The Price of Saving a Life: Naloxone's Cost Barrier in the US (filtermag.org)
The Price of Saving a Life: Naloxone’s Cost Barrier in the US
When I walk into my local pharmacy to pick up a naloxone kit, I don’t need to present a prescription. I don’t even need to state my reason for needing naloxone (I’m an opioid-dependent pain patient and I frequently interview people who use illicit opioids). The pharmacist asks whether I prefer the nasal spray or the injectable version, then takes me through a five-minute orientation, explaining how to use it to save someone else’s life. Then I leave with my kit.
No money changes hands. I owe nothing. My choice of injectable versus nasal spray is driven by my own comfort, not by their respective costs.
I live in Toronto. But in the United States, where the crisis of opioid-involved overdose deaths is raging (as it is in Canada) beyond anything we’ve seen before,
naloxone access is limited—not just by stigma and outdated, restrictive laws, but also by its rising cost.
The access issue is common to most countries. The cost barrier, however, is somewhat specific to the US, with
an average out of pocket cost of $31.01 in 2018. A single dose of generic naloxone in the European Union costs the equivalent of around $3.
Various ways to remedy this are proposed—some of them innovative, and ranging from market-based approaches to government-led ones. International examples show that the US could do better, but experts are skeptical about whether it will.
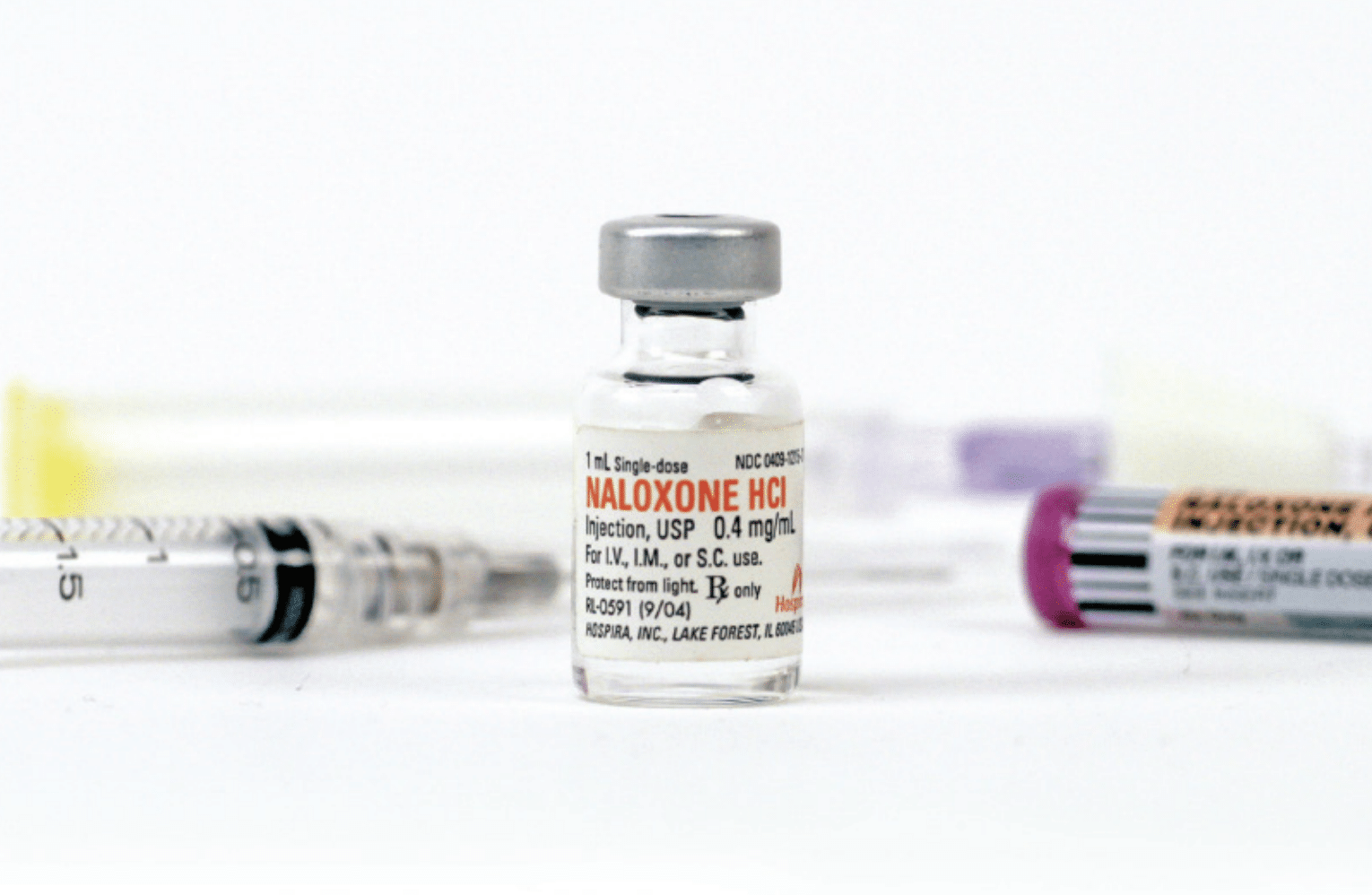
Naloxone is not a new drug. It was first patented in 1961 as a medication to reverse the common side effect of constipation in patients prescribed opioids, but was approved by the Food and Drug Administration for overdose reversal in 1971. The original patent expired long ago, so today the generic version only costs around $20. But new delivery systems—like the auto-injector and the nasal spray—have allowed for new patents, of which there are currently seven, with the auto-injector and nasal spray not due to expire
until 2035. In effect, companies are now charging for the delivery system, not the drug itself.
Narcan is the brand name for nasal spray naloxone. By contrast, injectable naloxone is administered by first filling a syringe from a small vial and then injecting that into the muscle of the thigh or shoulder. The injectable form is the cheapest, because it’s not covered by patent. Then there’s the auto-injector, Evzio, which you administer through an EpiPen-like delivery system.
No Standard Access
There is no standard way of acquiring naloxone in the US. Across the country, different people and organizations do so in different ways.
In San Francisco, the National Harm Reduction Coalition’s DOPE Project (Drug Overdose Prevention and Education) provides free injectable and nasal spray naloxone to people who use drugs. For the former, it relies on a deal painstakingly arranged by unpaid harm reductionists working with the pharmaceutical company Pfizer, which owns Hospira, the makers of injectable naloxone hydrochloride. This “ensures access to injectable doses of Pfizer for a cost I can’t disclose,” said DOPE Project manager Kristen Marshall. “That is the way historically anything has to get done when you are representing people outside the mainstream.”
The DOPE Project gets its Narcan, meanwhile, through a state-funded naloxone distribution program. “There’s no way we’d be able to afford that [without the program]. The fact that not every state has that kind of access is a problem,” Marshall said. “In places
like West Virginia, where we’re seeing the highest rates of
overdose deaths and
HIV, that’s not available.”
Like harm reductionists elsewhere, she sees access to the nasal spray as vital. At a time when many people are smoking fentanyl and overdosing
without ever having used a syringe, syringe-based naloxone can pose a barrier. She also noted that many venues—jails, libraries, hotels—are unwilling to keep syringes on hand.
“It’s infuriating how these resources go to the carceral system.”
NEXT Distro, a New York City-based organization that
distributes harm reduction supplies, gets its expired naloxone from the sources that actually have funding, often through large state grants, to purchase it: fire departments, police departments, jails, clinics, hospitals, security companies and certain community-based organizations.
“[Federal and state] grants are prioritizing funding for inefficient systems that are not suited to the needs of people who use drugs,” said Jamie Favaro, NEXT Distro’s executive director. “It’s infuriating how these resources go to the carceral system.”
So Favaro makes it easy for staff at fire departments or jails to find NEXT Distro online when they search for places to donate naloxone that inevitably expires unused. They recently received 800 doses (from a source she preferred not to reveal), which NEXT Distro is now pumping out to secondary suppliers—harm reduction organizations, often in southern states where naloxone is difficult to access (they try to redistribute the supply in the same state from which it was donated). But it’s often a “feast or famine” situation, in that they can’t rely on a steady supply of the expired naloxone that powers their work.
In her 2020 book,
OD: Naloxone and the Politics of Overdose, author and academic Nancy Campbell argues that the struggle for expansion of naloxone access fueled the harm reduction movement, turning overdose from a death sentence into an opportunity to fight for change. Building on the revolutionary zeal that animated advocacy for syringe access and blood-borne disease prevention, the fight for naloxone access became a fight to put lifesaving technology in the hands of the people best positioned to use it.
“It’s not just a technology,” Campbell told
Filter. The story of naloxone is “laden with people.”
.....snip/ more at the link

")