna COVID-19 vaccine for children under 6 in July
06/18/2022 05:37 PM
Taipei, June 18 (CNA) The Moderna COVID-19 vaccine will become available next month for children in Taiwan aged 6 months to 5 years, the Central Epidemic Command Center (CECC) said Saturday.
A shipment of the Moderna COVID-19 vaccine for children is scheduled to arrive to Taiwan in July, and the rollout is expected to start in the third week of the month, Lo Yi-chun (羅一鈞), deputy head of the CECC's medical response division, said at a daily COVID-19 press briefing.
Discussions are still ongoing with the American drugmaker on the exact date of the vaccine shipment and the number of doses, he said.
Meanwhile, Taiwan's Centers for Disease Control (CDC) is still waiting for the technical information from the makers of the Pfizer-BioNTech (BNT) vaccine concerning its use for children under the age of 5 years, Lo said.
Taiwan began offering the Moderna COVID-19 vaccine to children aged 6-11 on May 2 and started the rollout of the Pfizer-BioNTech (BNT) COVID-19 vaccine for children aged 5-11 on May 25.
More doses of the Moderna vaccine have been administered in Taiwan than the government has officially received because recipients of the Moderna booster shot are given half the standard dose of the first and second jab.
On Friday, Taiwan further granted emergency use authorization (EUA) to the Moderna vaccine for children aged 6 months to 5 years.
Regarding COVID-19 vaccine supplies for the wider population, Lo said Taiwan is likely to receive a shipment of Novavax, via the global vaccine sharing initiative COVAX, in July.
Taiwan has ordered more than 2 million doses of Novavax vaccine through COVAX and granted EUA for that brand on Friday.
To date, 91.15 percent of Taiwan's population has received at least one dose of a COVID-19 vaccine, while 82.6 percent has gotten at least two doses and 69.24 percent has received a booster shot, according to the latest CECC statistics.
(By Chang Ming-hsuan and Ko Lin)
Taiwan grants EUA to Moderna COVID-19 vaccine for children under 6 - Focus Taiwan
Taipei, June 17 (CNA) An emergency use authorization (EUA) has been granted to Moderna's COVID-19 vaccine for children aged between 6 months and 5 years, Taiwan's Food and Drug Administration (FDA) said in a statement released on Friday.
focustaiwan.tw
CORONAVIRUS/Taiwan grants EUA to Moderna COVID-19 vaccine for children under 6
06/17/2022 11:15 PM
Taipei, June 17 (CNA) An emergency use authorization (EUA) has been granted to Moderna's COVID-19 vaccine for children aged between 6 months and 5 years, Taiwan's Food and Drug Administration (FDA) said in a statement released on Friday.
An expert panel was convened on Friday to review the EUA request submitted by the American biotechnology company for its COVID-19 vaccine for young children, considering the ongoing outbreak and the growing number of young children who have developed severe infections, according to the FDA.
The Moderna vaccine will be administered in two 0.25 milliliter doses, each containing 25 micrograms of mRNA, with a minimum interval of 28 days, the FDA said.
In comparison, each dose given to people aged 12 and above contains 100 micrograms of mRNA, and 50 micrograms for children aged 6-11.
According to Moderna, its interim results from the Phase 2/3 study for the age group of 6 months to 5 years showed a robust neutralizing antibody response consistent with that of young adults, even at the lower 25-microgram dose.
The Moderna vaccine was first rolled out to people who were 18 and above in Taiwan in June 2021, high school students two month later, and to children aged 6-11 in May this year.
The schedule for the rollout of the Mooderna vaccine will be decided by the Advisory Committee on Immunization Practices convened by the Centers for Disease Control (CDC), the FDA said.
More doses of the Moderna vaccine have been administered in Taiwan than the government has officially received because recipients of the Moderna booster shot are given half the standard dose of the first and second jab.
On Friday, Taiwan reported 55,261 new COVID-19 infections -- 55,187 locally transmitted and 74 contracted abroad, bringing the total domestic cases for this year to 3,162,445.
While 4,739, or 0.15 percent, of this year's domestic cases have been classified as severe infections, 52 of these cases involve children aged 9 and below, according to CDC data.
Among these patients with severe infections, 4,015 have passed away, including 15 children who were 9 years or younger, CDC data showed.
(By Chang Ming-hsuan and Kay Liu)
Taiwan to roll out Moderna COVID-19 vaccine for children under 6 in July - Focus Taiwan
Taipei, June 18 (CNA) The Moderna COVID-19 vaccine will become available next month for children in Taiwan aged 6 months to 5 years, the Central Epidemic Command Center (CECC) said Saturday.
focustaiwan.tw
CORONAVIRUS/Taiwan to roll out Moderna COVID-19 vaccine for children under 6 in July
06/18/2022 05:37 PM
Taipei, June 18 (CNA) The Moderna COVID-19 vaccine will become available next month for children in Taiwan aged 6 months to 5 years, the Central Epidemic Command Center (CECC) said Saturday.
A shipment of the Moderna COVID-19 vaccine for children is scheduled to arrive to Taiwan in July, and the rollout is expected to start in the third week of the month, Lo Yi-chun (羅一鈞), deputy head of the CECC's medical response division, said at a daily COVID-19 press briefing.
Discussions are still ongoing with the American drugmaker on the exact date of the vaccine shipment and the number of doses, he said.
Meanwhile, Taiwan's Centers for Disease Control (CDC) is still waiting for the technical information from the makers of the Pfizer-BioNTech (BNT) vaccine concerning its use for children under the age of 5 years, Lo said.
Taiwan began offering the Moderna COVID-19 vaccine to children aged 6-11 on May 2 and started the rollout of the Pfizer-BioNTech (BNT) COVID-19 vaccine for children aged 5-11 on May 25.
More doses of the Moderna vaccine have been administered in Taiwan than the government has officially received because recipients of the Moderna booster shot are given half the standard dose of the first and second jab.
On Friday, Taiwan further granted emergency use authorization (EUA) to the Moderna vaccine for children aged 6 months to 5 years.
Regarding COVID-19 vaccine supplies for the wider population, Lo said Taiwan is likely to receive a shipment of Novavax, via the global vaccine sharing initiative COVAX, in July.
Taiwan has ordered more than 2 million doses of Novavax vaccine through COVAX and granted EUA for that brand on Friday.
To date, 91.15 percent of Taiwan's population has received at least one dose of a COVID-19 vaccine, while 82.6 percent has gotten at least two doses and 69.24 percent has received a booster shot, according to the latest CECC statistics.
(By Chang Ming-hsuan and Ko Lin)
Heliobas Disciple
TB Fanatic
This is serendipitous. I found this article in my 'save to post later 'bookmark folder that I use if I find covid articles during the day and don't have time to come on and post them, and since it was still in there I am assuming I never got around to posting it (or I did and I am duping myself). I don't always check there, unless I remember I saved something and want to retrieve it. (the next article I'm about to post is why I went looking). I started to post it and I realized it's about the articles I just posted on behalf of Profit of Doom a few posts up. cue the Twilight Zone theme.....

 www.theepochtimes.com
(fair use applies)
www.theepochtimes.com
(fair use applies)
Severe COVID ‘Rare’ in People Who Didn’t Get Vaccine, Survey Reveals
BY Alliance for Natural Health International
June 12, 2022
A survey of 300,000 people who didn’t get the COVID-19 vaccine revealed the unvaccinated didn’t place a disproportionate burden on health systems — in fact, they experienced very low rates of hospitalization and severe COVID-19.

There have been very few studies looking at how those who’ve elected to rely on natural immunity and natural products, as compared with those who’ve consented to COVID-19 genetic vaccines, the latter who may or may not have, also tried to optimize their immune systems, fare when it comes to COVID-19.
The few that have been done often mix vaccinated with unvaccinated, as shown in the case of U.K. data by professor Norman Fenton and his group at Queen Mary, University of London.
That changes with the first release of the analysis of survey data from the international Control Group project — also known as the Vax Control Group.
The citizen-led project was initiated by an Eastbourne (U.K.) cooperative, the Control Group Cooperative — and it’s had more than 300,000 subscribers.
Rob Verkerk Ph.D. of Alliance for Natural Health has led a team, including Dr. Naseeba Kathrada (general practitioner, South Africa, Caring Healthcare Workers Coalition), Christof Plothe D.O. (integrative and osteopathic practitioner, Germany) and Dr. Kat Lindley (family physician, USA), that has collated, analyzed and interpreted the first five months of survey data from “control group” participants.
The survey data offer important revelations, including:
No Jab, Lower Hospitalizations — Finds International Survey
An international survey of a health-aware, “Control Group” that includes over 300,000 people who have chosen to avoid COVID-19 vaccination, shows participants place minimal burden on health systems through their strong reliance on natural immunity, self-care and the use of natural health supplements to help prevent or even treat COVID-19.
Yet this group faces unfounded discrimination, job losses and mental health issues intensified by its marginalization by mainstream society.
The survey of participants in the “Control Group” includes a sub-group from the over 305,000 participants from more than 175 countries who have joined the citizen-led project and opted to not receive COVID-19 vaccines.
The findings just uploaded to the preprint server ResearchGate, show that during the 5-month survey period (Sept. 2021 through to Feb. 2022 inclusive), participants suffered low rates of severe COVID-19 disease, were infrequently hospitalized, and used natural health products extensively both for prevention and for treatment of mild to moderate COVID-19.
Data from these first five months of the Control Group survey were analyzed and interpreted by an independent, international team led by Robert Verkerk Ph.D., a multi-disciplinary scientist and the founder, executive and scientific director of the non-profit Alliance for Natural Health International.
Co-authors included three practicing clinicians, Dr. Naseeba Kathrada from South Africa, Christof Plothe D.O. from Germany and Dr. Katarina Lindley from the USA.
The authors came together to assess the survey data through their collaboration in recent months with the World Council for Health, a non-profit, global coalition of health-focused organizations and civil society groups.
The survey findings were based on a sub-cohort of approximately 18,500 Control Group participants who had completed questionnaires on a monthly basis over the first five months of the survey.
Among the wide-ranging data collected, the survey captured reasons why participants avoided vaccines, with distrust of governments and pharmaceutical companies as well as concerns over adverse reactions from insufficiently tested vaccines being high on the list.
Participants reported extensive mental health problems that may have been compounded by the stigmatization and discrimination facing those who shunned COVID-19 vaccines.
It also found that women, despite being unvaccinated for COVID-19, suffered menstrual and bleeding abnormalities that may have been associated with viral exposure, shedding, spike protein exposure or pandemic-related behavioral changes. Those who never wore masks reported the lowest levels of COVID-19 disease.
Given the participants are self-selected and have self-reported, the survey findings need to be interpreted with care when comparing them with national statistics or studies based on randomly selected populations.
The U.K.-based Control Group project was established in mid-2021 as a citizen-led cooperative that aims to evaluate long-term health outcomes among the COVID-19 vaccine-free as well as linking its members to country support networks and online community groups.
Originally published by Alliance for Natural Health International.
© 2022 Alliance for Natural Health International. This work is reproduced and distributed with the permission of The Alliance for Natural Health International.
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times.
Severe COVID ‘Rare’ in People Who Didn’t Get Vaccine, Survey Reveals
www.theepochtimes.com
Severe COVID ‘Rare’ in People Who Didn’t Get Vaccine, Survey Reveals
BY Alliance for Natural Health International
June 12, 2022
A survey of 300,000 people who didn’t get the COVID-19 vaccine revealed the unvaccinated didn’t place a disproportionate burden on health systems — in fact, they experienced very low rates of hospitalization and severe COVID-19.
There have been very few studies looking at how those who’ve elected to rely on natural immunity and natural products, as compared with those who’ve consented to COVID-19 genetic vaccines, the latter who may or may not have, also tried to optimize their immune systems, fare when it comes to COVID-19.
The few that have been done often mix vaccinated with unvaccinated, as shown in the case of U.K. data by professor Norman Fenton and his group at Queen Mary, University of London.
That changes with the first release of the analysis of survey data from the international Control Group project — also known as the Vax Control Group.
The citizen-led project was initiated by an Eastbourne (U.K.) cooperative, the Control Group Cooperative — and it’s had more than 300,000 subscribers.
Rob Verkerk Ph.D. of Alliance for Natural Health has led a team, including Dr. Naseeba Kathrada (general practitioner, South Africa, Caring Healthcare Workers Coalition), Christof Plothe D.O. (integrative and osteopathic practitioner, Germany) and Dr. Kat Lindley (family physician, USA), that has collated, analyzed and interpreted the first five months of survey data from “control group” participants.
The survey data offer important revelations, including:
- The unvaccinated “control group” participants don’t place a disproportionate burden on health systems — in fact, quite the opposite, they have experienced very low hospitalization rates and severe COVID-19 disease is rare.
- They are more likely to self-care, using natural products like vitamin D, vitamin C, zinc and quercetin.
- Many have used ivermectin and hydroxychloroquine.
- Women have suffered menstrual and bleeding abnormalities despite being unvaccinated, possibly owing to spike protein exposure and shedding.
- Their mental health burden has been considerable, possibly aggravated by their stigmatization by the mainstream, “vaccinated” society.
- They have been heavily discriminated against because of their decision to exercise their right to informed consent and refuse the administration of “genetic vaccines.”
No Jab, Lower Hospitalizations — Finds International Survey
An international survey of a health-aware, “Control Group” that includes over 300,000 people who have chosen to avoid COVID-19 vaccination, shows participants place minimal burden on health systems through their strong reliance on natural immunity, self-care and the use of natural health supplements to help prevent or even treat COVID-19.
Yet this group faces unfounded discrimination, job losses and mental health issues intensified by its marginalization by mainstream society.
The survey of participants in the “Control Group” includes a sub-group from the over 305,000 participants from more than 175 countries who have joined the citizen-led project and opted to not receive COVID-19 vaccines.
The findings just uploaded to the preprint server ResearchGate, show that during the 5-month survey period (Sept. 2021 through to Feb. 2022 inclusive), participants suffered low rates of severe COVID-19 disease, were infrequently hospitalized, and used natural health products extensively both for prevention and for treatment of mild to moderate COVID-19.
Data from these first five months of the Control Group survey were analyzed and interpreted by an independent, international team led by Robert Verkerk Ph.D., a multi-disciplinary scientist and the founder, executive and scientific director of the non-profit Alliance for Natural Health International.
Co-authors included three practicing clinicians, Dr. Naseeba Kathrada from South Africa, Christof Plothe D.O. from Germany and Dr. Katarina Lindley from the USA.
The authors came together to assess the survey data through their collaboration in recent months with the World Council for Health, a non-profit, global coalition of health-focused organizations and civil society groups.
The survey findings were based on a sub-cohort of approximately 18,500 Control Group participants who had completed questionnaires on a monthly basis over the first five months of the survey.
Among the wide-ranging data collected, the survey captured reasons why participants avoided vaccines, with distrust of governments and pharmaceutical companies as well as concerns over adverse reactions from insufficiently tested vaccines being high on the list.
Participants reported extensive mental health problems that may have been compounded by the stigmatization and discrimination facing those who shunned COVID-19 vaccines.
It also found that women, despite being unvaccinated for COVID-19, suffered menstrual and bleeding abnormalities that may have been associated with viral exposure, shedding, spike protein exposure or pandemic-related behavioral changes. Those who never wore masks reported the lowest levels of COVID-19 disease.
Given the participants are self-selected and have self-reported, the survey findings need to be interpreted with care when comparing them with national statistics or studies based on randomly selected populations.
The U.K.-based Control Group project was established in mid-2021 as a citizen-led cooperative that aims to evaluate long-term health outcomes among the COVID-19 vaccine-free as well as linking its members to country support networks and online community groups.
Originally published by Alliance for Natural Health International.
© 2022 Alliance for Natural Health International. This work is reproduced and distributed with the permission of The Alliance for Natural Health International.
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times.
Heliobas Disciple
TB Fanatic
This is the article I saw earlier today.

 www.dailymail.co.uk
(fair use applies)
www.dailymail.co.uk
(fair use applies)
WHO chief 'believes Covid DID leak from Wuhan lab' after a 'catastrophic accident' in 2019 despite publicly maintaining 'all hypotheses remain on the table'
By Glen Owen Political Editor For The Mail On Sunday
Published: 17:01 EDT, 18 June 2022 | Updated: 18:20 EDT, 18 June 2022
While publicly the group maintains that ‘all hypotheses remain on the table’ about the origins of Covid, the source said Tedros Adhanom Ghebreyesus, director-general of the World Health Organisation (WHO), had recently confided to a senior European politician that the most likely explanation was a catastrophic accident at a laboratory in Wuhan, where infections first spread during late 2019.
The Mail on Sunday first revealed concerns within Western intelligence services about the Wuhan Institute of Virology, where scientists were manipulating coronaviruses sampled from bats in caves nearly 1,000 miles away – the same caves where Covid-19 is suspected to have originated – in April 2020. The worldwide death toll from the Covid pandemic is now estimated to have hit more than 18 million.
The WHO was initially criticised for its deferential approach to China over the pandemic, as well as a willingness to accept Beijing’s protestations that claims of a laboratory leak were just a ‘conspiracy theory’.
However, in the absence of any compelling evidence of ‘zoonotic’ spread – the process by which a virus leaps from animals to humans – it is now adopting a more neutral public stance.
Dr Tedros updated member states on the pandemic this month, admitting: ‘We do not yet have the answers as to where it came from or how it entered the human population.
‘Understanding the origins of the virus is very important scientifically to prevent future epidemics and pandemics.
‘But morally, we also owe it to all those who have suffered and died and their families. The longer it takes, the harder it becomes. We need to speed up and act with a sense of urgency.
‘All hypotheses must remain on the table until we have evidence that enables us to rule certain hypotheses in or out. This makes it all the more urgent that this scientific work be kept separate from politics. The way to prevent politicisation is for countries to share data and samples with transparency and without interference from any government. The only way this scientific work can progress successfully is with full collaboration from all countries, including China, where the first cases of SARS-CoV-2 were reported.’

The Mail on Sunday first revealed concerns about the region's Institute of Virology in 2020

It was suggested Covid 'could easily have escaped while being analysed' by scientists
Last year, the WHO established the Scientific Advisory Group for the Origins of Novel Pathogens (Sago) to outline which studies would be needed to identify the origins of SARS-CoV-2 – as Covid is scientifically known – and to ‘create a global framework for studying the origins of emerging and re-emerging pathogens’.
An original probe into the outbreak by the WHO was resisted fiercely by China, leading to a report that concluded the SARS-CoV-2 virus probably passed to humans from a bat via another unidentified species.
But after 14 nations including the UK, US and Australia criticised its findings as being heavily compromised, Dr Tedros admitted the report’s flaws and ordered the new process.
The Government has taken a cautious approach to apportioning blame for Covid – something that China-sceptics attribute to a fear of offending Beijing.
However, American intelligence has placed the secretive Wuhan laboratory at the centre of its analysis.
Former US Secretary of State Mike Pompeo claimed that workers at the institute had fallen ill with Covid-like symptoms in autumn 2019 – weeks before the alarm was raised, and said that as part of military projects its scientists were experimenting with a bat coronavirus very similar to the one that causes Covid.
A WHO spokesman said: ‘Dr Tedros has been consistently saying all hypotheses remain on the table as scientists pursue their work.’
WHO chief 'believes Covid DID leak from Wuhan lab' after 'accident'
The head of the WHO believes Covid spread after a leak from a Wuhan lab, a senior Government source claims. Tedros Adhanom publicly maintains that 'all hypotheses remain'
WHO chief 'believes Covid DID leak from Wuhan lab' after a 'catastrophic accident' in 2019 despite publicly maintaining 'all hypotheses remain on the table'
By Glen Owen Political Editor For The Mail On Sunday
Published: 17:01 EDT, 18 June 2022 | Updated: 18:20 EDT, 18 June 2022
- Director-general Tedros Adhanom confided to a senior European official: source
- The Mail on Sunday first revealed concerns about Wuhan's Institute of Virology
- Worldwide death toll of Covid pandemic now estimated to be above 18million
- WHO initially branded lab leak fears 'a conspiracy theory', accepting China story
While publicly the group maintains that ‘all hypotheses remain on the table’ about the origins of Covid, the source said Tedros Adhanom Ghebreyesus, director-general of the World Health Organisation (WHO), had recently confided to a senior European politician that the most likely explanation was a catastrophic accident at a laboratory in Wuhan, where infections first spread during late 2019.
The Mail on Sunday first revealed concerns within Western intelligence services about the Wuhan Institute of Virology, where scientists were manipulating coronaviruses sampled from bats in caves nearly 1,000 miles away – the same caves where Covid-19 is suspected to have originated – in April 2020. The worldwide death toll from the Covid pandemic is now estimated to have hit more than 18 million.
The WHO was initially criticised for its deferential approach to China over the pandemic, as well as a willingness to accept Beijing’s protestations that claims of a laboratory leak were just a ‘conspiracy theory’.
However, in the absence of any compelling evidence of ‘zoonotic’ spread – the process by which a virus leaps from animals to humans – it is now adopting a more neutral public stance.
Dr Tedros updated member states on the pandemic this month, admitting: ‘We do not yet have the answers as to where it came from or how it entered the human population.
‘Understanding the origins of the virus is very important scientifically to prevent future epidemics and pandemics.
‘But morally, we also owe it to all those who have suffered and died and their families. The longer it takes, the harder it becomes. We need to speed up and act with a sense of urgency.
‘All hypotheses must remain on the table until we have evidence that enables us to rule certain hypotheses in or out. This makes it all the more urgent that this scientific work be kept separate from politics. The way to prevent politicisation is for countries to share data and samples with transparency and without interference from any government. The only way this scientific work can progress successfully is with full collaboration from all countries, including China, where the first cases of SARS-CoV-2 were reported.’
The Mail on Sunday first revealed concerns about the region's Institute of Virology in 2020
It was suggested Covid 'could easily have escaped while being analysed' by scientists
Last year, the WHO established the Scientific Advisory Group for the Origins of Novel Pathogens (Sago) to outline which studies would be needed to identify the origins of SARS-CoV-2 – as Covid is scientifically known – and to ‘create a global framework for studying the origins of emerging and re-emerging pathogens’.
An original probe into the outbreak by the WHO was resisted fiercely by China, leading to a report that concluded the SARS-CoV-2 virus probably passed to humans from a bat via another unidentified species.
But after 14 nations including the UK, US and Australia criticised its findings as being heavily compromised, Dr Tedros admitted the report’s flaws and ordered the new process.
The Government has taken a cautious approach to apportioning blame for Covid – something that China-sceptics attribute to a fear of offending Beijing.
However, American intelligence has placed the secretive Wuhan laboratory at the centre of its analysis.
Former US Secretary of State Mike Pompeo claimed that workers at the institute had fallen ill with Covid-like symptoms in autumn 2019 – weeks before the alarm was raised, and said that as part of military projects its scientists were experimenting with a bat coronavirus very similar to the one that causes Covid.
A WHO spokesman said: ‘Dr Tedros has been consistently saying all hypotheses remain on the table as scientists pursue their work.’
jward
passin' thru
My apologies, I'll delete my entry, and replace with something novel if I see it.
I posted this early this morning but it's so important it's worth repeating (and it's a page up so can't hurt to dupe it)
And btw, I should've posted this when I posted the substack - Taiwan joined the club. They are now also going to be boosting their babies as well.
HD
Heliobas Disciple
TB Fanatic
My apologies, I'll delete my entry, and replace with something novel if I see it.
You didn't have to delete it, I just pointed it out because of the possible confusion over 'did I see that somewhere before' when something is reposted , which I did (get confused!). I probably shouldn't have said anything. And that article is so horrible that maybe we should post it on every page. Why are we one of the only countries in the world who is doing this to our babies? This is how we (the USA) are the shining beacon on the hill? It is unfathomable
HD
Heliobas Disciple
TB Fanatic
US Regulators Authorize COVID-19 Vaccines for Children as Young as 6 Months of Age
By Zachary Stieber
June 17, 2022
U.S. regulators on June 17 authorized two COVID-19 vaccines for young children.
The U.S. Food and Drug Administration (FDA) granted emergency authorization for the Moderna and Pfizer COVID-19 vaccines for children as young as 6 months old.
Previously, only children 5 and up could get the Pfizer vaccine, and only people 18 and older could get Moderna’s jab.
“We know that many parents, caregivers and clinicians have been anxiously awaiting today’s authorizations. We’re acutely aware of the importance of having vaccines available for our youngest children. And as we’ve seen with the older age groups, we expect that the vaccines for younger children will provide protection for the most severe outcomes of COVID-19, such as hospitalization and death,” Dr. Robert Califf, the FDA’s commissioner, told reporters on a call.
About 19.5 million children under 5 reside in the United States, according to Census Bureau estimates.
The FDA’s move came two days after its vaccine advisory panel unanimously voted to recommend regulators grant emergency authorization for the shots.
Estimates from clinical trials the companies ran pegged the efficacy of Moderna’s vaccine against infection at 50.6 percent for children 6 months through 23 months of age and 36.8 percent for children aged 2 to 5, and the efficacy of Pfizer’s vaccine was estimated at 80.3 percent across the age groups.
For young children, the Moderna vaccine efficacy estimates were based on just 490 children and the Pfizer efficacy estimates were based on just 220 children.
The FDA said in its new statement that Pfizer’s estimate “was determined not to be reliable due to the low number of COVID-19 cases that occurred in study participants.”
No estimates were possible for protection against severe illness—which is the primary reason officials say to get vaccinated because the protection has waned considerably as new virus variants emerge—because of the low numbers of severe cases among vaccinated and unvaccinated volunteers.
“As with all vaccines for any population, when authorizing COVID-19 vaccines intended for pediatric age groups, the FDA ensures that our evaluation and analysis of the data is rigorous and thorough,” Dr. Peter Marks, a top official at the FDA, said in a statement.
Authorization has a lower evidentiary bar than approval, and is only possible because U.S. authorities have maintained a COVID-19 emergency designation despite cases, hospitalizations, and deaths linked to the disease plunging since the metrics hit fresh peaks in January.
Some outside experts have questioned the data from the trials.
“From an efficacy standpoint, it makes absolutely no sense to approve these products,” Brian Hooker, chief scientific officer for Children’s Health Defense, told The Epoch Times before the authorization.
Others agreed with authorizations, asserting the data indicated sufficient protection.
“Although the Moderna vaccine was not as effective, it is likely as effective as the vaccines are for Omicron (2-dose) for adults. Both vaccines increase antibodies which likely indicates a deeper T/B cell response being generated,” Dr. Monica Gandhi, a professor of medicine at the University of California, San Francisco, told The Epoch Times in an email. T and B cells are thought to protect against severe illness.
The Centers for Disease Control and Prevention (CDC) is meeting with its vaccine advisory panel on Friday and Saturday to discuss the data. The panel will decide whether to advise the CDC to say young kids should, or may, get the vaccines. The panel could also recommend the vaccines should only be administered to kids with serious health problems, like diabetes.
CDC Director Rochelle Walensky then makes the final decision.
I forgot to post the link for this article. Here it is now:
US Regulators Authorize COVID-19 Vaccines for Children as Young as 6 Months of Age
www.theepochtimes.com
Heliobas Disciple
TB Fanatic

US opens COVID vaccine to little kids; shots begin this week
U.S. health officials have opened COVID-19 vaccines for infants, toddlers and preschoolers — the last group without the shots.
 apnews.com
apnews.com
US opens COVID vaccine to little kids, shots begin next week
By MIKE STOBBE
yesterday
NEW YORK (AP) — The U.S. on Saturday opened COVID-19 vaccines to infants, toddlers and preschoolers.
The shots will become available next week, expanding the nation’s vaccination campaign to children as young as 6 months.
Advisers to the Centers for Disease Control and Prevention recommended the vaccines for the littlest children, and the final signoff came hours later from Dr. Rochelle Walensky, the agency’s director.
“We know millions of parents and caregivers are eager to get their young children vaccinated, and with today’s decision, they can,” Walensky said in a statement.
While the Food and Drug Administration approves vaccines, it’s the CDC that decides who should get them.
The shots offer young children protection from hospitalization, death and possible long-term complications that are still not clearly understood, the CDC’s advisory panel said.
The government has already been gearing up for the vaccine expansion, with millions of doses ordered for distribution to doctors, hospitals and community health clinics around the country.
Roughly 18 million kids will be eligible, but it remains to be seen how many will ultimately get the vaccines. Less than a third of children ages 5 to 11 have done so since vaccination opened up to them last November.
Here are some things to know:
WHAT KINDS ARE AVAILABLE?
Two brands — Pfizer and Moderna — got the green light Friday from the FDA and Saturday from the CDC. The vaccines use the same technology but are being offered at different dose sizes and number of shots for the youngest kids.
Pfizer’s vaccine is for children 6 months to 4 years old. The dose is one-tenth of the adult dose, and three shots are needed. The first two are given three weeks apart, and the last at least two months later.
Moderna’s is two shots, each a quarter of its adult dose, given about four weeks apart for kids 6 months through 5 years old. The FDA also approved a third dose, at least a month after the second shot, for children with immune conditions that make them more vulnerable to serious illness.
HOW WELL DO THEY WORK?
In studies, vaccinated youngsters developed levels of virus-fighting antibodies as strong as young adults, suggesting that the kid-size doses protect against coronavirus infections.
However, exactly how well they work is hard to pin down, especially when it comes to the Pfizer vaccine.
Two doses of Moderna appeared to be only about 40% effective at preventing milder infections at a time when the omicron variant was causing most COVID-19 illnesses. Pfizer presented study information suggesting the company saw 80% with its three shots. But the Pfizer data was so limited — and based on such a small number of cases — that experts and federal officials say they don’t feel there is a reliable estimate yet.
SHOULD MY LITTLE ONE BE VACCINATED?
Yes, according to the CDC. While COVID-19 has been the most dangerous for older adults, younger people, including children, can also get very sick.
Hospitalizations surged during the omicron wave. Since the start of the pandemic, about 480 children under age 5 are counted among the nation’s more than 1 million COVID-19 deaths, according to federal data.
“It is worth vaccinating even though the number of deaths are relatively rare, because these deaths are preventable through vaccination,” said Dr. Matthew Daley, a Kaiser Permanente Colorado researcher who sits on the CDC’s advisory committee.
In a statement Saturday, President Joe Biden urged parents to get them for their young children as soon as possible.
WHICH VACCINE SHOULD MY CHILD GET?
Either one, said Dr. Peter Marks, the FDA’s vaccine chief.
“Whatever vaccine your health care provider, pediatrician has, that’s what I would give my child,” Marks said Friday.
The doses haven’t been tested against each other, so experts say there’s no way to tell if one is better.
One consideration: It takes roughly three months to complete the Pfizer three-shot series, but just one month for Moderna’s two shots. So families eager to get children protected quickly might want Moderna.
WHO’S GIVING THE SHOTS?
Pediatricians, other primary care physicians and children’s hospitals are planning to provide the vaccines. Limited drugstores will offer them for at least some of the under-5 group.
U.S. officials expect most shots to take place at pediatricians’ offices. Many parents may be more comfortable getting the vaccine for their kids at their regular doctor, White House COVID-19 coordinator Dr. Ashish Jha said. He predicted the pace of vaccination will be far slower than it was for older populations.
“We’re going see vaccinations ramp up over weeks and even potentially over a couple of months,” Jha said.
CAN CHILDREN GET OTHER VACCINES AT THE SAME TIME?
It’s common for little kids to get more than one vaccine during a doctor’s visit.
In studies of the Moderna and Pfizer shots in infants and toddlers, other vaccinations were not given at the same time so there is no data on potential side effects when that happens.
But problems have not been identified in older children or adults when COVID-19 shots and other vaccinations were given together, and the CDC is advising that it’s safe for younger children as well.
WHAT IF MY CHILD RECENTLY HAD COVID-19?
About three-quarters of children of all ages are estimated to have been infected at some point. For older ages, the CDC has recommended vaccination anyway to lower the chances of reinfection.
Experts have noted re-infections among previously infected people and say the highest levels of protection occur in those who were both vaccinated and previously infected.
The CDC has said people may consider waiting about three months after an infection to be vaccinated.
Heliobas Disciple
TB Fanatic

COVID-19 vaccines and kids: What parents should know
Two years into the coronavirus pandemic, children as young as 6 months old are now eligible to get vaccinated against COVID-19. The Centers for Disease Control and Prevention (CDC) on Saturday greenlit the Pfizer and Moderna COVID-19 vaccines for kids under 6, the last remaining age group to be...
COVID-19 vaccines and kids: What parents should know
KATIE KINDELAN - GMA
Sat, June 18, 2022, 10:46 PM
Two years into the coronavirus pandemic, children as young as 6 months old are now eligible to get vaccinated against COVID-19.
The Centers for Disease Control and Prevention (CDC) on Saturday greenlit the Pfizer and Moderna COVID-19 vaccines for kids under 6, the last remaining age group to be eligible.
Here are nine questions answered about the COVID-19 vaccines and kids as families seek to make the best decisions.
1. What is the science behind the COVID-19 vaccine?
Both the Pfizer and Moderna vaccines use mRNA technology, which does not enter the nucleus of the cells and doesn't alter human DNA. Instead, it sends a genetic "instruction manual" that prompts cells to create proteins that look like the outside of the virus -- a way for the body to learn and develop defenses against future infection.
The Johnson & Johnson vaccine uses an inactivated adenovirus vector, Ad26, that cannot replicate. The Ad26 vector carries a piece of DNA with instructions to make the SARS-CoV-2 spike protein that triggers an immune response.
This same type of vaccine has been authorized for Ebola and has been studied extensively for other illnesses and for how it affects women who are pregnant or breastfeeding.
Neither of these vaccine platforms can cause COVID-19.
2. What is the status of vaccine eligibility for kids?
The Pfizer vaccine has already been available for those who are 5 and older but now is also available for kids ages 6 months through 4 years.
Moderna's vaccine has previously been available only for people ages 18 and older. The latest vaccine authorization is for kids ages 6 months to 5 years.
3. Why do kids need to be vaccinated against COVID-19?
While there have not been as many deaths from COVID-19 among children as adults, particularly adults in high-risk categories, kids can still get the virus and they can also transmit the virus to adults.
More than 13 million children have tested positive for the virus since the onset of the pandemic over two years ago, according to the American Academy of Pediatrics (AAP).
"We know that COVID does not spare kids," ABC News medical contributor Dr. John Brownstein, an epidemiologist and chief innovation officer at Boston Children's Hospital, said in December. "Maybe it’s less severe than their adult counterparts but we also know that the virus has had real significant impacts on morbidity and mortality in kids."
"We also know that kids play an important role as vectors of spread," he said. "And especially in light of increases we’re seeing right now, with increases of cases in kids in record numbers, infections among kids further perpetuate community transmission and further create risks for those who would be the most vulnerable of the virus."
4. Do kids experience the same vaccine side effects as adults?
Adolescents experienced a similar range of side effects to Pfizer's vaccine as seen in older teens and young adults -- generally seen as cold-like symptoms in the two to three days after the second dose -- and had an "excellent safety profile," Peter Marks, director of the FDA's Center for Biologics Evaluation and Research, said in August.
None of the children in Pfizer’s clinical trials of kids ages 5-11 experienced a rare heart inflammation side effect known as myocarditis, which has been associated with the mRNA vaccines in very rare cases, mostly among young men.
5. Is there data showing COVID-19 vaccines are safe for kids?
The CDC released three studies in December showing COVID-19 vaccines are safe and effective for children.
One study, which evaluated the safety reports of more than 42,000 children ages 5 to 11 who received a Pfizer shot, found the side effects from the Pfizer vaccine were mostly mild and temporary. It also found that myocarditis, a heart inflammation side effect that has been associated with the mRNA vaccines in very rare cases, does not appear to be a risk.
A second study, which looked at data from 243 children ages 12 to 17 in Arizona, found the Pfizer vaccine was 92% effective at preventing infection. The study, conducted between July and December when delta was the dominant variant in the U.S., also found that adolescents who developed COVID-19 reported a lower percentage of time masked in school and time masked in the community.
The third study, also conducted when delta was dominant, found that among children ages 5 to 17 hospitalized due to COVID-19, less than 1% were fully vaccinated against the virus.
6. How effective are the vaccines in children?
Pfizer said its three-dose vaccine was 80% effective against symptomatic omicron COVID-19 infection among children 6 months to under 5 years old.
In March, the company said its clinical trials showed the vaccine was safe and 100% effective in children ages 12-15, similar to the 95% efficacy among adult clinical trial participants.
Moderna’s preliminary analysis found its two-dose pediatric vaccine was 51% effective against symptomatic COVID-19 among children 6 months to under 2 years old, and 27% among children 2 to 5 years old -- roughly the same efficacy seen in adults during the omicron surge. Protection against serious disease and death was higher.
7. Do kids get the same dose of the vaccines as adults?
Pfizer's vaccine for kids under age 5 is three doses of 3 micrograms each. Each dose is one-tenth the adult dose.
Moderna's shot is two doses, with each dose a quarter of the adult dose. Moderna is also studying a third shot, or booster, for young children.
Kids ages 5 to 11 are given a 10-micrograms dose of the Pfizer vaccine, one-third of the adolescent and adult dose. Like with adults and adolescents, the pediatric vaccine is delivered in two doses, three weeks apart.
For 12-to-15-year-olds, the FDA has authorized the same dosing as adults with the Pfizer two-dose vaccine.
The FDA and CDC have recommended the Pfizer booster shots now available for kids ages 11 and older be administered five months after the primary vaccine series.
8. Could COVID-19 vaccines impact puberty and menstruation?
There is currently no clinical evidence to suggest any of the COVID-19 vaccines can have long-term effects on puberty or fertility.
9. Where can kids get vaccinated against COVID-19?
Vaccines are accessible at pediatricians' offices, children's hospitals, pharmacies like CVS, Walgreens and Rite-Aid and school and community-based clinics.
Parents can search for appointments at Vaccines.gov to find a local provider.
Heliobas Disciple
TB Fanatic

CDC recommends Pfizer, Moderna Covid vaccines for children under 5
The CDC recommended Saturday that children as young as 6 months old receive Covid-19 vaccines developed by Pfizer-BioNTech and Moderna.
 www.statnews.com
www.statnews.com
CDC recommends Pfizer, Moderna Covid vaccines for children under 5
By Jason Mast
June 18, 2022
The Centers for Disease Control and Prevention recommended Saturday that children as young as 6 months old receive Covid-19 vaccines developed by Pfizer-BioNTech and Moderna.
The move follows an unanimous vote earlier in the day by an advisory panel of outside experts known as Advisory Committee on Immunization Practices, or ACIP.
“Together, with science leading the charge, we have taken another important step forward in our nation’s fight against COVID-19. We know millions of parents and caregivers are eager to get their young children vaccinated, and with today’s decision, they can,” said CDC Director Rochelle Walensky in a statement.
Shots could be offered at pharmacies and other providers as soon as Monday.
“I have the ability with my vote today to save more lives than my particular decisions with extremely sick children have saved throughout my career,” said Sarah Long, a professor of pediatrics at Drexel University College of Medicine and a committee member.
For a subset of parents and guardians with children under the age of 5, the vaccines have been eagerly anticipated for months — a tool, like the first inoculations for adults, for restoring their lives to a sense of normalcy. During a public comment period for the hearing Friday, parents shared stories of kids who haven’t been able to visit grandparents or spoke aspirationally about doing basic things they read about in books, like going to the aquarium.
Yet it remains unclear how many families will elect to vaccinate their kids. Although CDC officials spent two days presenting data on the risk Covid-19 poses to kids — in terms of severe disease, the rare inflammatory condition known as MIS-C, and potential long Covid — much of the public messaging over the past two years has emphasized that kids are unlikely to become gravely ill from the virus.
Pfizer’s Covid vaccine has been available for all adolescents since May 2021 and to children 5 to 11 since October, but only 59% of children ages 12 to 17 and 29% of children 5 to 11 have gotten two doses of vaccine.
Moderna and Pfizer vaccines for kids, compared
2 min 16 sec
Experts expect that trend to continue with even younger kids. In an April Kaiser Family Foundation poll, less than 1 in 5 parents of children under 5 said they were eager to get their kids inoculated once shots became available.
One state, Florida, declined to preorder vaccines for young children at all, although CDC officials assured the ACIP that pharmacies and clinics in the state are able to order them.
The advisory committee expressed little doubt about the need for vaccines in children. Rather, much of the discussion centered on how they can communicate to parents that need, and how to ensure the vaccines are made as widely available as possible, especially as the vaccine rollout will increasingly rely on primary care providers.
“There is a large risk of inequitable access,” said Beth Bell, a clinical professor at the department of global health at the University of Washington.
In a Friday presentation, CDC pediatrician Katherine Fleming-Dutra showed data that 202 children between 6 months and 4 years of age had died of Covid-19 during the pandemic, making it among the five leading causes of death for young children.
That’s more deaths per year than hepatitis, meningitis, rotavirus, and other common infectious diseases each caused before routine vaccinations were recommended. And the risk wasn’t limited to any particular group: More than half of young children hospitalized due to Covid-19 had no underlying conditions.
“I am struck by these numbers,” said Katherine Poehling, director of pediatric population health at Wake Forest University School of Medicine and a committee member. “I’m also concerned that there’s really an underappreciation of the potential severity.”
The Moderna vaccine appears to provide protection after two doses, inducing a similar level of antibody in kids as it did in adults and reducing the risk of developing symptomatic Covid-19 during the initial Omicron wave by around 37%.
Pfizer’s data, however, was more complicated, and advisers raised questions about the exact figure the company’s scientists put out.
The company initially tried to develop a two-dose shot before switching to a three-dose series after the initial strategy failed to induce a sufficient number of antibodies or protect kids against Omicron. The three-dose shot induced a high level of antibodies, but because Pfizer began the trial toward the end of the Omicron surge, it only saw 10 Covid cases in the three-dose study: three in the vaccine group and seven in the placebo group, for 80% efficacy.
Advisers raised questions about the small sample size for the 80% estimate, arguing the vaccine was safe and effective but that they needed to manage parental expectations about how much protection it really offers — and how important it is that children come back for a third dose.
“I would not bet against the vaccine here,” Bill Gruber, Pfizer’s vice president of vaccine clinical research and development, said during one exchange.
“To be clear, I’m not betting against the vaccine,” responded Matthew Daley, a senior investigator at the Institute for Health Research at Kaiser Permanente Colorado. “I’m just arguing for greater transparency about what we know and don’t know with parents and that includes what to expect after a second dose.”
Others argued clinicians shouldn’t focus on efficacy figures. Rather, the antibody levels from both trials suggest that young children develop the same levels of immunity that have protected adults against severe disease during Omicron. And the side effect data shows the vaccine is safe.
“We talk a lot about the data, and we may lose the notion that we’re saving children’s lives,” said Long.
In part because the two vaccines have different dose schedules, the rollout will raise new questions. In the public hearing, one parent asked for wide availability of both series, so families can make a choice, and one committee member, Veronica McNally, asked for the CDC to create handouts clearly comparing the two shots. But it’s unclear how many people will have both vaccines offered at local pharmacies or providers.
The vaccine is also being rolled out in children who are also going through their routine pediatric vaccination. Neither Moderna nor Pfizer studied how the vaccine performed when co-administered with another shot, but the CDC recommended that in most cases, clinicians should administer at the same time as other vaccines, especially as many kids have fallen behind their vaccination schedule during the pandemic.
Children who are moderately or severely immunocompromised would receive a different schedule: Three doses for Moderna and three doses of Pfizer-BioNTech but spread further apart.
And both shots come in 10-dose vials that expire 12 hours after they’ve been opened. Advisers asked about single-dose vials, fearing that a vial will be opened to vaccinate one child and the rest will be wasted.
CDC officials argued it was a legitimate concern but not the main one.
“It is important to get shots with the arms and take advantage of every opportunity,“ said José Romero, director of National Center for Immunization and Respiratory Diseases. “Don’t feel guilty.”
Heliobas Disciple
TB Fanatic

Heliobas Disciple
TB Fanatic
Moving on to other covid news:
(fair use applies)
Studies Suggest Possible Link of Neuromyelitis Optica Diagnosis After COVID-19 Vaccination
By Marina Zhang
June 18, 2022
Emergent peer-reviewed studies have highlighted the occurrence of neuromyelitis optica after COVID-19 vaccinations, suggesting that the autoimmune disease may be occurring as a vaccine adverse event.
The studies’ general findings indicate an occurrence of neuromyelitis optica (NMO) in healthy individuals within around two weeks after Pfizer, Moderna, and AstraZeneca vaccines. In patients already affected by the disease or a similar neurological autoimmune disease such as multiple sclerosis, an exacerbation of symptoms or relapse was observed.
So far, at least six cases of NMO occurring after COVID-19 vaccination have been reported in case studies around the world. Though some individuals made a full recovery, some were discharged with long-term medications or unresolved symptoms.
Neuromyelitis optica is a rare autoimmune disease in which the immune system mistakenly attacks the spinal cord and the nerves in the eyes. Though there is no cure, treatment can prevent future relapses that will do further damage to nerves.
While the cause of the disease is unknown, it is usually triggered by an infection or another autoimmune disease. It can affect anyone at any age, though it is more common in women than in men.
The 5-year survival rate for single attack NMO is 90 percent if treated, and for relapsing (more than one attack) NMO, it is nearly 70 percent.
Symptoms include pain in the eyes, loss of vision, paralysis, weakness or pain in the arms and legs, bladder and bowel problems as well as uncontrollable vomiting and hiccups.
Adverse events are medical occurrences, generally developing within 28 days after vaccination. According to the World Health Organization, “any untoward medical occurrence which follows immunization,” even one not caused by the vaccine, would be considered an adverse event.
Neuromyelitis Optica Occurring After Pfizer Vaccine
Two studies, one in Turkey and one in Germany suggested that the Pfizer vaccination may have been the trigger for the NMO disorder. The two women affected developed NMO symptoms within 24 hours and 23 days, respectively, after getting the vaccine.
In the Turkish study, a 43-year-old, previously healthy woman developed impaired vision 24 hours after the second dose of the Pfizer vaccine.
A month after treatment she experienced a second attack, with pain, increased sensation, and tingling on the right side of her body, muscle weakness, and urinary retention.
The doctors diagnosed her with NMO “possibly triggered by the administration of the COVID-19 mRNA-BNT162b2 vaccine.” She made a near-complete recovery and was put on long-term monoclonal antibody treatment.
The German study examined a 68-year-old woman, who had lived with suspected multiple sclerosis for many years, the primary symptom being mild leg paralysis. After earlier receiving tetanus and pneumococcal vaccines, she had suffered a loss of mobility in her legs, which was treated successfully. However, 23 days after receiving the first Pfizer dose in May 2021, her symptoms were severely exacerbated. She lost the ability to walk and experienced a lack of bladder and bowel control.
The woman declined the second dose of the vaccine and there was no relapse of symptoms.
Neuromyelitis Optica Occurring After Moderna Vaccines
The two Moderna studies both conducted in the United States also involved women. The first patient was a healthy 19 year old; the second was 46 years old with a medical history of vitamin B deficiency. Both showed symptoms within 15 and 2 days of getting the first dose of the vaccine respectively.
The 19-year-old woman had severe weakness in her arms and legs and urinary incontinence after receiving the Moderna vaccine.
After receiving the first dose of the vaccine, the 46-year-old woman suffered weakness in her upper and lower extremities, urinary retention, and decreased sensation, as well as “constant, shooting, 10 out of 10 upper back pain.” Though her lower limb weakness and urinary retention were resolved, the report indicated that the decreased sensation may have persisted.
Neuromyelitis Optica Occurring After AstraZeneca Vaccines
In Thailand and Brazil, studies detailed adverse reactions after the AstraZeneca vaccines. The Thailand study found a previously healthy 46-year-old woman developed right leg weakness and loss of sensation in her right side ten days after the first dose. Though her leg weakness improved, abnormal sensations persisted.
The latter study examined a 62-year-old woman, with stable NMO for 8 years, who saw a relapse 7 days after her first dose, experiencing a loss of vision in the left eye. Her vision recovered in 3 weeks.
The case studies mentioned above are not exhaustive. Studies also cited the Sinovac® and Sputnik V COVID-19 vaccines in NMO cases occurring after vaccine administration.
The authors of the studies highlighted a need for future research and a “high degree of suspicion” in diagnosis and intervention. As NMO is a rapidly-progressive disease, if untreated, consequences can be severe, with possibilities of disability and death.
AstraZeneca spokesperson Sinead Keller told the Epoch Times that “cases of neuromyelitis have been reported rarely following vaccination,” with no confirmed causal relationship between the vaccination and this “extremely rare event.”
“We continue to work with regulators around the world to closely monitor safety information from all available sources as part of our routine surveillance,” Keller wrote in an email on June 16.
While not all of the cases have concluded a positive link, the findings suggest a possible connection between NMO and COVID-19 vaccination.
The Epoch Times reached out to Pfizer and Moderna for comment.
Studies Suggest Possible Link of Neuromyelitis Optica Diagnosis After COVID-19 Vaccination
By Marina Zhang
June 18, 2022
Emergent peer-reviewed studies have highlighted the occurrence of neuromyelitis optica after COVID-19 vaccinations, suggesting that the autoimmune disease may be occurring as a vaccine adverse event.
The studies’ general findings indicate an occurrence of neuromyelitis optica (NMO) in healthy individuals within around two weeks after Pfizer, Moderna, and AstraZeneca vaccines. In patients already affected by the disease or a similar neurological autoimmune disease such as multiple sclerosis, an exacerbation of symptoms or relapse was observed.
So far, at least six cases of NMO occurring after COVID-19 vaccination have been reported in case studies around the world. Though some individuals made a full recovery, some were discharged with long-term medications or unresolved symptoms.
Neuromyelitis optica is a rare autoimmune disease in which the immune system mistakenly attacks the spinal cord and the nerves in the eyes. Though there is no cure, treatment can prevent future relapses that will do further damage to nerves.
While the cause of the disease is unknown, it is usually triggered by an infection or another autoimmune disease. It can affect anyone at any age, though it is more common in women than in men.
The 5-year survival rate for single attack NMO is 90 percent if treated, and for relapsing (more than one attack) NMO, it is nearly 70 percent.
Symptoms include pain in the eyes, loss of vision, paralysis, weakness or pain in the arms and legs, bladder and bowel problems as well as uncontrollable vomiting and hiccups.
Adverse events are medical occurrences, generally developing within 28 days after vaccination. According to the World Health Organization, “any untoward medical occurrence which follows immunization,” even one not caused by the vaccine, would be considered an adverse event.
Neuromyelitis Optica Occurring After Pfizer Vaccine
Two studies, one in Turkey and one in Germany suggested that the Pfizer vaccination may have been the trigger for the NMO disorder. The two women affected developed NMO symptoms within 24 hours and 23 days, respectively, after getting the vaccine.
In the Turkish study, a 43-year-old, previously healthy woman developed impaired vision 24 hours after the second dose of the Pfizer vaccine.
A month after treatment she experienced a second attack, with pain, increased sensation, and tingling on the right side of her body, muscle weakness, and urinary retention.
The doctors diagnosed her with NMO “possibly triggered by the administration of the COVID-19 mRNA-BNT162b2 vaccine.” She made a near-complete recovery and was put on long-term monoclonal antibody treatment.
The German study examined a 68-year-old woman, who had lived with suspected multiple sclerosis for many years, the primary symptom being mild leg paralysis. After earlier receiving tetanus and pneumococcal vaccines, she had suffered a loss of mobility in her legs, which was treated successfully. However, 23 days after receiving the first Pfizer dose in May 2021, her symptoms were severely exacerbated. She lost the ability to walk and experienced a lack of bladder and bowel control.
The woman declined the second dose of the vaccine and there was no relapse of symptoms.
Neuromyelitis Optica Occurring After Moderna Vaccines
The two Moderna studies both conducted in the United States also involved women. The first patient was a healthy 19 year old; the second was 46 years old with a medical history of vitamin B deficiency. Both showed symptoms within 15 and 2 days of getting the first dose of the vaccine respectively.
The 19-year-old woman had severe weakness in her arms and legs and urinary incontinence after receiving the Moderna vaccine.
After receiving the first dose of the vaccine, the 46-year-old woman suffered weakness in her upper and lower extremities, urinary retention, and decreased sensation, as well as “constant, shooting, 10 out of 10 upper back pain.” Though her lower limb weakness and urinary retention were resolved, the report indicated that the decreased sensation may have persisted.
Neuromyelitis Optica Occurring After AstraZeneca Vaccines
In Thailand and Brazil, studies detailed adverse reactions after the AstraZeneca vaccines. The Thailand study found a previously healthy 46-year-old woman developed right leg weakness and loss of sensation in her right side ten days after the first dose. Though her leg weakness improved, abnormal sensations persisted.
The latter study examined a 62-year-old woman, with stable NMO for 8 years, who saw a relapse 7 days after her first dose, experiencing a loss of vision in the left eye. Her vision recovered in 3 weeks.
The case studies mentioned above are not exhaustive. Studies also cited the Sinovac® and Sputnik V COVID-19 vaccines in NMO cases occurring after vaccine administration.
The authors of the studies highlighted a need for future research and a “high degree of suspicion” in diagnosis and intervention. As NMO is a rapidly-progressive disease, if untreated, consequences can be severe, with possibilities of disability and death.
AstraZeneca spokesperson Sinead Keller told the Epoch Times that “cases of neuromyelitis have been reported rarely following vaccination,” with no confirmed causal relationship between the vaccination and this “extremely rare event.”
“We continue to work with regulators around the world to closely monitor safety information from all available sources as part of our routine surveillance,” Keller wrote in an email on June 16.
While not all of the cases have concluded a positive link, the findings suggest a possible connection between NMO and COVID-19 vaccination.
The Epoch Times reached out to Pfizer and Moderna for comment.
Jaybird
Veteran Member
Don't know who that is but they need to put there big girl panties on.
Heliobas Disciple
TB Fanatic
Efficacy Estimates for Pfizer's Vaccine for Young Children Come Under Scrutiny
(fair use applies)
Efficacy Estimates for Pfizer’s Vaccine for Young Children Come Under Scrutiny
By Zachary Stieber
June 18, 2022
The efficacy estimates Pfizer has offered for its COVID-19 vaccine for young children are being dismissed as unreliable even as the shot is being readied to be administered to millions of American toddlers and babies.
A Pfizer clinical trial for children aged 6 months to 5 years pegged the efficacy at 80.3 percent overall—82.3 percent for children aged 2 to 5, and 75.5 percent for kids 6 months to 2 years.
But those estimates were determined “not to be reliable due to the low number of COVID-19 cases that occurred in study participants,” the Food and Drug Administration (FDA) said in a statement on June 17.
The estimates were based on just 10 COVID-19 cases—seven among kids who received a placebo, and three among those who received the vaccine. All occurred after Feb. 7.
But they were portrayed as evidence the vaccine should be given to children across the country during meetings with vaccine advisory panels for the FDA and Centers for Disease Control and Prevention (CDC) this week.
“High efficacy was observed in the course of this trial,” Dr. William Gruber, a senior vice president for vaccine clinical research and development at Pfizer, told panelists during a meeting on Friday.
Gruber also showed a slide presenting the data.
The low number of cases resulted in wide-ranging confidence intervals, which indicate how confident one can be in the numbers.
The claimed efficacy is “a meaningless statistic,” Dr. Harvey Risch, a professor of epidemiology at the Yale School of Public Health, told The Epoch Times in an email.
A CDC official acknowledged during one of the meetings that the efficacy could end up being dramatically different than the numbers Pfizer is promoting.
“I would really hope in our communications that we not use that 80% effectiveness because my level of confidence in that number—I believe the vaccine is effective; I do not have any idea what that number will actually end up being,” Dr. Amanda Cohn, the official, said.
“Thirty days after vaccination, this could fall off very quickly, and we just want to monitor it closely,” she added.
Dr. Sarah Long, a member of the Advisory Committee on Immunization Practices, which advises the CDC on vaccine recommendations, was among those sharing a similar view on Friday, when the panel heard from Gruber.
“I just think we should assume we don’t have efficacy data” because of the small number of cases, she said.
Long was speaking hours after the FDA authorized the Pfizer and Moderna COVID-19 vaccines for toddlers and babies.
The primary endpoints of the trials of the vaccine makers were certain levels of neutralizing antibodies, thought to be a marker of protection against the CCP (Chinese Communist Party) virus, also known as SARS-CoV-2, the virus causes COVID-19.
The companies took a subset of trial participants and compared the levels of antibodies that the vaccines triggered with levels recorded in a randomized set of adults from trials conducted in 2020.
Dr. Stephen Hahn, the FDA’s commissioner at the time, said in interviews that year that the agency would not authorize any COVID-19 vaccines that weren’t at least 50 percent efficacious. The agency said that it “would expect that a COVID-19 vaccine would prevent disease or decrease its severity in at least 50% of people who are vaccinated.”
But it later offered a loophole to drug makers who already had authorized vaccines—they could use a technique called immunobridging, or compare the levels of antibodies in populations for whom the vaccines weren’t yet authorized to the levels in adults from previous trials.
Pfizer and Moderna both took advantage.
Pfizer ended up comparing the effect of three doses on kids to the effect of two doses on adults. Moderna stuck with a two-dose primary regimen.
The companies only measured clinical efficacy, or protection against infection, secondarily.
“Remember, the efficacy was not a requirement for approval,” Gruber said.
Moderna’s trial found efficacy that was substandard; just 43.7 percent effective in the youngest group, and 37.5 percent effective in the other children, if using the case definition from the trial. Using the CDC’s clinical definition, the efficacy improved a small amount, but not much.
Pfizer’s was pegged much higher, but can’t be relied upon, authorities now say.
Dr. Peter Marks, a top FDA official, told reporters on a June 17 call that Moderna’s data was “more mature” than Pfizer’s.
The median followup time for Moderna’s trial was over two months. Pfizer participants, on the other hand, had a median followup time of just 35 and 40 days, respectively, for infants and toddlers.
The issue stems from Pfizer adding a third dose to its trial because the second dose provided virtually no protection against infection.
“I think we will have to wait a little bit longer for Pfizer to have more mature effectiveness data to have to have the kind of confidence that we’d like to put out numbers,” Marks added.
But officials maintain that the unreliable estimates don’t matter.
“From FDA’s perspective, we would have been confident in the clinical benefit of this three-dose primary series based on the immunobridging alone, even if there were no efficacy data,” Dr. Dorian Fink, another FDA official, told the CDC advisory panel.
Risch disagrees.
“Immunobridging is irrelevant if there is approximately no serious risk to start with, which is the case for healthy children,” he told The Epoch Times.
The CDC’s panel is preparing to vote Saturday to advise the CDC on which children under 5 can get the vaccines.
Long, the panel member, indicated she was ready to vote for widespread use, even without any reliable efficacy figures.
“I would be comfortable enough with the immunobridging,” she said.
Officials and the vaccine companies say getting better effectiveness data will be possible once children in the real world, or outside the trials, receive the vaccines.
“Exactly what the vaccine efficacy is after dose three I think needs further data to inform,” Fink said. “And we would expect to get some of these data hopefully from updated analyses from the clinical trial if more cases are accrued recognizing of course that if the vaccine is authorized, that will result in unblinding of placebo recipients so they can get their three-dose series … and also from real-world effectiveness data.”
(fair use applies)
Efficacy Estimates for Pfizer’s Vaccine for Young Children Come Under Scrutiny
By Zachary Stieber
June 18, 2022
The efficacy estimates Pfizer has offered for its COVID-19 vaccine for young children are being dismissed as unreliable even as the shot is being readied to be administered to millions of American toddlers and babies.
A Pfizer clinical trial for children aged 6 months to 5 years pegged the efficacy at 80.3 percent overall—82.3 percent for children aged 2 to 5, and 75.5 percent for kids 6 months to 2 years.
But those estimates were determined “not to be reliable due to the low number of COVID-19 cases that occurred in study participants,” the Food and Drug Administration (FDA) said in a statement on June 17.
The estimates were based on just 10 COVID-19 cases—seven among kids who received a placebo, and three among those who received the vaccine. All occurred after Feb. 7.
But they were portrayed as evidence the vaccine should be given to children across the country during meetings with vaccine advisory panels for the FDA and Centers for Disease Control and Prevention (CDC) this week.
“High efficacy was observed in the course of this trial,” Dr. William Gruber, a senior vice president for vaccine clinical research and development at Pfizer, told panelists during a meeting on Friday.
Gruber also showed a slide presenting the data.
The low number of cases resulted in wide-ranging confidence intervals, which indicate how confident one can be in the numbers.
The claimed efficacy is “a meaningless statistic,” Dr. Harvey Risch, a professor of epidemiology at the Yale School of Public Health, told The Epoch Times in an email.
A CDC official acknowledged during one of the meetings that the efficacy could end up being dramatically different than the numbers Pfizer is promoting.
“I would really hope in our communications that we not use that 80% effectiveness because my level of confidence in that number—I believe the vaccine is effective; I do not have any idea what that number will actually end up being,” Dr. Amanda Cohn, the official, said.
“Thirty days after vaccination, this could fall off very quickly, and we just want to monitor it closely,” she added.
Dr. Sarah Long, a member of the Advisory Committee on Immunization Practices, which advises the CDC on vaccine recommendations, was among those sharing a similar view on Friday, when the panel heard from Gruber.
“I just think we should assume we don’t have efficacy data” because of the small number of cases, she said.
Long was speaking hours after the FDA authorized the Pfizer and Moderna COVID-19 vaccines for toddlers and babies.
The primary endpoints of the trials of the vaccine makers were certain levels of neutralizing antibodies, thought to be a marker of protection against the CCP (Chinese Communist Party) virus, also known as SARS-CoV-2, the virus causes COVID-19.
The companies took a subset of trial participants and compared the levels of antibodies that the vaccines triggered with levels recorded in a randomized set of adults from trials conducted in 2020.
Dr. Stephen Hahn, the FDA’s commissioner at the time, said in interviews that year that the agency would not authorize any COVID-19 vaccines that weren’t at least 50 percent efficacious. The agency said that it “would expect that a COVID-19 vaccine would prevent disease or decrease its severity in at least 50% of people who are vaccinated.”
But it later offered a loophole to drug makers who already had authorized vaccines—they could use a technique called immunobridging, or compare the levels of antibodies in populations for whom the vaccines weren’t yet authorized to the levels in adults from previous trials.
Pfizer and Moderna both took advantage.
Pfizer ended up comparing the effect of three doses on kids to the effect of two doses on adults. Moderna stuck with a two-dose primary regimen.
The companies only measured clinical efficacy, or protection against infection, secondarily.
“Remember, the efficacy was not a requirement for approval,” Gruber said.
Moderna’s trial found efficacy that was substandard; just 43.7 percent effective in the youngest group, and 37.5 percent effective in the other children, if using the case definition from the trial. Using the CDC’s clinical definition, the efficacy improved a small amount, but not much.
Pfizer’s was pegged much higher, but can’t be relied upon, authorities now say.
Dr. Peter Marks, a top FDA official, told reporters on a June 17 call that Moderna’s data was “more mature” than Pfizer’s.
The median followup time for Moderna’s trial was over two months. Pfizer participants, on the other hand, had a median followup time of just 35 and 40 days, respectively, for infants and toddlers.
The issue stems from Pfizer adding a third dose to its trial because the second dose provided virtually no protection against infection.
“I think we will have to wait a little bit longer for Pfizer to have more mature effectiveness data to have to have the kind of confidence that we’d like to put out numbers,” Marks added.
But officials maintain that the unreliable estimates don’t matter.
“From FDA’s perspective, we would have been confident in the clinical benefit of this three-dose primary series based on the immunobridging alone, even if there were no efficacy data,” Dr. Dorian Fink, another FDA official, told the CDC advisory panel.
Risch disagrees.
“Immunobridging is irrelevant if there is approximately no serious risk to start with, which is the case for healthy children,” he told The Epoch Times.
The CDC’s panel is preparing to vote Saturday to advise the CDC on which children under 5 can get the vaccines.
Long, the panel member, indicated she was ready to vote for widespread use, even without any reliable efficacy figures.
“I would be comfortable enough with the immunobridging,” she said.
Officials and the vaccine companies say getting better effectiveness data will be possible once children in the real world, or outside the trials, receive the vaccines.
“Exactly what the vaccine efficacy is after dose three I think needs further data to inform,” Fink said. “And we would expect to get some of these data hopefully from updated analyses from the clinical trial if more cases are accrued recognizing of course that if the vaccine is authorized, that will result in unblinding of placebo recipients so they can get their three-dose series … and also from real-world effectiveness data.”
Heliobas Disciple
TB Fanatic

‘Severely Flawed’: Cardiologist Criticizes FDA-Funded Study Suggesting Myocarditis, Pericarditis Risks from COVID-19 Vaccines
By Marina Zhang and Enrico Trigoso
June 18, 2022 Updated: June 19, 2022
“Severely flawed” is a cardiologist’s verdict on a peer-reviewed study funded by the Food and Drug Administration (FDA) suggesting possible risks of developing myocarditis and pericarditis after getting a COVID-19 vaccine.
The recent FDA study published on June 11, 2022, used health insurance databases to identify myocarditis or pericarditis hospitalizations occurring in people aged 18 to 64 years, 1 to 7 days after a Pfizer or Moderna vaccine.
The authors found that though only 12 to 14 percent of the studied cohort were 18- to 25-year-olds, 33 to 42 percent of the myocarditis or pericarditis events occurred in people of this age group, suggesting that this age group may be linked with these vaccine adverse events.
“These results do not indicate a statistically significant risk difference between mRNA-1273 (the Moderna vaccine) and BNT162b2 (the Pfizer vaccine), but it should not be ruled out that a difference might exist,” the authors wrote in the study.
However, cardiologist Dr. Sanjay Verma told The Epoch Times that the study “using a 7-day limit for clinical endpoints” for myocarditis or pericarditis events after vaccination was “severely flawed.”
Verma, who practices in Coachella Valley, California, has been seeing many more heart problems since the vaccines rolled out.
“Continued increased risk [of myocarditis or pericarditis]” was found by the Centers for Disease and Prevention (CDC)’s Reports (MMWR) “even at 21 days after vaccination,” Verma wrote in an email.
Explaining that spike proteins have been found in blood circulation even four months after injection, “there is no medical justification for a 7- or 21-day cutoff,” he said.
Further, a British pre-print led by researchers from the University of Oxford found “continued increased risk of myocarditis after the booster,” which was not assessed by the FDA study.
Verma pointed out further issues in the study, stating that it does not include 12- to 17-year-olds, “who are the highest risk cohort.”
The same CDC MMWR report also found that the 12- to 17-year-old cohort has “2 to 3 times increased incidence compared to the 18- to 29-year-old cohort,” the doctor explained.
After the second dose, males aged 12 to 17 years had an incidence of 22.0 to 35.9 myocarditis or pericarditis cases out of 100,000 as compared to males aged 18 to 29 years who had an incidence of 6.5 to 15 cases out of 100,000, demonstrating that teens have a higher risk than adults.
Verma also added that “the study does not account for those who may have died before hospitalization,” who would not be “included in insurance claims database.”
Nonetheless, the cardiologist noted a “tremendous improvement” in the study for using health insurance databases as compared to prior FDA studies that exclusively relied on the Vaccine Adverse Event Reporting System (VAERS), which would most likely result in a lower incidence of cases.
“Overall, the findings of the study are interesting, but the above limitations likely yield significant underestimation of the true risk of myocarditis or pericarditis after COVID vaccination.”
“Public safety and ethical post market pharmacovigilance warrants more robust active longitudinal follow-up to ensure informed consent and appropriate risk stratification counseling,” Verma concluded.
Heliobas Disciple
TB Fanatic

Fauci Won't Commit to Stop Funding Chinese Research With US Tax Dollars
www.theepochtimes.com
Fauci Refuses to ‘Stop Funding Chinese’ Research With US Tax Dollars
‘China is the drug he just can’t quit’: GOP Senator slams NIAD head’s remarks
By Eva Fu
June 17, 2022 Updated: June 18, 2022
Dr. Anthony Fauci said he was unable to commit to stop federal funding from going to Chinese scientific research, despite the U.S. intelligence community assessing the regime as America’s top adversary.
Fauci, the head of the National Institute of Allergy and Infectious Diseases (NIAID), made the remarks while appearing virtually at the Health, Education, Labor & Pensions Committee hearing on June 16, during an exchange with Sen. Roger Marshall (R-Kansas).
“The NIH is still funding research in China, at least $8 million since 2020. In the Intelligence Community’s 2022 Annual Threat Assessment, the Chinese Communist Party is presented as one of the top threats to the United States, along with Russia, Iran, Syria, and North Korea. To my knowledge, only China is receiving U.S. research dollars,” said the senator during the hearing. “When will you as director of NIAID stop funding research in China?”
Since 2020, the National Institutes of Health (NIH) has awarded a total of $8.3 million in grants to the Chinese Center for Disease Control and Prevention and its division National Center for AIDS/STD Control and Prevention, along with five top public universities in mainland China and Hong Kong, according to the NIH website.
Although this amount doesn’t capture dollars later funneled to a Chinese institution through a U.S.-based organization, such as New York-based EcoHealth Alliance, which had partnered with the Wuhan Institute of Virology to perform coronavirus-related experiments that some experts said fit the definition of gain-of-function research, that is, experiments that increase the pathogenicity or transmissibility of a virus.
Fauci, in response to Marshall’s question, said that the U.S. federal agencies “had very productive peer-reviewed highly regarded research projects with our Chinese colleagues that have led to some major advances in biomedical research.”
“So I don’t think I’d be able to tell you that we are going to stop funding Chinese,” Fauci said.
“We obviously need to be careful and make sure that when we do fund them we have the proper peer review and we go through all the established guidelines,” he continued, adding that “grants that go to foreign countries, including China, have State Department clearance.”
“Dr. Fauci’s remarks prove that China is the drug he just can’t quit,” Marshall later told The Epoch Times about the NIAID head’s response.
“Dr. Fauci told the truth for once after years of repeated dishonesty that has eroded Americans’ trust in our public health institutions. In the aftermath of the coronavirus pandemic, our government should know it’s dangerous and wrong to continue funding research projects supported by the Chinese Communist Party.”
The senator, at the hearing, followed up by asking Fauci if he agrees that the American public lacks records and studies from EcoHealth Alliance’s research.
Fauci’s answer was evasive.
“We have access to an extraordinary amount of information that has gone there,” he said, arguing that the publicly available information in the scientific journals is sufficient.
“Obviously none of us know everything that’s going on in China but if the question at hand is the rather small … peer-reviewed high-priority grant that was given from Eco[Health] to China in a sub-award we have a lot of good information that’s in the publishing.”
The NIH gave a total of $3.1 million grant to EcoHealth over the five years from 2014 to 2019. A fifth of that, $599,000, went to the Wuhan lab, in part for identifying and altering bat coronaviruses deemed likely to infect humans, documents obtained by The Intercept show.
Fauci earlier this week tested positive for COVID-19 and joined the Thursday Senate hearing remotely. His response to Marshall omitted reference EcoHealth’s lack of disclosure over some of its research activities, which would have prompted an NIH review over biosafety measures.
In one experiment at the Wuhan facility, funded by NIH via EcoHealth, mice infected with a modified version of the original bat coronavirus “became sicker than those infected” with the original version, an “unexpected result” that was not “something that the researchers set out to do,” Lawrence Tabak, the principal deputy director at the NIH, told lawmakers last October.
He said EcoHealth had violated grant terms by failing to promptly notify the NIH about the finding.
Fauci, at the Thursday hearing, also told Sen. Mike Braun (R-Ind.) that he believes the outbreak of the virus “is very, very likely a jump in species from an animal host,” and less likely to be the result of a lab leak.
“I believe it’s essential to have cooperation and collaboration with the Chinese,” he said when Braun asked him whether he thinks Beijing will cooperate with him to “get to the thorough bottom of” COVID-19 origins.
Heliobas Disciple
TB Fanatic

CDC Puts Mexico at Highest Risk Level for Travel Destinations Amidst Increasing COVID-19 Cases
By Marina Zhang
June 18, 2022
The Centers for Disease Control and Prevention (CDC) placed Mexico at the highest level for travel destination risk on June 13, advising travelers to be up to date on their vaccinations, or avoid traveling to Mexico.
The popular tourist destination for Americans was moved to level 3 for travel risks on June 13. COVID-19 cases have been increasing in Mexico since May 30, with cases averaging around 4,500 cases in the past week.
Along with Mexico, New Caledonia and the United Arab Emirates were also added to level 3 for travel risks on June 13.
New Caledonian cases averaged 42 cases a day, with no new cases on June 13, while the United Arab Emirates gained around 1,300 new cases on June 13, averaging a bit over 1,000 cases for the past seven days.
On April 18, the CDC overhauled its travel risk rating system. Level 3 is now considered the “high” category of travel risk, while level 4 is reserved for special circumstances.
A level 3 travel risk means there have been over 100 new cases per 100,000 residents, while a level 4 risk indicates a strong recommendation to avoid the destination.
The news comes as the federal government removed negative COVID-19 test requirements on June 10, for international air travelers coming into the United States.
The CDC “will end COVID-19 testing requirement for air travelers entering the country,” said the White House spokesman Kevin Munoz on Twitter, adding that it “will evaluate its need based on the science and in context of circulating variants.”
In recent days, travel industry groups have pressed the Biden administration to end the mandatory testing requirement, describing the rule as harmful and needless.
Several countries have already dropped negative testing requirements to enter their respective countries in recent months. That includes Canada, which in April dropped its pre-arrival testing requirement for vaccinated people.
Roger Dow of the U.S. Travel Association said that as COVID-19 restrictions on numerous other businesses have been lifted, “the travel industry remains disproportionately harmed by this requirement.”
“Other countries with whom we directly compete for global travelers have removed their pre-departure testing requirements and reopened their tourism economies, putting the U.S. at a serious competitive disadvantage for export dollars,” Dow argued in a May 31 statement after travel industry leaders met with White House staff.
Jack Phillips contributed to this report.
Heliobas Disciple
TB Fanatic
Catching COVID-19 Could Increase Your Risk of Parkinson’s Disease
According to a recent study, the coronavirus can increase the mouse brain's susceptibility to a toxin that causes the death of nerve cells seen in Parkinson's disease COVID-19 patients commonly report symptoms such as brain fog, headaches, and insomnia. These neurological complications after a vi
scitechdaily.com
Catching COVID-19 Could Increase Your Risk of Parkinson’s Disease
By Thomas Jefferson University
June 18, 2022
According to a recent study, the coronavirus can increase the mouse brain’s susceptibility to a toxin that causes the death of nerve cells seen in Parkinson’s disease
COVID-19 patients commonly report symptoms such as brain fog, headaches, and insomnia. These neurological complications after a viral infection are not new; in fact, it took patients nearly a decade to develop the neurological disease known as “post-encephalic parkinsonism” after the 1918 influenza pandemic. In a recent study with mice, Jefferson and colleagues demonstrate that the SARS-CoV-2 virus that caused the COVID-19 pandemic could raise the likelihood of the brain degeneration found in Parkinson’s disease.
“Parkinson’s is a rare disease that affects 2% of the population above 55 years, so the increase in risk is not necessarily a cause for panic,” says Richard Smeyne, Ph.D., Director of the Jefferson Comprehensive Parkinson’s Disease and Movement Disorder Center at the Vickie and Jack Farber Institute for Neuroscience and first author of the study. “But understanding how coronavirus impacts the brain can help us prepare for the long-term consequences of this pandemic.”
The study, published on May 17 in the journal Movement Disorders, expands on prior findings from the Smeyne lab indicating that viruses can increase the susceptibility of brain cells or neurons to damage or death. In that earlier study, the researchers discovered that mice exposed to the H1N1 influenza strain that caused the 2009 flu pandemic were more vulnerable to MPTP, a toxin known to cause some of the characteristic symptoms of Parkinson’s disease, most notably the loss of neurons that express the chemical dopamine and increased inflammation in the basal ganglia, a brain region that is crucial for movement. Researchers in Denmark verified the results in people, showing that influenza more than quadrupled the probability of acquiring Parkinson’s disease within 10 years of initial infection.
The new study employed mice that were genetically altered to express the human ACE-2 receptor, which the SARS-CoV-2 virus utilizes to get access to the cells in our airways. These mice were infected with SARS-CoV-2 and then allowed to recover. Importantly, the dosage used in this research corresponds to a mild COVID-19 infection in people, with around 80% of infected mice surviving. Thirty-eight days after the surviving mice had recovered, one group was given a modest dosage of MPTP that would not ordinarily trigger neuron loss. The control group was given saline. The animals were sacrificed and their brains were examined two weeks later.
The researchers discovered that COVID-19 infection alone had no impact on dopaminergic neurons in the basal ganglia. However, mice given a modest dosage of MPTP after recovering from infection demonstrated the classic pattern of neuron loss found in Parkinson’s disease. This increased sensitivity following COVID-19 infection was comparable to what was reported in the influenza trial, suggesting that both viruses might cause an equal increase in the risk of developing Parkinson’s.
“We think about a ‘multi-hit’ hypothesis for Parkinson’s – the virus itself does not kill the neurons, but it does make them more susceptible to a ‘second hit’, such as a toxin or bacteria or even an underlying genetic mutation,” explains Dr. Smeyne.
Both influenza and SARS-CoV2 have been found to cause a “cytokine storm” or an overproduction of pro-inflammatory chemicals. These chemicals can cross the blood-brain barrier and activate the brain’s immune cells – microglia. Indeed, the researchers found increased numbers of activated microglia in the basal ganglia of mice that recovered from SARS-CoV2 and received MPTP. While the mechanism is not fully understood, the researchers believe the increased microglia inflame the basal ganglia and cause cellular stress. This then lowers the neurons’ threshold to withstand subsequent stress.
This study was co-led by collaborator Peter Schmidt, Ph.D., a neuroscientist from New York University. “We were concerned about the long-term consequences of viral infection,” Dr. Schmidt said. “Dr. Smeyne is a leader in this area of research and Jefferson was the ideal site to perform the analysis.”
The researchers are planning to determine whether vaccines can mitigate the experimental increase in Parkinson’s pathology linked to prior SARS-CoV-2 infection. They are also testing other variants of the virus, as well as doses that correspond to milder cases in humans.
While their findings thus far bolster a possible link between the coronavirus and Parkinson’s disease, Dr. Smeyne says there are some important caveats. “First of all, this is preclinical work. It is too soon to say whether we would see the same thing in humans, given that there seems to be a 5-10 year lag between any changes in clinical manifestation of Parkinson’s in humans.” This lag, he says, however, could be used to our advantage. “If it does turn out that COVID-19 increases the risk of Parkinson’s, it will be a major burden on our society and healthcare system. But we can anticipate that challenge by advancing our knowledge of potential ‘second hits’ and mitigating strategies.”
This work was supported by a grant from the State of North Carolina and NIH R21 NS122280. The authors report no conflict of interest.
Reference: “COVID-19 Infection Enhances Susceptibility to Oxidative Stress-Induced Parkinsonism” by Richard J. Smeyne Ph.D., Jeffrey B. Eells Ph.D., Debotri Chatterjee BA, Matthew Byrne BS, Shaw M. Akula Ph.D., Srinivas Sriramula Ph.D., Dorcas P. O’Rourke DVM and Peter Schmidt Ph.D., 17 May 2022, Movement Disorders.
DOI: 10.1002/mds.29116
Heliobas Disciple
TB Fanatic

Omicron Variant Less Likely To Cause Long COVID
The SARS-CoV-2 Omicron variant is less likely to cause long COVID than the Delta variant, new research has found. Analysis by researchers from King’s College London of data from the ZOE COVID Symptom study app is published today (June 18, 2022) in a letter to the medical journal The Lancet. The f
scitechdaily.com
Omicron Variant Less Likely To Cause Long COVID
By King's College London
June 18, 2022
According to new research, the risk of long COVID was less during the Omicron wave compared to the Delta wave.
The SARS-CoV-2 Omicron variant is less likely to cause long COVID than the Delta variant, new research has found.
Analysis by researchers from King’s College London of data from the ZOE COVID Symptom study app is published today (June 18, 2022) in a letter to the medical journal The Lancet. The findings are from the first peer-reviewed study to report on long COVID risk and the Omicron variant.
Long COVID is defined by NICE guidelines as having new or ongoing symptoms four weeks or more after the start of the disease. Symptoms include fatigue, shortness of breath, loss of concentration, and joint pain. The symptoms can adversely affect day-to-day activities, and in some cases can be severely limiting.
Researchers found the odds of experiencing long COVID were between 20-50% less during the Omicron period versus the Delta period, depending on age and time since vaccination.
The study identified 56,003 UK adult cases first testing positive between December 20, 2021, and March 9, 2022, when Omicron was the dominant strain. Researchers compared these cases to 41,361 cases first testing positive between June 1, 2021, and November 27, 2021, when the Delta variant was dominant.
The analysis shows 4.4% of Omicron cases were long COVID, compared to 10.8% of Delta cases. However, the absolute number of people experiencing long COVID was in fact higher in the Omicron period. This was because of the vast number of people infected with Omicron from December 2021 to February 2022. The UK Office of National Statistics estimated the number of people with long COVID actually increased from 1.3 million in January 2022 to 2 million as of May 1st, 2022.
Lead author, Dr. Claire Steves from King’s College London, said: “The Omicron variant appears substantially less likely to cause Long-COVID than previous variants but still 1 in 23 people who catch COVID-19 go on to have symptoms for more than four weeks. Given the numbers of people affected it’s important that we continue to support them at work, at home and within the NHS.”
Reference: “Risk of long COVID associated with delta versus omicron variants of SARS-CoV-2” by Michela Antonelli, Joan Capdevila Pujol, Tim D Spector, Sebastien Ourselin and Claire J Steves, 18 June 2022, The Lancet.
DOI: 10.1016/S0140-6736(22)00941-2
Heliobas Disciple
TB Fanatic

South Africa hails COVID vaccine patent waiver
South Africa on Saturday hailed a WTO agreement to allow developing countries to start producing their own COVID vaccines following a near two-year battle.
South Africa hails COVID vaccine patent waiver
June 18, 2022
South Africa on Saturday hailed a WTO agreement to allow developing countries to start producing their own COVID vaccines following a near two-year battle.
"We secured an agreement. It was a strongly-fought agreement," said Minister of Trade Ebrahim Patel, who along with India and NGOs had been calling for an intellectual property rights waiver on COVID-related treatments.
The World Trade Organization (WTO) announced a relaxation of intellectual property restrictions on vaccines on Wednesday in a move aimed at a providing more equitable access to jabs but which many observers criticised for being limited in time and scope.
After months of wrangling, and talks going down to the wire this week to win over some major players in pharmaceutical manufacturing to a compromise text, the United States and China finally clinched the deal by agreeing on which countries would benefit from the waiver.
Both South Africa and India had been vocal in their demands for such a move which they said was needed to stop "vaccine apartheid".
According to the WTO, 60 percent of the world's population has received two doses of anti-COVID vaccine but there are glaring examples of inequity with only 17 percent having been jabbed in Libya, with the figure just eight percent in Nigeria and less than five in Cameroon.
In a statement, the South African government saluted a waiver designed to provide local vaccine manufacturers with the right to produce either vaccines or ingredients or elements that are under patents, without the authority of the patent holder, hailing this as a notable step forward—even if limited to five years.
Pretoria added that "to scale up the production on the continent, further partnerships will be needed including access to know-how and technologies".
The accord for the time being excludes, however, tests and costly therapeutic treatments against COVID on which the WTO is to pronounce in the coming six months.
Commercialisation in Africa will be a challenge, however.
Durban-based South African pharma giant Aspen, which clinched a deal last November with US-based Johnson & Johnson to manufacture a "made in Africa for Africa" Aspen-branded COVID vaccine Aspenovax, said last month it could pull the plug owing to lack of orders.
"Our focus now is to ensure we address demand by persuading global procurers for vaccines to source from African producers," said Patel.
South Africa has three sites under the aegis of Aspen in Durban, Afrigen in Cape Town and Biovac, also in Cape Town, which makes the Pfizer-BioNTech vaccine.
Afrigen's biotech consortium makes the messenger RNA jab based on the Moderna formula, the first to be made based on a broadly used vaccine that does not require the developer's assistance and approval.
Heliobas Disciple
TB Fanatic
I had Covid 2 weeks ago and yesterday I got run down from lack of sleep and having a garage sale and now the Covid has come back and I tested positive again. Can it return if you have a weakening in your immune system?
Are you feeling sick again or did you just test positive again? And did you test negative before you just tested positive? Could just be a testing issue - false positive now - or - false negative before and you're just taking longer to fully clear the virus from showing up on the test. Try testing again and see what comes up.
If you're actually sick again, I don't know the answer to your question. It can recur, and it makes sense if your immune system is weak that you'd be more vulnerable, but it may just be that you were exposed again. I'm surprised however that your immunity from a few weeks earlier didn't protect you. By any chance did you take paxlovid? There is a known rebound from it - you feel better while you take it and then a few days after you stop, you get sick again. So if you took it, this is not unexpected. If you didn't - I'm at a loss. Also, if your comfortable answering - are you vaccinated/boosted? that may play a role as well.
Are you taking any vitamins or other supplements? There have been a lot of posts on this thread and on TB in general about Vitamin D, Vitamin C, Zinc, Quericitin and then the prescription anti-virals. Of course, you should only take something if it's not going to interfere with other medications you may be taking or if you have allergies,etc. Only you and your doctor would know that.
Feel better, I will add my prayers for you to have a quick recovery if indeed you are sick again.
HD
Heliobas Disciple
TB Fanatic
Large covid percentage increases
21 min 42 sec
Jun 18, 2022
Dr. John Campbell
US, Variant Proportions, omicron mutants proliferate
https://covid.cdc.gov/covid-data-trac... BA.4 8.3% BA.5 13.3% Evolutionally driver Vaccine immune escape More severe? No Same symptoms? Yes Hospital admissions Up 4.6% on the week Seven day average, 4,330 UK covid England Summary | Coronavirus (COVID-19) in the UK https://www.ons.gov.uk/peoplepopulati... Week ending 11 June 2022 Percentage testing positive increased in England, Wales, Scotland and Northern Ireland Omicron variants BA.4 and BA.5. Percentage that had COVID-19 in the week ,131,000 (1 in 50 people) in England 64,800 (1 in 45 people) in Wales 42,900 (1 in 45 people) in Northern Ireland 176,900 (1 in 30 people) in Scotland Deaths involving COVID-19 fall Week ending 3 June 2022 UK, 211 deaths registered in the UK involving coronavirus 258 fewer than the previous week Total deaths registered in the UK, W/E 3rd June 7,881 (16% below the five-year average) 186 deaths involving COVID-19 in England and Wales 58.1% disease, underlying cause of death (64.9% in the previous week) Antibodies 99.3% in England 99.3% in Wales 99.4% in Northern Ireland 99.4% in Scotland Proportion of those aged under 16 years Antibodies at or above 179ng/ml (23 to 26 May 2022) Aged 8 to 11, 95.9% Aged 12 to 15, 95.7% Testing negative means that an individual did not have enough antibodies to be detected in the test, not that they do not have any immune protection against the virus.
Heliobas Disciple
TB Fanatic

Rational Nosocomophobia ?
Are we doing more harm than good in the name of public "health"?
Rational Nosocomephobia?
Are we doing more harm than good in the name of pubic "health"?
Robert W Malone MD, MS
12 hr ago

People have been asking me what I think of the CDC approval of these vaccine for babies and young children, and I have to ask them, do you really not know what I think?
I mean, seriously?
Have you looked at the VAERS data lately? The CDC apparently has not. In the USA alone, there have been 831,801 adverse events, of which 12,776 are life threatening. There have been 63,978 hospitalizations. There have been 13,293 deaths and 14,232 permanent disabilities from these vaccines. True, these are “unverified - but previous research has shown that the VAERS system under-reported adverse events associated with vaccines, not over-reported. Physicians and health care professionals rarely report adverse events past the 30 day window, so the true number of adverse events are unknown. But we do know that they are higher than reported. Remember that the mRNA in these vaccines continues to produce spike protein for at least 60 days. Then there are the international post-vaccine adverse event summaries.
The CDC, under Freedom of Information Act Request (FOIA) has now admitted that even though they had promised to analyze the VAERS data before advising about these vaccines for children, they did not. The VAERS data were NOT taken into consideration before the authorization of these genetic agents for babies and young children. Frankly, this is shocking. So shocking, it is hard for me to even write about it.
Now, approximately 430 children with other severe illnesses have died with COVID in the last 2.5 years (that would be 172 per year). Plus there have been 2,600 hospitalizations of children, most with underlying conditions - over that 2.5 year period. These numbers show that even before Omicron, in the case of children, COVID is less severe than flu. By way of comparison, on average influenza virus infection kills about 200 children yearly (the H1N1 pandemic 2009-10 had 358 pediatric flu-related deaths). Just like with COVID, 78% of those deaths were in children with other co-morbidities.
Omicron in children is much less severe. We know this. The scientific evidence is clear. Yet the FDA goes back to data from the DELTA variant when discussing the effects of this virus.
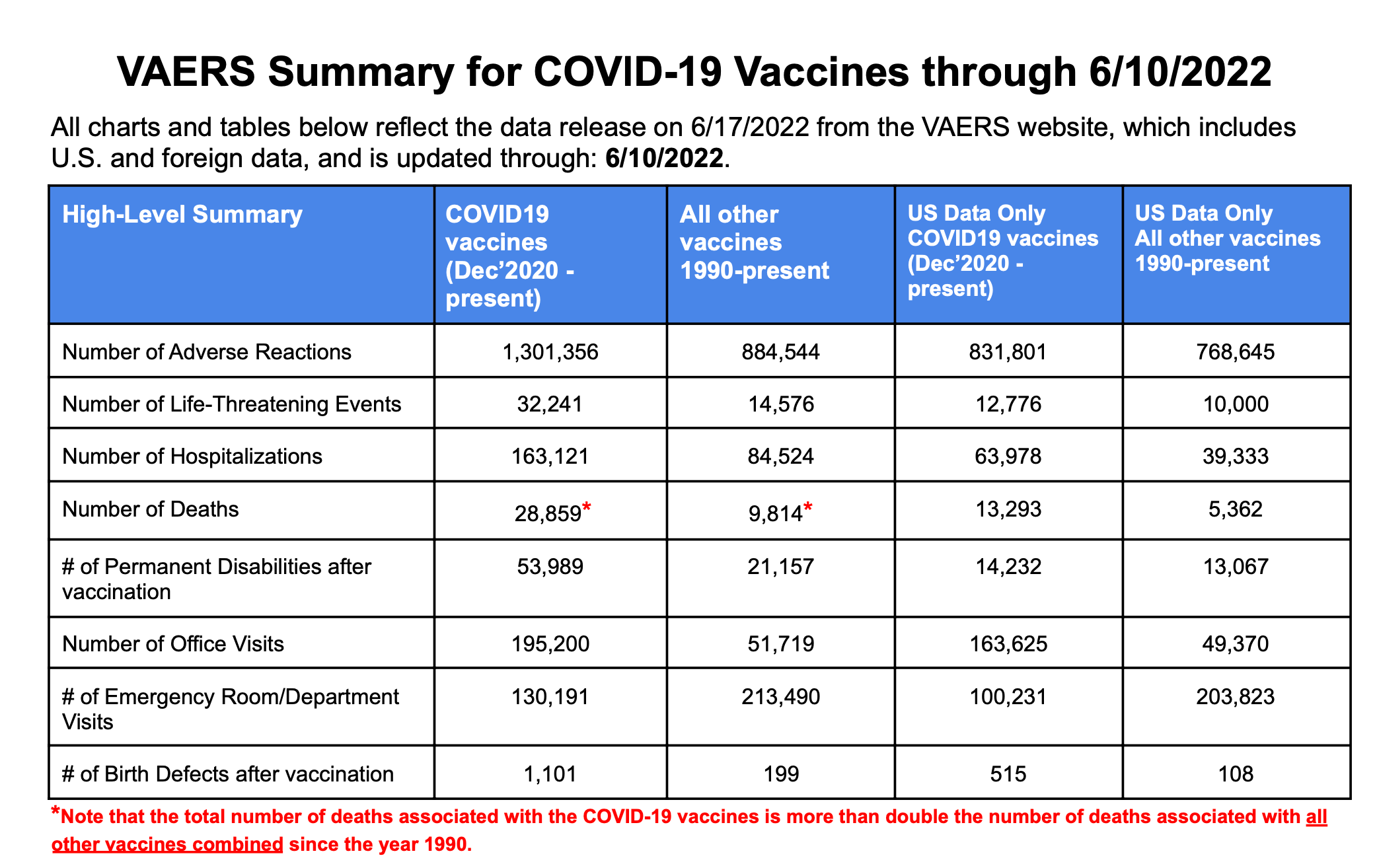
Now that omicron is here, the vaccine is completely mismatched for the circulating variant. Further vaccination with this mismatched product will continue to drive development of viral escape mutants that evade both monoclonal antibodies as well as vaccine-induced antibodies, and the effects of the vaccine are minimal at best at stopping transmission or disease in children and healthy, young adults. The adverse events and death rate are quite significant with these genetic vaccines, and there is some evidence of enhanced disease in the “fully” inoculated (three, four, five doses?). Something that our government refuses to research. In fact, there is evidence in countries such as Portugal, that there is more disease in the vaccinated. Remember that other nations, such as those in Africa, with very low vaccination rates, have had the least amount of death and disease.
Needle Phobia
Giving children booster after booster, injection after injection, week after week is not only a bad idea for control of the virus, it is also psychologically unhealthy for children. Just stop and think for a minute, the Pfizer vaccine is a THREE dose regime as an initial prime-boost. There will be more, because we know that three doses is only going to last for a very limited time. Of course, this research was also not conducted before authorization.
A chronically ill child, that requires many visits to the doctor’s office can develop phobias, such as needle phobia, Nosocomephobia (or "white coat syndrome"), Hemophobia or even Latrophobia. What does it do to a child to be taken to a clinic to be vaccinated - a painful procedure, week after week? To endure side-effects from a vaccine week after week? Then top this off with the 70+ other vaccines on the pediatric schedule? When does it end? To go through these procedures for a disease that is no more severe than the common cold?
Governor DeSantis again has it right.
It is time to stop. Parents must stop. The time is now to just say no.
Heliobas Disciple
TB Fanatic
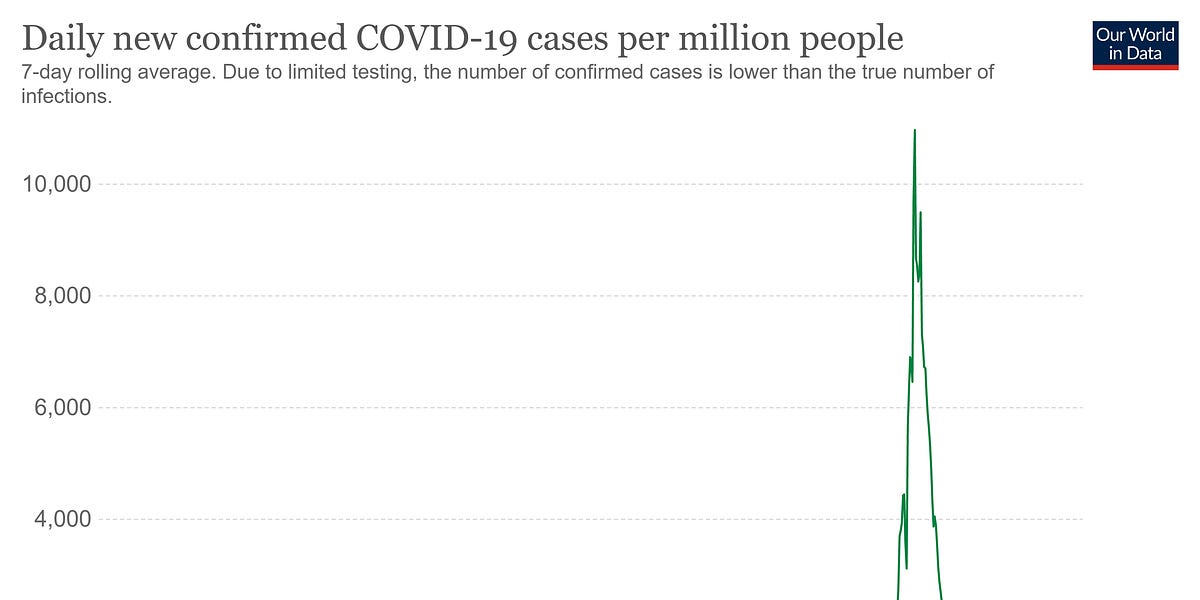
"Israel sees 70% spike in number of seriously ill COVID patients within a week"; see UK graph; go back to prior substacks, we have been warning about this, e.g. Vanden Bossche, we theorized
that sub-optimal non-sterilizing non-neutralizing vaccinal antibodies (Abs) bind to the spike but not eliminate, yet enhances/facilitates infection in vaxxed person, & soon we will see serious disease
"Israel sees 70% spike in number of seriously ill COVID patients within a week"; see UK graph; go back to prior substacks, we have been warning about this, e.g. Vanden Bossche, we theorized
that sub-optimal non-sterilizing non-neutralizing vaccinal antibodies (Abs) bind to the spike but not eliminate, yet enhances/facilitates infection in vaxxed person, & soon we will see serious disease
Dr. Paul Alexander
4 hr ago
Most if not all Israel is vaccinated and many boosted. The UK and Scottish data told us that the vaccinated, especially the double and triple vaccinated (over 50) are at increased risk of infection, hospitalization, and death.
I present the Israel case graph as of today and also the UK case graph as of today, both are showing rises in infection/cases (new wave).
The issue is that the same vaccinal Abs that enhance and facilitate infection in the upper respiratory tract (URT), have been blocking severe disease in the lower respiratory tract (LRT) deep inside the lung. GVB is prescient in this.
That is why we were seeing at first when Omicron emerged, a very strange situation we never saw before where a virus could do both things, cause infection yet mild illness. We even thought OMI was nature’s gift with mild illness. We spoke about this changing as the sub-optimal vaccinal immune pressure would cause the variants to overcome the pressure and we would shift from blocking illness in the LRT (transfection from infected to uninfected cells) to severe disease. Could this now be happening in Israel? I don’t know. We thought that it would happen in one of the most vaccinated nations. Could this be the beginning of a very dangerous situation we spoke about prior? Or is this the usual deaths that emerge 2-3 weeks post infection/case peak (death curve)? All the same, Israel is experiencing some trouble. Why? Near 100% vaccinated.
These vaccines are causing a serious problem.
See paper below by Yahi et al. as a concern for ADE in people receiving vaccines based on the original Wuhan strain spike sequence (either mRNA or viral vectors). Under these circumstances, second generation vaccines with spike protein formulations lacking structurally-conserved ADE-related epitopes should be considered. Yahi et al.’s research demonstrated in the case of the Delta variant (and certainly now in Omicron BA 4 & BA 5 sub-variants), neutralizing (blocking) antibodies have a decreased affinity for the spike protein, whereas facilitating or enhancing (non-neutralizing) antibodies displayed a pronounced increased affinity for the spike protein.
Israel cases:
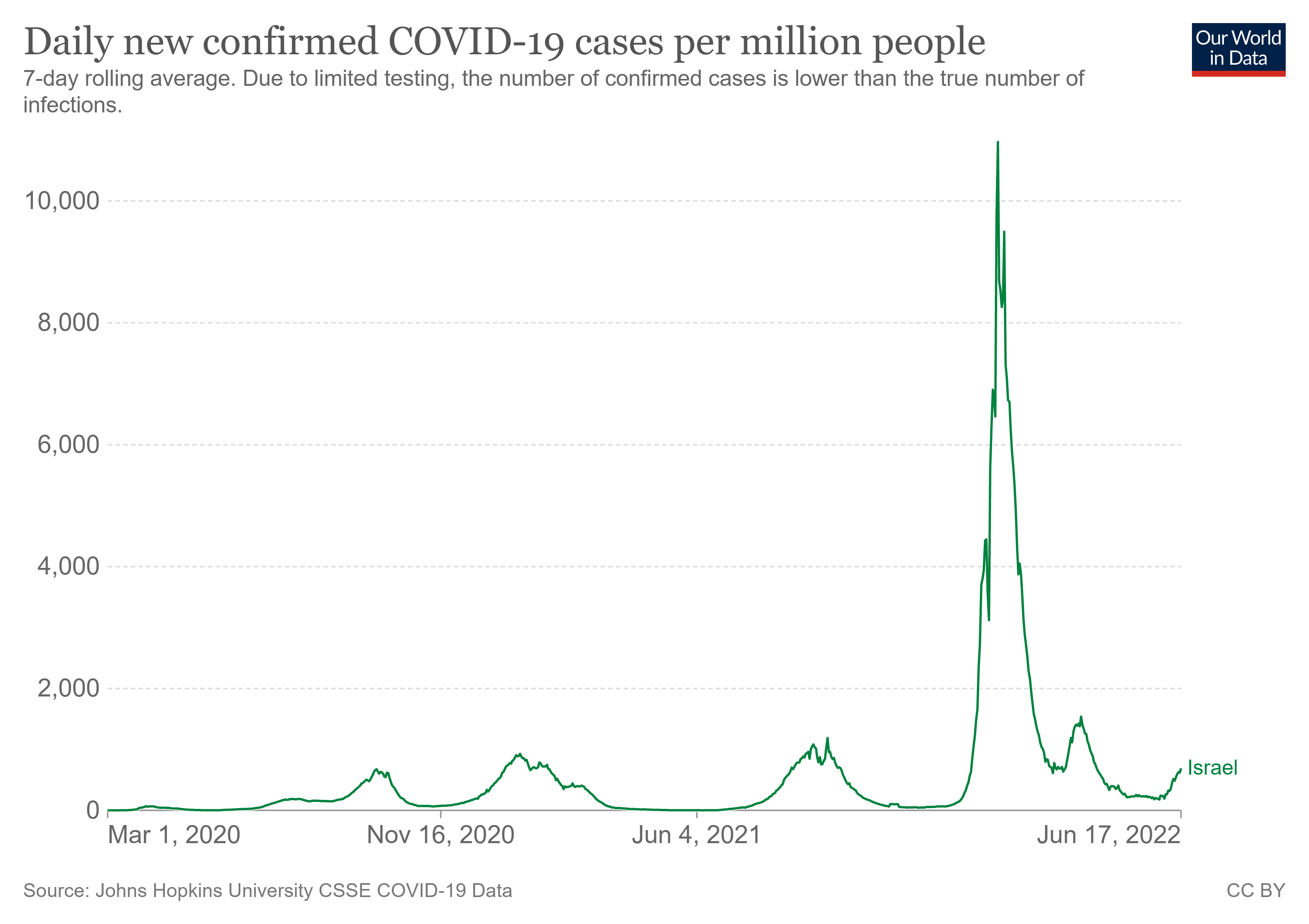
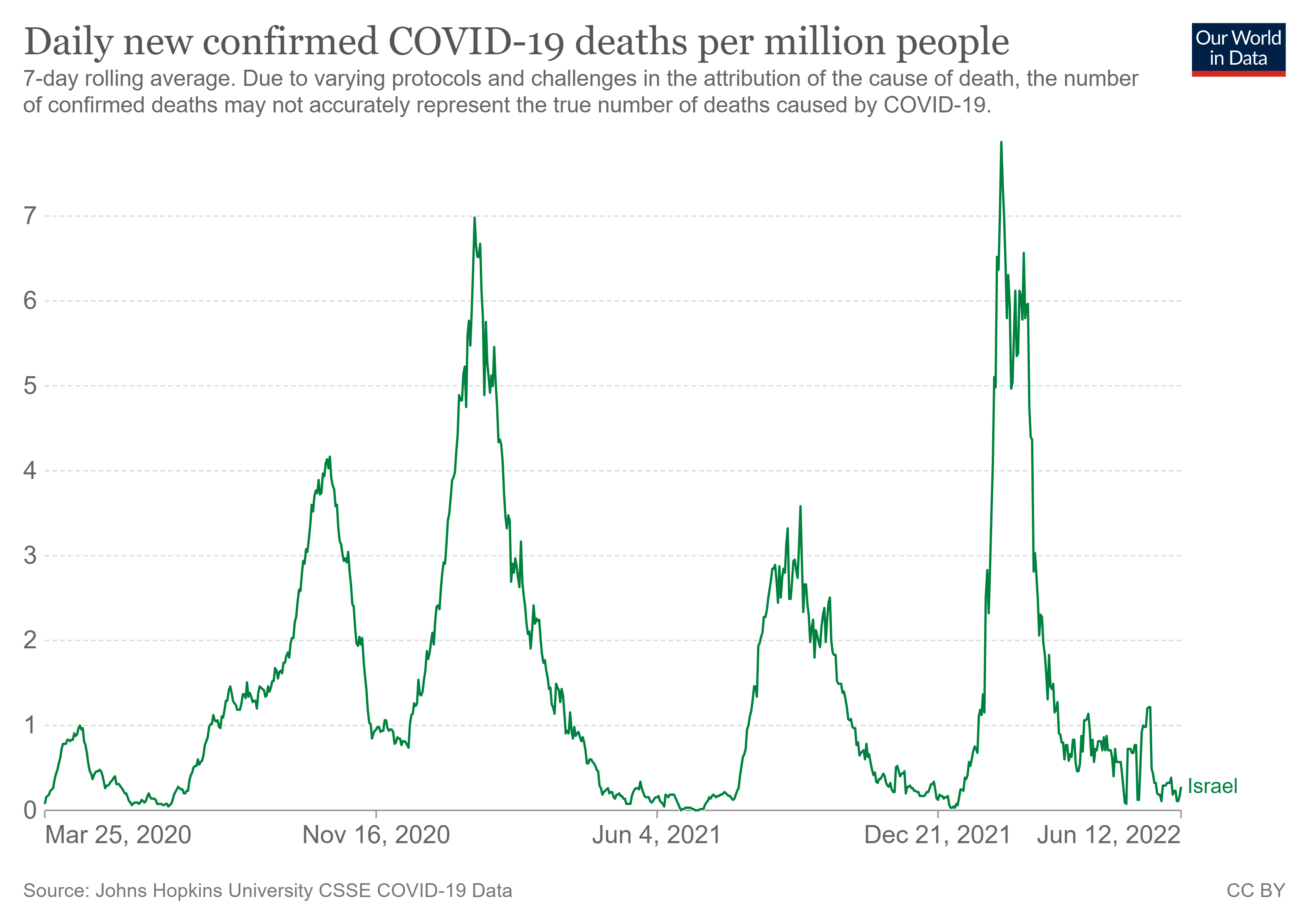
UK cases:
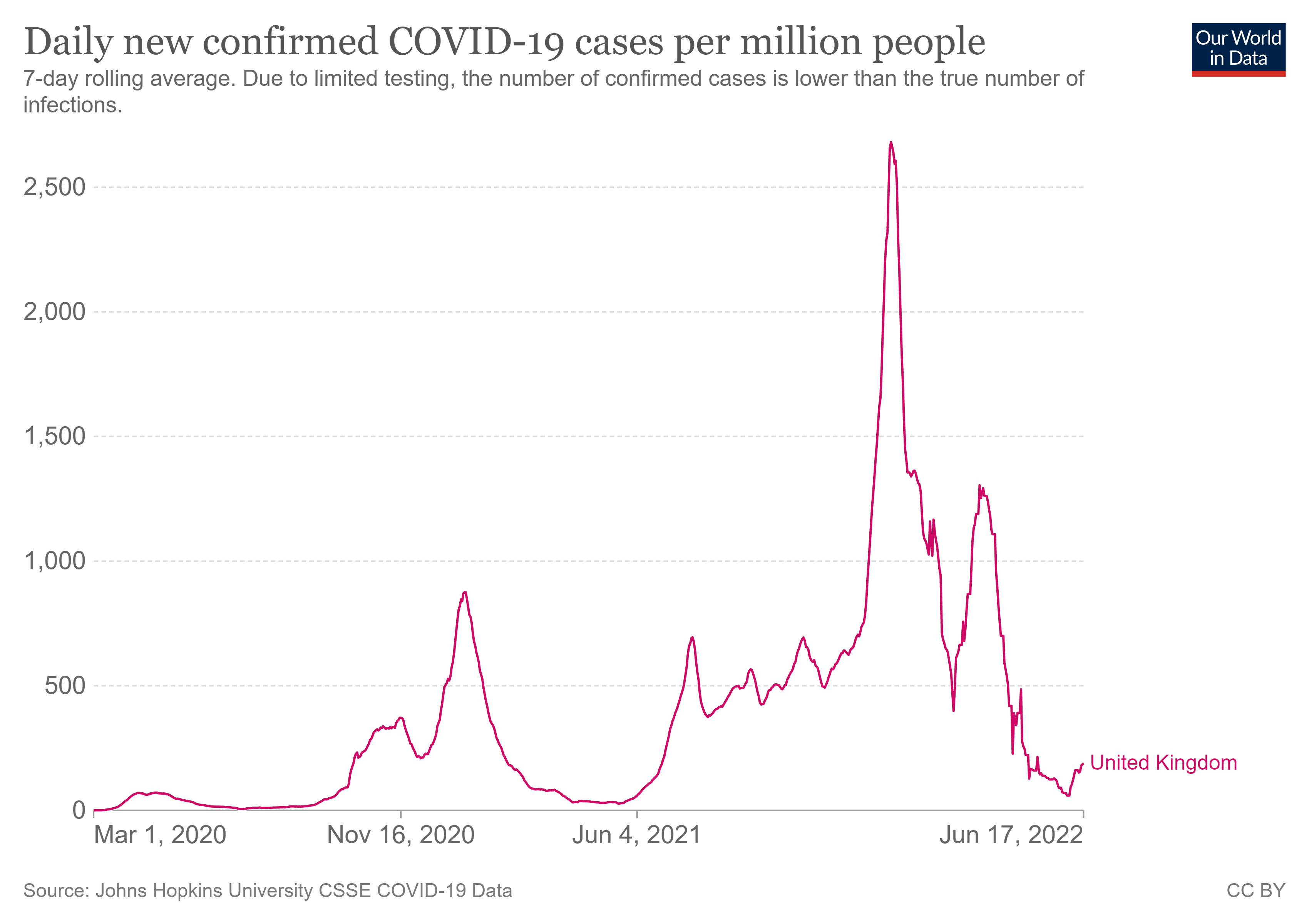
SOURCE:
Israel sees 70% spike in number of seriously ill COVID patients within a week
‘It’s an unpredictable and unstable situation,’ says immune system expert Prof. Cyrille Cohen, urging lawmakers to ‘actively encourage herd immunity among the vulnerable’
SOURCE:
Yahi et al.: Infection-enhancing anti-SARS-CoV-2 antibodies recognize both the original Wuhan/D614G strain and Delta variants. A potential risk for mass vaccination?
Heliobas Disciple
TB Fanatic
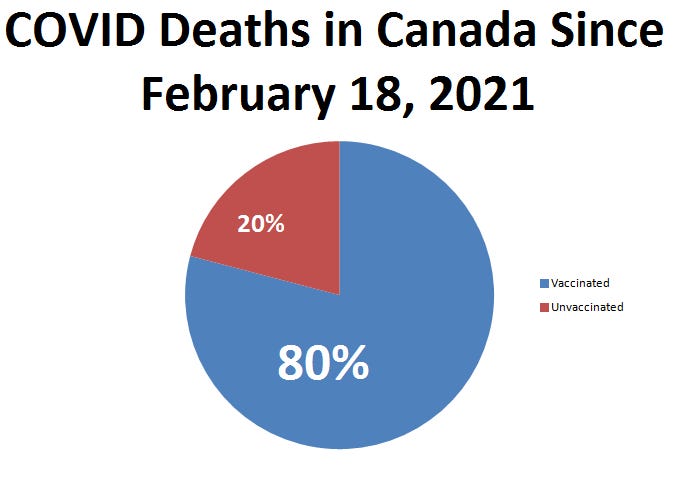
The Most Damning Evidence that Vaccines Don't Work
Health Canada Shenanigans
 sheldonyakiwchuk.substack.com
sheldonyakiwchuk.substack.com
The Most Damning Evidence that Vaccines Don't Work
Health Canada Shenanigans
Sheldon Yakiwchuk
18 hr ago
According to the COVID-19 epidemiology update, from December 14th, 2020 to May 29, 2022 - there were 19,230 Deaths.
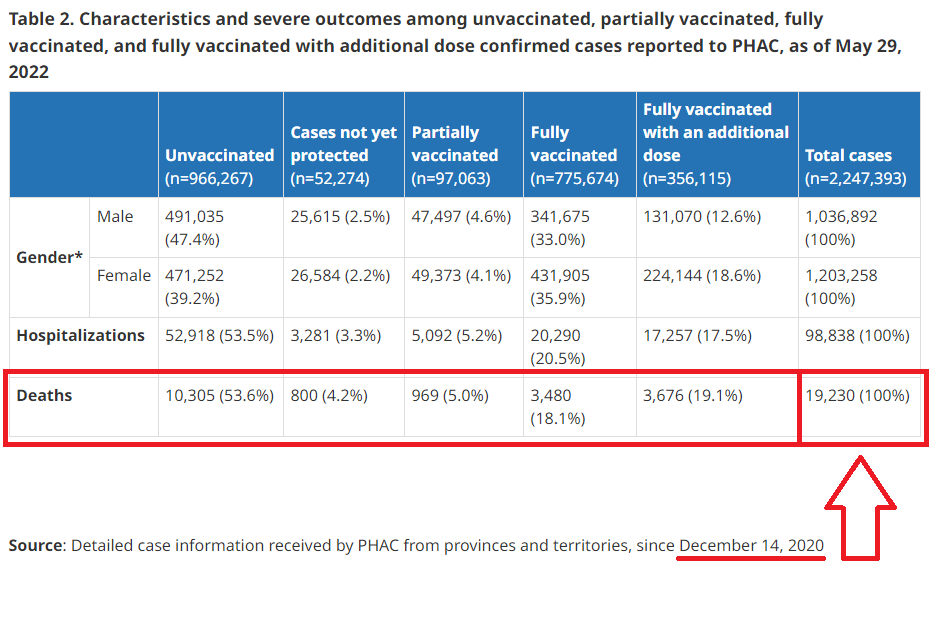
And this indicates that 10,305 of those in this - 53.6% - were Unvaccinated, meaning that the remaining 8,925 Deaths were Vaccinated (46.4%).
When a lot of people look at this, they still see success…I don’t know how, there is only a 3.6% variance between Vaccinated and Unvaccinated - not really much more than coin toss odds by getting jabbed or not.
But this assumes that everybody was vaccinated on the same day, which they weren’t. So when you try to overlay the vaccine schedule into this, this is where things become a lot crazy.
On December 14, 2020 According to the Epidemiology Update, there were 13,553 Deaths:

These would all be unvaccinated since this was the very first day of vaccinations. But now check this out…

It took from December 14, 2020 to February 18, 2021 to get 1% of the Population Vaccinated. By February 18, 2021 there were a total of 21,498 Deaths.

Meaning that there were 7,945 Deaths - From December 14, 2020 to February 18, 2021.
Because only 1% of the population had been vaccinated, these would most likely be Unvaccinated Deaths as well.
So…let’s take a look at the Total Deaths reported again from December 14, 2020 to current - 19,230 and subtract those 7,945 deaths and we’d get that from February 18, 2021 to current there have been 11,285 deaths, giving a mortality to 1% of the population vaccinated, to be something like this:
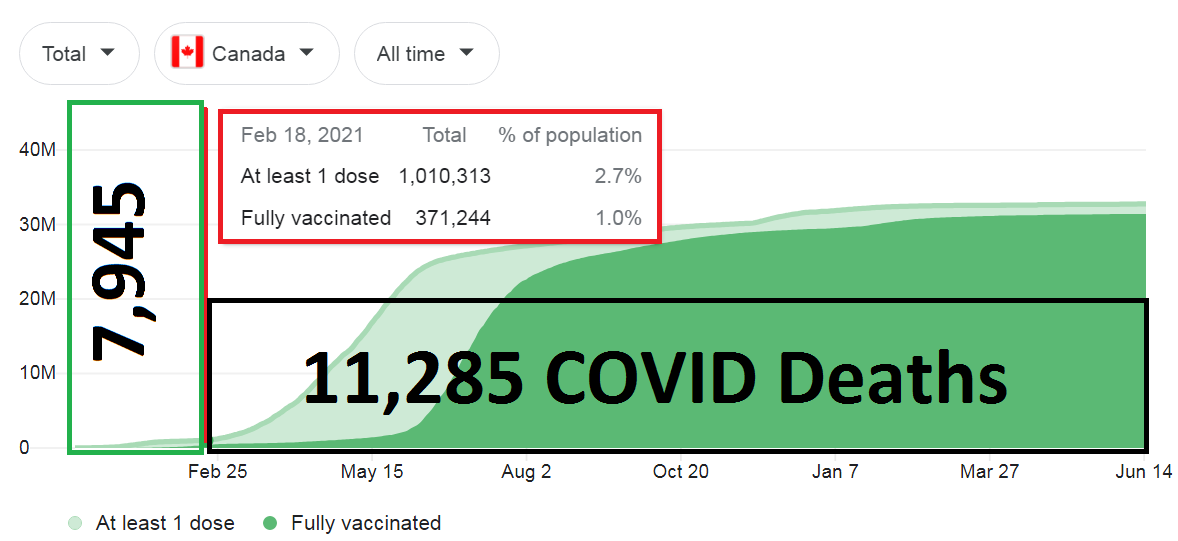
Since February 18, 2021 - there have been a total of 8,925 people who have been Vaccinated that died - meaning that only 2,360 Unvaccinated people have died in this period. What this looks like is, that since 1% of the population has been vaccinated, this is what the COVID deaths look like:
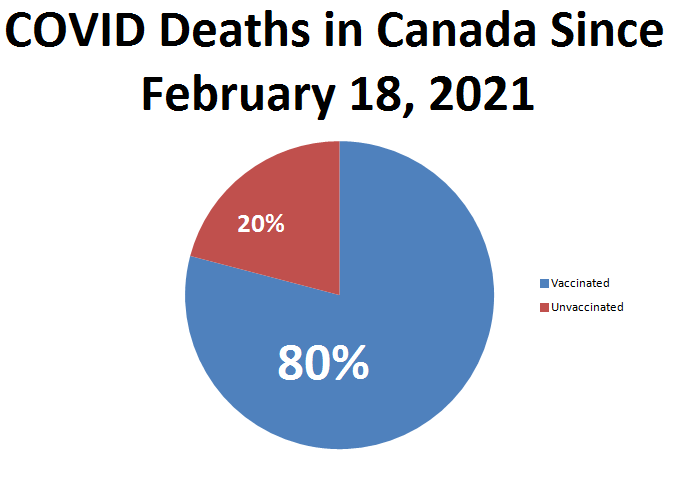
20% of the COVID Mortality is in the Unvaccinated Population.
80% of the COVID Mortality is in the Vaccinated.
We all know there is something fishy about the Health Canada Data that’s being presented but if this is the information we are left to work with, it really doesn’t look that good for the Vaccines…when 80% of the Mortality that’s happened since 1% of the population was vaccinated, are actually Vaccinated.
YIKES!
Heliobas Disciple
TB Fanatic

Where do those Numbers on the Chart Come From?
Explained.
Sheldon Yakiwchuk
16 hr ago
I have been doing a comparative weekly analysis on the Province of Alberta and on the Statistics posted by Health Canada throughout the last several months and have watched this whole Vaccination Sham unfold.
Having been fully immersed in the data daily, it’s easy for me to know exactly what I am looking at and for…and when I explain it, try to do it so that it makes sense to everybody and while it may…there can still be some confusion.
The biggest question asked via email, twitter and comments is - Where does this information come from…So, I’m going to lay it all out for you and then when you provide the information to others, you can share this to help them understand as well.
The most recent chart - that’s pretty damning is the following:

Because it literally shows 97.5% of the Cases, 62% of the Hospitalizations and 89% of the Mortality in V-Totals - Sum of all Vaccinated stratification.
The one thing you can notice is that underneath Cases/Hospitalizations and Deaths are 2 dates. May 29th and May 8th. 29th data is on top because it will show the Newest Numbers, which are typically an increase over the previous week and when setting up my Spreadsheets, it’s just easier (maybe lazy) for me to use the AutoSum button and replace : with -.
I try to keep this as a Weekly Update but quite often, Health Canada doesn’t cooperate so all I can do is keep several tabs open and keep refreshing.
You don’t have to do this.
The Wayback Time Machine helps…as does saving some screen shots of the data (it gets removed after updates).
Let’s begin!
On the Health Canada COVID-19 epidemiology update →Link, if you scroll down, you will come to Table 2.
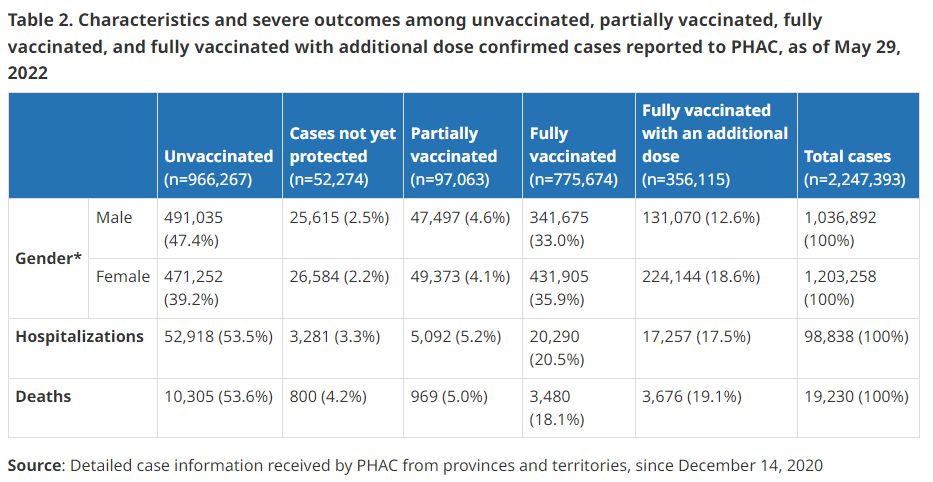
You’ve seen me post this same table several times…but may not completely understand where the information comes from.
Let’s break it down!
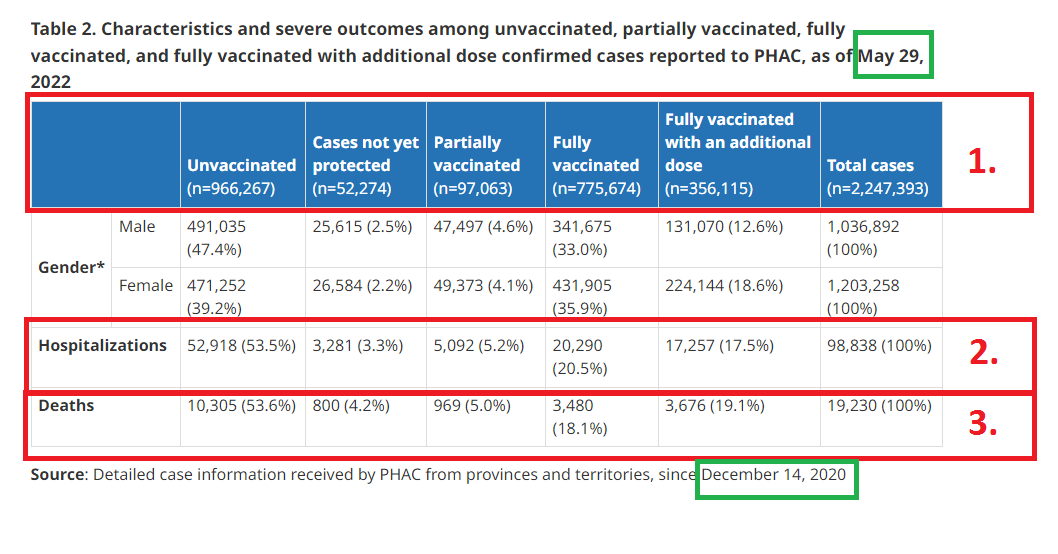
In the Top Green box on this chart, it will give the Current Date of the report. Note: Health Canada is typically 2-3 weeks behind in their reporting.
The Bottom Green box on this chart, is the date that they started recording deaths from COVID under a Vaccinated stratified chart - will always be December 14th.
- Top bar is headers, but in the brackets, these are the total cases for each of the groups, ex: Unvaccinated (n=966,267).
- Hospitalizations for each of the groups.
- Deaths for each of the group - left to right.
Finding the comparative dates and data can be tricky and a lot relies on luck, screen shots and having an idea of what I am looking for.
Lot’s of credit goes back to the Wayback Machine for Historical Data.
Click this link (WB Machine HC Data Base) to pull the dates for comparison, note that the Table 2 isn’t always updated daily and you’ll most likely have to pull the PDF version to even see it.
You can find the PDF update version in the top right hand corner of the screen:
I hope this helps answer your questions and sorry for the delay in getting back to a lot of you regarding this question.
Keep posting in comments or reply to your emails if you need more help and I will answer as time affords.
Heliobas Disciple
TB Fanatic
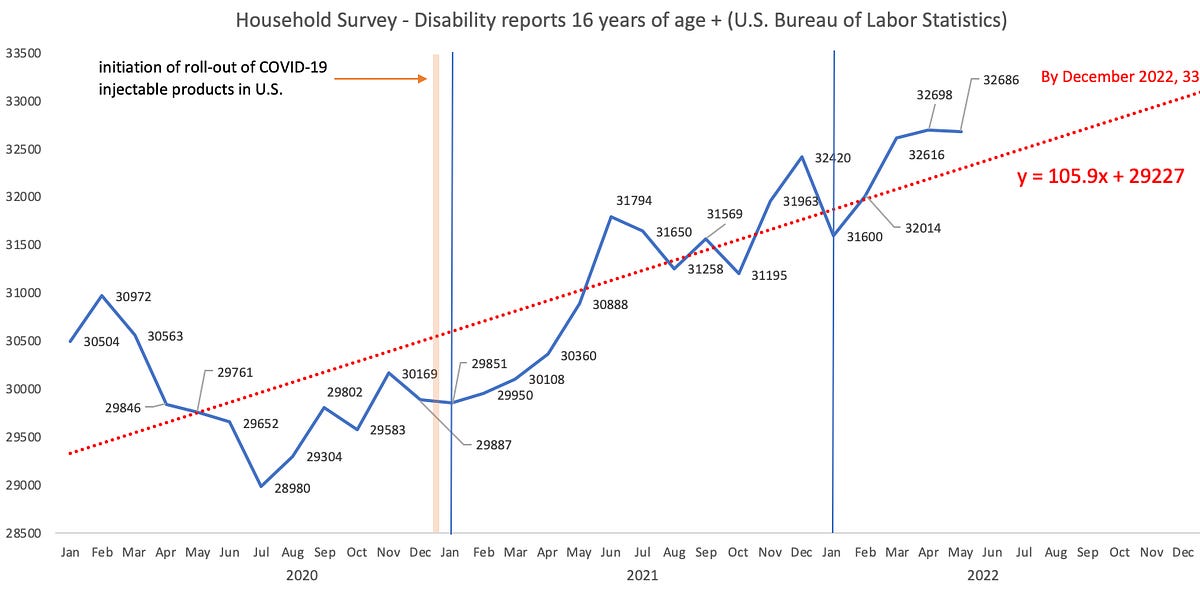
Disability claims - U.S. Bureau of Labor Statistics vs. VAERS
A quick and dirty analysis.
 jessicar.substack.com
jessicar.substack.com
Disability claims - U.S. Bureau of Labor Statistics vs. VAERS
A quick and dirty analysis.
Jessica Rose
21 hr ago
Note: I started this the other day but got distracted.
I was on a call the other night with PANDA and Edward Dowd spoke. He spoke on new data concerning disability claims.
This is a category in VAERS that I have been tracking for a long time now. According to sources, 2.9 million additional disability reports that came from household survey data have been reported since the injection roll-out. El Gato Malo wrote a great piece on this that you can read here.
There’s a graph that I can share from that post for U.S. citizens 16 years and older that will make it easy to see that there’s something ‘different’ about 2021 with regard to disability claims.
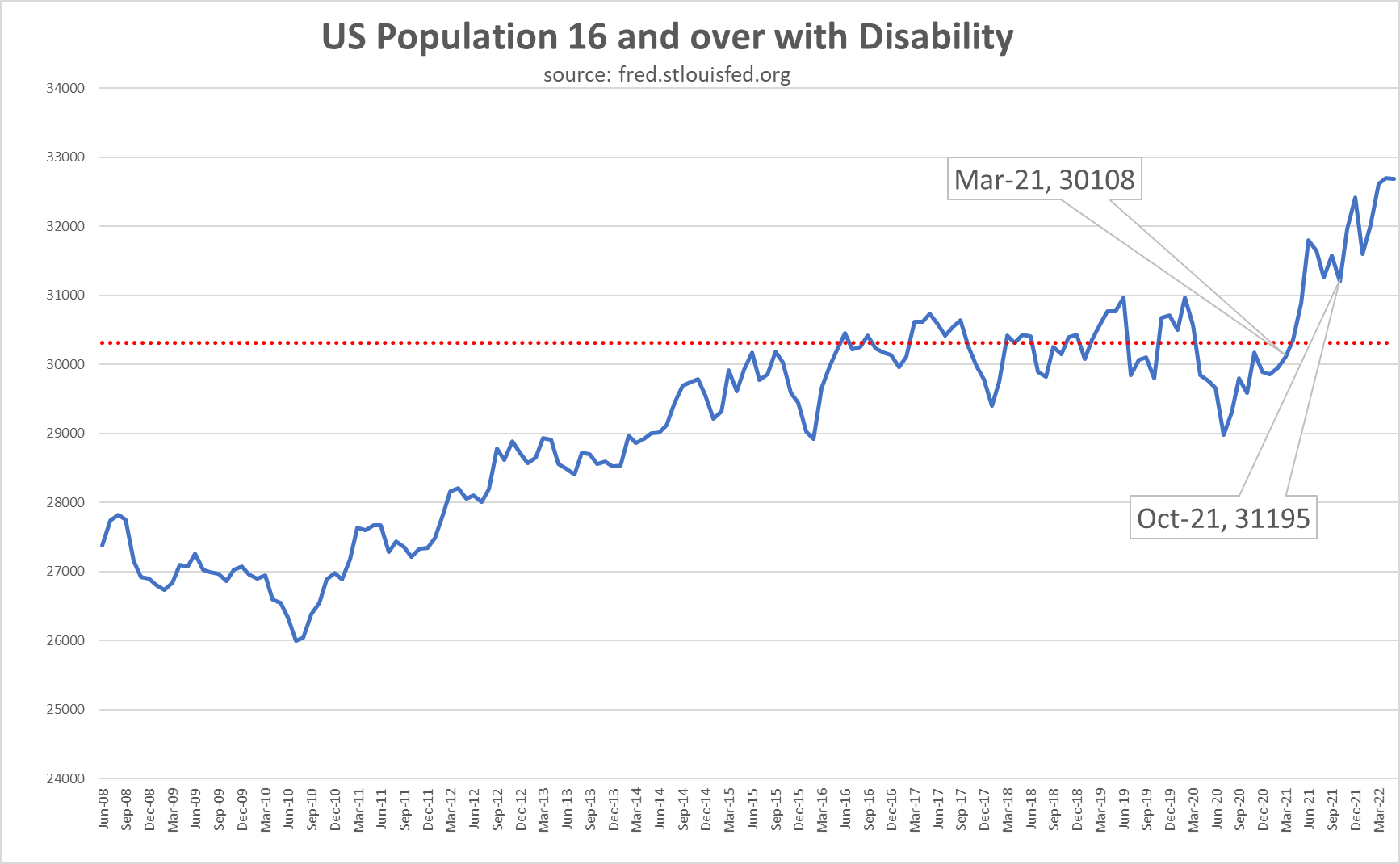
Figure 1: boriquagato.substack.com/p/do-vaccine-rollouts-correlate-to?s=r
The data comes from the U.S. Bureau of Labor Statistics and collected using household surveys.
Household surveys are questionnaires that are given to a sample of households in a population. Their primary advantage is to provide considerable discretion to the interviewer about the information requested of respondents. Their major drawbacks are that information provided by the respondent is often inaccurate (response error), and, in many cases, the information requested is not provided at all (nonresponse problems).1
I always like to reproduce charts and results from original data sources so I did and I added a linear trend line. It’s really just a linear model that allows one to ‘forecast forward’ to guess what the future might bring if the trend continues. The slope is very positive and if the trend does continue, there is an anticipated 10.5% increase in disability claims (since the injection roll-out) and 10.3% above the average for 2020. There’s no way to know for sure if this trend will continue, however, but I would bet that the slope of this line might even increase.
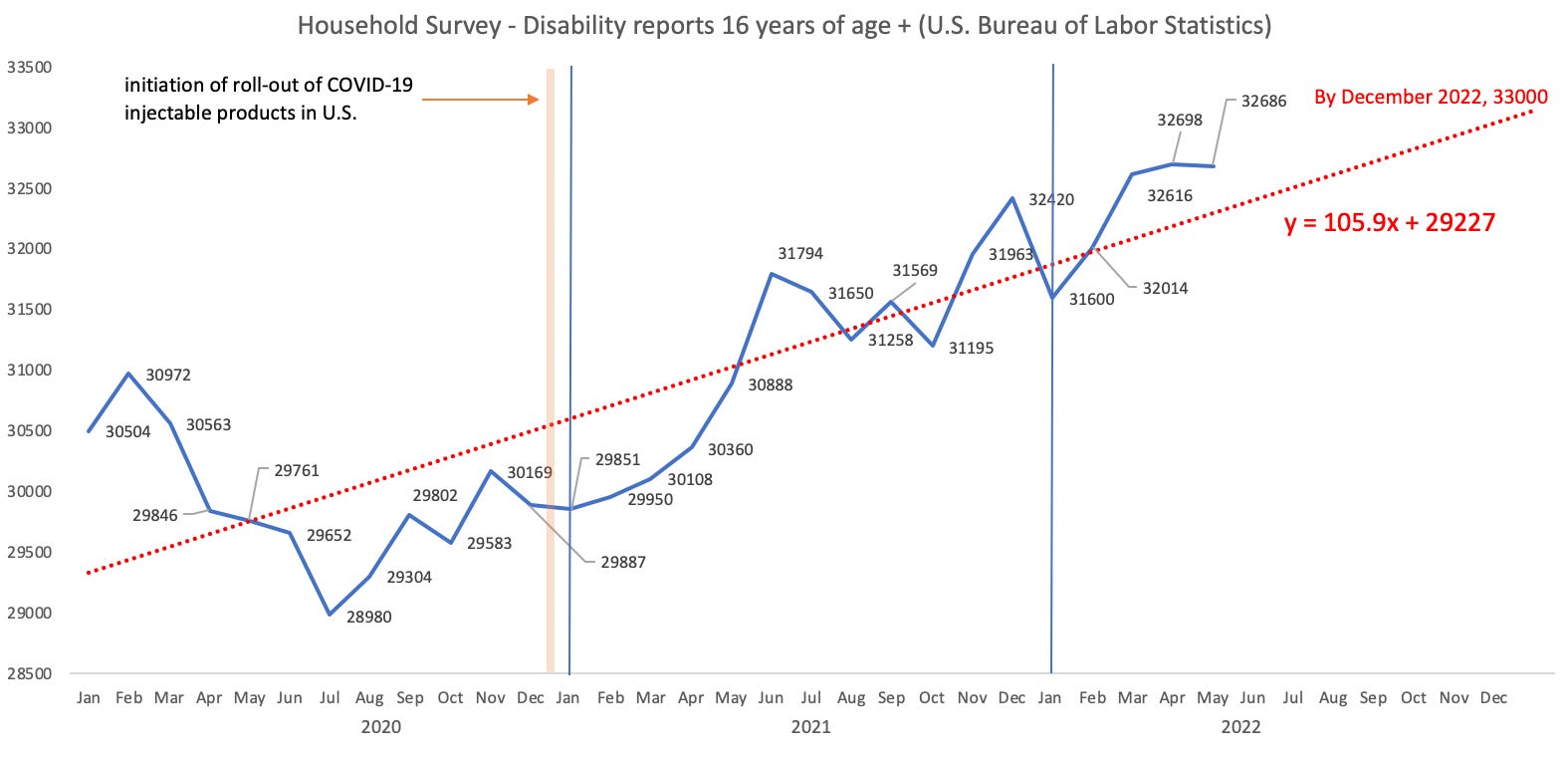
Figure 2: Disability reports collected via household survey for individuals 16 years of age and older (Units: thousands of persons per month not seasonally adjusted).
So it seems from this reliable data set that there is an unexplained rise in disability claims in 2021 that continues into 2022. The means for 2020, 2021 and 2022 up until May are 29,918,583, 31,083,833 and 32,322,800. This ‘means’ (hardy har) that we are 3.9% and 8% above the average for 2020 in 2021 and 2022. Why?
In the meeting, there was mention of a skewed distribution of disability data when stratifying by gender. Apparently, more reports from females with disabilities were being filed. I imagine since this is household survey data that this means that more females are actually suffering rather than just simply filing disability claims. This is likely due to longer lifespan and degeneration of ability with age.
So I checked VAERS as a means to confirm this mention. Sure enough, there were almost twice the number of disability reports from females. The average age of the females reporting is 48 and for males, 52. The rate of reporting of adverse events to VAERS is higher for females (65.4% (F); 32.1% (M); 2.5% (U)), so this likely why we see more disability reports in VAERS from females. There are 793,195 reports in VAERS made by females and 389,082 made by males so the ratio is 2:1 which is comparable to the ratio of disability reports 32,693 (F) and 17,034 (M) at 1.9:1 so all I can really say about disability reports and gender skewing is that there are twice as many REPORTS made by females. I can’t really say anything about whether or not there are more incidents.
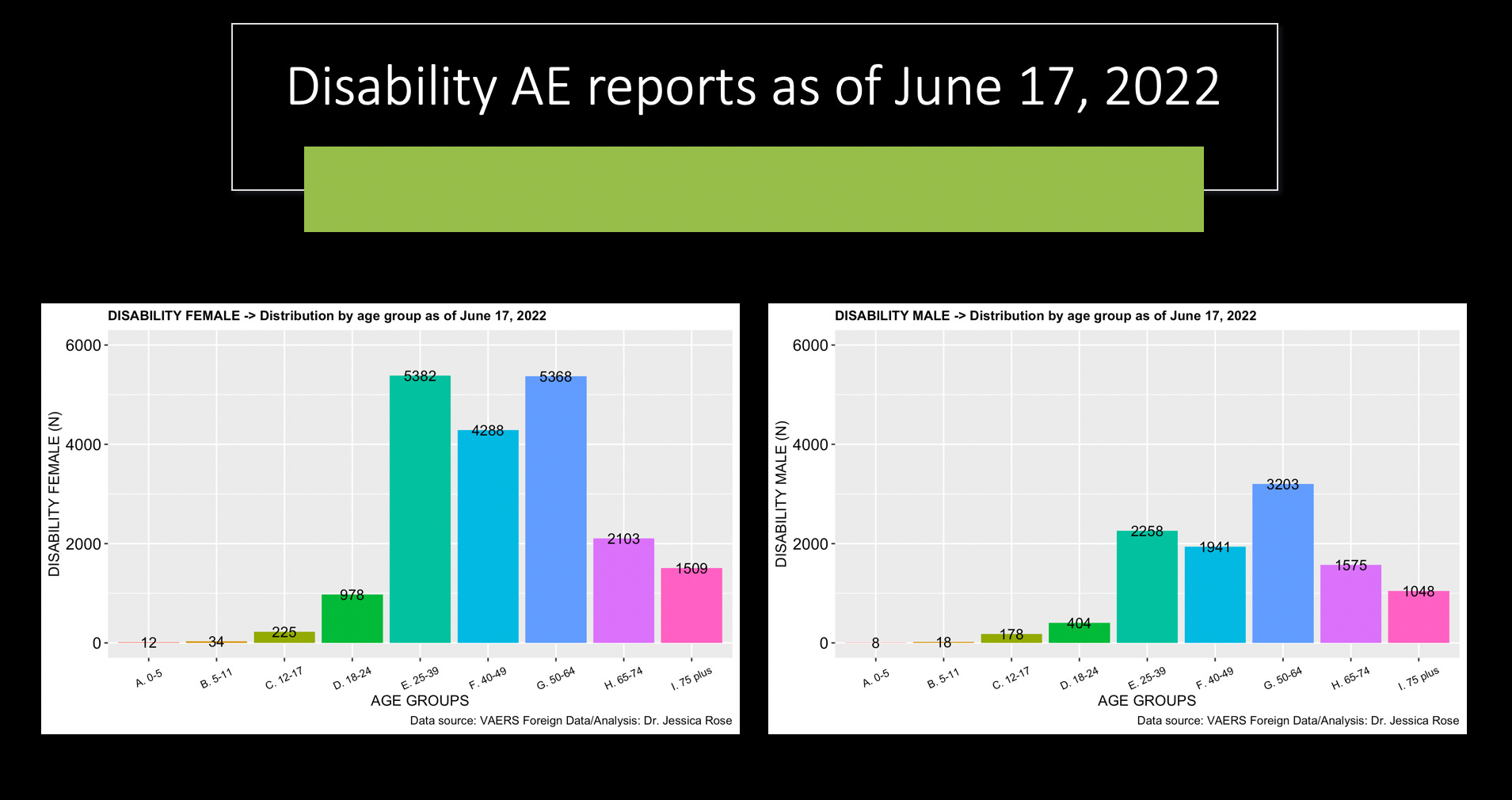
Figure 2: Disability reports filed in VAERS as of June 17, 2022.
I also plotted the data in a single bar plot so everyone could visualize this way if that’s better. Notice that we lose ~20,000 data points from missing field entries in the age and gender variables.
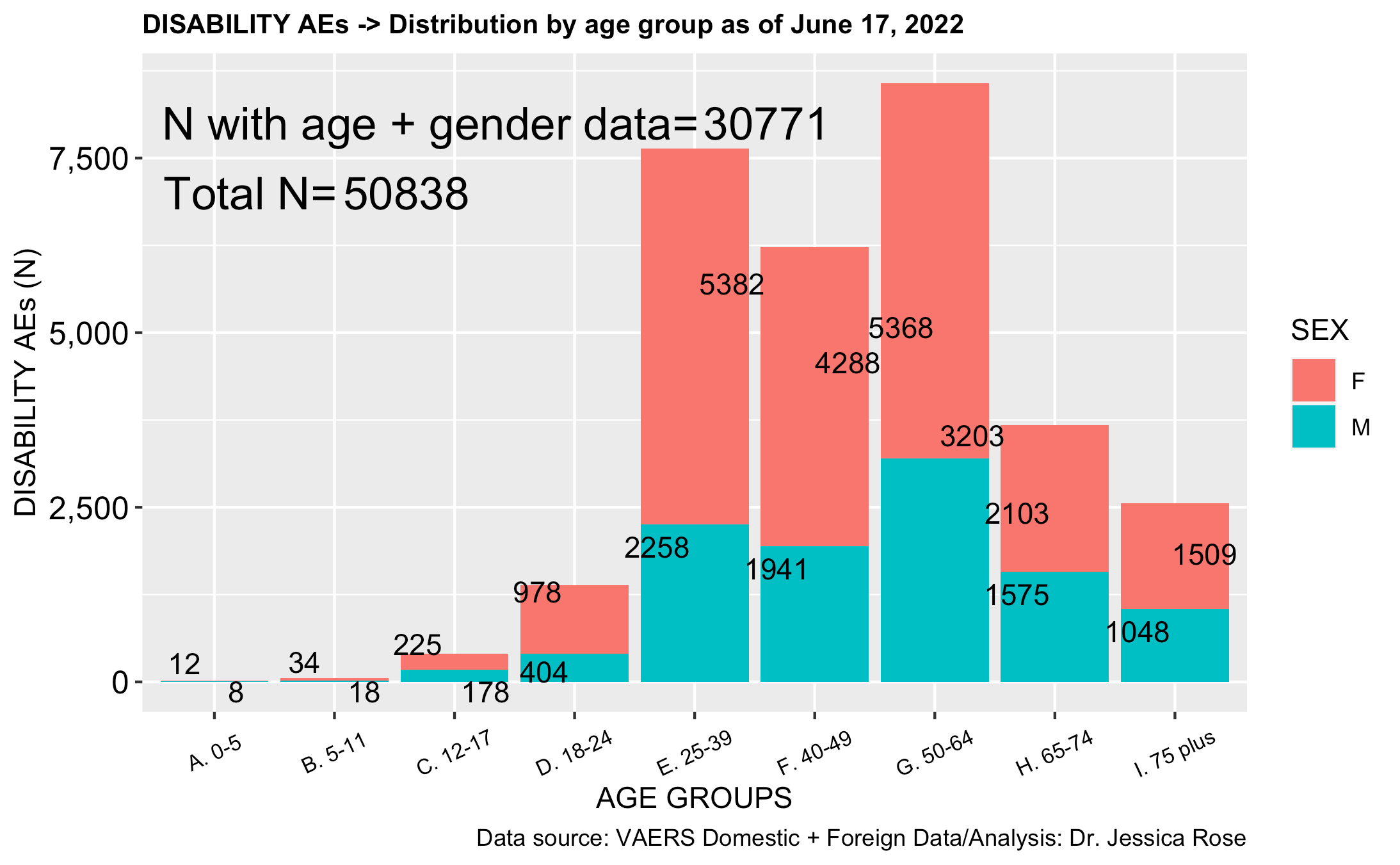
Figure 3: Disability reports field to VAERS as of June 10, 2022 stratified by age and labelled according to gender. Many data points are lost due to missing gender and age data.
This made me wonder if there was a way I could find out using VAERS data if any disabilities were being specifically reported to VAERS by females and not males. I mean, besides bleeding/menstrual disorders. I realize that there’s no real way to ascertain this definitively without background rates, but it might provide insight.

Figure 4: Bar plot showing the percentage of disability-associated select adverse events according to females and males.
So there’s not much to say here on the subject of determining whether or not females are suffering more disability. These 13 stand-alone adverse events were selected randomly and only a couple (Bell’s palsy, Cardiovascular accident and Unilateral blindness) indicate that the men might be suffering more than women from these conditions. But, there’s no real way to know from this data. Females reported 1933 different types of adverse events while males reported 1,576 in the context of disability reports in VAERS. Many were menstrual disorders. Of the total types, 508 were reported for males that were not reported by females, and 865 were reported by females and not males. Below is a table showing the top 10 adverse event types reported for males (left) and females (right). Note the discrepancies in the absolute counts.
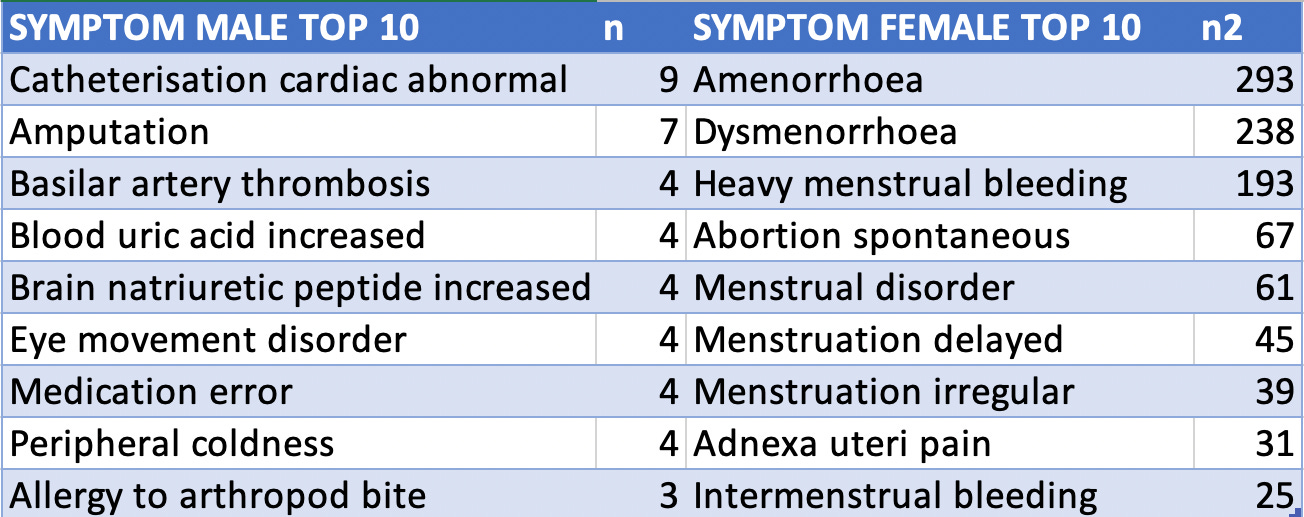
Figure 5: Top 10 adverse event reports associated with Disability for males (left) and females (right). These represent adverse events not reported in the other gender.
Just in case you’re wondering what kinds of adverse events are associated with disability as per gender, I made the following plots. Sorry for the small font.
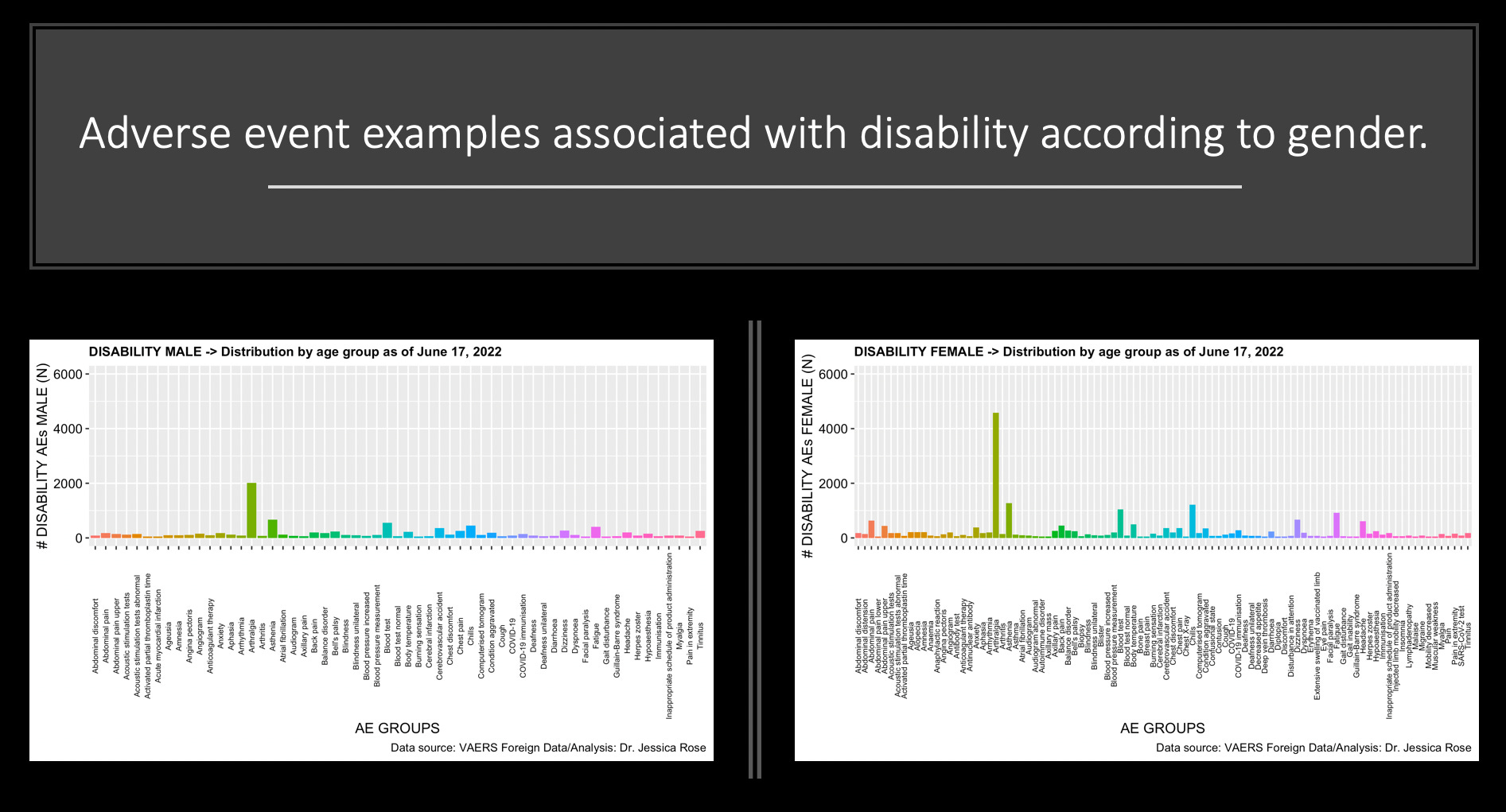
Figure 6: Adverse event reports associated with Disability for males (left) and females (right). These represent adverse events not reported in the other gender.
Demographic characteristics In 2021, persons with a disability accounted for 11.9 percent of the civilian non-institutional population. Persons with a disability tend to be older than persons with no disability, reflecting the increased incidence of disability with age. In 2021, half of persons with a disability were age 65 and over, compared with 18 percent of those with no disability. Overall, women were somewhat more likely to have a disability than men, partly reflecting the greater life expectancy of women.
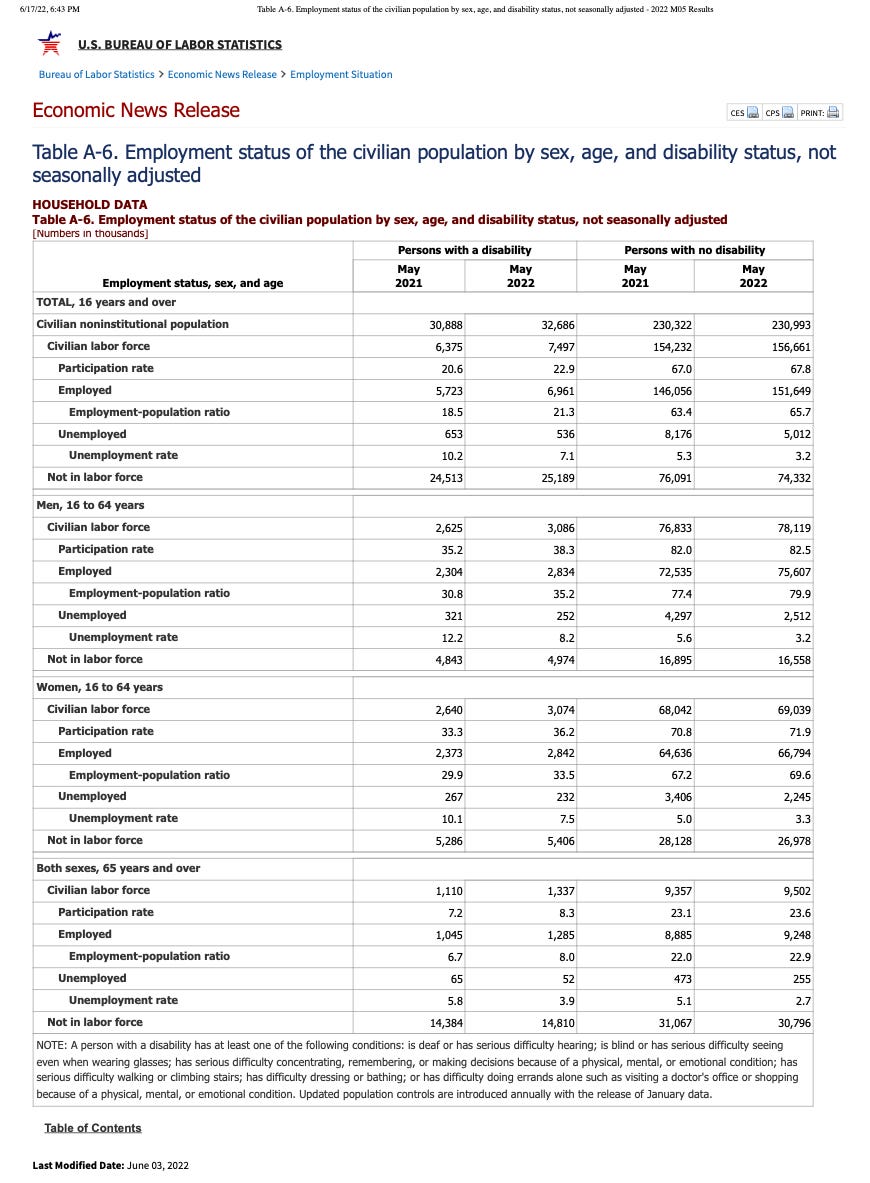
I’m going to post this article and come back to it.
") Hopefully. I am far too into the amyloidogenicity potential of spike peptides now to focus properly on anything else.
Hopefully. I am far too into the amyloidogenicity potential of spike peptides now to focus properly on anything else.1 https://www.sciencedirect.com/topics/social-sciences/household-survey
Heliobas Disciple
TB Fanatic
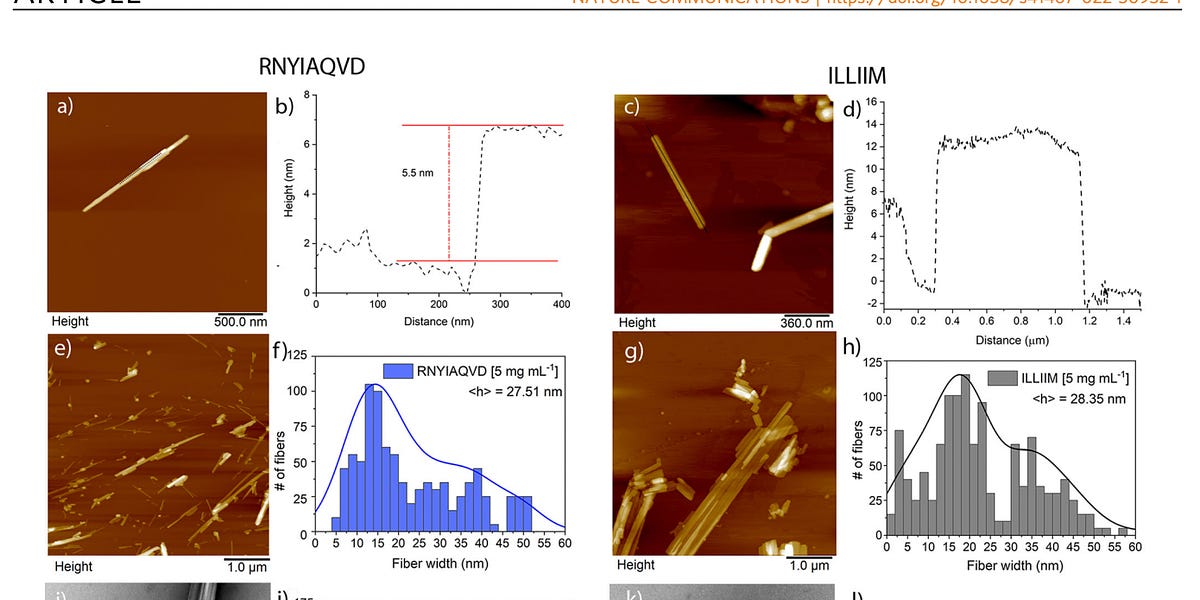
An incredible paper was just published (thank you David Wiseman for the heads up)
It's incredible in terrifying ways.
jessicar.substack.com
An incredible paper was just published (thank you David Wiseman for the heads up)
It's incredible in terrifying ways.
Jessica Rose
Jun 18
Please read this paper entitled: “Neurotoxic amyloidogenic peptides in the proteome of SARS-COV2: potential implications for neurological symptoms in COVID-19”. It was published in Nature Communications on June 13, 2022.1
The bottom line of this incredible work is that there are two amyloidogenic proteins in the Open Reading Frames (ORF) 6 and 10 from SARS-nCoV-2 (the ORF-10 one does not have a homologue in SARS-nCoV - that means it’s unique to SARS-nCoV-2), that form crystalline amyloid structures independently, and together, at room temperature!, very quickly, and that these structures induce programmed cell death in neural cells.
Before I unpack this article, I want to say something. I think this was able to be published in this prestigious journal for 2 reasons: 1. this is about COVID-19 (SARS-nCoV-2) and 2. this is about the ORFs and NOT the spike protein amyloidogenic peptides.
Before I start, here’s the genome of SARS-nCoV-2 and some information on the ORF-6 2 3 4 which is a highly pathogenic protein in and of itself.5

Modeling of the SARS-COV-2 Genome using I-TASSER. zhanglab.dcmb.med.umich.edu
Let’s start. These amazing people did the same kind of thing as described in this paper that I described here. To briefly summarize, they used amyloid prediction algorithms (TANGO) and other bioinformatics tools (ZIPPER) to provide choices of residue windows of specific lengths. They found 2 contender amyloidogenic peptides that reside in the SARS-nCoV-2 ORFs 6 and 10: ILLIIM and RNYIAQVD, respectively. These were the two that they decided to synthesize and study because of their predicted amyloidogeneticity potential.
Amyloid aggregation prediction algorithms identified two short peptides from ORF6 and ORF10 that are likely to form amyloids.
My readers know all too well by now (because you’re amazing), that amyloid proteins are really beta-sheet rich. Below is Figure 1 from the paper which shows where the peptides reside in the respective ORFs (ORF-6 and ORF-10) and their beta sheet propensities.
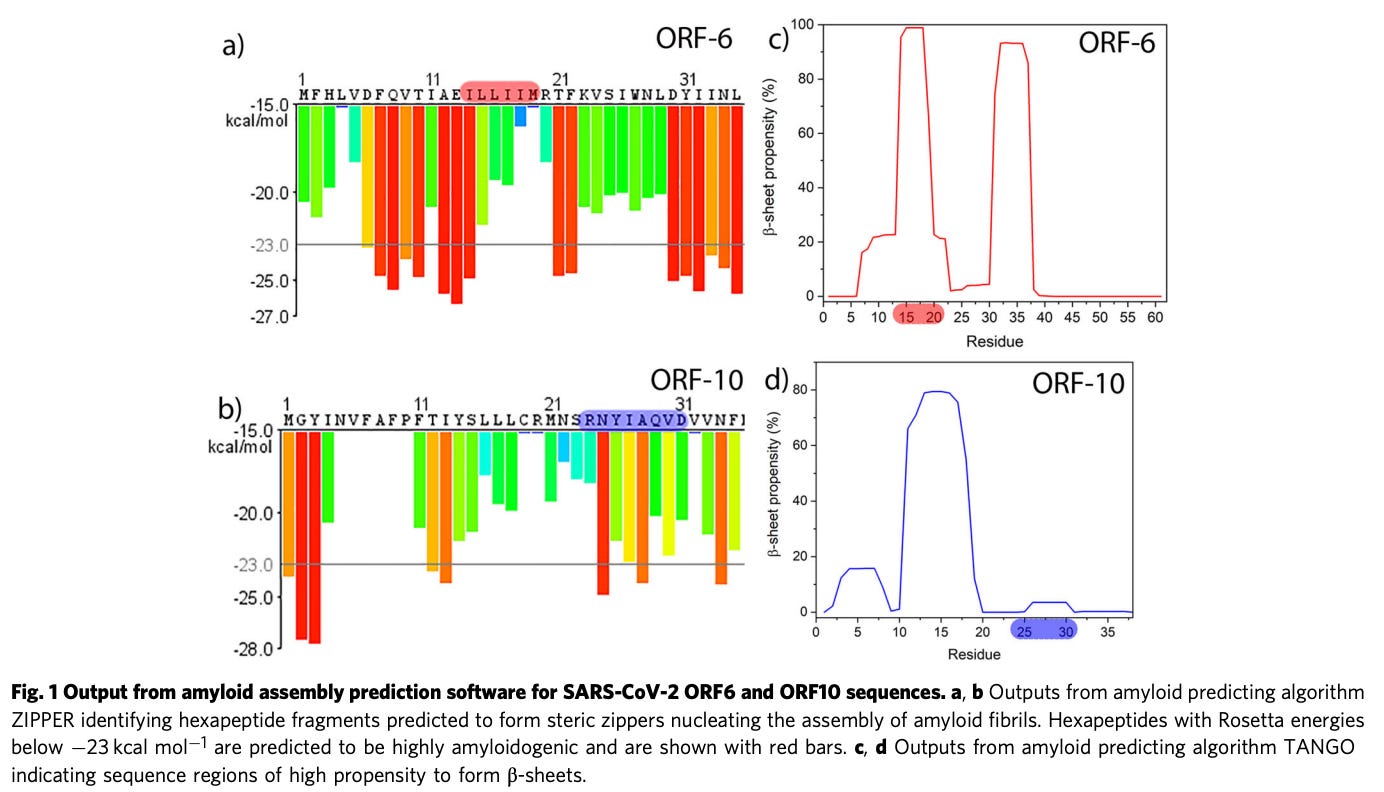
Nanoscale imaging reveals both peptide sequences self assemble into polymorphic amyloid assemblies.
Two things struck me about the conditions under which the structures assembled: assembly happened at room temperature and it happened immediately.
Atomic force microscopy (AFM) imaging of the two peptide assemblies revealed that both peptides assembled at 37 °C almost immediately at 1 mg mL−1 (Supplementary Figs. 1 and 2) into a highly polymorphic mixture of nanofibrous and crystalline structures.
Aren’t those images incredible! The needle-like structures that each peptide formed independently were slightly different whereby:
ILLIIM tends to form very large (2–3 μm in width) multi-laminar crystalline assemblies (Fig. 2g), whereas RNYIAQVD predominantly forms long linear needle-like structures.
Another thing that struck me about what they found was these peptides that assemble into these structures ‘tend[ed] to stack on top of each other forming multi-laminar structures’.
The authors used all sorts of techniques such as “X-ray scattering, spectroscopic characterization, fluorescent microscopy and molecular modeling confirm the amyloid nature of the assemblies”.
In light of these incredible findings, there still may not be an effect in vivo or in the living organisms like humans. They hypothesized toxicity to human neurons and investigated this hypothesis using a human cell line called SH-SY5Y exposed to both ILLIIM and RNYIAQVD. They found that ILLIIM and RNYIAQVD triggered late-stage apoptosis in the cells (programmed cell death) where ILLIIM did so prominently as very low concentrations (0.04 mg mL−1 vs 0.15 mg mL−1 for ILLIIM and RNYIAQVD, respectively.
Summary: Two peptides from ORF-6 and ORF-10 of SARS-nCoV-2 induce apoptosis in human neural cells.
They subsequently conclude that this be what’s causing all the neurological problems associated with COVID-19.
The cytotoxicity and protease-resistant structure of these assemblies may result in their persistent presence in the CNS of patients post-infection that could partially explain the lasting neurological symptoms of COVID-19.
I know what you’re thinking.
Let’s ask the three questions of our lifetimes, shall we?
Question 1: Are amyloidogenic peptides residing in the SARS-nCoV-2 spike protein and are they capable of inducing apoptosis in neural cells and/or other cells types?
Question 2: Since the modified spike proteins, used to construct the LNP-encased payload in the Moderna and Pfizer injectable biological products, are derived from the SARS-nCoV-2 spike, do these proposed amyloidogenic properties carry over?
Question 3: If the modified spike protein in the COVID-19 injectable products contain amyloidogenic peptides capable of assembling into amyloid structures, is this why we are seeing such systemic neurological, hepatological, cardiovascular and reproductive damages with regard to adverse event reports in databases such as VAERS, Eudra and Yellowcard?
1 Charnley, M., Islam, S., Bindra, G.K. et al. Neurotoxic amyloidogenic peptides in the proteome of SARS-COV2: potential implications for neurological symptoms in COVID-19. Nat Commun 13, 3387 (2022). Neurotoxic amyloidogenic peptides in the proteome of SARS-COV2: potential implications for neurological symptoms in COVID-19 - Nature Communications.
2 Baric Ralph A. et al., Severe Acute Respiratory Syndrome Coronavirus Open Reading Frame (ORF) 3b, ORF 6, and Nucleocapsid Proteins Function as Interferon Antagonists. Journal of Virology. 2007. Vol. 81, No.2 https://journals.asm.org/doi/10.1128/jvi.01782-06?permanently=true.
3 Lei, X., Dong, X., Ma, R. et al. Activation and evasion of type I interferon responses by SARS-CoV-2. Nat Commun 11, 3810 (2020). https://doi.org/10.1038/s41467-020-17665-9.
4 Lee, JG., Huang, W., Lee, H. et al. Characterization of SARS-CoV-2 proteins reveals Orf6 pathogenicity, subcellular localization, host interactions and attenuation by Selinexor. Cell Biosci 11, 58 (2021). Characterization of SARS-CoV-2 proteins reveals Orf6 pathogenicity, subcellular localization, host interactions and attenuation by Selinexor - Cell & Bioscience.
5 Nasim Kheshtchin, Parisa Bakhshi, Samaneh Arab, Maryam Nourizadeh, Immunoediting in SARS-CoV-2: Mutual relationship between the virus and the host, International Immunopharmacology, 105, (108531), (2022).
naegling62
Veteran Member
I think it needed the caption " and Jesus wept" to clarify things.Don't know who that is but they need to put there big girl panties on.
psychgirl
Has No Life - Lives on TB
Thank you for doing so. I was a little horrified by that members comment, actually.I think it needed the caption " and Jesus wept" to clarify things.
But I suppose anyone could make such an error if in a hurry.
Craftypatches
Veteran Member
I’m going shortly to a minute clinic to get tested again. It wasn’t paxlovid. I waited 5 days and was symptom free as my daughter and grandkids were here. They said I would no longer be contagious. I am fully vaccinated/boosted and was taking the vitamins. The night before it returned we had terrible storms so I didn’t sleep well. Then I got up early to have a garage sale with my daughter. About 3 pm at the garage sale I got extreme fatigue just like before and my nose started gushing like I had to use paper towels, Kleenexes didn’t even work. Went to bed and they left. I told them better get away from me. I tested at home that evening and was positive. Back to having a scratchy throat and some coughing and runny nose and headache. Exactly as before! I think they don’t know everything about this virus and they are rushing it too much to say you can’t give it if you are symptom free! That’s what I think! Thanks for your prayers! I just never heard of it returning but obviously my immunity was down. And I didn’t want all those shots but my friends insist on it. I looked up what the name of the med was they gave me and it was called molnupiravir 200 mg. I received the meds June 9th and started taking then right away. By Friday I was sick again. I probably infected people at the garage sale when I thought I was symptom free!Are you feeling sick again or did you just test positive again? And did you test negative before you just tested positive? Could just be a testing issue - false positive now - or - false negative before and you're just taking longer to fully clear the virus from showing up on the test. Try testing again and see what comes up.
If you're actually sick again, I don't know the answer to your question. It can recur, and it makes sense if your immune system is weak that you'd be more vulnerable, but it may just be that you were exposed again. I'm surprised however that your immunity from a few weeks earlier didn't protect you. By any chance did you take paxlovid? There is a known rebound from it - you feel better while you take it and then a few days after you stop, you get sick again. So if you took it, this is not unexpected. If you didn't - I'm at a loss. Also, if your comfortable answering - are you vaccinated/boosted? that may play a role as well.
Are you taking any vitamins or other supplements? There have been a lot of posts on this thread and on TB in general about Vitamin D, Vitamin C, Zinc, Quericitin and then the prescription anti-virals. Of course, you should only take something if it's not going to interfere with other medications you may be taking or if you have allergies,etc. Only you and your doctor would know that.
Feel better, I will add my prayers for you to have a quick recovery if indeed you are sick again.
HD
Last edited:
Zoner
Veteran Member
Two important interviews in this tweet
Rumble link: Steve Bannon's War Room Radio Special Episode1,233
YouTube link to Geert/Weinstein interview
View: https://youtu.be/NY9Wrpw3igs
View: https://twitter.com/curlsgreeneyes9/status/1538598043334983682?s=21&t=wQp6LXwrYqNBHRAvFxs-Zg
Rumble link: Steve Bannon's War Room Radio Special Episode1,233
YouTube link to Geert/Weinstein interview
View: https://twitter.com/curlsgreeneyes9/status/1538598043334983682?s=21&t=wQp6LXwrYqNBHRAvFxs-Zg
Last edited:
Craftypatches
Veteran Member
I found out the molnupiravir made my Merck is called an antiviral but it doesn’t kill the virus at all. It is also a rebound drug meaning some people get the Covid back after finishing it. All it does is mask the symptoms until your body fights it off. If you still have it after taking the medicine, it goes full scale back to like you were at the beginning of the virus, How can they call this an antiviral drug? They even said don’t tell this to people as they don’t really want people to know! So isolate 5 days and 5 days after that wear a mask.I’m going shortly to a minute clinic to get tested again. It wasn’t paxlovid. I waited 5 days and was symptom free as my daughter and grandkids were here. They said I would no longer be contagious. I am fully vaccinated/boosted and was taking the vitamins. The night before it returned we had terrible storms so I didn’t sleep well. Then I got up early to have a garage sale with my daughter. About 3 pm at the garage sale I got extreme fatigue just like before and my nose started gushing like I had to use paper towels, Kleenexes didn’t even work. Went to bed and they left. I told them better get away from me. I tested at home that evening and was positive. Back to having a scratchy throat and some coughing and runny nose and headache. Exactly as before! I think they don’t know everything about this virus and they are rushing it too much to say you can’t give it if you are symptom free! That’s what I think! Thanks for your prayers! I just never heard of it returning but obviously my immunity was down. And I didn’t want all those shots but my friends insist on it. I looked up what the name of the med was they gave me and it was called molnupiravir 200 mg. I received the meds June 9th and started taking then right away. By Friday I was sick again. I probably infected people at the garage sale when I thought I was symptom free!