On the morning of Jan. 15, 2022, Debbie Botzum-Pearman, who had been a strong healthy woman for 66 ...

www.theepochtimes.com
(fair use applies)
Spike Protein From Infection and Vaccines Contributing to Autoimmune Diseases, Studies Suggest
BY Marina Zhang
September 19, 2022
On the morning of Jan. 15, 2022, Debbie Botzum-Pearman, who had been a strong healthy woman for 66 years, woke up paralyzed from the chest down.
On Sept. 13, 2022, nearly nine months later, she managed to stand up without assistance for 10 seconds. Since then, she has made a steady recovery. She has regained sensation in her thighs and taken her first steps with a walker. But, a long journey remains ahead of her.
Debbie’s symptoms appeared less than a month after her first Pfizer COVID-19 booster shot. She had taken the shot in mid-December and felt fine, the same as with her previous COVID-19 shots.
Looking back now, Debbie realized that leading up to her sudden paralysis, she had been feeling that her bra was getting too tight. This sensation is also called MS (multiple sclerosis) hug, and some people can experience these symptoms even without MS.
The first dominoes toppled on Jan. 14. She was finishing her painting work at her friend’s house when she realized that she could not pee despite having the urge to urinate.
“I was drinking water … could not pee, just could not pee,” she told The Epoch Times.
She got home that day and as she was walking up the stairs, her left leg gave out and she peed over herself.
She went to bed and on the following morning, Debbie was paralyzed from the chest down and rushed to urgent care.
“I probably had 15 MRIs and a spinal tap [at the hospital] … they came back [a few days later] with neuromyelitis [optica],” Debbie said.
“[Neuromyelitis] ate away, I don’t know, four or five inches [of my spinal cord on the MRI], which is repairing itself now.”
Neuromyelitis, scientifically known as neuromyelitis optica (NMO), is a rare condition affecting around 1 to 2 people out of 100,000 every year. The condition destroys the nerves in the central nervous system and the eyes, and can cause paralysis, weakness, and even blindness if not treated.
Onset of NMO is usually precipitated by a viral or bacterial infection such as Epstein-Barr virus (EBV) or bacterial meningitis. It primarily appears during childhood as well as in women in their 30s and 40s. Risk factors include smoking and having a family history of autoimmune disease.
However, apart from her sex, Debbie did not have any of these risk factors.
Neuromyelitis is mostly unheard of, often overshadowed by and misdiagnosed as the more well known MS, which is another, distinct disease.
Fortunately for Debbie, her doctor was competent and had excellent clinical judgment. Even before the tests and diagnosis returned, he ruled that Debbie was experiencing NMO. Her doctor also allegedly concluded that the booster shot from a month ago was the cause.
The Epoch Times could not verify the identity of the doctor nor his statement, but Debbie and her stepson, Jared Pearman, expressed that the anonymous doctor’s statements were what drove their suspicions that her illness was vaccine induced.
Debbie recalled it was probably the day she was admitted, “[the doctor] came in, shut the door and asked if I had the booster. I didn’t mention [that I had the booster] and he’s the one who declared that it was from the vaccine,” she said.
Debbie was put on a blood purifying machine (plasmapheresis) which cycled out the plasma from her blood to remove autoantibodies that were attacking her own nerves.
Debbie was in the hospital for a week, and she recalled that pretty much every day she was having blood treatments.
Both Debbie and Jared have nothing but gratitude for the doctor; they are convinced that if it was not for the doctor’s quick judgment, Debbie would have fared a lot worse. However, the doctor allegedly told Debbie that he could not make his diagnosis known in the hospital, lest he get fired.
“One of the things that really strikes us is how disincentivized everyone in the medical community is of discussing and analyzing adverse effects to the vaccine … [the doctor] had to secretly acknowledge that [the vaccine] was what caused her symptoms in order to save her life,” said Jared.
“I understand that there [may be] 1 in a million [chance of getting certain adverse effects], that 1 in a million is a real person who has a real life that gets ruined, and sometimes that’s your card.”
Spike Protein and Autoimmunity
Debbie is in no way an isolated case. Since the rollout of the COVID-19 mRNA and DNA injections, reports of neuromyelitis, multiple sclerosis, Guillain-Barre syndrome, rheumatoid arthritis, shingles, lupus, diabetes, and many other autoimmune conditions have either suddenly appeared, or relapsed, often with worsened symptoms.
Autoimmunity is a health condition where the body’s immune system becomes confused and unable to differentiate between self and non-self and attacks its own tissues.
The development of autoimmunity is believed to be a result of the interactions of both genetic and environmental factors. Certain autoimmune diseases tend to cluster in families, such as rheumatoid arthritis, Hashimoto’s thyroiditis, and lupus.
Although genetics plays a role, the development of autoimmunity also depends on environmental exposures to infections and toxins as well as lifestyle, nutritional health, and various metabolic and detoxification processes.
In the case of COVID-19 and its vaccines, many studies since the start of the pandemic have shown that the spike protein shares similarities with human proteins both in its structure and in its basic chemical sequence.
This means the spike protein can increase the risk of developing autoimmunity and implies that the mRNA and DNA vaccines, which cause the body to make large amounts of spike protein, would do the same.
“If the spike protein from SARS-CoV-2 contribute to autoimmunity, then why not spike protein from the vaccine? It seems that somehow when we get to that point, the scientists and many people try to keep their distance,” said Dr. Aristo Vojdani, head of Immunosciences Lab and a pioneer in the field of clinical immunology.
Cross Reactivity Hypothesis
A recent study published by Florida International University concluded that this is possible after comparing COVID-19 spike protein sequences to structures of both human and animal proteins.
The authors found that human proteins had the most sequence sets that were the same as spike proteins with 627 regions in common.
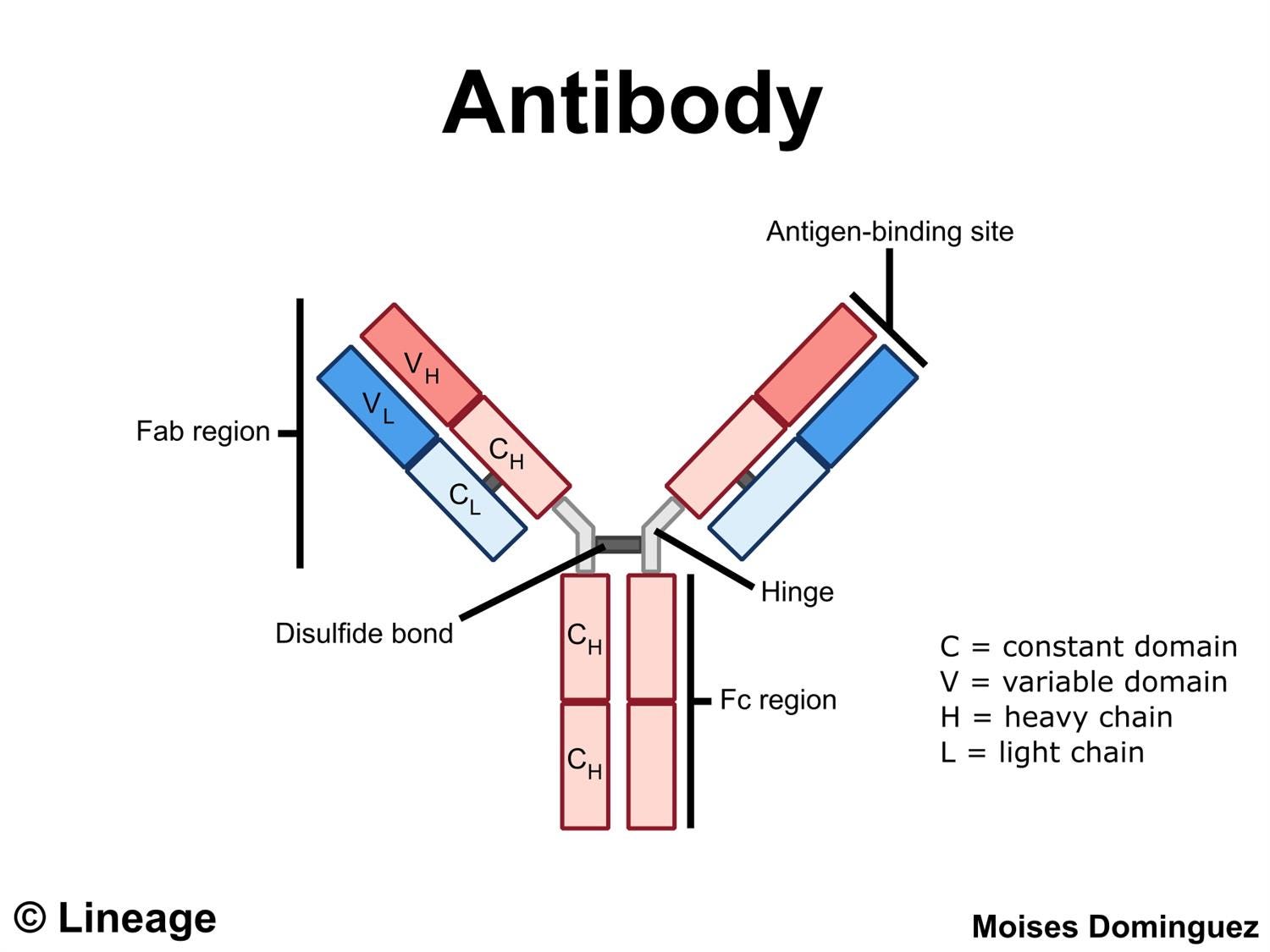
A spike protein is made up of 1,273 amino acids. Therefore, the data showing that the protein shares around 600 regions composed of sequences made up of sets of at least five amino acids, indicates that the spike protein shares many similarities, with areas of overlapping hot spots.
There are also 20 regions where the spike protein shares not only the same sequences of amino acids, it also shares the same shape.
Dr. Peter McCullough, cardiologist and co-author of Courage to Face the Virus, told The Epoch Times that the study explains the phenomena being seen in vaccinated and infected individuals.
“One is the actin-binding protein IPP that would influence heart muscle. So the auto-attack against this actin binding muscle could be part of the pathogenesis of myocarditis. The same is true for the tropomyosin alpha 3 chain [found in smooth muscles]. So some of these 3d targets are explaining some of these post respiratory illnesses in post vaccine syndromes that we’re seeing.”
The authors of the study specifically focused on two sequences with high similarity. One is the TQLPP sequence which is found on the human protein thrombopoietin, a protein in charge of recruiting platelets to stop bleeding. Another is the ELDKY sequence which is shared across the PRKG1 protein which is involved in platelet activation and calcium regulation, both of which are critical for blood clots.
Another protein is the aforementioned tropomyosin. The authors also speculated that antibody cross reacting to tropomyosin may be linked to cardiac diseases. “Antibodies cross-reacting with PRKG1 and tropomyosin may cause known COVID-19 complications such as blood-clotting disorders and cardiac disease, respectively,” they wrote.
However, Dr. Aristo Vojdani, an expert in autoimmunity, owner of 17 U.S. patents, co-author to 200 studies and two books on immunity told The Epoch Times that the regions identified by the recent study are not all of the regions that share similarities with human proteins.
He cited a study led by Dr. Yehuda Shoenfeld that found the spike protein shares similarities with 34 different human proteins in amino acid sequences in sets of sixes.
These include proteins found in the thyroid, brain, nose, ear, skin, muscles, heart, blood, nerves, joints, intestines, and many more.
Shoenfeld and his colleagues speculated that the spike protein may trigger Guillain-Barre syndrome, viral arthritis, immune thrombocytopenic purpura (bleeding), antiphospholipid syndrome, Kawasaki disease, systemic lupus erythematosus, and many others.
“The goal of the vaccine is to produce exactly the same spike protein that is in the virus … Because after vaccination, individuals will produce neutralizing antibodies. So in reality when the real virus will get into the human body those antibodies made against spike protein through mRNA injection or vaccination notifies [the body there’s] the virus,” said Vojdani.
Therefore, if the spike protein in the virus increases the risk of autoimmunity, there is reason to believe the spike proteins produced from the injections should do the same.
Studies Show Anti-SARS-CoV-2-Antibodies Attacking Human Tissue
In rebuttal, some studies have stated that similarities between human tissues and the spike protein are not enough for autoimmunity to occur.
Therefore, Vojdani and his colleagues have done further studies to test if spike proteins actually do pose a significant risk.
In one study, Vojdani took laboratory-made antibodies that attack human tissues, such as thyroid proteins, mitochondria, smooth muscle, and other proteins, and mixed them with spike proteins.
“[The antibodies] reacted strongly [with the spike proteins],” Vojdani said.
Because antibodies that attack human proteins also attack spike proteins, this implies that antibodies made against spike proteins may also attack human proteins.
His second evidence came from another study where he took monoclonal antibodies made in the laboratories against the SARS-CoV-2 virus, and added them to human tissue.
“They reacted from moderately to strongly with various tissue antigens including the muscles, joints, thyroid, brain, skin, gastrointestinal tract, almost any antigen taken from different parts of the body.”
The study found the anti-spike protein-antibodies reacted particularly strongly against proteins in the motor neurons, followed by strong reactions against mitochondrial proteins and against DNA. Having anti-DNA antibodies (ANA) are a hallmark sign of autoimmunity.
“That [is] additional evidence to support that spike protein not only shares homology with human tissue, when we will make antibodies … those antibodies may turn against our body and induce autoimmunity.”
“The third evidence came in our research where we obtained sera [the liquid in the blood, excluding red and white blood cells] … from many individuals with COVID versus healthy subjects.”
Vojdani and his colleagues found serum isolated from people who were infected with COVID-19 had more antibodies against human tissues than people who were not infected.
These studies all indicated that the spike protein is capable of inducing autoantibodies, possibly leading to autoimmune disease.
Vojdani said that he is waiting for more research to implicate the mRNA and DNA vaccine induced spike proteins’ roles in autoimmunity, because it normally can take several months to decades for autoimmunity to develop.
“It’s really too early to come to any conclusion, whether the vaccine contributes to autoimmunity.”
Though, he suggested researchers can test for vaccine-induced autoimmunity by harvesting antibodies from the vaccinated and comparing them to human proteins, possibly even testing to see if they react with human tissue.
Why Are Experts Concerned More About Vaccines Than Virus?
Dr. McCullough said that in infection, most people are able to clear the virus within days or weeks with early treatment, and most of the virus are also confined to the lungs, while the vaccines are directly shot into the muscles.
“Many [COVID-19] patients with respiratory illness, when they get early treatment, they just have a few days of symptoms, and that’s it—there’s little chance of systemic invasion. Whereas with the vaccine, everybody has systemic invasion of spike protein because it’s bypassing the sinuses.”
McCullough cited a paper led by Dr. Alana Ogata that detected S1 proteins (a portion of the spike protein) over 40 days and spike proteins around 30 days post-vaccination respectively. This is longer than the average period of infectiousness.
However, McCullough’s bigger concern is that with vaccine rollouts and people unaware of the risks, they would be taking boosters every six months, with the spike protein produced systematically, and persisting in the body for months.
“The opportunity for autoimmunity with injections every six months and boosters is tremendous,” he said. “The vaccines, because of the fact that they’re given by an injection in the arm—[it] is called parenteral [injections] … We are really, really running risks of autoimmunity in patients.”
Additionally, with a global rollout of the vaccines, and knowing that there may still be regions on the spike proteins that align with human sequences that we do not know about, McCullough speculates that it puts people at risk of developing autoimmune diseases that are less studied, more obscure, including possibly whole new types of autoimmune conditions.
“Autoimmunity is already a human problem … now we’re introducing a possibility for a massive number of new autoimmune syndromes, and it’s just because of the indiscriminate use of [COVID-19] vaccines.”
“[If] they were using [vaccines in] a small limited, high risk group, we wouldn’t be facing some of these very large possibilities of bad things happening in the human population, to two thirds of the world taking a vaccine. Even if a tiny percent develop autoimmunity, it’s going to be a massive number of people with autoimmune syndromes … it is really going to be a problem because of indiscriminate vaccination.”
Treatment Options
Dr. Ana Maria Mihalcea, who is an internal medical doctor and practices integrative and chelating medicine, said that she has had successes in treating patients who developed autoimmunity following vaccination.
“This is tested with a blood test looking for anti-nuclear antibodies (ANA), in essence they are showing an attack of the immune system against their own DNA,” she wrote in an email.
Mihalcea said that many people have treated autoimmunity associated with possible vaccine adverse effects with high doses of vitamin C and D daily (anti-inflammatory), as well as multiple vitamins, N-Acetyl cysteine (antioxidant and anti-inflammatory), and blood thinners.
Daily intake of quercetin (anti-inflammatory and ameliorates autoimmunity in animal studies), zinc (deficiencies associated with autoimmunity), dimethyl glycine (improves immune function), and methylene blue (antimicrobial, antitoxin, anti-inflammatory), as well as ivermectin (anti-inflammatory, improves cell healing) twice a week and hydroxychloroquine (anti-inflammatory, common autoimmune drug) three times a week are also recommended.
“In addition, I have done Vitamin C infusions and used the anti-aging peptides Epithalon which lengthens telomeres, repairs DNA, and age-reverses cells, and GHK Copper.”
Studies have shown that GHK copper can reset the human DNA, possibly resetting cellular action including autoimmune activity.
Debbie’s Journey Now
Jared expressed that what he found the most difficult to accept was the severe censorship and neglect Debbie faced during her recovery.
“When Debbie stands there and says, ‘I got the 1 in a million card’ [and got an adverse effect from the vaccine], everyone says ‘no, you didn’t, and don’t even talk about it and be quiet, otherwise you’re gonna get me fired,’ that’s a really crazy thing to have to deal with when she’s also trying to just deal with making her body work again.”
After a week of hospital treatment, Debbie entered remission and was put into rehabilitation to return mobility to her core and legs. She was left mostly unattended in the two months of rehabilitation and developed bed sores and deep venous blood clots from sitting and lying immobile for hours on end.
Since beginning rehabilitation at home in April, she has slowly gained mobility and sensation in her lower limbs. Yet, preceding regaining sensations, she experienced two months of excruciating pain.
“My feet felt like they were on fire and I would have shooting pain all the way up to my thighs, very, very, very painful. More painful than having a baby.”
However, her clinicians gave her the paradoxical answer that pain was a good sign, it showed the nerves going back online. Debbie toughed it out but sensation in her legs is still mostly abnormal.
“My legs, if I move them and I don’t have socks on, … feel like [they are being rubbed by] sandpaper. If I have a glass with condensation and it drips on my thigh, it hurts.”
Debbie stood up unassisted for the first time on Sept. 13, 2022.
Her doctors have told Debbie that she can make a full recovery. Debbie believes she is around 50 to 60 percent through her journey.
Pfizer did not respond to The Epoch Times’ request for comment.